
How the Severity and Mechanism of Recurrent Laryngeal Nerve Dysfunction during Monitored Thyroidectomy Impact on Postoperative Voice

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Objective and Subjective Voice Analyses
2.2. Statistical Analysis
3. Results
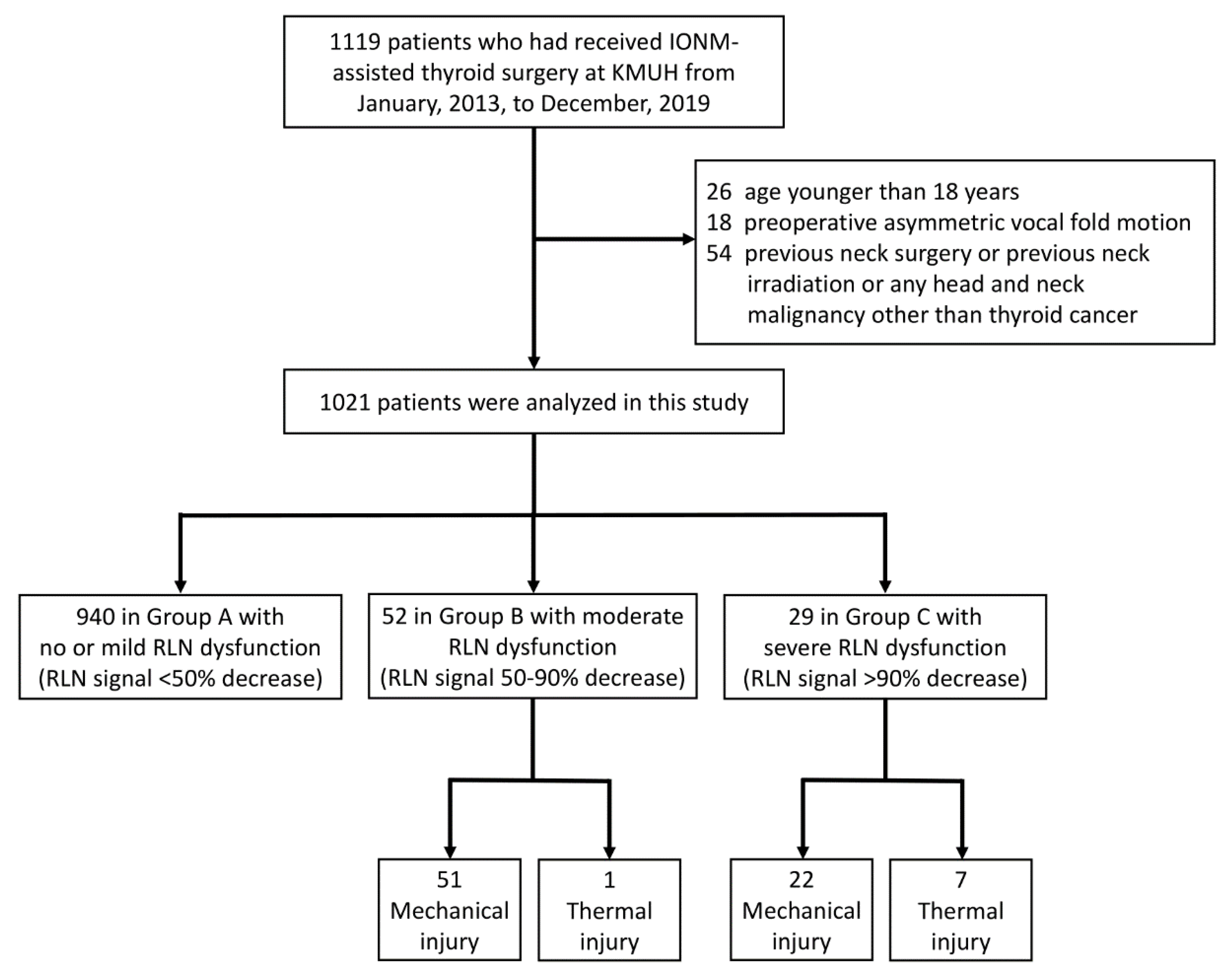
3.1. Demographic Characteristics of Patients
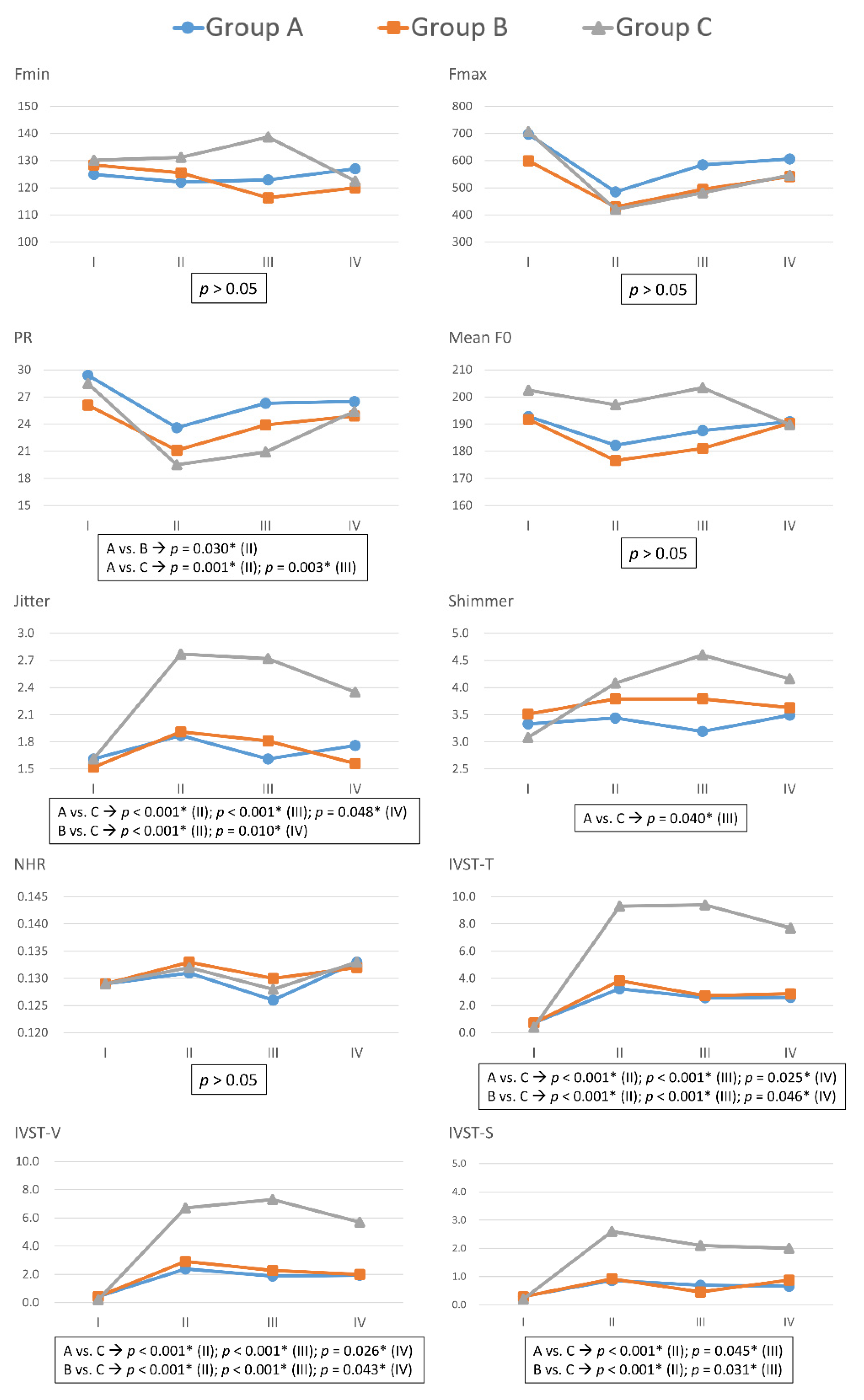
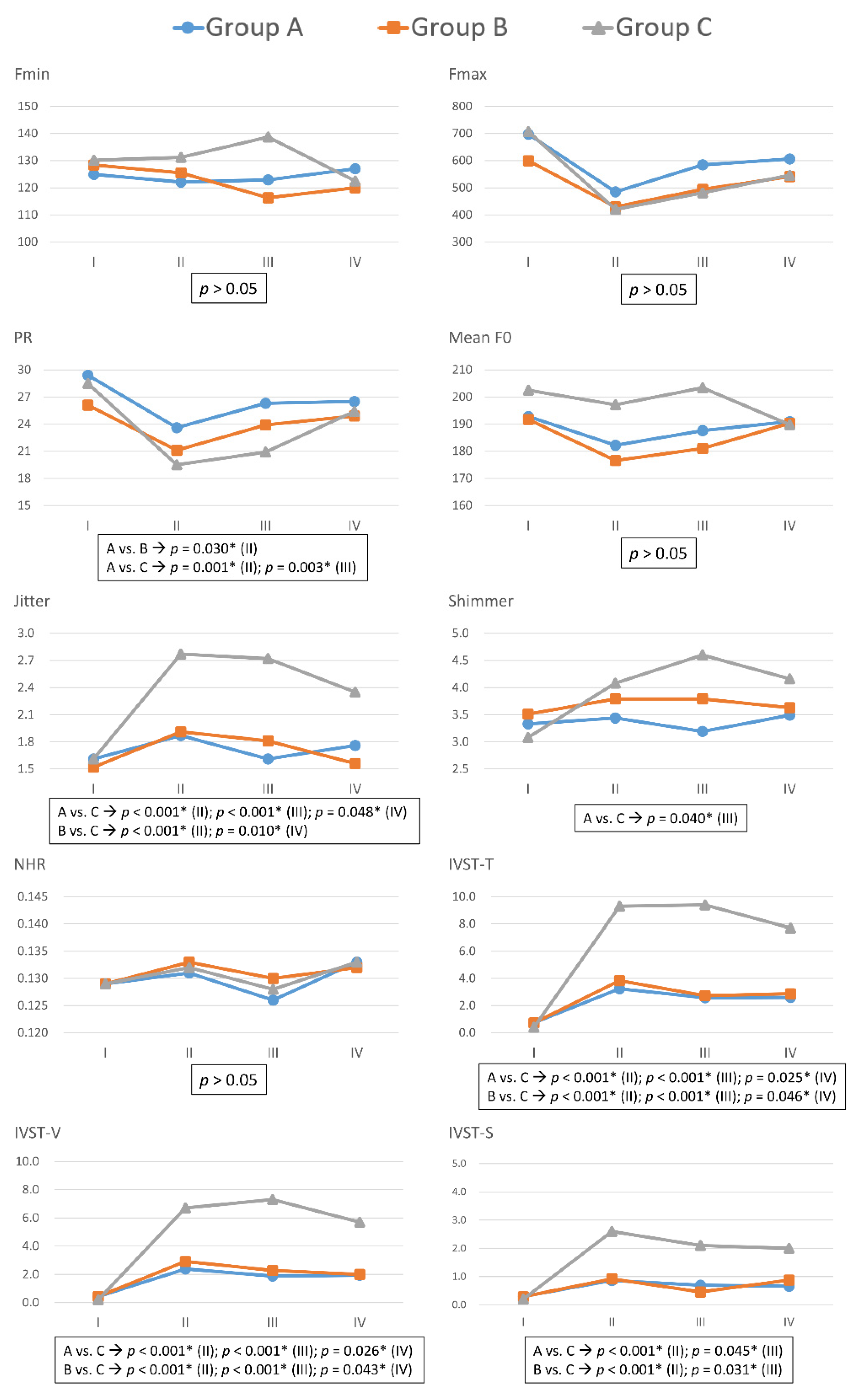
3.2. Voice Parameters in Patients with Different Severity of RLN Dysfunction
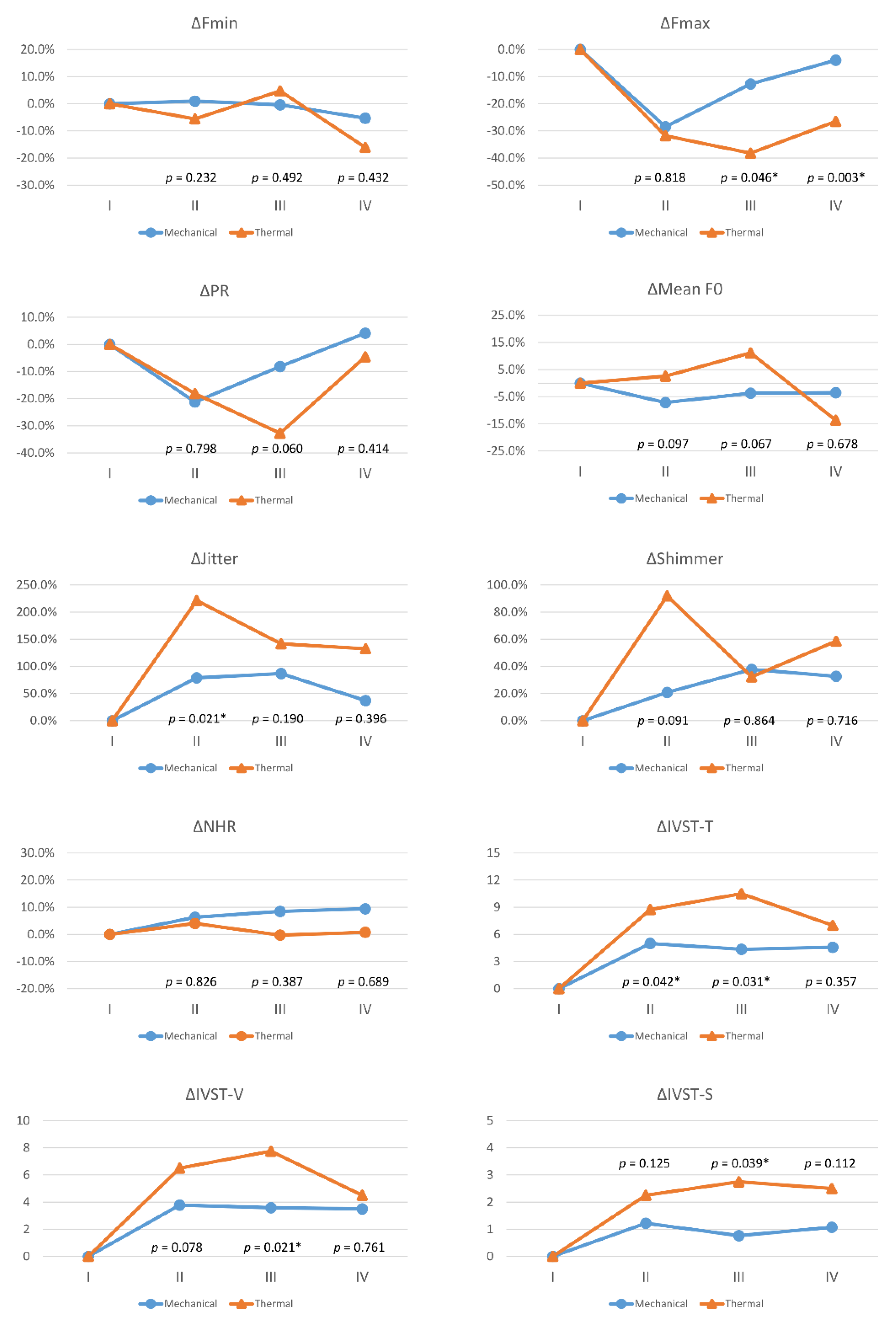
3.3. Voice Parameter Changes (Δ) with Different Mechanism of RLN Dysfunction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meek, P.; Carding, P.N.; Howard, D.; Lennard, T. Voice change following thyroid and parathyroid surgery. J. Voice 2008, 22, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Périé, S.; Laccourreye, O.; Bou-Malhab, F.; Brasnu, D. Aspiration in unilateral recurrent laryngeal nerve paralysis after surgery. Am. J. Otolaryngol. 1998, 19, 18–23. [Google Scholar] [CrossRef]
- Wu, C.W.; Hao, M.; Tian, M.; Dionigi, G.; Tufano, R.P.; Kim, H.Y.; Jung, K.Y.; Liu, X.; Sun, H.; Lu, I.C.; et al. Recurrent laryngeal nerve injury with incomplete loss of electromyography signal during monitored thyroidectomy-evaluation and outcome. Langenbeck Arch. Surg. 2017, 402, 691–699. [Google Scholar] [CrossRef]
- Wu, C.W.; Lee, K.D.; Tae, K.; Ji, Y.B.; Kim, S.U.; Lee, H.S.; Lee, K.W.; Chiang, F.Y. Recurrent Laryngeal Nerve (RLN) Injury in Thyroid Surgery: Lessons Learned from the Intraoperative Neural Monitoring (IONM). Int. J. Head Neck Sci. 2017, 1, 19–26. [Google Scholar] [CrossRef]
