
Stem Cell Markers CXCR-4 and CD133 Predict Aggressive Phenotype and Their Double Positivity Indicates Poor Prognosis of Oral Squamous Cell Carcinoma

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials & Methods
2.1. Tissues & Cell Line
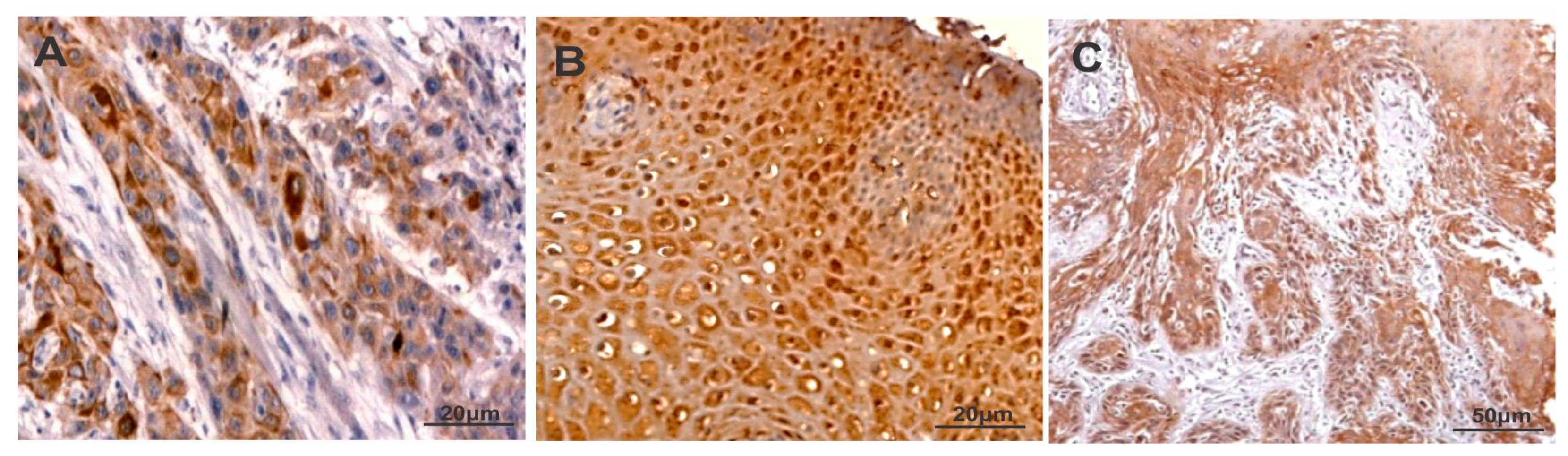
2.2. Immunohistochemistry
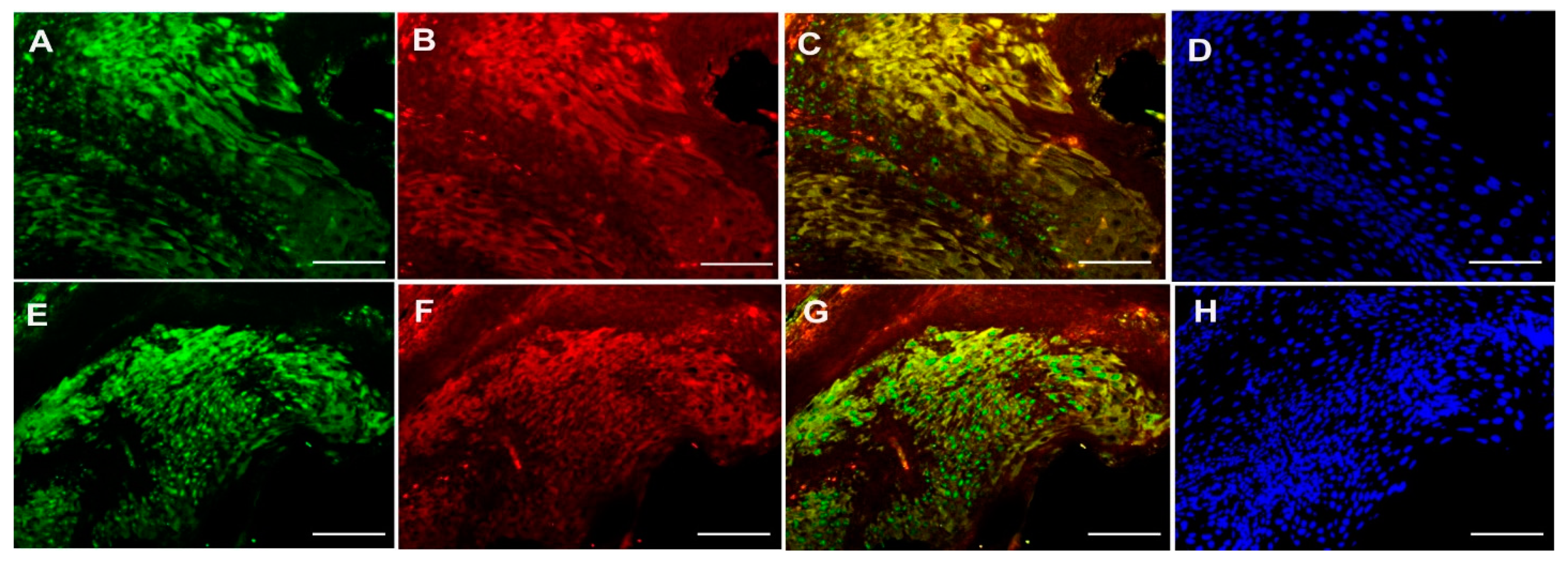
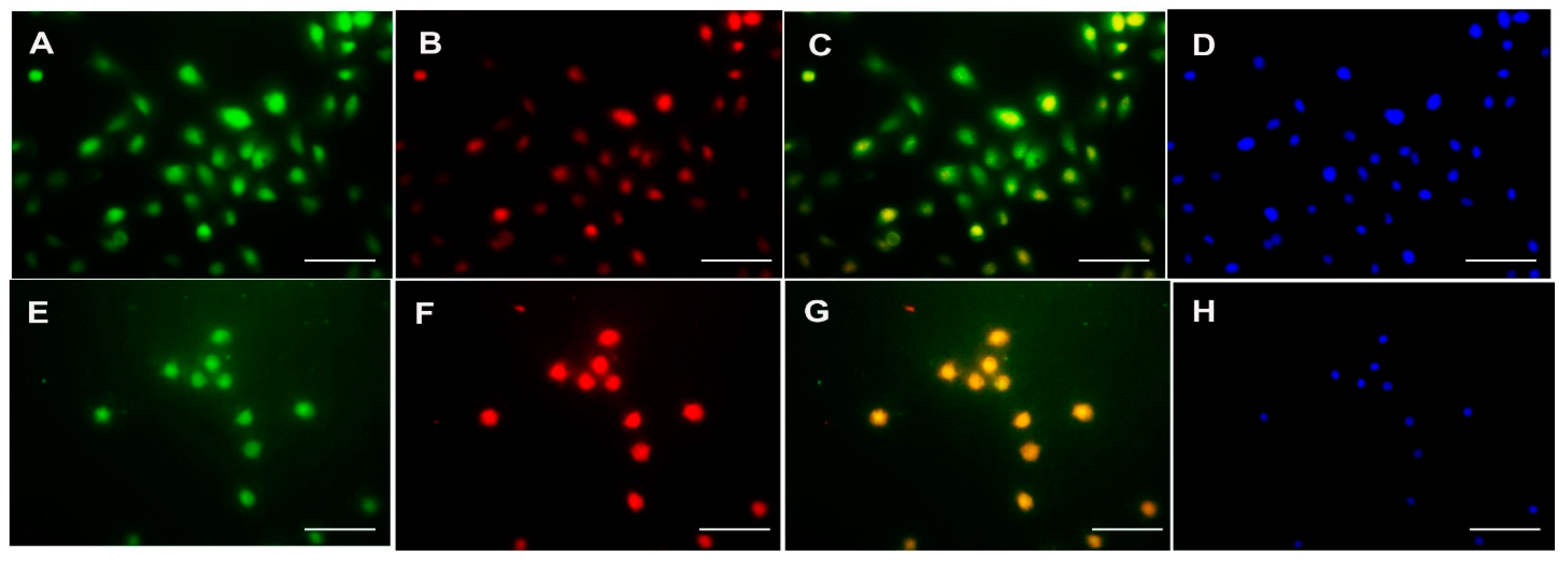
2.3. Immunofluorescence
2.4. Statistical Analysis
3. Results
3.1. CXCR4
3.2. PKC-δ
3.3. CD133
3.4. Correlation of CXCR-4 Expression with PKC-δ and CD133 in Oral Squamous Cell Carcinoma
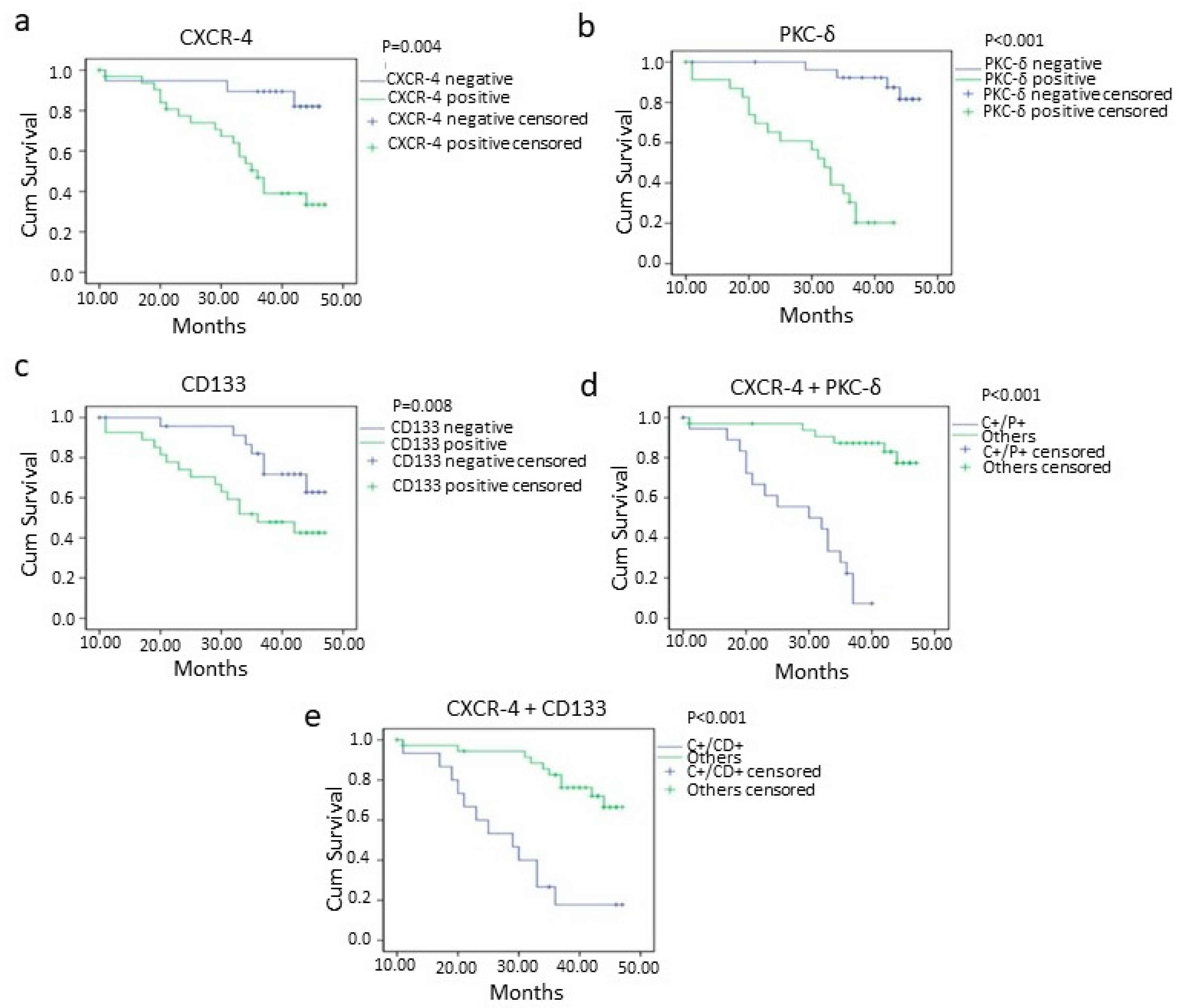
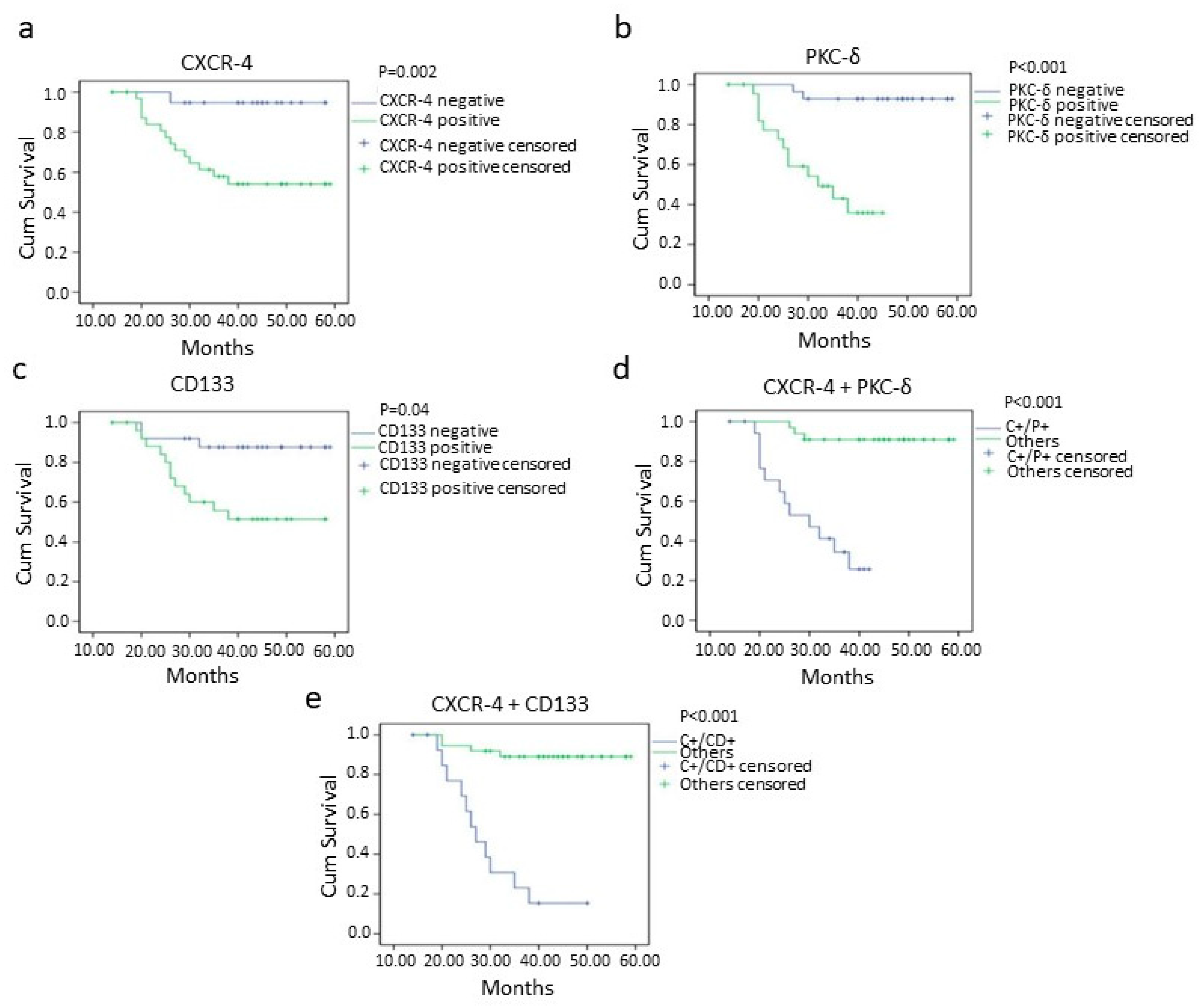
3.5. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levine, A.J.; Puzio-Kuter, A.M. The control of the metabolic switch in cancers by oncogenes and tumor suppressor genes. Science 2010, 330, 1340–1344. [Google Scholar] [CrossRef] [Green Version]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef]
- Gokulan, R.; Halagowder, D. Expression pattern of Notch intracellular domain (NICD) and Hes-1 in preneoplastic and neoplastic human oral squamous epithelium: Their correlation with c-Myc, clinicopathological factors and prognosis in Oral cancer. Med. Oncol. 2014, 31, 126. [Google Scholar] [CrossRef]
- Sawant, S.; Gokulan, R.; Dongre, H.; Vaidya, M.; Chaukar, D.; Prabhash, K.; Ingle, A.; Joshi, S.; Dange, P.; Joshi, S.; et al. Prognostic role of Oct4, CD44 and c-Myc in radio-chemo-resistant oral cancer patients and their tumourigenic potential in immunodeficient mice. Clin. Oral Investig. 2016, 20, 43–56. [Google Scholar] [CrossRef]
- Reya, T.; Morrison, S.J.; Clarke, M.F.; Weissman, I.L. Stem cells, cancer, and cancer stem cells. Nature 2001, 414, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Settleman, J. EMT, cancer stem cells and drug resistance: An emerging axis of evil in the war on cancer. Oncogene 2010, 29, 4741–4751. [Google Scholar] [CrossRef] [Green Version]
- Kucia, M.; Ratajczak, J.; Ratajczak, M.Z. Bone marrow as a source of circulating CXCR4+ tissue-committed stem cells. Biol. Cell 2005, 97, 133–146. [Google Scholar] [CrossRef]
