Simple Summary
Diabetes mellitus is a common disease in patients with cancer. It is a risk factor for certain cancers such as pancreatic, liver, colon, breast, and endometrial cancer. Furthermore, several new cancer treatments or the use of steroids may unmask underlying diabetes or aggravate preexisting diabetes. Evidence suggests that patients with cancer and diabetes have higher cancer-related mortality. Moreover, concurrent complications associated with diabetes in patients with cancer may influence the choice of cancer therapy. This review highlights the relationship between diabetes and cancer and various aspects of the management of diabetes in patients with cancer.
Abstract
Background: Diabetes mellitus and cancer are commonly coexisting illnesses, and the global incidence and prevalence of both are rising. Cancer patients with diabetes face unique challenges. This review highlights the relationship between diabetes and cancer and various aspects of the management of diabetes in cancer patients. Methods: A literature search using keywords in PubMed was performed. Studies that were published in English prior to July 2021 were assessed and an overview of epidemiology, cancer risk, outcomes, treatment-related hyperglycemia and management of diabetes in cancer patients is provided. Results: Overall, 8–18% of cancer patients have diabetes as a comorbid medical condition. Diabetes is a risk factor for certain solid malignancies, such as pancreatic, liver, colon, breast, and endometrial cancer. Several novel targeted compounds and immunotherapies can cause hyperglycemia. Nevertheless, most patients undergoing cancer therapy can be managed with an appropriate glucose lowering agent without the need for discontinuation of cancer treatment. Evidence suggests that cancer patients with diabetes have higher cancer-related mortality; therefore, a multidisciplinary approach is important in the management of patients with diabetes and cancer for a better outcome. Conclusions: Future studies are required to better understand the underlying mechanism between the risk of cancer and diabetes. Furthermore, high-quality prospective studies evaluating management of diabetes in cancer patients using innovative tools are needed. A patient-centered approach is important in cancer patients with diabetes to avoid adverse outcomes.
1. Introduction
Diabetes is a common disease among cancer patients, yet few prospective studies have evaluated its impact on cancer care. Approximately 10% of the North American population have diabetes, of which about 95% have type 2 diabetes [1,2]. Diabetes is a risk factor for certain solid malignancies such as pancreatic, liver, colon, breast, and endometrial cancer [3,4]. Cancer patients with diabetes face unique challenges. Several novel cancer therapies or the concurrent use of steroids may unmask underlying diabetes or aggravate preexisting diabetes [5,6,7]. Evidence suggests that cancer patients with diabetes have higher cancer-related mortality and patients with diabetes are at an increased risk of various infections and infection-related morbidity and mortality [4,8,9,10]. In general, individuals with diabetes have an annual mortality rate twice that of the general population of similar age [11,12,13]. Cancer patients with diabetes may receive suboptimal care that could lead to inferior outcomes [14]. Moreover, concurrent complications associated with diabetes such as chronic renal insufficiency, cardiovascular disease, peripheral neuropathy, and chronic infection in diabetic patients may influence the choice of cancer therapy. Therefore, these factors may limit the use of certain drugs or optimal dosing that may lead to lower benefits and shorter survival. In the context of the current scarcity of literature on diabetes and cancer, this review has been undertaken to provide an overview of the epidemiology, cancer risk, outcomes, cancer treatment-related hyperglycemia and the management of diabetes in cancer patients.
2. Literature Search
A literature search using PubMed was performed and the studies that were published in English involving human subjects prior to July 2021 were assessed. The following keywords were used in combination: ‘diabetes mellitus’, ‘diabetes’, ‘hyperglycemia’, ‘diabetic ketoacidosis’, ‘prediabetes’, ‘insulin’, ‘oral hypoglycemic agent’, and ‘cancer’, ‘malignancy’, ‘targeted therapy’, ‘immunotherapy’, or ‘cancer therapy’.
3. Classification
Type 1 diabetes is characterized by a lack of insulin production by the pancreas mostly due to the autoimmune-mediated destruction of pancreatic beta cell. In contrast, type 2 diabetes is characterized by combination of peripheral insulin resistance and dysfunctional insulin secretion by pancreatic beta cells, which results in high but inappropriately low circulating insulin concentrations for the level of glycemia [15]. Most people with diabetes have type 2 diabetes and only about 5-10% of individuals have type 1 diabetes. Both type 1 and type 2 diabetes are multifactorial diseases involving several genetic and environmental factors. However, obesity and other life style factors play an important role in the development of type 2 diabetes [15]. Diabetes can also develop secondarily to medication or from an underlying illness. Various cancer directed agents that are discussed below could unmask underlying diabetes or cause secondary diabetes [16,17,18]. Among secondary diabetes, type 3c diabetes mellitus is secondary to diseases of the exocrine pancreas including pancreatitis and pancreatic cancer [19].
4. Epidemiology
Cancer and diabetes have several common risk factors, such as obesity, smoking, aging, physical inactivity and unhealthy diet [20]. The global incidence and prevalence of both cancer and diabetes are rising. It is estimated that in 2017 more than 450 million people were living with diabetes worldwide, whereas the current incidence of cancer excluding non-melanoma skin cancer is about 19.3 million [21,22]. Cancer is primarily a disease of older adults, with the median age of a cancer diagnosis being 66 years [23]. Approximately 60% of patients that are newly-diagnosed with cancer are aged ≥65 and about 25% of persons aged ≥65 develop diabetes mellitus [24]. Overall, 8–18% of cancer patients have diabetes as a comorbid medical condition, with the percentage depending on the cancer site. A case of new-onset diabetes could be marker of underlying pancreatic cancer. A population-based study found that 1% of subjects aged ≥50 years with new-onset diabetes had underlying pancreatic cancer [25].
Given the high prevalence of diabetes in the general population, screening for diabetes is important in cancer patients prior to commencement of systemic anticancer therapy. In addition, patients with diabetes should be undergo age-appropriate cancer screenings [26].
5. Link between Diabetes and Cancer
5.1. Mechanism of Cancer Risk in Diabetes
Hyperglycemia, insulin resistance, elevated insulin and insulin-like growth factor-1 (IGF-1) levels, inflammatory cytokines, dyslipidemia, increased leptin, and decreased adiponectin have been attributed to the increased risk of cancer in patients with diabetes [27]. Insulin is a member of a family of growth factors that includes IGF-I and IGF-II [28]. Insulin is most widely known for its metabolic effects, but it also has important mitogenic effects [27,28]. Hyperinsulinemia due to insulin resistance, hyperglycemia, dysregulations of sex hormones, oxidative stress, and inflammatory cytokines potentially play a role in the development of cancer [29,30], and elevated glucose levels lead to the proliferation of various solid tumor cell lines [31,32]. Both the liver and the pancreas are exposed to a high insulin concentration, as insulin is transported to the liver via the portal vein following release from pancreatic β-cells [29]. In addition, underlying obesity associated with diabetes has cancer-promoting effects secondary to increased peripheral estrogens, increased pro-mitogen cytokines and growth factors related to excess fat tissue [27]. Moreover, fat-associated chronic inflammation, the release of inflammatory cytokines and the generation of reactive oxygen species (ROS) result in cell damage, cancer growth, and invasiveness [27,33].
5.2. Role of the Microbiome in Cancer and Diabetes
It is worth mentioning the evolving role of the gut microbiome in the development of diabetes and cancer [34,35,36]. The human digestive tract has trillions of microorganisms including bacteria, viruses, yeast, protozoa, and fungi that interact with each other and the host and play a role in homeostasis and the development of diseases. Cancer cells depend on glucose and glycolysis as a key source of energy. The complex interaction between the gut microbiome, sugar compounds, insulin resistance, and cancer is not fully known. Nevertheless, evidence supports that extrinsic factors including diet, the environment, and sugar compounds disrupt the gut microbial diversity and function, a phenomenon known as dysbiosis, and increase the risk of insulin resistance, diabetes and several types of gastrointestinal, hepatobiliary and head and neck cancers such as liver, pancreatic, esophageal, and most notably colorectal cancer [34,35,37,38,39]. The underlying mechanism leading to cancer is not known and may involve chronic inflammation, impaired host immune function, production of carcinogenic byproducts, and disruption of programmed cell death [36,40]. In addition, there is emerging evidence that certain infection such as candidiasis, which is more common patients with diabetes, has been associated with an increased risk of cancer [37,41,42].
5.3. Epidemiological Link between Diabetes and Cancer
Most published studies evaluating the association between cancer and diabetes have not made a distinction between the two main types of diabetes. As type 2 diabetes is more common than type 1diabetes, the study populations have been largely comprised of individuals with type 2 diabetes. Nevertheless, studies that focused on individuals with type I diabetes and were adequately powered have shown an excess risk of cancer and cancer-related mortality for overall and various site-specific cancers in both type 1 and type 2 diabetes [43,44].
Stocks et al. examined six European cohorts including 274,126 men and 275,818 women, showing that for a 1 mmol/l increment in blood glucose the relative risk of cancer in men is 1.05 (1.01–1.10) and in women is 1.11 (1.05–1.16) [45]. Diabetes and hyperglycemia are associated with an elevated risk of developing pancreatic, liver, colorectal, breast, bladder and endometrial cancer, and a lower risk of prostate cancer [3,4,46,47]. A meta-analysis of 151 cohorts including over 32 million people, 1.1 million cancer cases, and 150,000 cancer deaths showed a strong association between type 2 diabetes and liver, pancreatic, and endometrial cancer incidence, and pancreatic cancer mortality [3]. A population-based case control study using the Surveillance Epidemiology and End-Results Program (SEER) data showed that diabetes was an independent risk factor for hepatocellular cancer, with an odds ratio of 3.08 (95% CI: 2.74–3.46) [48]. Likewise, a meta-analysis of 40 studies showed that women with diabetes have a relative risk of development of breast cancer of 1.27 (95% CI: 1.16–1.39) [49]. Another meta-analysis of 35 cohort studies showed that diabetes was associated with an independent relative risk of pancreatic cancer of 1.94 (95% CI: 1.66–2.27) [50]. However, the association between pancreatic cancer and diabetes is complex; a recent diagnosis of diabetes may be an early sign of pancreatic cancer and may reflect insulin resistance that is elicited by pancreatic cancer [51]. A comprehensive umbrella review of 27 meta-analyses of type 2 diabetes and various cancers demonstrated that diabetes is associated with a 10% relative risk of cancer (RR: 1.10; 95% CI: 1.04–1.17) [52].