- Chiang, F.-Y.; Lee, K.-W.; Chen, H.-C.; Chen, H.-Y.; Lu, I.-C.; Kuo, W.-R.; Hsieh, M.-C.; Wu, C.-W. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J. Surg. 2010, 34, 223–229. [Google Scholar] [CrossRef]
- Randolph, G.W.; Dralle, H.; International Intraoperative Monitoring Study Group; Abdullah, H.; Barczynski, M.; Bellantone, R.; Brauckhoff, M.; Carnaille, B.; Cherenko, S.; Chiang, F.Y. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: International standards guideline statement. Laryngoscope 2011, 121, S1–S16. [Google Scholar] [CrossRef] [PubMed]
- Chiang, F.-Y.; Lu, I.-C.; Kuo, W.-R.; Lee, K.-W.; Chang, N.-C.; Wu, C.-W. The mechanism of recurrent laryngeal nerve injury during thyroid surgery—The application of intraoperative neuromonitoring. Surgery 2008, 143, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Snyder, S.K.; Lairmore, T.C.; Hendricks, J.C.; Roberts, J.W. Elucidating mechanisms of recurrent laryngeal nerve injury during thyroidectomy and parathyroidectomy. J. Am. Coll. Surg. 2008, 206, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.; Randolph, G.; Dionigi, G.; Barczynski, M.; Chiang, F.Y.; Wu, C.W.; Musholt, T.; Uludag, M.; Makay, Ö.; Sezer, A. Prediction of postoperative vocal fold function after intraoperative recovery of loss of signal. Laryngoscope 2019, 129, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Duclos, A.; Lifante, J.-C.; Ducarroz, S.; Soardo, P.; Colin, C.; Peix, J.