
Papillary Thyroid Cancer Prognosis: An Evolving Field

 ,
,  , , , , , ,
, , , , , ,  and
and 
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
2. Thyroid Nodules
3. Thyroid Cancer Therapy
4. Thyroid Cancer Patient’s Staging
4.1. Clinicopathological Features Affecting the Prognosis of DTC Patients
4.2. Molecular Risk Stratification of DTC Patients
4.2.1. BRAFV600E Mutation
4.2.2. TERT Promoter Mutations
4.2.3. The Connection BRAFV600E-TERTp Mutations
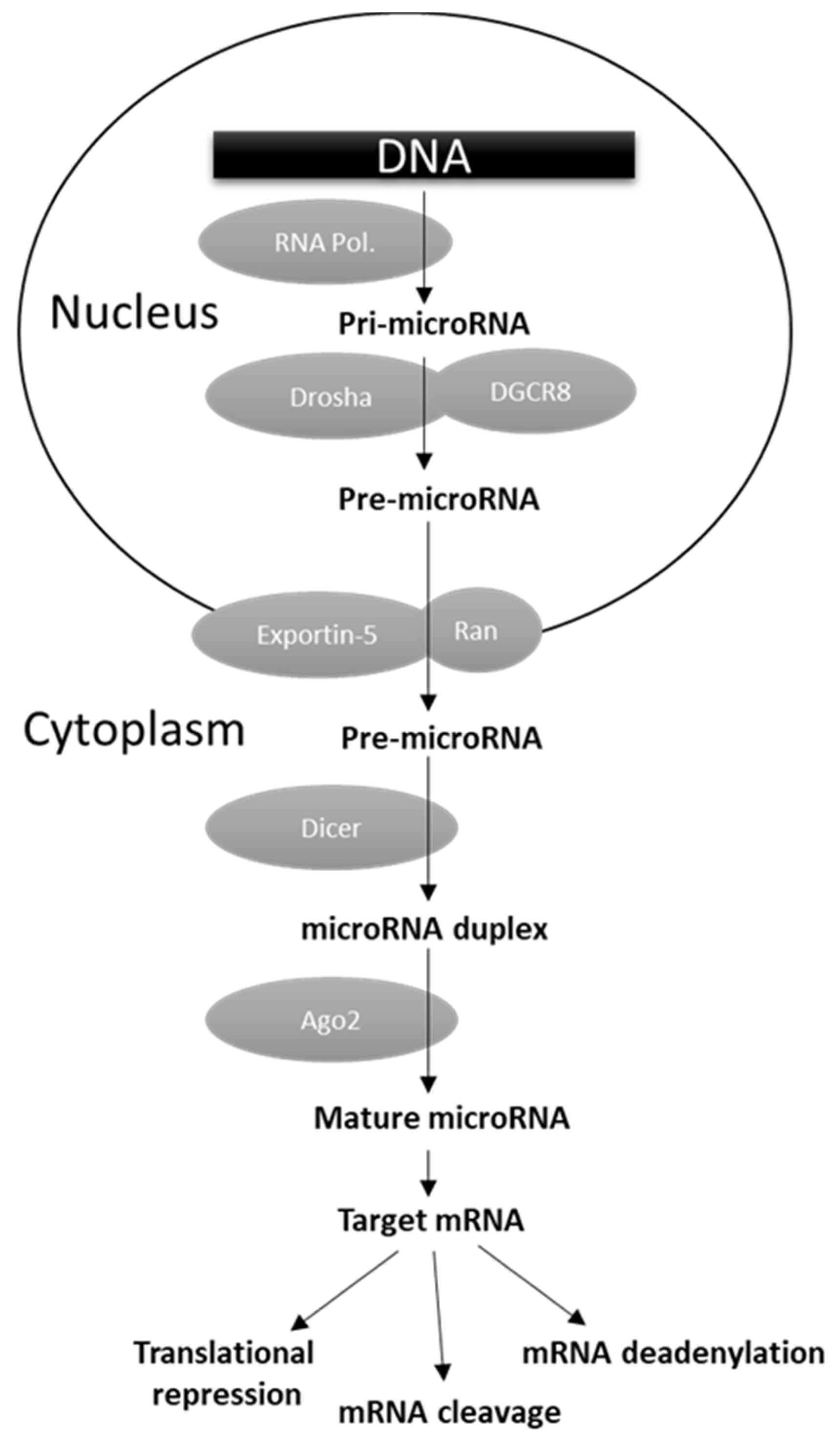
4.2.4. MicroRNAs
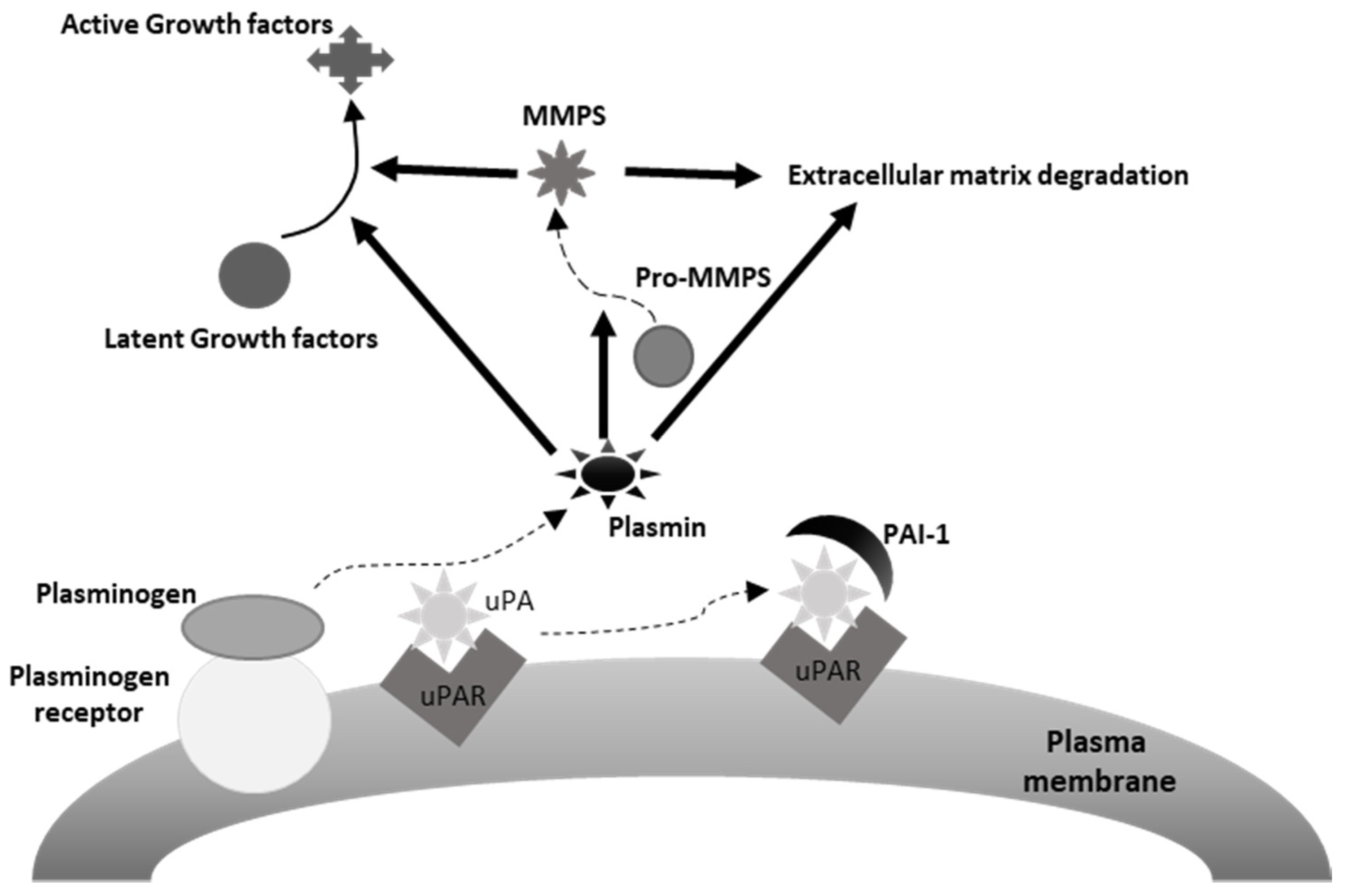
4.2.5. Components of the Urokinase Plasminogen Activating System
4.2.6. Other Possible Biomarkers
5. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Trimboli, P.; Ulisse, S.; Graziano, F.; Marzullo, A.; Ruggieri, M.; Calvanese, A.; Piccirilli, F.; Cavaliere, R.; Fumarola, A.; D’Armiento, M. Trend in Thyroid Carcinoma Size, Age at Diagnosis, and Histology in a Retrospective Study of 500 Cases Diagnosed Over 20 Years. Thyroid 2006, 16, 1151–1155. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Increasing Incidence of Thyroid Cancer in the United States, 1973–2002. JAMA 2006, 295, 2164–2167. [Google Scholar] [CrossRef]
- Davies, L.; Morris, L.G.; Haymart, M.; Chen, A.Y.; Goldenberg, D.; Morris, J.; Ogilvie, J.B.; Terris, D.J.; Netterville, J.; Wong, R.J.; et al. American Association of Clinical Endocrinologists and American College of Endocrinology Disease State Clinical Review: The Increasing Incidence of Thyroid Cancer. Endocr. Pract. 2015, 21, 686–696. [Google Scholar] [CrossRef]
- Nikiforov, Y.E. Diagnostic Pathology and Molecular Genetics of the Thyroid; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009. [Google Scholar]