5.4. Diabetic Pharmacotherapy and Risk of Cancer
Insulin is the mainstay of treatment for type 1 diabetes, but for type 2 diabetes, both hypoglycemic medication and insulin are used. There have been concerns regarding whether exogenous insulin, especially insulin glargine, could increase the risk of cancer [53,54]. The ORIGIN trial investigators randomized 12,537 subjects with impaired glucose tolerance, or type 2 diabetes to insulin glargine or standard care and examined cardiovascular outcomes and incidence of cancer [55]. The investigators did not find an increased risk of cancer with the use of basal insulin glargine (hazard ratio for cancer, 1.00). At the present time, it is not conclusive whether there is an increased risk of malignancy from exogenous insulin that warrants a change in the clinical practice [56]. With respect to the association between other anti-diabetes medications and cancer incidence and mortality, the current data are conflicting and there is no definite evidence that they either increase or decrease the risk of cancer [57]. For example, retrospective cohort studies have shown that incretin-based therapies involving glucagon-like peptide 1 receptor agonists (GLP-1 RAs) and dipeptidyl peptidase 4 (DPP-4) inhibitors in patients with diabetes have been associated with an increased risk of pancreatic cancer [58]. However, a meta-analysis of 33 studies did not confirm a positive relationship between incretin-based therapies and pancreatic cancer and a causal relationship between incretin-based therapies and pancreatic cancer or pancreatitis is no known [59,60].
On the contrary, preclinical studies have demonstrated antineoplastic effects of metformin, an oral biguanide, and this has subsequently been supported by several large epidemiological studies and meta-analyses [61,62]. However, to date, no randomized clinical trial has confirmed its protective effect in cancer.
6. Diabetes Mellitus & Cancer Outcomes
Diabetes may negatively influence prognosis because of other associated comorbidities, as well as the risk of non-cancer-related causes of death [12,14]. Continuous exposure to hyperglycemia and elevated concentrations of circulating insulin might stimulate cancer growth and progression, leading to poorer prognosis. Patients with established diabetes, elevated insulin concentrations, elevated insulin-like growth factors, and abnormal glucose tolerance experience higher mortality and recurrence rates after diagnosis and treatment of underlying cancer [9,63,64,65]. Several cohort studies have suggested a higher cancer-related mortality among patients with diabetes and certain solid malignancies [8,9]. Epidemiological studies have shown that cancer mortality rises in linear fashion with increasing glucose concentrations [65,66]. A systemic review of 23 studies demonstrated that patients diagnosed with cancer who have pre-existing diabetes are at a 41% increased risk for long-term, all-cause mortality compared with those without diabetes [63]. Another meta-analysis of 15 studies showed that underlying diabetes was associated with increased odds of postoperative mortality across all cancer types (OR = 1.85 [95% CI: 1.40–2.45]) [67]. Goodwin et al. evaluated insulin levels in 512 nondiabetic women with early-stage breast cancer [64]. The highest levels of fasting insulin were significantly associated with distant recurrence and death, even after adjustment for body mass index (BMI), age, hormonal receptor status, and other known prognostic factors in breast cancer. A recent pooled analysis of 3 adjuvant randomized trials involving 5922 patients with stage II and III colon cancer showed that diabetes was associated with 21% increased risk of cancer relapse and 29% increased risk of mortality [68].
The National Health and Nutrition Examination Survey (NHANES II) Mortality Study found that people with diabetes had an elevated risk of dying of infections [69]. In addition, there is evidence that patients with hyperglycemia have a significantly higher in-hospital mortality rate than subjects with normoglycemia [70]. In an adjuvant colon cancer trial, patients with diabetes experienced an elevated incidence of diarrhea, and were more likely to have leukopenia, thrombocytopenia, elevated creatinine, and hypocalcemia [71]. There is also evidence that patients with cancer and underlying diabetes may receive suboptimal care that could compromise their outcomes. For example, a Dutch study showed that diabetic patients with esophageal, colon, breast, and ovarian cancer received less aggressive cancer treatment than those without diabetes [14].
7. Anti-Cancer Therapy & Hyperglycemia
Over the past two decades, treatment landscapes of most solid and hematological malignancies have changed, with the emergence of targeted and immunotherapy. In contrast to conventional cytotoxic agents that have minimal or no direct effect on hyperglycemia, several novel targeted compounds and immunotherapy agents can cause hyperglycemia (Table 1). The rate of hyperglycemia varies with underlying cancer type, comorbid illnesses, concurrent medications, targeted agent use and treatment schedule. Immunotherapies such as PD/PD-L and CTLA-4 inhibitors can reduce the production of insulin from islet cells as in type 1 diabetes mellitus, whereas targeted treatments such as PI3K/mTOR inhibitors can induce insulin resistance similar to that seen in type 2 diabetes mellitus [6,72].

Table 1.
Cancer drugs and their mechanism causing hyperglycemia.
7.1. Immunotherapy
Immune checkpoint inhibitors including PD/PDL-1 and CTLA-4 inhibitors are a major breakthrough in the management of cancer [73]. These drugs activate T-cells and enhance the immune response against malignant cells, but at the same time can cause autoimmune phenomena including autoimmune endocrinopathies such as hypothyroidism, hyperthyroidism, adrenal insufficiency or hypophysitis. Uncommonly, autoimmune diabetes mellitus has also been reported following the use of a combination of CTLA-4 and PD/PD-L1 inhibitors such as ipilimumab and nivolumab, or the PD/PD L1 inhibitors nivolumab or pembrolizumab alone [72].
7.2. Targeted Therapy
Targeted therapy aims to affect signaling pathways or proteins that are aberrant in the malignant cells and inhibit cell proliferation, regulate the cell cycle or induce apoptosis [74]. However, various targeted agents have been associated with a high risk of hyperglycemia. Among these agents, PI3K/mTOR inhibitors are the most likely to cause hyperglycemia.
7.2.1. PI3K/mTOR Inhibition
The PI3K/Akt/mTOR pathway is commonly activated in various solid cancers [75]. PI3K/mTOR pathway inhibition also affects insulin signaling, resulting in insulin resistance.
Mammalian Target of Rapamycin (mTOR) Inhibitors
Everolimus is an orally administered rapamycin analog and mTOR inhibitor that has been approved for the management of advanced breast cancer, renal cell cancer, and pancreatic neuroendocrine tumors. Everolimus can cause hyperglycemia in 10–50% of patients. However, severe hyperglycemia is not common and was only noted in about 10% cases [7]. A meta-analysis of nine randomized clinical trials involving 3879 patients with various solid tumors showed that everolimus was associated with a high risk of all-grade (RR = 2.60, 95% CI: 2.03–3.31) and high-grade (RR = 3.0, 95% CI: 1.72–5.23) hyperglycemia. The incidences of all- and high-grade everolimus-related hyperglycemia were 6.8% (95% CI: 3.4–13.2%) and 2.5% (95% CI: 1.2–4.9%), respectively [76]. Temsirolimus is a potent, highly-specific inhibitor of mTOR that is administered intramuscularly. It has been used in the management of advanced solid malignancies such as renal cell cancer. The incidence of grade 3 or higher hyperglycemia with temsirolimus is about 9% [77].
Phosphatidylinositol 3-Kinase (PI3K) Inhibitors
Alpelisib is a PI3K3CA inhibitor. In the randomized control SOLAR-1 trial, alpelisib has shown efficacy in combination with fulvestrant, an endocrine therapy, in women with advanced hormone receptor-positive breast cancer with a PIK3CA mutation [78]. However, women who received alpelisib had an any-grade hyperglycemia rates of 63.7%, and a grade 3 hyperglycemia rate of 32.7%. In addition, 3.9% of patients who received alpelisib developed grade 4 hyperglycemia compared to 0.3% in the placebo group.
AKT Inhibitors
Ipatasertib is a selective inhibitor of AKT, a frequently activated protein kinase in human cancers. In a phase I dose escalation trial in patients with various solid tumors, hyperglycemia was noted in 13% of patients [79]. Capivasertib is another pan-AKT kinase inhibitor that was evaluated in a phase I trial with or without fulvestrant in women with metastatic breast cancer [80]. The monotherapy was associated with all-grade hyperglycemia in 45% patients and grade 3 hyperglycemia in 30% of patients.
7.2.2. Insulin-like Growth Factor Type 1 Receptor (IGF-1R)
IGF-1R is partially homologous to the insulin receptor and activates the Ras/MAPK/ERK and PI3K/AKT/mTOR pathways [81]. It promotes cell proliferation and resistance to apoptosis [82]. IGF-1R inhibitors have been evaluated in various solid tumors [83,84,85]. IGF-1R inhibitors include both monoclonal antibodies and small molecules. Hyperglycemia is found to be common side effect of IGF-1R inhibitors.
IGF-1R Monoclonal Antibodies
Dalotuzumab (MK-0646) is a humanized IgG1 monoclonal antibody against IGF-1R that does not cross-react with the insulin receptor [86]. In a randomized trial, addition of dalotuzumab to irinotecan and cetuximab in patients with metastatic colorectal cancer did not improve survival and was associated with high rate of grade 3 hyperglycemia compared to the placebo (21.0% vs. 5.2%) [85].
Small Molecule Inhibitors of IGF-IR and the Insulin Receptor
Linsitinib is an oral, small molecule, dual inhibitor of IGF-1R and the insulin receptor that was evaluated in a placebo-controlled phase 3 trial in patients with advanced adrenocortical tumors [87]. Linsitinib did not improve survival compared to the placebo. Overall incidence of grade 3 hyperglycemia with linsitinib was 2%, which was much lower than with the monoclonal antibody.
Other IGF-1R Inhibitors
Ganetespib is a highly potent heat shock protein 90 inhibitor that blocks multiple oncogenic pathways, including IGF-1R, EGFR, vascular endothelial growth factor, c-MET, and human epidermal growth factor receptor 2 (HER2). In a phase I trial involving patients with hepatocellular carcinoma, ganetespib-related hyperglycemia along with lipasemia were the most common grade 3/4 adverse effects and were reported in 21% of patients (overall 64% patients experienced any-grade hyperglycemia) [88]. Yet, in a subsequent phase 3 trial in patients with advanced lung cancer, ganetespib-related hyperglycemia was not reported as an adverse effect [89]. Ceritinib is a potent oral tyrosine kinase inhibitor of ALK and a less potent inhibitor of IGF-1R. In a phase I study, 10% of patients with lung cancer who were treated with a 750 mg dose of ceritinib experienced any grade of hyperglycemia [90].
IGF-1R inhibitors are currently not in use in clinical practice and trials are ongoing with monoclonal antibody and small molecule inhibitors to determine their role in the management of refractory cancer.
7.2.3. Epidermal Growth Factor Receptor (EGFR) Inhibitors
The EGFR family includes HER2/neu (ErbB2), HER3 (ErbB3), and HER4 (ErbB4). Tyrosine kinase EGFR inhibitors are available as the monoclonal antibodies cetuximab and panitumumab, or small molecules such as geftinib, erlotinib, afatninib and osimertinib, which are commonly used in the management of gastrointestinal and EFGR mutant lung cancers, respectively [91,92]. In general, these agents do not cause hyperglycemia, as the EFGR pathway is not directly involved in glucose metabolism. Rociletinib is a third generation EGFR inhibitor that in a phase I/II trial has demonstrated efficacy in patients with EGFR-mutant non-small cell lung cancer with the T790M resistance mutation who progressed on standard anti-EFGR treatment [93]. Unlike other agents, the rate of grade 3 hyperglycemia in patients who received therapeutic doses of rociletinib was 22%, and it was the most common grade 3 adverse event. The rate of all-grade hyperglycemia was dose dependent (35% of the patients treated with a dose of 500 mg vs. 67% treated with a dose of 1000 mg).