-L. Influence of intraoperative neuromonitoring on surgeons’ technique during thyroidectomy. World J. Surg. 2011, 35, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.W.; Wang, M.H.; Chen, C.C.; Chen, H.C.; Chen, H.Y.; Yu, J.Y.; Chang, P.Y.; Lu, I.C.; Lin, Y.C.; Chiang, F.Y. Loss of signal in recurrent nerve neuromonitoring: Causes and management. Gland. Surg. 2015, 4, 19–26. [Google Scholar] [CrossRef]
- Wu, C.W.; Chen, C.C.; Wang, M.H.; Huang, T.Y.; Chiang, F.Y.; Dionigi, G. Recent Advances in Analysis and Management of Loss of Signal during Monitored Thyroidectomy. Int. J. Head Neck Sci. 2018, 2, 147–155. [Google Scholar] [CrossRef]
- Stojadinovic, A.; Shaha, A.R.; Orlikoff, R.F.; Nissan, A.; Kornak, M.-F.; Singh, B.; Boyle, J.O.; Shah, J.P.; Brennan, M.F.; Kraus, D.H. Prospective functional voice assessment in patients undergoing thyroid surgery. Ann. Surg. 2002, 236, 823–832. [Google Scholar] [CrossRef]
- Musholt, T.J.; Musholt, P.B.; Garm, J.; Napiontek, U.; Keilmann, A. Changes of the speaking and singing voice after thyroid or parathyroid surgery. Surgery 2006, 140, 978–989. [Google Scholar] [CrossRef]
- Sinagra, D.L.; Montesinos, M.R.; Tacchi, V.A.; Moreno, J.C.; Falco, J.E.; Mezzadri, N.A.; Debonis, D.L.; Curutchet, H.P. Voice changes after thyroidectomy without recurrent laryngeal nerve injury. J. Am. Coll. Surg. 2004, 199, 556–560. [Google Scholar] [CrossRef]
- Rosato, L.; Carlevato, M.T.; De Toma, G.; Avenia, N. Recurrent laryngeal nerve damage and phonetic modifications after total thyroidectomy: Surgical malpractice only or predictable sequence? World J. Surg. 2005, 29, 780–784. [Google Scholar] [CrossRef]