- Ibrahimpasic, T.; Ghossein, R.; Shah, J.P.; Ganly, I. Poorly Differentiated Carcinoma of the Thyroid Gland: Current Status and Future Prospects. Thyroid 2019, 29, 311–321. [Google Scholar] [CrossRef]
- Janjua, N.; Wreesmann, V.B. Aggressive differentiated thyroid cancer. Eur. J. Surg. Oncol. (EJSO) 2018, 44, 367–377. [Google Scholar] [CrossRef]
- O’Neill, J.P.; Shaha, A.R. Anaplastic thyroid cancer. Oral Oncol. 2013, 49, 702–706. [Google Scholar] [CrossRef]
- Bai, Y.; Kakudo, K.; Jung, C.K. Updates in the Pathologic Classification of Thyroid Neoplasms: A Review of the World Health Organization Classification. Endocrinol. Metab. 2020, 35, 696–715. [Google Scholar] [CrossRef]
- Agrawal, N.; Akbani, R.; Aksoy, B.A.; Ally, A.; Arachchi, H.; Asa, S.; Auman, J.T.; Balasundaram, M.; Balu, S.; Baylin, S.B.; et al. Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef]
- Kondo, T.; Ezzat, S.; Asa, S. Pathogenetic mechanisms in thyroid follicular-cell neoplasia. Nat. Rev. Cancer 2006, 6, 292–306. [Google Scholar] [CrossRef]
- Antonelli, A.; Baldini, E.; Sorrenti, S.; Fallahi, P.; Miccoli, P.; Filippini, A.; Ulisse, S. Emerging therapeutic approaches for the most aggressive epithelial thyroid cancers. In Thyroid Cancer Advances in Diagnosis and Therapy; InTech: Rijeka, Croatia, 2016; pp. 171–191. [Google Scholar]
- Lemoine, N.R.; Mayall, E.S.; Wyllie, F.S.; Farr, C.J.; Hughes, D.; Padua, R.A.; Thurston, V.; Williams, E.D.; Wynford-Thomas, D. Activated ras oncogenes in human thyroid cancers. Cancer Res. 1988, 48, 4459–4463. [Google Scholar]
- Suárez, H.G.; Du Villard, J.A.; Caillou, B.; Schlumberger, M.; Tubiana, M.; Parmentier, C.; Monier, R. Detection of activated ras oncogenes in human thyroid carcinomas. Oncogene 1988, 2, 403–406. [Google Scholar]