7.2.4. BCR-ABL Multi-Targeted Tyrosine-Kinase Inhibitors
Nilotinib, dasatinib, and ponatinib are next-generation multi-targeted tyrosine-kinase inhibitors that have been used in the management of chronic myelogenous leukemia (CML) and Philadelphia chromosome–positive acute lymphoblastic leukemia and proven to be more effective than imatinib [94]. They are associated with a high risk of hyperglycemia. For example, in a phase 3 trial involving 846 patients with CML, the rates of all grade and grade 3 or 4 hyperglycemia were 36% and 6%, respectively, with 300 mg nilotinib, and 41% and 4%,respectively, with 400 mg nilotinib compared with 20% and 0% respectively, with imatinib [95]. Hyperglycemia is thought to be related to the development of tissue insulin resistance and compensatory hyperinsulinemia [96].
7.3. Hormone Therapy
7.3.1. Anti-Estrogen Therapy
Case-control and case-cohort studies have shown that postmenopausal women with breast cancer treated with anti-estrogen therapy have a high incidence of insulin resistance and diabetes [57,97,98]. For example, a case-cohort study involving breast cancer survivors showed that adjuvant tamoxifen was associated with a 2.2 fold risk of diabetes whereas aromatase inhibitors were associated with a 4.2 fold risk of diabetes [98].
7.3.2. Androgen Deprivation Therapy
Androgen deprivation therapy with a gonadotropin-releasing hormone analog or antagonist with or without an oral antiandrogen is used commonly in the management of prostate cancer. The use of these agents has been linked increasingly to insulin resistance metabolic syndrome and an increased incidence of diabetes [57,99,100].
7.3.3. Somatostatin Analogs
Octreotide and lanreotide are somatostatin analogs that have shown efficacy in neuroendocrine tumors including secretory insulinomas, VIPomas, glucagonomas and other non-functional neuroendocrine tumors [101,102,103]. All-grade hyperglycemia has been noted in 2% to 27% cases.
7.4. Corticosteroids
Corticosteroids are commonly used in cancer patients as a part of treatment regimen for lymphomas, leukemias, myeloma, and solid tumors such as prostate cancers, as adjunctive agents for nausea and vomiting, supportive measures to improve appetite, and to reduce edema in patients with metastasis to the brain and spinal cord [57,104,105,106]. Corticosteroids are known to induce hyperglycemia [107,108]. In general, patients treated with glucocorticoids have an odds ratio for new-onset diabetes mellitus of about 1.5 to 2.5 [5]. Reduced insulin sensitivity with increased glucose production and inhibition of the production and secretion of insulin by pancreatic β-cells are considered to be the key mechanism of glucose intolerance [5]. For cancer patients with known diabetes, the use of corticosteroids requires close monitoring of blood glucose concentrations and appropriate intervention to prevent complications related to hyperglycemia. Patients on oral hypoglycemics may require short-term insulin during the period of therapy. Patients using insulin should adjust dosages based on frequent monitoring of serum glucose concentrations.
7.5. Miscellaneous Compounds
Asparaginase is used commonly in the management of acute lymphoblastic leukemia. Hyperglycemia is common with the use of asparaginase and in pediatric patients with cancer, it varies from 2.5% to 23% [109]. Diazoxide is a potassium channel activator and blocks insulin secretion by opening potassium channels of β cells, resulting in hyperglycemia. It has been used in the management of insulinoma [110].
8. Factors That Influence the Choice of Cancer Therapy in Patients with Diabetes
In addition to poorly controlled blood glucose, the choice of anticancer therapy in patients with diabetes could be influenced by underlying chronic renal insufficiency, cardiovascular disease, peripheral neuropathy, and chronic infection as described below. These factors limit the use of certain drugs or their dosage, which can lead to lower response rates, inferior outcomes, and shorter survival. Furthermore, the presence of diabetic-related comorbid illnesses also affects the eligibility to participate in clinical trials with novel agents.
8.1. Renal Disease
Kidney impairment is a relatively common complication of diabetes [111]. Diabetic patients with kidney impairment are usually not appropriate candidates for nephrotoxic agents. Alternative drugs or reduction in the dosage are required for drugs cleared by the kidney or for drugs metabolized in the liver and later excreted by the kidney. For example, patients with diabetes and germ cell tumors who have kidney impairment will require adjustment in cisplatin dosage [112]. Likewise, underlying kidney impairment increases the risk of toxicity related to capecitabine, an antimetabolite that is commonly used in gastrointestinal cancers [113].
8.2. Cardiovascular Disease
A wide range of chemotherapy agents have been associated with cardiotoxicity, including arrhythmias, myocardial necrosis causing a dilated cardiomyopathy, and vasospasm or vasoocclusion resulting in angina or myocardial infarction [114]. Furthermore, targeted therapy, endocrine therapy and radiation increase the risk of cardiovascular complications. Many patients with diabetes have pre-existing heart disease or are at high risk of development of cardiac toxicity that can influence the choice of appropriate treatment in such patients [111]. Adjuvant trastuzumab in women with HER2-positive breast cancer has been associated with significant reduction in recurrent breast cancer and mortality, however it is contraindicated in individuals with left ventricle dysfunction as it increases the risk of symptomatic cardiac dysfunction [115].
8.3. Neuropathy
Peripheral neuropathy is a common complication of diabetes and may affect more than 50% of patients [116]. Peripheral neuropathies are the dose-limiting side effects of several chemotherapeutic agents, such as platinum compounds (cisplatin, carboplatin, oxaliplatin), vinca alkaloids (vincristine, vinblastin, vinorelbine), taxanes (docetaxel, paclitaxel), bortezomib and thalidomide [117]. The presence of diabetic neuropathy limits the use of such agents. Adjuvant use of oxaliplatin-based therapy in patients with stage 3 colon cancer has been associated with a reduced rate of recurrence and a better overall survival [118]. Hence, omission of oxaliplatin in diabetic patients with node-positive colon cancer and neuropathy could increase their risk of recurrent cancer.
9. Screening & Diagnosis of Diabetes in Cancer Patients
Up to a third of people with diabetes are undiagnosed. The stress of the illness and treatment may unmask underlying diabetes in patients with cancer. The diagnosis of diabetes is per criteria established by the American Association of Diabetes and the World Health Organization [119]: In an asymptomatic individual, diabetes is diagnosed if they have any of the following criteria: fasting blood glucose ≥7.0 mmol/L (126 mg/dL) or a 2-hour blood glucose level of ≥11.1 mmol/L (200 mg/dL) following a 75 g oral glucose tolerance test or a hemoglobin A1C (HbAIC) value ≥ 6.5% (48 mmol/mol). In symptomatic individuals, diabetes is diagnosed with a random blood glucose level of ≥11.1 mmol/L (200 mg/dL).
Screening of patients with cancer with fasting or random blood glucose and HbA1c is important before embarking on systemic therapy. This is especially important in patients who have risk factors for diabetes such as a high body mass index (BMI), physical inactivity, a family history of diabetes, and history of gestational diabetes, or those who will be treated with targeted agents that are associated with hyperglycemia. Patients with elevated fasting glucose concentrations should have formal testing for diabetes and appropriate treatment. Patients with cancer who are started on targeted therapy or steroids that may induce hyperglycemia and diabetes should have education on self-monitoring of glucose and a baseline glucose level. Given the fact that steroid-related hyperglycemia and diabetes are mostly diagnosed during the postprandial state postprandial blood glucose with or without HbA1c should be performed as a screening test in patients taking steroid [120].
10. Management of Diabetes in Cancer Patients
10.1. Multidisciplinary Management
Few prospective studies are available on the management of cancer patients with diabetes. Multidisciplinary management of diabetes in patients requiring cancer treatment, involving a diabetes specialist, educator, dietician, pharmacist, and psychosocial support professional, in collaboration with the cancer care team, is vital in order to avoid diabetes-related complications and thereby inferior outcomes. Diabetic patients on anticancer therapy require management of hyperglycemia, fluids and electrolytes, along with management of hypertension, cardiovascular complications, infection, and autonomic neuropathy of the gastrointestinal tract. Patient education and self-management training, interdisciplinary team counseling, home blood glucose monitoring, monitoring side effects and patient’s adherence to prescribed treatment, and ongoing education are important components of management of diabetes in cancer patients. Clinicians must consider the cardiac, renal, and neurological complications that are commonly associated with diabetes.
10.2. Management of Hyperglycemia
Hyperglycemia in cancer patients exacerbates dehydration that may result from diarrhea and decreased oral intake because of anorexia, nausea, and mucositis, which are common in cancer patients. It can predispose to acidosis and worsen the side effects of cancer therapy [121,122]. Patients with cancer and diabetes require close monitoring of blood glucose during their cancer treatment, and health outcomes could potentially be improved by ensuring optimal blood glucose during treatment [123,124]. Patients on oral hypoglycemic agents may require a short course of insulin during cancer therapy, whereas patients using insulin may need further dose adjustment. Basal insulin inhibits hepatic glucose production overnight and between meals, and prandial or mealtime insulin promotes glucose uptake into muscles following a meal. Treatment-related complications and reduced oral intake, especially in patients with advanced cancer, could increase the risk of hypoglycemia from insulin and oral hypoglycemic agents; hence, less aggressive measures are warranted in such patients.
Diabetic ketoacidosis is a life-threatening complication of diabetes that is associated with hyperglycemia, ketonemia, and acidosis. Some patients with cancer may present with diabetic ketoacidosis as the initial manifestation of underlying diabetes mellitus [125,126]. These patients require rapid correction of hypovolemia and electrolyte abnormalities along with low-dose insulin infusion. In most cases, cancer treatment can be resumed after resolution of ketoacidosis as along as an optimal blood glucose level can be achieved.