- Borel, F.; Tresallet, C.; Hamy, A.; Mathonnet, M.; Lifante, J.-C.; Brunaud, L.; Marret, O.; Caillard, C.; Espitalier, F.; Drui, D. Self-assessment of voice outcomes after total thyroidectomy using the Voice Handicap Index questionnaire: Results of a prospective multicenter study. Surgery 2020, 167, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.P.; Raffaelli, M.; D’Alatri, L.; Marchese, M.R.; Rigante, M.; Paludetti, G.; Bellantone, R. Voice and swallowing changes after thyroidectomy in patients without inferior laryngeal nerve injuries. Surgery 2006, 140, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, C.E.; Asimakopoulou, P.; Proimos, E.; Perogamvrakis, G.; Papoutsaki, E.; Chimona, T. Subjective and objective voice assessments after recurrent laryngeal nerve-preserved total thyroidectomy. J. Voice 2017, 31, 515.e515–515.e521. [Google Scholar] [CrossRef]
- Jeannon, J.P.; Orabi, A.; Bruch, G.; Abdalsalam, H.; Simo, R. Diagnosis of recurrent laryngeal nerve palsy after thyroidectomy: A systematic review. Int. J. Clin. Pract. 2009, 63, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.; Randolph, G.W.; Dionigi, G.; Wu, C.W.; Barczynski, M.; Chiang, F.Y.; Al-Quaryshi, Z.; Angelos, P.; Brauckhoff, K.; Cernea, C.R. International neural monitoring study group guideline 2018 part I: Staging bilateral thyroid surgery with monitoring loss of signal. Laryngoscope 2018, 128, S1–S17. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.W.; Dionigi, G.; Barczynski, M.; Chiang, F.Y.; Dralle, H.; Schneider, R.; Al-Quaryshi, Z.; Angelos, P.; Brauckhoff, K.; Brooks, J.A. International neuromonitoring study group guidelines 2018: Part II: Optimal recurrent laryngeal nerve management for invasive thyroid cancer—Incorporation of surgical, laryngeal, and neural electrophysiologic data. Laryngoscope 2018, 128, S18–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, F.