- Zou, Y.R.; Kottmann, A.H.; Kuroda, M.; Taniuchi, I.; Littman, D.R. Function of the chemokine receptor CXCR4 in haematopoiesis and in cerebellar development. Nature 1998, 393, 595–599. [Google Scholar] [CrossRef]
- Kucia, M.; Reca, R.; Miekus, K.; Wanzeck, J.; Wojakowski, W.; Janowska-Wieczorek, A.; Ratajczak, J.; Ratajczak, M.Z. Trafficking of normal stem cells and metastasis of cancer stem cells involve similar mechanisms: Pivotal role of the SDF-1-CXCR4 axis. Stem Cells 2005, 23, 879–894. [Google Scholar] [CrossRef]
- Tang, C.H.; Chuang, J.Y.; Fong, Y.C.; Maa, M.C.; Way, T.D.; Hung, C.H. Bone-derived SDF-1 stimulates IL-6 release via CXCR4, ERK and NF-kappaB pathways and promotes osteoclastogenesis in human oral cancer cells. Carcinogenesis 2008, 29, 1483–1492. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.T.; Chu, C.Y.; Lu, Y.C.; Chang, C.C.; Lin, B.R.; Wu, H.H.; Liu, H.L.; Cha, S.T.; Prakash, E.; Ko, J.Y.; et al. CXCL12/CXCR4 promotes laryngeal and hypopharyngeal squamous cell carcinoma metastasis through MMP-13-dependent invasion via the ERK1/2/AP-1 pathway. Carcinogenesis 2008, 29, 1519–1527. [Google Scholar] [CrossRef] [Green Version]
- Teicher, B.A.; Fricker, S.P. CXCL12 (SDF-1)/CXCR4 pathway in cancer. Clin. Cancer Res. 2010, 16, 2927–2931. [Google Scholar] [CrossRef] [Green Version]
- Xu, C.; Zhao, H.; Chen, H.; Yao, Q. CXCR4 in breast cancer: Oncogenic role and therapeutic targeting. Drug Des. Devel. Ther. 2015, 9, 4953–4964. [Google Scholar] [CrossRef] [Green Version]
- Xia, J.; Chen, N.; Hong, Y.; Chen, X.; Tao, X.; Cheng, B.; Huang, Y. Expressions of CXCL12/CXCR4 in oral premalignant and malignant lesions. Mediat. Inflamm. 2012, 2012, 516395. [Google Scholar] [CrossRef]
- Hong, J.S.; Pai, H.K.; Hong, K.O.; Kim, M.A.; Kim, J.H.; Lee, J.I.; Hong, S.P.; Hong, S.D. CXCR-4 knockdown by small interfering RNA inhibits cell proliferation and invasion of oral squamous cell carcinoma cells. J. Oral Pathol. Med. 2009, 38, 214–219. [Google Scholar] [CrossRef]