Management of targeted treatment-related type 2 diabetes mellitus includes diet, exercise, oral hypoglycemic agents with or without insulin (Table 2). Metformin does not cause hypoglycemia and is the treatment of choice for sustained grade 1, grade 2, and asymptomatic grade 3 hyperglycemia. However, it is not recommended in patients who are at risk of lactic acidosis, such as those with significant impairment of liver or kidney function. Furthermore, metformin can cause gastrointestinal side effects and its use may be limited in patients with significant gastrointestinal side effects of cancer therapy. Metformin 500 mg twice a day or Metformin XR at a dose of 500 mg may be considered for mild increases in fasting plasma glucose, and can be titrated to a maximum dose of 2,000 mg daily over a period of several weeks. The treatment goals include a fasting plasma glucose level of < 8.9 mm/L (160 mg/dL), a random plasma glucose level of < 11.1 mm/L (200 mg/dL), and HbA1c ≤ 8% for the prevention of hyperglycemia-related symptoms and complications including infection, osmotic diuresis, and hypercoagulability, as well as hypoglycemia [123]. If fasting glucose level is higher than 14 mm/l (250 mg/dl), cancer treatment interruption can be considered until blood glucose is better controlled (Figure 1). If hyperglycemia is not optimally controlled at the maximum tolerated dose of metformin, another oral agent such as dipeptidyl-4 inhibitors, glitazones, or a sulfonylurea may be considered before commencement of insulin. Sodium glucose transporter-2 (SGLT-2) inhibitors may also be used, however patients on SGLT-2 inhibitors should be monitored closely for urinary tract infection and candiadiasis. In addition, there are reports of euglycemic diabetic ketoacidosis related to SGLT-2 inhibitors [127]. Glucagon like peptide (GLP)-1 agonists that are available in oral and injection forms are another option, however their gastrointestinal side effects and weight loss can be troublesome in cancer patients. If hyperglycemia is not controlled with glucose lowering agents, insulin is the preferred option [123,124]. Rapid-acting insulin prior to meals facilitates flexible meal times. Healthy diet, physical activity and optimal body weight should be encouraged for cancer patients with diabetes.
Table 2.
List of current drugs that are used in the management of diabetes mellitus.
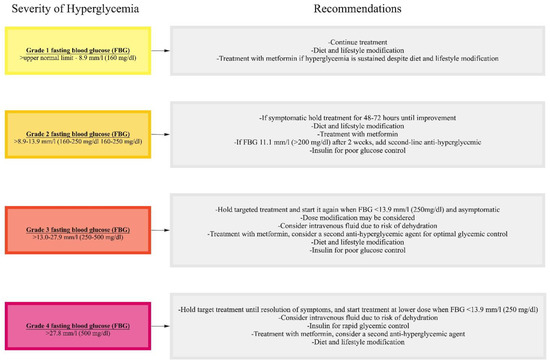
Figure 1.
Management of targeted treatment-related hyperglycemia.
For most patients with hyperglycemia related to checkpoint inhibitor treatment, immunotherapy can be continued along with the management of diabetes. However, for patients who develop diabetic ketoacidosis secondary to immunotherapy, it will be an individual decision whether or not to continue immune checkpoint inhibitor treatment based on the severity of adverse effects, disease burden and overall health of the patient. Regardless, immunotherapy should be paused until diabetic ketoacidosis is resolved.
10.3. Management of Fluid and Electrolyte Balance
Factors that influence the fluid intake or volume loss in diabetic patients are severe mucositis from chemotherapy or radiation, nausea and vomiting from highly emetogenic chemotherapy such as a platinum compounds, and diarrhea caused by agents such as 5-FU, irinotecan and targeted therapies. Hyperglycemia in diabetic patients is further exacerbated by dehydration resulting from treatment-related side effects. Optimal glycemic control along with periodic intravenous hydration and judicious use of anti-emetics and anti-diarrheal agents can prevent complications from dehydration including diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome [128,129].
10.4. Management of Hypertension
Many targeted therapies such as anti-vascular endothelial growth factor (VEGF) agents including bevacizumab, sunitinib, and sorafenib can cause hypertension [130]. Uncontrolled hypertension in a diabetic patient may aggravate or unmask renal insufficiency. Close monitoring and management of blood pressure is therefore important in diabetic patients who are on targeted therapy. Furthermore, surveillance and early intervention of hypertension is especially important in cancer survivors with diabetes to reduce morbidity and mortality and lower the risk of associated target organ damage.
10.5. Management of Cardiovascular Complications
Heart disease, especially coronary heart disease, is a major cause of morbidity and mortality in patients with diabetes mellitus [131,132,133,134]. Compared with patients without diabetes, patients with diabetes more often have multi-vessel disease and episodes of silent ischemia [111,131]. Patients with diabetes may also have a higher risk of other complications, including arrhythmias, cardiogenic shock, heart failure, renal failure, and recurrent myocardial infarction [132,133,134]. Patients with diabetes with a history of coronary artery disease and congestive heart failure on anticancer therapy require close follow-up. Dyspnea with no obvious cause in a patient with cancer and complicated diabetes should be considered an angina equivalent, and workup for underlying undiagnosed coronary artery disease including electrocardiogram (ECG), cardiac enzyme tests, and stress tests should be performed. It is imperative to pay special attention to preventive strategies for cancer survivors with diabetes to reduce future risk of cardiovascular complications, including weight management, regular exercise, treatment of hyperlipidemia, and optimal glucose control [134].
10.6. Management of Infection
Patients with diabetes are at higher risk of infection from various pathogens involving various organ sites than the general population (Table 3). Soft tissue, skin, and mucosal infections, including superficial fungal infections and urinary tract infections, are common. In addition, patients with diabetes are at high risk of serious infection such as pyomyositis, emphysematous cholecystitis, malignant external otitis, and necrotizing fasciitis. Hyperglycemia is associated with dysfunctional immune responses, impaired circulation, sensory peripheral and autonomic neuropathy, and skin and mucosal colonization with pathogens such as Staphylococcus aureus and Candida species predispose patients with diabetes to infection [135,136]. Anticancer therapy further increases infection risk and complications by causing bone marrow suppression, poor wound healing, and breaks in the mucosa. There are several factors that predispose patients with diabetes to Candida spp. colonization and infection, including higher salivary glucose levels, reduced salivary flow, microvascular degeneration, epithelial cell surface adhesion, and impaired candidacidal activity of neutrophils, all of which are further aggravated by the immunosuppressive effects of cancer treatment [137]. Candida spp. infection has also been associated with an increased risk of cancer including oral cancer [138].
Table 3.
List of common infections and their etiologies in patients with diabetes.
Patient and family education, prophylactic use of antibiotics, growth factors, appropriate nutrition and physical activity may reduce the risk of serious infection in diabetic patients [139,140]. A diabetic patient with febrile neutropenia should be treated with a broad-spectrum antibiotic such as cefepime, carbapenem, or piperacillin-tazobactam. The addition of vancomycin can be considered in the presence of hypotension, mucositis, skin or catheter site infection, history of MRSA colonization, recent quinolone prophylaxis and overall clinical deterioration. An antifungal agent should be considered if neutropenia is expected to persist for more than 5 to 7 days and the patient is persistently febrile without an obvious source of infection.
10.7. Management of Diabetic Autonomic Neuropathy of the Gastrointestinal Tract
Diabetic autonomic neuropathy may involve the cardiovascular, genitourinary, and the neuroendocrine system as well as the upper and lower gastrointestinal tract [141,142]. Patients with diabetic gastroparesis can experience significant nausea and vomiting during anticancer therapy. Primary treatment of gastroparesis includes dietary changes (low fat diet and frequent small meals) and administration of antiemetic and prokinetic agents. Diarrhea and rarely steatorrhea can occur with diabetic enteropathy and can be exacerbated during cancer treatment. Fluid electrolyte balance, optimizing glycemic control, treating underlying infection, and anti-diarrheal agents are the corner stones of treatment.
11. Survivorship Care
As expected, diabetes is more frequent in cancer survivors compared to the general population [143]. Furthermore, cancer survivors with diabetes have a higher rate of comorbid illnesses compared with survivors with no history of diabetes [144]. As mentioned above cancer survivors with diabetes are at high risk of both acute and chronic toxicities from cancer treatment. Chemotherapy and endocrine therapy especially increase the risk of cardiovascular disease including heart disease, hypertension, kidney disease, and stroke, as well as osteoporosis [132,133,134,145]. In addition, cancer survivors with comorbid illnesses including diabetes, experience overall poorer health and a higher rate of disability [143,146]. Therefore, ongoing surveillance and screening for vascular comorbid illnesses related to diabetes and early intervention are key for cancer survivors with diabetes. Furthermore, continuing emphasis and behavioral intervention on life style factors and promotion of regular aerobic physical activity, weight management, a healthy diet, stress management, reducing alcohol consumption, smoking cessation and self-management of diabetes are important to reduce future complications [147].
12. Future Directions
Although the association between diabetes and carcinogenesis has been suggested by several studies, the underlying mechanism is not well known. Oxidative stress may be the place where metabolic and oncogenic processes cross paths and may result in oncogenesis [148,149]. Treatment of diabetes could further compound this, as certain antidiabetic drugs may increase the risk of oncogenesis while others may decrease the risk [150]. However, a definite causal relationship between antidiabetic medication and cancer has not yet been established. Multiple factors potentially contribute to the progression of cancer in patients with obesity and type 2 diabetes, including hyperinsulinemia and insulin-like growth factor I, hyperglycemia, dyslipidemia, adipokines and cytokines, and the gut microbiome [151]. A better understanding of the underlying mechanism between diabetes, and cancer risk is needed, along with large prospective, biomarker-driven population-based studies to explore the causal relationship between the duration and severity of diabetes and different cancers. Conclusive evidence may help to implement primary prevention, early detection/cancer screening, and effective therapeutic measures. High-quality prospective studies using innovative tools are needed to determine whether more rigorous management of insulin resistance and hyperglycemia in patients with cancer improves their outcomes. Moreover, establishment of a national or an international database of patients with cancer and diabetes, identification of personal, tumor-related, and contextual factors that are associated with inferior outcomes, and an increased focus on health services and the implementation of research are important for better outcomes.
13. Conclusions
Diabetes and hyperglycemia are associated with an elevated risk of developing of many cancers. Hyperglycemic and diabetic patients experience higher mortality and recurrence rates after diagnosis with, and treatment for, cancer. Presence of renal insufficiency, neuropathy, cardiac dysfunction, and chronic infection in diabetic patients with cancer limit the use of certain drugs or their dosage, which can lead to lower response rates and shorter survival. Clinicians must consider the cardiac, renal, and neurologic complications commonly associated with diabetes in patients undergoing anticancer therapy. Patients on targeted therapy can be managed with appropriate glucose lowering agents without the need of discontinuation of cancer treatment in most cases. In addition, promotion of physical activity, healthy diet and optimal body weight are especially important in diabetic cancer survivors. A patient-centered approach by a multidisciplinary team comprised of various health care professionals and development of clinical pathways are vital to avoid diabetes-related complications and thereby inferior outcomes.
Author Contributions
Conceptualization, R.K.S., S.A., D.L., S.Y.; methodology, S.A., R.K.S.; software, not applicable; validation, not applicable; formal analysis, not applicable; investigation, R.K.S., S.A., D.L., S.Y.; resources, R.K.S., S.A.; data curation, not applicable; writing—original draft preparation, R.K.S., S.A., D.L., S.Y.; writing—review and editing, R.K.S., S.A., D.L., S.Y.; visualization, R.K.S., S.A.; supervision, S.A.; project administration, S.A., R.K.S.; funding acquisition, not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors would like to thank to Rafay Ahmed for his assistance in the development of Figure 1.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Centers for Disease Control and Prevention. About “NIOSH”. Available online: https://www.cdc.gov/niosh/about/default.html (accessed on 21 September 2020).