-Y.; Lu, I.-C.; Chen, H.-C.; Chen, H.-Y.; Tsai, C.-J.; Hsiao, P.-J.; Lee, K.-W.; Wu, C.-W. Anatomical variations of recurrent laryngeal nerve during thyroid surgery: How to identify and handle the variations with intraoperative neuromonitoring. Kaohsiung J. Med. Sci. 2010, 26, 575–583. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.-L.; Wu, C.-W.; Zhao, Y.-S.; Wang, T.; Chen, P.; Xin, J.-W.; Li, S.-J.; Zhang, D.-Q.; Zhang, G.; Fu, Y.-T. Exclusive real-time monitoring during recurrent laryngeal nerve dissection in conventional monitored thyroidectomy. Kaohsiung J. Med. Sci. 2016, 32, 135–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, R.; Randolph, G.W.; Sekulla, C.; Phelan, E.; Thanh, P.N.; Bucher, M.; Machens, A.; Dralle, H.; Lorenz, K. Continuous intraoperative vagus nerve stimulation for identification of imminent recurrent laryngeal nerve injury. Head Neck 2013, 35, 1591–1598. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-W.; Dionigi, G.; Sun, H.; Liu, X.; Kim, H.Y.; Hsiao, P.-J.; Tsai, K.-B.; Chen, H.-C.; Chen, H.-Y.; Chang, P.-Y. Intraoperative neuromonitoring for the early detection and prevention of RLN traction injury in thyroid surgery: A porcine model. Surgery 2014, 155, 329–339. [Google Scholar] [CrossRef]
- Dionigi, G.; Donatini, G.; Boni, L.; Rausei, S.; Rovera, F.; Tanda, M.L.; Kim, H.Y.; Chiang, F.-Y.; Wu, C.-W.; Mangano, A. Continuous monitoring of the recurrent laryngeal nerve in thyroid surgery: A critical appraisal. Int. J. Surg. 2013, 11, S44–S46. [Google Scholar] [CrossRef]