- Ishikawa, T.; Nakashiro, K.; Hara, S.; Klosek, S.K.; Li, C.; Shintani, S.; Hamakawa, H. CXCR4 expression is associated with lymph-node metastasis of oral squamous cell carcinoma. Int. J. Oncol. 2006, 28, 61–66. [Google Scholar] [CrossRef]
- Huang, S.J.; Tseng, Y.K.; Lo, Y.H.; Wu, P.C.; Lee, J.H.; Liou, H.H.; Liang, C.C.; Yang, C.M.; Wang, C.C.; Yen, L.M.; et al. Association of SDF-1 and CXCR4 Polymorphisms With Susceptibility to Oral and Pharyngeal Squamous Cell Carcinoma. Anticancer Res. 2019, 39, 2891–2902. [Google Scholar] [CrossRef]
- Taki, M.; Higashikawa, K.; Yoneda, S.; Ono, S.; Shigeishi, H.; Nagayama, M.; Kamata, N. Up-regulation of stromal cell-derived factor-1alpha and its receptor CXCR4 expression accompanied with epithelial-mesenchymal transition in human oral squamous cell carcinoma. Oncol. Rep. 2008, 19, 993–998. [Google Scholar]
- Zhuang, X.M.; Zhou, B. CXCR4 enhances cisplatin resistance of human tongue squamous cell carcinoma. J. Oral Pathol. Med. 2019, 48, 122–128. [Google Scholar] [CrossRef]
- Petit, I.; Goichberg, P.; Spiegel, A.; Peled, A.; Brodie, C.; Seger, R.; Nagler, A.; Alon, R.; Lapidot, T. Atypical PKC-zeta regulates SDF-1-mediated migration and development of human CD34+ progenitor cells. J. Clin. Investig. 2005, 115, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.; Ouyang, N.; Lin, L.; Chen, L.; Wu, W.; Su, F.; Yao, Y.; Yao, H. HGF-induced PKCzeta activation increases functional CXCR4 expression in human breast cancer cells. PLoS ONE 2012, 7, e29124. [Google Scholar] [CrossRef] [Green Version]
- Basu, A.; Pal, D. Two faces of protein kinase Cdelta: The contrasting roles of PKCdelta in cell survival and cell death. Sci. World J. 2010, 10, 2272–2284. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Forman, L.W.; Williams, R.M.; Faller, D.V. Protein kinase C-delta inactivation inhibits the proliferation and survival of cancer stem cells in culture and in vivo. BMC Cancer 2014, 14, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, N.H.; Li, J.; Li, Y.; Zhang, X.T.; Liao, W.T.; Zhang, J.Y.; Li, R.; Luo, R.C. Co-expression of CXCR4 and CD133 proteins is associated with poor prognosis in stage II-III colon cancer patients. Exp. Ther. Med. 2012, 3, 973–982. [Google Scholar] [CrossRef]