- Liu, J.; Ren, Z.H.; Qiang, H.; Wu, J.; Shen, M.; Zhang, L.; Lyu, J. Trends in the incidence of diabetes mellitus: Results from the Global Burden of Disease Study 2017 and implications for diabetes mellitus prevention. BMC Public Health 2020, 20, 1415. [Google Scholar] [CrossRef]
- Ling, S.; Brown, K.; Miksza, J.K.; Howells, L.; Morrison, A.; Issa, E.; Yates, T.; Khunti, K.; Davies, M.J.; Zaccardi, F. Association of Type 2 Diabetes with Cancer: A Meta-analysis with Bias Analysis for Unmeasured Confounding in 151 Cohorts Comprising 32 Million People. Diabetes Care 2020, 43, 2313–2322. [Google Scholar] [CrossRef] [PubMed]
- Bjornsdottir, H.H.; Rawshani, A.; Rawshani, A.; Franzén, S.; Svensson, A.-M.; Sattar, N.; Gudbjörnsdottir, S. A national observation study of cancer incidence and mortality risks in type 2 diabetes compared to the background population over time. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Clore, J.N.; Thurby-Hay, L. Glucocorticoid-Induced Hyperglycemia. Endocr. Pract. 2009, 15, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.; Vudattu, N.; Sznol, M.; Gettinger, S.; Kluger, H.; Lupsa, B.; Herold, K.C. Precipitation of Autoimmune Diabetes with Anti-PD-1 Immunotherapy. Diabetes Care 2015, 38, e55–e57. [Google Scholar] [PubMed]
- Morviducci, L.; Rota, F.; Rizza, L.; Di Giacinto, P.; Ramponi, S.; Nardone, M.; Tubili, C.; Lenzi, A.; Zuppi, P.; Baldelli, R. Everolimus is a new anti-cancer molecule: Metabolic side effects as lipid disorders and hyperglycemia. Diabetes Res. Clin. Pract. 2018, 143, 428–431. [Google Scholar] [CrossRef]
- Coughlin, S.S.; E Calle, E.; Teras, L.R.; Petrelli, J.; Thun, M.J. Diabetes Mellitus as a Predictor of Cancer Mortality in a Large Cohort of US Adults. Am. J. Epidemiol. 2004, 159, 1160–1167. [Google Scholar] [CrossRef]
- Saydah, S.H.; Loria, C.M.; Eberhardt, M.S.; Brancati, F.L. Abnormal glucose tolerance and the risk of cancer death in the United States. Am. J. Epidemiol. 2003, 157, 1092–1100. [Google Scholar] [CrossRef]
- Liu, X.; Ji, J.; Sundquist, K.; Sundquist, J.; Hemminki, K. The impact of type 2 diabetes mellitus on cancer-specific survival: A follow-up study in Sweden. Cancer 2012, 118, 1353–1361. [Google Scholar] [CrossRef]
- Hansen, L.J.; Olivarius, N.D.F.; Siersma, V. 16-year excess all-cause mortality of newly diagnosed type 2 diabetic patients: A cohort study. BMC Public Health 2009, 9, 400. [Google Scholar] [CrossRef]
- Jansson, S.P.; Andersson, D.K.; Svardsudd, K. Mortality Trends in Subjects with and without Diabetes during 33 Years of Follow-up. Diabetes Care 2010, 33, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Salehidoost, R.; Mansouri, A.; Amini, M.; Yamini, S.A.; Aminorroaya, A. Diabetes and all-cause mortality, a 18-year follow-up study. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- van de Poll-Franse, L.V.; Houterman, S.; Janssen-Heijnen, M.L.; Dercksen, M.W.; Coebergh, J.W.; Haak, H.R. Less aggressive treatment and worse overall survival in cancer patients with diabetes: A large population based analysis. Int. J. Cancer 2007, 120, 1986–1992. [Google Scholar] [CrossRef]
- Skyler, J.S.; Bakris, G.L.; Bonifacio, E.; Darsow, T.; Eckel, R.H.; Groop, L.; Groop, P.-H.; Handelsman, Y.; Insel, R.A.; Mathieu, C.; et al. Differentiation of Diabetes by Pathophysiology, Natural History, and Prognosis. Diabetes 2016, 66, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Ariaans, G.; de Jong, S.; Gietema, J.; Lefrandt, J.; de Vries, E.; Jalving, M. Cancer-drug induced insulin resistance: Innocent bystander or unusual suspect. Cancer Treat. Rev. 2015, 41, 376–384. [Google Scholar] [CrossRef]
- Gallo, M.; Muscogiuri, G.; Felicetti, F.; Faggiano, A.; Trimarchi, F.; Arvat, E.; Vigneri, R.; Colao, A. Adverse glycaemic effects of cancer therapy: Indications for a rational approach to cancer patients with diabetes. Metabolism 2018, 78, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Silvestris, N.; Argentiero, A.; Beretta, G.D.; Di Bartolo, P.; Montagnani, M.; Danesi, R.; Ferrari, P.; D’Oronzo, S.; Gori, S.; Russo, A.; et al. Management of metabolic adverse events of targeted therapies and immune checkpoint inhibitors in cancer patients: An Associazione Italiana Oncologia Medica (AIOM)/Associazione Medici Diabetologi (AMD)/Società Italiana Farmacologia (SIF) multidisciplinary consensus position paper. Crit. Rev. Oncol. Hematol. 2020, 154, 103066. [Google Scholar]
- A Hart, P.; Bellin, M.D.; Andersen, D.K.; Bradley, D.; Cruz-Monserrate, Z.; E Forsmark, C.; O Goodarzi, M.; Habtezion, A.; Korc, M.; Kudva, Y.C.; et al. Type 3c (pancreatogenic) diabetes mellitus secondary to chronic pancreatitis and pancreatic cancer. Lancet Gastroenterol. Hepatol. 2016, 1, 226–237. [Google Scholar] [CrossRef]
- Shi, Y.; Hu, F.B. The global implications of diabetes and cancer. Lancet 2014, 383, 1947–1948. [Google Scholar] [CrossRef]
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P.F. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- White, M.C.; Holman, D.M.; Boehm, J.E.; Peipins, L.A.; Grossman, M.; Henley, S.J. Age and cancer risk: A potentially modifiable relationship. Am. J. Prev. Med. 2014, 46 (Suppl. 1), S7–S15. [Google Scholar] [CrossRef]
- Kirkman, M.S.; Briscoe, V.J.; Clark, N.; Florez, H.; Haas, L.B.; Halter, J.B.; Huang, E.S.; Korytkowski, M.T.; Munshi, M.N.; Odegard, P.S.; et al. Diabetes in Older Adults. Diabetes Care 2012, 35, 2650–2664. [Google Scholar] [CrossRef]
- Chari, S.T.; Leibson, C.L.; Rabe, K.G.; Ransom, J.; de Andrade, M.; Petersen, G.M. Probability of Pancreatic Cancer Following Diabetes: A Population-Based Study. Gastroenterology 2005, 129, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.; Kim, K.-W. Diabetes and Cancer: Cancer Should Be Screened in Routine Diabetes Assessment. Diabetes Metab. J. 2019, 43, 733. [Google Scholar] [CrossRef] [PubMed]
- Sciacca, L.; Vigneri, R.; Tumminia, A.; Frasca, F.; Squatrito, S.; Frittitta, L. Clinical and molecular mechanisms favoring cancer initiation and progression in diabetic patients. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 808–815. [Google Scholar] [CrossRef]
- Hirsch, I.B.; Juneja, R.; Beals, J.M.; Antalis, C.J.; E Wright, E. The Evolution of Insulin and How it Informs Therapy and Treatment Choices. Endocr. Rev. 2020, 41, 733–755. [Google Scholar] [CrossRef]
- Giovannucci, E.L.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and Cancer: A consensus report. Diabetes Care 2010, 33, 1674–1685. [Google Scholar] [CrossRef]
- Wang, M.; Yang, Y.; Liao, Z. Diabetes and cancer: Epidemiological and biological links. World J. Diabetes 2020, 11, 227–238. [Google Scholar] [CrossRef]
- Duan, W.; Shen, X.; Lei, J.; Xu, Q.; Yu, Y.; Li, R.; Wu, E.; Ma, Q. Hyperglycemia, a Neglected Factor during Cancer Progression. BioMed Res. Int. 2014, 2014, 461917. [Google Scholar] [CrossRef]
- Masur, K.; Vetter, C.; Hinz, A.; Tomas, N.; Henrich, H.; Niggemann, B.; Zänker, K.S. Diabetogenic glucose and insulin concentrations modulate transcriptom and protein levels involved in tumour cell migration, adhesion and proliferation. Br. J. Cancer 2010, 104, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, F.M.; de Sousa, F.R.; Barbosa, A.L.; Martins, S.C.; Araújo, R.L.; Soares, R.; Abreu, C. Metabolic syndrome and risk of cancer: Which link? Metabolism 2015, 64, 182–189. [Google Scholar] [CrossRef]
- Lee, K.A.; Luong, M.K.; Shaw, H.; Nathan, P.; Bataille, V.; Spector, T.D. The gut microbiome: What the oncologist ought to know. Br. J. Cancer 2021, 125, 1197–1209. [Google Scholar] [CrossRef]
- Gurung, M.; Li, Z.; You, H.; Rodrigues, R.; Jump, D.B.; Morgun, A.; Shulzhenko, N. Role of gut microbiota in type 2 diabetes pathophysiology. EBioMedicine 2020, 51, 102590. [Google Scholar] [CrossRef] [PubMed]
- Vivarelli, S.; Salemi, R.; Candido, S.; Falzone, L.; Santagati, M.; Stefani, S.; Torino, F.; Banna, G.L.; Tonini, G.; Libra, M. Gut Microbiota and Cancer: From Pathogenesis to Therapy. Cancers 2019, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, N.; Kounatidis, D.; Christodoulatos, G.; Panagopoulos, F.; Karampela, I.; Dalamaga, M. Mycobiome and Cancer: What Is the Evidence? Cancers 2021, 13, 3149. [Google Scholar] [CrossRef]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.-M.; Kennedy, S.; et al. Richness of human gut microbiome correlates with metabolic markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Holmes, E.; Kinross, J.; Burcelin, R.; Gibson, G.; Jia, W.; Pettersson, S. Host-Gut Microbiota Metabolic Interactions. Science 2012, 336, 1262–1267. [Google Scholar] [CrossRef]
- Karpiński, T.M. Role of Oral Microbiota in Cancer Development. Microorganisms 2019, 7, 20. [Google Scholar] [CrossRef]