- Dionigi, G.; Wu, C.-W.; Kim, H.Y.; Rausei, S.; Boni, L.; Chiang, F.-Y. Severity of recurrent laryngeal nerve injuries in thyroid surgery. World J. Surg. 2016, 40, 1373–1381. [Google Scholar] [CrossRef]
- Borel, F.; Christou, N.; Marret, O.; Mathonnet, M.; Caillard, C.; Bannani, S.; Drui, D.; Espitalier, F.; Blanchard, C.; Mirallié, E. Long-term voice quality outcomes after total thyroidectomy: A prospective multicenter study. Surgery 2018, 163, 796–800. [Google Scholar] [CrossRef]
- Dewan, K.; Vahabzadeh-Hagh, A.; Soofer, D.; Chhetri, D.K. Neuromuscular compensation mechanisms in vocal fold paralysis and paresis. Laryngoscope 2017, 127, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Chiang, F.-Y.; Wang, L.-F.; Huang, Y.-F.; Lee, K.-W.; Kuo, W.-R. Recurrent laryngeal nerve palsy after thyroidectomy with routine identification of the recurrent laryngeal nerve. Surgery 2005, 137, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekhar, S.S.; Randolph, G.W.; Seidman, M.D.; Rosenfeld, R.M.; Angelos, P.; Barkmeier-Kraemer, J.; Benninger, M.S.; Blumin, J.H.; Dennis, G.; Hanks, J. Clinical practice guideline: Improving voice outcomes after thyroid surgery. Otolaryngol. Head Neck Surg. 2013, 148, S1–S37. [Google Scholar] [CrossRef] [PubMed]
- Tsou, Y.-A.; Liu, Y.-W.; Chang, W.-D.; Chen, W.-C.; Ke, H.-C.; Lin, W.-Y.; Yang, H.-R.; Shie, D.-Y.; Tsai, M.-H. Using innovative acoustic analysis to predict the postoperative outcomes of unilateral vocal fold paralysis. BioMed Res. Int. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakis, I.; Klang, P.; Talat, N.; Galata, G.; Schulte, K.