- Miraglia, S.; Godfrey, W.; Yin, A.H.; Atkins, K.; Warnke, R.; Holden, J.T.; Bray, R.A.; Waller, E.K.; Buck, D.W. A novel five-transmembrane hematopoietic stem cell antigen: Isolation, characterization, and molecular cloning. Blood 1997, 90, 5013–5021. [Google Scholar] [CrossRef] [PubMed]
- Jaszai, J.; Fargeas, C.A.; Florek, M.; Huttner, W.B.; Corbeil, D. Focus on molecules: Prominin-1 (CD133). Exp. Eye Res. 2007, 85, 585–586. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Hawkins, C.; Clarke, I.D.; Squire, J.A.; Bayani, J.; Hide, T.; Henkelman, R.M.; Cusimano, M.D.; Dirks, P.B. Identification of human brain tumour initiating cells. Nature 2004, 432, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Horst, D.; Kriegl, L.; Engel, J.; Kirchner, T.; Jung, A. CD133 expression is an independent prognostic marker for low survival in colorectal cancer. Br. J. Cancer 2008, 99, 1285–1289. [Google Scholar] [CrossRef]
- Chiou, S.H.; Yu, C.C.; Huang, C.Y.; Lin, S.C.; Liu, C.J.; Tsai, T.H.; Chou, S.H.; Chien, C.S.; Ku, H.H.; Lo, J.F. Positive correlations of Oct-4 and Nanog in oral cancer stem-like cells and high-grade oral squamous cell carcinoma. Clin. Cancer Res. 2008, 14, 4085–4095. [Google Scholar] [CrossRef] [Green Version]
- Ravindran, G.; Sawant, S.S.; Hague, A.; Kingsley, K.; Devaraj, H. Association of differential beta-catenin expression with Oct-4 and Nanog in oral squamous cell carcinoma and their correlation with clinicopathological factors and prognosis. Head Neck 2015, 37, 982–993. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Shi, S.; Yen, Y.; Brown, J.; Ta, J.Q.; Le, A.D. A subpopulation of CD133(+) cancer stem-like cells characterized in human oral squamous cell carcinoma confer resistance to chemotherapy. Cancer Lett. 2010, 289, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Damek-Poprawa, M.; Volgina, A.; Korostoff, J.; Sollecito, T.P.; Brose, M.S.; O’Malley, B.W., Jr.; Akintoye, S.O.; DiRienzo, J.M. Targeted inhibition of CD133+ cells in oral cancer cell lines. J. Dent. Res. 2011, 90, 638–645. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.S.; Han, Z.P.; Jing, Y.Y.; Tao, S.F.; Li, T.J.; Wang, H.; Wang, Y.; Li, R.; Yang, Y.; Zhao, X.; et al. CD133(+)CXCR4(+) colon cancer cells exhibit metastatic potential and predict poor prognosis of patients. BMC Med. 2012, 10, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermann, P.C.; Huber, S.L.; Herrler, T.; Aicher, A.; Ellwart, J.W.; Guba, M.; Bruns, C.J.; Heeschen, C. Distinct populations of cancer stem cells determine tumor growth and metastatic activity in human pancreatic cancer. Cell Stem Cell 2007, 1, 313–323. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.C.; Hu, F.W.; Yu, C.H.; Chou, M.Y. Targeting CD133 in the enhancement of chemosensitivity in oral squamous cell carcinoma-derived side population cancer stem cells. Head Neck 2016, 38 (Suppl. S1), E231–E238. [Google Scholar] [CrossRef] [PubMed]
- Pindborg, J.J.; Wahi, P.N. Histological Typing of Cancer and Precancer of the Oral Mucosa, 2nd ed.; Springer: Berlin, Germany, 1997. [Google Scholar]
- Ravindran, G.; Devaraj, H. Prognostic significance of neural stem cell markers, Nestin and Musashi-1, in oral squamous cell carcinoma: Expression pattern of Nestin in the precancerous stages of oral squamous epithelium. Clin. Oral. Investig. 2015, 19, 1251–1260. [Google Scholar] [CrossRef]
- Moitra, K. Overcoming Multidrug Resistance in Cancer Stem Cells. Biomed. Res. Int. 2015, 2015, 635745. [Google Scholar] [CrossRef] [Green Version]
- Uchida, D.; Begum, N.M.; Almofti, A.; Nakashiro, K.; Kawamata, H.; Tateishi, Y.; Hamakawa, H.; Yoshida, H.; Sato, M. Possible role of stromal-cell-derived factor-1/CXCR4 signaling on lymph node metastasis of oral squamous cell carcinoma. Exp. Cell Res. 2003, 290, 289–302. [Google Scholar] [CrossRef]
- Delilbasi, C.B.; Okura, M.; Iida, S.; Kogo, M. Investigation of CXCR4 in squamous cell carcinoma of the tongue. Oral Oncol. 2004, 40, 154–157. [Google Scholar] [CrossRef]