- Chung, L.-M.; Liang, J.-A.; Lin, C.-L.; Sun, L.-M.; Kao, C.-H. Cancer risk in patients with candidiasis: A nationwide population-based cohort study. Oncotarget 2017, 8, 63562–63573. [Google Scholar] [CrossRef]
- Ramirez-Garcia, A.; Rementeria, A.; Aguirre-Urizar, J.M.; Moragues, M.D.; Antoran, A.; Pellon, A.; Abad-Diaz-de-Cerio, A.; Hernando, F.L. Candida albicans and cancer: Can this yeast induce cancer development or progression? Crit. Rev. Microbiol. 2016, 42, 181–193. [Google Scholar]
- Carstensen, B.; Read, S.H.; Friis, S.; Sund, R.; Keskimäki, I.; Svensson, A.-M.; Ljung, R.; Wild, S.H.; Kerssens, J.J.; Harding, J.L.; et al. Diabetes and Cancer Research Consortium. Cancer incidence in persons with type 1 diabetes: A five-country study of 9000 cancers in type 1 diabetic individuals. Diabetologia 2016, 59, 980–988. [Google Scholar] [CrossRef]
- Harding, J.L.; Shaw, J.E.; Peeters, A.; Cartensen, B.; Magliano, D.J. Cancer Risk among People with Type 1 and Type 2 Diabetes: Disentangling True Associations, Detection Bias, and Reverse Causation. Diabetes Care 2014, 38, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Stocks, T.; Rapp, K.; Bjørge, T.; Stocks, T.; Rapp, K.; Bjørge, T.; Manjer, J.; Ulmer, H.; Selmer, R.; Lukanova, A.; et al. Blood glucose and risk of incident and fatal cancer in the metabolic syndrome and cancer project (Me-Can): Analysis of six prospective cohorts. PLoS Med. 2009, 6, 100020. [Google Scholar] [CrossRef]
- Cannata, D.; Fierz, Y.; Vijayakumar, A.; Le Roith, D. Type 2 diabetes and cancer: What is the connection? Mt. Sinai J. Med. 2010, 77, 197–213. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhang, X.; Ma, Y.; Yuan, C.; Wang, M.; Wu, K.; Tabung, F.K.; Tobias, D.; Hu, F.B.; Giovannucci, E.; et al. Incident Type 2 Diabetes Duration and Cancer Risk: A Prospective Study in Two US Cohorts. J. Natl. Cancer Inst. 2021, 113, 381–389. [Google Scholar] [CrossRef] [PubMed]
- A Davila, J.; O Morgan, R.; Shaib, Y.; A McGlynn, K.; El-Serag, H.B. Diabetes increases the risk of hepatocellular carcinoma in the United States: A population based case control study. Gut 2005, 54, 533–539. [Google Scholar] [CrossRef]
- Boyle, P.; Boniol, M.; Koechlin, A.; Robertson, C.; Valentini, F.; Coppens, K.; Fairley, L.-L.; Zheng, T.; Zhang, Y.; Pasterk, M.; et al. Diabetes and breast cancer risk: A meta-analysis. Br. J. Cancer 2012, 107, 1608–1617. [Google Scholar] [CrossRef]
- Ben, Q.; Xu, M.; Ning, X.; Liu, J.; Hong, S.; Huang, W.; Zhang, H.; Li, Z. Diabetes mellitus and risk of pancreatic cancer: A meta-analysis of cohort studies. Eur. J. Cancer 2011, 47, 1928–1937. [Google Scholar] [CrossRef]
- Wang, F.; Gupta, S.; Holly, E.A. Diabetes Mellitus and Pancreatic Cancer in a Population-Based Case-Control Study in the San Francisco Bay Area, California. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1458–1463. [Google Scholar] [CrossRef]
- Tsilidis, K.K.; Kasimis, J.C.; Lopez, D.S.; E Ntzani, E.; Ioannidis, J.P.A. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies. BMJ 2015, 350, g7607. [Google Scholar] [CrossRef]
- Currie, C.J.; Johnson, J. The safety profile of exogenous insulin in people with type 2 diabetes: Justification for concern. Diabetes Obes. Metab. 2011, 14, 1–4. [Google Scholar] [CrossRef]
- Smith, U.; Gale, E.A.M. Does diabetes therapy influence the risk of cancer? Diabetology 2009, 52, 1699–1708. [Google Scholar] [CrossRef]
- ORIGIN Trial Investigators; Gerstein, H.C.; Bosch, J.; Dagenais, G.R.; Díaz, R.; Jung, H.; Maggioni, A.P.; Pogue, J.; Probstfield, J.; Ramachandran, A.; et al. Basal insulin and cardiovascular and other outcomes in dysglycemia. N. Engl. J. Med. 2012, 367, 319–328. [Google Scholar]
- Home, P.; DeFronzo, R.A.; Eldor, R.; Abdul-Ghani, M. Insulin Therapy and Cancer. Diabetes Care 2013, 36, S240–S244. [Google Scholar] [CrossRef]
- Shlomai, G.; Neel, B.; Leroith, D.; Gallagher, E.J. Type 2 Diabetes Mellitus and Cancer: The Role of Pharmacotherapy. J. Clin. Oncol. 2016, 34, 4261–4269. [Google Scholar] [CrossRef] [PubMed]
- Boniol, M.; Franchi, M.; Bota, M.; Leclercq, A.; Guillaume, J.; van Damme, N.; Corrao, G.; Autier, P.; Boyle, P. Incretin-Based Therapies and the Short-term Risk of Pancreatic Cancer: Results From Two Retrospective Cohort Studies. Diabetes Care 2017, 41, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Forsmark, C.E. Incretins, Diabetes, Pancreatitis and Pancreatic Cancer: What the GI specialist needs to know. Pancreatology 2016, 16, 10–13. [Google Scholar] [CrossRef]
- Wang, H.; Liu, Y.; Tianpei, H.; Yang, J.; Lu, R.; Zhan, S.; Haukka, J.; Hong, T. Incretin-based therapies and risk of pancreatic cancer in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Diabetes Obes. Metab. 2018, 20, 910–920. [Google Scholar] [CrossRef]
- Morales, D.R.; Morris, A.D. Metformin in Cancer Treatment and Prevention. Annu. Rev. Med. 2015, 66, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Rizos, C.V.; Elisaf, M.S. Metformin and cancer. Eur. J. Pharmacol. 2013, 705, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Barone, B.B.; Yeh, H.C.; Snyder, C.F.; Peairs, K.S.; Stein, K.B.; Derr, R.L.; Wolff, A.C.; Brancati, F.L. Long-term All-Cause Mortality in Cancer Patients With Preexisting Diabetes Mellitus. A Systematic Review and Meta-analysis. JAMA 2008, 300, 2754–2764. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, P.J.; Ennis, M.; Pritchard, K.I.; Trudeau, M.E.; Koo, J.; Madarnas, Y.; Hartwick, W.; Hoffman, B.; Hood, N. Fasting insulin and outcome in early-stage breast cancer: Results of a prospective cohort study. J. Clin. Oncol. 2002, 20, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Seshasai, S.R.K.; Kaptoge, S.; Thompson, A.; Di Angelantonio, E.; Gao, P.; Sarwar, N.; Whincup, P.H.; Mukamal, K.J.; Gillum, R.F.; Holme, I.; et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar]
- Zhou, X.H.; Qiao, Q.; Zethelius, B.; Pyörälä, K.; Söderberg, S.; Pajak, A.; Stehouwer, C.D.A.; Heine, R.J.; Jousilahti, P.; Ruotolo, G.; et al. DECODE Study Group. Diabetes, prediabetes and cancer mortality. Diabetology 2010, 53, 1867–1876. [Google Scholar] [CrossRef]
- Barone, B.B.; Yeh, H.C.; Snyder, C.F.; Peairs, K.S.; Stein, K.B.; Derr, R.L.; Wolff, A.C.; Brancati, F.L. Postoperative Mortality in Cancer Patients With Preexisting Diabetes: Systematic review and meta-analysis. Diabetes Care 2010, 33, 931–939. [Google Scholar] [CrossRef]
- Bergen, E.S.; Christou, N.; Malicot, K.L.; Canton, C.; Di Batolomeo, M.; Galli, F.; Galli, F.; Labianca, R.; Shi, Q.; Alberts, S.R.; et al. 391MO Impact of diabetes and metformin use on recurrence and outcome in early colon cancer (CC) patients—A pooled analysis of 3 adjuvant trials. Ann. Oncol. 2021, 32, S530–S582. [Google Scholar] [CrossRef]
- Bertoni, A.G.; Saydah, S.; Brancati, F.L. Diabetes and the Risk of Infection-Related Mortality in the U.S. Diabetes Care 2001, 24, 1044–1049. [Google Scholar] [CrossRef]
- Umpierrez, G.E.; Isaacs, S.D.; Bazargan, N.; You, X.; Thaler, L.M.; Kitabchi, A.E. Hyperglycemia: An Independent Marker of In-Hospital Mortality in Patients with Undiagnosed Diabetes. J. Clin. Endocrinol. Metab. 2002, 87, 978–982. [Google Scholar] [CrossRef]
- Meyerhardt, J.A.; Catalano, P.J.; Haller, D.G.; Mayer, R.J.; Macdonald, J.S.; Benson, A.B., 3rd; Fuchs, C.S. Impact of diabetes mellitus on outcomes in patients with colon cancer. J. Clin. Oncol. 2003, 21, 433–440. [Google Scholar] [CrossRef]
- Shariff, A.I.; Syed, S.; A Shelby, R.; Force, J.; Clarke, J.M.; D’Alessio, D.; Corsino, L. Novel cancer therapies and their association with diabetes. J. Mol. Endocrinol. 2019, 62, R187–R199. [Google Scholar] [CrossRef]
- Liu, M.; Guo, F. Recent updates on cancer immunotherapy. Precis. Clin. Med. 2018, 1, 65–74. [Google Scholar] [CrossRef]
- Padma, V.V. An overview of targeted cancer therapy. BioMedicine 2015, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.X.; Loh, K.; Yap, Y.-S. PI3K/Akt/mTOR inhibitors in breast cancer. Cancer Biol. Med. 2015, 12, 342–354. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.Y.; Shameem, R.; Wu, S. Risk of hyperglycemia attributable to everolimus in cancer patients: A meta-analysis. Acta Oncol. 2016, 55, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Szczylik, C.; Feingold, J.; Strahs, A.; Berkenblit, A. Temsirolimus safety profile and management of toxic effects in patients with advanced renal cell carcinoma and poor prognostic features. Ann. Oncol. 2008, 19, 1387–1392. [Google Scholar] [CrossRef]
- André, F.; Ciruelos, E.; Rubovszky, G.; André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; et al. SOLAR-1 Study Group. Alpelisib for PIK3CA-Mutated, Hormone Receptor–Positive Advanced Breast Cancer. N. Engl. J. Med. 2019, 380, 1929–1940. [Google Scholar] [CrossRef]