-M. Long-term quality of voice is usually acceptable after initial hoarseness caused by a thyroidectomy or a parathyroidectomy. Gland. Surg. 2019, 8, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.; Heyduck, A.; Hoffmann, T.K.; Brosch, S.; Buchberger, M.A.; Schorer, K.; Weber, T.; Pickhard, A. Quality of Voice and Prognostic Markers for the Recovery of Vocal Fold Paralysis After Thyroid Surgery. Ann. Otol. Rhinol. Laryngol. 2019, 128, 1104–1110. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Total 1021 Cases | Group A | Group B | Group C | p Value |
|---|---|---|---|---|
| Number (%) | 940 (92.1) | 52 (5.1) | 29 (2.8) | |
| Age (mean ± SD) | 50.9 ± 13.3 | 52.2 ± 14.1 | 52.1 ± 10.4 | 0.377 |
| Gender | 0.968 | |||
| Male (%) | 206 (21.9) | 12 (23.1) | 6 (20.7) | |
| Female (%) | 734 (78.1) | 40 (76.9) | 23 (79.3) | |
| Surgical extent | 0.004 | |||
| Unilateral (%) | 254 (27.0) | 8 (15.4) | 1 (3.4) | |
| Bilateral (%) | 686 (73.0) | 44 (84.6) | 28 (96.6) | |
| Pathology | 0.017 | |||
| Benign (%) | 610 (64.9) | 27 (51.9) | 13 (44.8) | |
| Graves’ disease | 37 | 4 | 3 | |
| Benign intrathoracic goiter | 58 | 6 | 3 | |
| Malignant (%) | 330 (35.1) | 25 (48.1) | 16 (55.2) | |
| Neck dissection | <0.001 | |||
| Without CND or LND (%) | 782 (83.2) | 36 (69.3) | 13 (44.8) | |
| With CND, without LND (%) | 136 (14.5) | 10 (19.2) | 13 (44.8) | |
| With CND and LND (%) | 22 (2.3) | 6 (11.5) | 3 (10.4) | |
| Injury mechanism and type | 1626 NAR | 96 NAR | 57 NAR | 0.006 |
| Mechanical | 0 NAR | 51 NAR | 22 NAR | |
| Type 1 | - | 43 NAR | 17 NAR | |