- Takabayashi, T.; Takahashi, N.; Okamoto, M.; Yagi, H.; Sato, M.; Fujieda, S. Lipopolysaccharides increase the amount of CXCR4, and modulate the morphology and invasive activity of oral cancer cells in a CXCL12-dependent manner. Oral Oncol. 2009, 45, 968–973. [Google Scholar] [CrossRef]
- Lee, J.I.; Jin, B.H.; Kim, M.A.; Yoon, H.J.; Hong, S.P.; Hong, S.D. Prognostic significance of CXCR-4 expression in oral squamous cell carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.L.; Ji, Y.; Ge, D.; Guo, J.; Ding, J.Y. The expression of CXCR4 and its relationship with matrix metalloproteinase-9/vascular endothelial growth factor in esophageal squamous cell cancer. Dis. Esophagus 2011, 24, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Uchida, D.; Onoue, T.; Kuribayashi, N.; Tomizuka, Y.; Tamatani, T.; Nagai, H.; Miyamoto, Y. Blockade of CXCR4 in oral squamous cell carcinoma inhibits lymph node metastases. Eur. J. Cancer 2011, 47, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, G.; Devaraj, H. Aberrant expression of CD133 and musashi-1 in preneoplastic and neoplastic human oral squamous epithelium and their correlation with clinicopathological factors. Head Neck 2012, 34, 1129–1135. [Google Scholar] [CrossRef]
- Lu, C.; Xu, F.; Gu, J.; Yuan, Y.; Zhao, G.; Yu, X.; Ge, D. Clinical and biological significance of stem-like CD133(+)CXCR4(+) cells in esophageal squamous cell carcinoma. J. Thorac. Cardiovasc. Surg. 2015, 150, 386–395. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protein | No. of Cases | 0 | 1+ | 2+ | 3+ |
|---|---|---|---|---|---|
| CXCR-4 | 51 | 11 | 7 | 15 | 18 |
| PKC-δ | 51 | 13 | 8 | 20 | 10 |
| CD133 | 51 | 9 | 13 | 18 | 11 |
| CXCR-4 | PKC-δ | CD133 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Negative (18) | Positive (33) | p Value | Negative (21) | Positive (30) | p Value | Negative (22) | Positive (29) | p Value | ||
| No. of Patients | ||||||||||
| Age | ||||||||||
| ≤60 | 26 | 12 | 14 | p < 0.14 | 10 | 16 | p < 0.77 | 8 | 18 | p < 0.09 |
| >60 | 25 | 6 | 19 | 11 | 14 | 14 | 11 | |||
| Gender | ||||||||||
| Male | 29 | 11 | 18 | p < 0.77 | 15 | 14 | p < 0.09 | 14 | 15 | p < 0.56 |