- Doi, T.; Fujiwara, Y.; Matsubara, N.; Tomomatsu, J.; Iwasa, S.; Tanaka, A.; Endo-Tsukude, C.; Nakagawa, S.; Takahashi, S. Phase I study of ipatasertib as a single agent and in combination with abiraterone plus prednisolone in Japanese patients with advanced solid tumors. Cancer Chemother. Pharmacol. 2019, 84, 393–404. [Google Scholar] [CrossRef]
- Smyth, L.M.; Tamura, K.; Oliveira, M.; Ciruelos, E.M.; Mayer, I.A.; Sablin, M.-P.; Biganzoli, L.; Ambrose, H.J.; Ashton, J.; Barnicle, A.; et al. Capivasertib, an AKT Kinase Inhibitor, as Monotherapy or in Combination with Fulvestrant in Patients with AKT1E17K-Mutant, ER-Positive Metastatic Breast Cancer. Clin. Cancer Res. 2020, 26, 3947–3957. [Google Scholar] [CrossRef]
- van der Veeken, J.; Oliveira, S.; Schiffelers, R.M.; Storm, G.; van Bergen En Henegouwen, P.M.; Roovers, R.C. Crosstalk between epidermal growth factor receptor- and insulin-like growth factor-1 receptor signaling: Implications for cancer therapy. Curr. Cancer Drug Targets 2009, 9, 748–760. [Google Scholar] [CrossRef]
- Pollack, M. The insulin and insulin-like growth factor receptor family in neoplasia: An update. Nat. Rev. Cancer 2012, 12, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Becerra, C.R.; Salazar, R.; Garcia-Carbonero, R.; Thomas, A.L.; Vázquez-Mazón, F.J.; Cassidy, J.; Maughan, T.; Castillo, M.G.; Iveson, T.; Yin, N.; et al. Figitumumab in patients with refractory metastatic colorectal cancer previously treated with standard therapies: A nonrandomized, open-label, phase II trial. Cancer Chemother. Pharmacol. 2014, 73, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Higano, C.S.; Berlin, J.; Gordon, M.; Lorusso, P.; Tang, S.; Dontabhaktuni, A.; Schwartz, J.D.; Cosaert, J.; Mehnert, J.M. Safety, tolerability, and pharmacokinetics of single and multiple doses of intravenous cixutumumab (IMC-A12), an inhibitor of the insulin-like growth factor-I receptor, administered weekly or every 2 weeks in patients with advanced solid tumors. Investig. New Drugs 2015, 33, 450–462. [Google Scholar] [CrossRef] [PubMed]
- Sclafani, F.; Kim, T.Y.; Cunningham, D.; Tabernero, J.; Schmoll, H.J.; Roh, J.K.; Kim, S.Y.; Park, Y.S.; Guren, T.K.; Hawkes, E.; et al. A Randomized Phase II/III Study of Dalotuzumab in Combination With Cetuximab and Irinotecan in Chemorefractory, KRASWild-Type, Metastatic Colorectal Cancer. J. Natl. Cancer Inst. 2015, 107, djv258. [Google Scholar] [CrossRef] [PubMed]
- Scartozzi, M.; Bianconi, M.; Maccaroni, E.; Giampieri, R.; Berardi, R.; Cascinu, S. Dalotuzumab, a recombinant humanized mAb targeted against IGFR1 for the treatment of cancer. Curr. Opin. Mol. Ther. 2010, 12, 361–371. [Google Scholar]
- Fassnacht, M.; Berruti, A.; Baudin, E.; Demeure, M.J.; Gilbert, J.; Haak, H.; Kroiss, M.; Quinn, D.I.; Hesseltine, E.; Ronchi, C.L.; et al. Linsitinib (OSI-906) versus placebo for patients with locally advanced or metastatic adrenocortical carcinoma: A double-blind, randomised, phase 3 study. Lancet Oncol. 2015, 16, 426–435. [Google Scholar] [CrossRef]
- Goyal, L.; Wadlow, R.; Blaszkowsky, L.S.; Wolpin, B.M.; Abrams, T.A.; McCleary, N.J.; Sheehan, S.; Sundaram, E.; Karol, M.D.; Chen, J.; et al. A phase I and pharmacokinetic study of ganetespib (STA-9090) in advanced hepatocellular carcinoma. Investig. New Drugs 2015, 33, 128–137. [Google Scholar] [CrossRef]
- Pillai, R.N.; Fennell, D.A.; Kovcin, V.; Ciuleanu, T.E.; Ramlau, R.; Kowalski, D.; Schenker, M.; Yalcin, I.; Teofilovici, F.; Vukovic, V.M. Randomized Phase III Study of Ganetespib, a Heat Shock Protein 90 Inhibitor, With Docetaxel Versus Docetaxel in Advanced Non-Small-Cell Lung Cancer (GALAXY-2). J. Clin. Oncol. 2020, 38, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Kim, D.-W.; Mehra, R.; Tan, D.S.; Felip, E.; Chow, L.Q.; Camidge, D.R.; Vansteenkiste, J.; Sharma, S.; De Pas, T.; et al. Ceritinib inALK-Rearranged Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 370, 1189–1197. [Google Scholar] [CrossRef]
- Dassonville, O.; Bozec, A.; Fischel, J.L.; Milano, G. EGFR targeting therapies: Monoclonal antibodies versus tyrosine kinase inhibitors: Similarities and differences. Crit. Rev. Oncol. 2007, 62, 53–61. [Google Scholar] [CrossRef]
- Xu, M.J.; Johnson, D.E.; Grandis, J.R. EGFR-targeted therapies in the post-genomic era. Cancer Metastasis Rev. 2017, 36, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Soria, J.-C.; Goldman, J.W.; Wakelee, H.A.; Gadgeel, S.M.; Varga, A.; Papadimitrakopoulou, V.; Solomon, B.J.; Oxnard, G.R.; Dziadziuszko, R.; et al. Rociletinib in EGFR-Mutated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 372, 1700–1709. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Liu, J.; Huang, X.; Jiang, Q. Adverse effects of dasatinib on glucose-lipid metabolism in patients with chronic myeloid leukaemia in the chronic phase. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef]
- Saglio, G.; Kim, D.-W.; Issaragrisil, S.; Le Coutre, P.; Etienne, G.; Lobo, C.; Pasquini, R.; Clark, R.E.; Hochhaus, A.; Hughes, T.; et al. Nilotinib versus Imatinib for Newly Diagnosed Chronic Myeloid Leukemia. N. Engl. J. Med. 2010, 362, 2251–2259. [Google Scholar] [CrossRef] [PubMed]
- Racil, Z.; Razga, F.; Drapalova, J.; Buresova, L.; Zackova, D.; Palackova, M.; Semerad, L.; Malaskova, L.; Haluzik, M.; Mayer, J. Mechanism of impaired glucose metabolism during nilotinib therapy in patients with chronic myelogenous leukemia. Haematology 2013, 98, e124–e126. [Google Scholar] [CrossRef]
- Gibb, F.W.; Dixon, J.M.; Clarke, C.; Homer, N.Z.; Faqehi, A.M.M.; Andrew, R.; Walker, B.R. Higher Insulin Resistance and Adiposity in Postmenopausal Women with Breast Cancer Treated with Aromatase Inhibitors. J. Clin. Endocrinol. Metab. 2019, 104, 3670–3678. [Google Scholar] [CrossRef]
- Hamood, R.; Hamood, H.; Merhasin, I.; Keinan-Boker, L. Diabetes after Hormone Therapy in Breast Cancer Survivors: A Case-Cohort Study. J. Clin. Oncol. 2018, 36, 2061–2069. [Google Scholar] [CrossRef]
- Wang, H.; Sun, X.; Zhao, L.; Chen, X.; Zhao, J. Androgen deprivation therapy is associated with diabetes: Evidence from meta-analysis. J. Diabetes Investig. 2016, 7, 629–636. [Google Scholar] [CrossRef]
- Yu, I.-C.; Lin, H.-Y.; Sparks, J.; Yeh, S.; Chang, C. Androgen Receptor Roles in Insulin Resistance and Obesity in Males: The Linkage of Androgen-Deprivation Therapy to Metabolic Syndrome. Diabetes 2014, 63, 3180–3188. [Google Scholar] [CrossRef]
- Angeletti, S.; Corleto, V.D.; Schillaci, O.; Marignani, M.; Annibale, B.; Moretti, A.; Silecchia, G.; Scopinaro, F.; Basso, N.; Bordi, C.; et al. Use of the somatostatin analogue octreotide to localise and manage somatostatin-producing tumours. Gut 1998, 42, 792–794. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Müller, H.-H.; Schade-Brittinger, C.; Klose, K.-J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.-F.; Bläker, M.; et al. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors: A Report From the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, P.J.; Kris, M.G.; Basch, E.; Bohlke, K.; Barbour, S.Y.; Clark-Snow, R.A.; Danso, M.A.; Dennis, K.; Dupuis, L.L.; Dusetzina, S.B.; et al. Antiemetics: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 2782–2797. [Google Scholar] [CrossRef]
- Ly, K.I.; Wen, P.Y. Clinical Relevance of Steroid Use in Neuro-Oncology. Curr. Neurol. Neurosci. Rep. 2017, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- McKay, L.I.; Cidlowski, J.A. Corticosteroids in the Treatment of Neoplasms. In Holland-Frei Cancer Medicine, 6th ed.; Kufe, D.W., Pollock, R.E., Weichselbaum, R.R., Bast, R.C., Jr., Gansler, T.S., Holland, J.F., Frei, E., III, Eds.; BC Decker: Hamilton, ON, Canada, 2003. [Google Scholar]
- Barbour, S.Y. Corticosteroids in the Treatment of Chemotherapy-Induced Nausea and Vomiting. J. Natl. Compr. Cancer Netw. 2012, 10, 493–499. [Google Scholar] [CrossRef]
- Haywood, A.; Good, P.; Khan, S.; Leupp, A.; Jenkins-Marsh, S.; Rickett, K.; Hardy, J.R. Corticosteroids for the management of cancer-related pain in adults. Cochrane Database Syst. Rev. 2015, 2021, CD010756. [Google Scholar] [CrossRef]
- Ahmad, M.H.; Shafiq, I. Diabetic ketoacidosis following PEG-asparaginase therapy. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018, 18-0064. [Google Scholar] [CrossRef]
- Komatsu, Y.; Nakamura, A.; Takihata, M.; Inoue, Y.; Yahagi, S.; Tajima, K.; Tsuchiya, H.; Takano, T.; Yamakawa, T.; Yoshida, M.; et al. Safety and tolerability of diazoxide in Japanese patients with hyperinsulinemic hypoglycemia. Endocr. J. 2016, 63, 311–314. [Google Scholar] [CrossRef]
- Zaccardi, F.; Webb, D.R.; Yates, T.; Davies, M. Pathophysiology of type 1 and type 2 diabetes mellitus: A 90-year perspective. Postgrad. Med. J. 2015, 92, 63–69. [Google Scholar] [CrossRef]