| Type 2 | - | 8 NAR | 5 NAR | |
| Thermal | 0 NAR | 1 NAR | 7 NAR | |
| Vocal fold motion | <0.001 | |||
| Asymmetric during Period-III | 0 (0.0) | 13 (25.0) | 27 (93.1) | |
| Asymmetric during Period-IV | 0 (0.0) | 4 (7.7) | 18 (62.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, T.-Y.; Yu, W.-H.V.; Chiang, F.-Y.; Wu, C.-W.; Fu, S.-C.; Tai, A.-S.; Lin, Y.-C.; Tseng, H.-Y.; Lee, K.-W.; Lin, S.-H. How the Severity and Mechanism of Recurrent Laryngeal Nerve Dysfunction during Monitored Thyroidectomy Impact on Postoperative Voice. Cancers 2021, 13, 5379. https://doi.org/10.3390/cancers13215379
Huang T-Y, Yu W-HV, Chiang F-Y, Wu C-W, Fu S-C, Tai A-S, Lin Y-C, Tseng H-Y, Lee K-W, Lin S-H. How the Severity and Mechanism of Recurrent Laryngeal Nerve Dysfunction during Monitored Thyroidectomy Impact on Postoperative Voice. Cancers. 2021; 13(21):5379. https://doi.org/10.3390/cancers13215379
Chicago/Turabian StyleHuang, Tzu-Yen, Wing-Hei Viola Yu, Feng-Yu Chiang, Che-Wei Wu, Shih-Chen Fu, An-Shun Tai, Yi-Chu Lin, Hsin-Yi Tseng, Ka-Wo Lee, and Sheng-Hsuan Lin. 2021. "How the Severity and Mechanism of Recurrent Laryngeal Nerve Dysfunction during Monitored Thyroidectomy Impact on Postoperative Voice" Cancers 13, no. 21: 5379. https://doi.org/10.3390/cancers13215379
APA StyleHuang, T.-Y., Yu, W.-H. V., Chiang, F.-Y., Wu, C.-W., Fu, S.-C., Tai, A.-S., Lin, Y.-C., Tseng, H.-Y., Lee, K.-W., & Lin, S.-H. (2021). How the Severity and Mechanism of Recurrent Laryngeal Nerve Dysfunction during Monitored Thyroidectomy Impact on Postoperative Voice. Cancers, 13(21), 5379. https://doi.org/10.3390/cancers13215379