| Female | 22 | 7 | 15 | 6 | 16 | 8 | 14 | |||
| Stage | ||||||||||
| I–II | 24 | 9 | 15 | p < 0.78 | 14 | 10 | p < 0.02 * | 16 | 8 | p < 0.001 * |
| III–IV | 27 | 9 | 18 | 7 | 20 | 6 | 21 | |||
| Lymph node Metastasis | ||||||||||
| Negative | 23 | 15 | 8 | p < 0.001 ** | 16 | 7 | p < 0.001 ** | 15 | 8 | p < 0.005 ** |
| Positive | 28 | 3 | 25 | 5 | 23 | 7 | 21 | |||
| Histological Grade | ||||||||||
| Well Differentiated | 8 | 6 | 2 | p < 0.02 * | 6 | 2 | p < 0.10 | 7 | 1 | p < 0.008 ** |
| Moderately Differentiated | 19 | 7 | 12 | 7 | 12 | 9 | 10 | |||
| Poorly Differentiated | 24 | 5 | 19 | 8 | 16 | 6 | 18 | |||
| Location of the Tumours | ||||||||||
| Tongue | 15 | 8 | 7 | p < 0.42 | 7 | 8 | p < 0.54 | 6 | 9 | p < 0.56 |
| Buccal | 9 | 3 | 6 | 5 | 4 | 4 | 5 | |||
| Palate | 8 | 3 | 5 | 4 | 4 | 4 | 4 | |||
| Gingiva | 10 | 2 | 8 | 3 | 7 | 6 | 4 | |||
| Floor of Mouth | 9 | 2 | 7 | 2 | 7 | 2 | 7 | |||
| Expression of CXCR-4 | Expression of PKC-δ | Expression of CD133 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| (No. of Patients = 51) | 0 (13) | 1+ (8) | 2+ (10) | 3+ (20) | 0 (9) | 1+ (13) | 2+ (11) | 3+ (18) | |
| 0 | 11 | 9 | 2 | 0 | 0 | 9 | 2 | 0 | 0 |
| 1+ | 7 | 3 | 3 | 1 | 0 | 0 | 5 | 2 | 0 |
| 2+ | 15 | 1 | 3 | 2 | 9 | 0 | 6 | 3 | 6 |
| 3+ | 18 | 0 | 0 | 7 | 11 a | 0 | 0 | 3 | 12 b |
| Variables | Overall Survival | Disease-Free Survival | |
|---|---|---|---|
| p Value | p Value | ||
| 1 | Age | 0.30 | 0.42 |
| 2 | Sex | 0.78 | 0.52 |
| 3 | Stage (I,II/III,IV) | 0.0008 ** | 0.03 * |
| 4 | Grade (Well/Moderate/Poor) | 0.38 | 0.53 |
| 5 | LN Metastasis (+/−) | <0.001 ** | 0.01 * |
| 6 | CXCR-4 (+/−) | 0.004 ** | 0.002 ** |
| 7 | PKC-δ (+/−) | <0.001 ** | <0.001 ** |
| 8 | CD133 (+/−) | 0.008 * | 0.04 |
| 9 | CXCR-4 + PKC-δ (C+/P+ vs. others) | <0.001 ** | <0.001 ** |
| 10 | CXCR-4 + CD133 (C+/CD+ vs. others) | <0.001 ** | <0.001 ** |
| 11 | PKC- + CD133 (P+/CD+ vs. others) | <0.001 ** | <0.001 ** |
| Variables | Overall Survival | Disease-Free Survival | |||||
|---|---|---|---|---|---|---|---|