- Bennis, Y.; Savry, A.; Rocca, M.; Gauthier-Villano, L.; Pisano, P.; Pourroy, B. Cisplatin dose adjustment in patients with renal impairment, which recommendations should we follow? Int. J. Clin. Pharm. 2014, 36, 420–429. [Google Scholar] [CrossRef]
- Poole, C.; Gardiner, J.; Twelves, C.; Johnston, P.; Harper, P.; Cassidy, J.; Monkhouse, J.; Banken, L.; Weidekamm, E.; Reigner, B. Effect of renal impairment on the pharmacokinetics and tolerability of capecitabine (Xeloda) in cancer patients. Cancer Chemother. Pharmacol. 2002, 49, 225–234. [Google Scholar] [CrossRef]
- Ewer, M.S.; Ewer, S.M. Cardiotoxicity of anticancer treatments. Nat. Rev. Cardiol. 2015, 12, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Sami, A.; Xiang, J. HER2-directed therapy: Current treatment options for HER2-positive breast cancer. Breast Cancer 2015, 22, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.L.; Vincent, A.M.; Cheng, H.T.; Feldman, E.L. Diabetic neuropathy: Mechanisms to management. Pharmacol. Ther. 2008, 120, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Zukas, A.M.; Schiff, D. Neurological complications of new chemotherapy agents. Neuro-Oncology 2018, 20, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; Gallois, C. Adjuvant Chemotherapy for Stage III Colon Cancer. Cancers 2020, 12, 2679. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. 1), S15–S33. [Google Scholar] [CrossRef]
- Tamez-Pérez, H.E.; Quintanilla-Flores, D.L.; Rodríguez-Gutiérrez, R.; González-González, J.G.; Tamez-Peña, A.L. Steroid hyperglycemia: Prevalence, early detection and therapeutic recommendations: A narrative review. World J. Diabetes 2015, 6, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.V.; Bishop, G.; Benito-Herrero, M. Diabetic Ketoacidosis in Type 2 Diabetics: A Novel Presentation of Pancreatic Adenocarcinoma. J. Gen. Intern. Med. 2010, 25, 369–373. [Google Scholar] [CrossRef]
- Markabawi, D.; Kondapi, D.; Tambe, V.; Seth, R. When it is not just DKA; diabetic ketoacidosis as a first presentation of pancreatic adenocarcinoma. Am. J. Emerg. Med. 2018, 36, 1720.e1–1720.e2. [Google Scholar] [CrossRef]
- Busaidy, N.L.; Farooki, A.; Dowlati, A.; Perentesis, J.P.; Dancey, J.E.; Doyle, L.A.; Brell, J.M.; Siu, L.L. Management of metabolic effects associated with anticancer agents targeting the PI3K-Akt-mTOR pathway. J. Clin. Oncol. 2012, 30, 2919–2928. [Google Scholar] [CrossRef] [PubMed]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach: Update to a Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2014, 38, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Farah, S.J.; Masri, N.; Ghanem, H.; Azar, M. Diabetic Ketoacidosis Associated With Alpelisib Treatment of Metastatic Breast Cancer. AACE Clin. Case Rep. 2020, 6, e349–e351. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Morgan, A.; Shah, S.; Ebeling, P.R. Rapid-onset diabetic ketoacidosis secondary to nivolumab therapy. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018, 18–0021. [Google Scholar] [CrossRef] [PubMed]
- Kapila, V.; Topf, J. Sodium-Glucose Co-transporter 2 Inhibitor-Associated Euglycemic Diabetic Ketoacidosis after Bariatric Surgery: A Case and Literature Review. Cureus 2021, 13, 17093. [Google Scholar] [CrossRef] [PubMed]
- Bossi, P.; Antonuzzo, A.; Cherny, N.; Rosengarten, O.; Pernot, S.; Trippa, F.; Schuler, U.; Snegovoy, A.; Jordan, K.; Ripamonti, C. Diarrhoea in adult cancer patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv126–iv142. [Google Scholar] [CrossRef] [PubMed]
- Roila, F.; Molassiotis, A.; Herrstedt, J.; Aapro, M.; Gralla, R.J.; Bruera, E.; Clark-Snow, R.A.; Dupuis, L.L.; Einhorn, L.H.; Feyer, P.; et al. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Ann. Oncol. 2016, 27, v119–v133. [Google Scholar] [CrossRef]
- Katsi, V.; Magkas, N.; Georgiopoulos, G.; Athanasiadi, E.; Virdis, A.; Masi, S.; Kliridis, P.; Hatziyanni, A.; Tsioufis, C.; Tousoulis, D. Arterial hypertension in patients under antineoplastic therapy: A systematic review. J. Hypertens. 2019, 37, 884–901. [Google Scholar] [CrossRef]
- Leon, B.M.; Maddox, T.M. Diabetes and cardiovascular disease: Epidemiology, biological mechanisms, treatment recommendations and future research. World J. Diabetes 2015, 6, 1246–1258. [Google Scholar] [CrossRef]
- Chang, H.M.; Moudgil, R.; Scarabelli, T.; Okwuosa, T.M.; Yeh, E.T.H. Cardiovascular Complications of Cancer Therapy: Best Practices in Diagnosis, Prevention, and Management: Part 1. J. Am. Coll. Cardiol. 2017, 70, 2536–2551. [Google Scholar] [CrossRef]
- Chang, H.M.; Okwuosa, T.M.; Scarabelli, T.; Moudgil, R.; Yeh, E.T.H. Cardiovascular Complications of Cancer Therapy: Best Practices in Diagnosis, Prevention, and Management: Part 2. J. Am. Coll. Cardiol. 2017, 70, 2552–2565. [Google Scholar] [CrossRef]
- Yeh, E.T.; Bickford, C.L. Cardiovascular Complications of Cancer Therapy: Incidence, Pathogenesis, Diagnosis, and Management. J. Am. Coll. Cardiol. 2009, 53, 2231–2247. [Google Scholar] [CrossRef] [PubMed]
- Carey, I.M.; Critchley, J.A.; DeWilde, S.; Harris, T.; Hosking, F.J.; Cook, D.G. Risk of Infection in Type 1 and Type 2 Diabetes Compared With the General Population: A Matched Cohort Study. Diabetes Care 2018, 41, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Critchley, J.A.; Carey, I.M.; Harris, T.; DeWilde, S.; Hosking, F.J.; Cook, D.G. Glycemic Control and Risk of Infections Among People With Type 1 or Type 2 Diabetes in a Large Primary Care Cohort Study. Diabetes Care 2018, 41, 2127–2135. [Google Scholar] [CrossRef]
- Rodrigues, C.F.; Rodrigues, M.E.; Henriques, M. Candida sp. Infections in Patients with Diabetes Mellitus. J. Clin. Med. 2019, 8, 76. [Google Scholar] [CrossRef]
- Di Cosola, M.; Cazzolla, A.P.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Santacroce, L. Candida albicans and Oral Carcinogenesis. A Brief Review. J. Fungi 2021, 12, 476. [Google Scholar] [CrossRef] [PubMed]
- Gafter-Gvili, A.; Fraser, A.; Paul, M.; van de Wetering, M.; Kremer, L.; Leibovici, L. Antibiotic prophylaxis for bacterial infections in afebrile neutropenic patients following chemotherapy. Cochrane Database Syst. Rev. 2012, 1, CD004386. [Google Scholar] [CrossRef]
- Renner, P.; Milazzo, S.; Liu, J.P.; Zwahlen, M.; Birkmann, J.; Horneber, M. Primary prophylactic colony-stimulating factors for the prevention of chemotherapy-induced febrile neutropenia in breast cancer patients. Cochrane Database Syst. Rev. 2012, 10, CD007913. [Google Scholar] [CrossRef]
- Verrotti, A.; Prezioso, G.; Scattoni, R.; Chiarelli, F. Autonomic Neuropathy in Diabetes Mellitus. Front. Endocrinol. 2014, 5, 205. [Google Scholar] [CrossRef]
- Vinik, A.I.; Maser, R.E.; Michell, B.D.; Freeman, R. Diabetic Autonomic Neuropathy. Diabetes Care 2003, 26, 1553–1579. [Google Scholar] [CrossRef]
- Onitilo, A.A.; Donald, M.; Stankowski, R.V.; Engel, J.M.; Williams, G.; Doi, S. Breast and Prostate Cancer Survivors in a Diabetic Cohort: Results from the Living with Diabetes Study. Clin. Med. Res. 2013, 11, 210–218. [Google Scholar] [CrossRef][Green Version]
- Stava, C.J.; Beck, M.L.; Feng, L.; Lopez, A.; Busaidy, N.; Vassilopoulou-Sellin, R. Diabetes mellitus among cancer survivors. J. Cancer Surviv. 2007, 1, 108–115. [Google Scholar] [CrossRef]
- Tella, S.H.; Gallagher, J.C. Prevention and treatment of postmenopausal osteoporosis. J. Steroid Biochem. Mol. Biol. 2013, 142, 155–170. [Google Scholar] [CrossRef]
- Edgington, A.; Morgan, M.A. Looking Beyond Recurrence: Comorbidities in Cancer Survivors. Clin. J. Oncol. Nurs. 2011, 15, E3–E12. [Google Scholar] [CrossRef]
- Ligibel, J. Lifestyle Factors in Cancer Survivorship. J. Clin. Oncol. 2012, 30, 3697–3704. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.S.; Grant, S.F.; Herman, M.E. Intersections and Clinical Translations of Diabetes Mellitus with Cancer Promotion, Progression and Prognosis. Postgrad. Med. 2019, 131, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Lu, P.; Beeraka, N.M.; Sukocheva, O.A.; Madhunapantula, S.V.; Liu, J.; Sinelnikov, M.Y.; Nikolenko, V.N.; Bulygin, K.V.; Mikhaleva, L.M.; et al. Mitochondrial mutations and mitoepigenetics: Focus on regulation of oxidative stress-induced responses in breast cancers. Semin. Cancer Biol. 2020, 6, 05954. [Google Scholar] [CrossRef] [PubMed]
- Klil-Drori, A.; Azoulay, L.; Pollak, M.N. Cancer, obesity, diabetes, and antidiabetic drugs: Is the fog clearing? Nat. Rev. Clin. Oncol. 2016, 14, 85–99. [Google Scholar] [CrossRef]
- Gallagher, E.J.; LeRoith, D. Obesity and Diabetes: The Increased Risk of Cancer and Cancer-Related Mortality. Physiol. Rev. 2015, 95, 727–748. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).