| p Value | Hazards Ratio | 95% CI | p Value | Hazards Ratio | 95% CI | ||
| 1 | Stage (I,II/III,IV) | 0.005 ** | 8.354 | 1.877–37.180 | 0.04 * | 2.529 | 1.028–6.220 |
| 2 | Grade (Well/Moderate/Poor) | 0.394 | 0.627 | 0.214–1.836 | 0.479 | 0.734 | 0.312–1.727 |
| 3 | LN Metastasis(+/−) | 0.046 * | 10.895 | 1.072–55.034 | 0.014 * | 3.292 | 1.274–8.503 |
| 4 | CXCR-4 (+/−) | 0.023 * | 10.567 | 1.388–80.442 | 0.006 ** | 5.612 | 1.651–19.078 |
| 5 | PKC-δ (+/−) | 0.001 ** | 12.682 | 2.833–56.771 | <0.001 ** | 14.473 | 4.034–51.927 |
| 6 | CD133 (+/−) | 0.01 * | 4.688 | 1.321–16.640 | 0.049 * | 2.440 | 0.993–5.998 |
| Variables | Overall Survival | Disease-Free Survival | |||||
|---|---|---|---|---|---|---|---|
| p Value | Hazards Ratio | 95% CI | p Value | Hazards Ratio | 95% CI | ||
| 1 | CXCR-4 | 0.226 | 3.645 | 0.448–29.628 | 0.029 * | 4.652 | 1.172–18.471 |
| 2 | PKC-δ | 0.107 | 3.589 | 0.757–17.004 | 0.001 ** | 16.173 | 3.332–78.496 |
| 3 | CD133 | 0.282 | 2.109 | 0.541–8.217 | 0.023 * | 3.801 | 1.202–12.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caspa Gokulan, R.; Devaraj, H. Stem Cell Markers CXCR-4 and CD133 Predict Aggressive Phenotype and Their Double Positivity Indicates Poor Prognosis of Oral Squamous Cell Carcinoma. Cancers 2021, 13, 5895. https://doi.org/10.3390/cancers13235895
Caspa Gokulan R, Devaraj H. Stem Cell Markers CXCR-4 and CD133 Predict Aggressive Phenotype and Their Double Positivity Indicates Poor Prognosis of Oral Squamous Cell Carcinoma. Cancers. 2021; 13(23):5895. https://doi.org/10.3390/cancers13235895
Chicago/Turabian StyleCaspa Gokulan, Ravindran, and Halagowder Devaraj. 2021. "Stem Cell Markers CXCR-4 and CD133 Predict Aggressive Phenotype and Their Double Positivity Indicates Poor Prognosis of Oral Squamous Cell Carcinoma" Cancers 13, no. 23: 5895. https://doi.org/10.3390/cancers13235895
APA StyleCaspa Gokulan, R., & Devaraj, H. (2021). Stem Cell Markers CXCR-4 and CD133 Predict Aggressive Phenotype and Their Double Positivity Indicates Poor Prognosis of Oral Squamous Cell Carcinoma. Cancers, 13(23), 5895. https://doi.org/10.3390/cancers13235895