- Grieco, M.; Santoro, M.; Berlingieri, M.T.; Melillo, R.M.; Donghi, R.; Bongarzone, I.; Pierotti, M.A.; Della Ports, G.; Fusco, A.; Vecchiot, G. PTC is a novel rearranged form of the ret proto-oncogene and is frequently detected in vivo in human thyroid papillary carcinomas. Cell 1990, 60, 557–563. [Google Scholar] [CrossRef]
- Pierotti, M.A.; Bongarzone, I.; Borrello, M.G.; Mariani, C.; Miranda, C.; Sozzi, G.; Greco, A. Rearrangements of TRK proto-oncogene in papillary thyroid carcinomas. J. Endocrinol. Investig. 1995, 18, 130–133. [Google Scholar] [CrossRef]
- Kimura, E.T.; Nikiforova, M.N.; Zhu, Z.; Knauf, J.A.; Nikiforov, Y.E.; Fagin, J.A. High prevalence of BRAF mutations in thyroid cancer: Genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carci-noma. Cancer Res. 2003, 63, 1454–1457. [Google Scholar]
- Cohen, Y.; Xing, M.; Mambo, E.; Guo, Z.; Wu, G.; Trink, B.; Beller, U.; Westra, W.H.; Ladenson, P.W.; Sidransky, D. BRAF Mutation in Papillary Thyroid Carcinoma. J. Natl. Cancer Inst. 2003, 95, 625–627. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Bishop, J.; Shan, Y.; Pai, S.; Liu, D.; Murugan, A.K.; Sun, H.; El-Naggar, A.K.; Xing, M. Highly prevalent TERT promoter mutations in aggressive thyroid cancers. Endocr.-Relat. Cancer 2013, 20, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Qu, S.; Liu, R.; Sheng, C.; Shi, X.; Zhu, G.; Murugan, A.K.; Guan, H.; Yu, H.; Wang, Y.; et al. TERT Promoter Mutations and Their Association withBRAFV600E Mutation and Aggressive Clinicopathological Characteristics of Thyroid Cancer. J. Clin. Endocrinol. Metab. 2014, 99, E1130–E1136. [Google Scholar] [CrossRef]
- Soares, P.; Lima, J.; Preto, A.; Castro, P.; Vinagre, J.; Celestino, R.; Couto, J.P.; Prazeres, H.; Eloy, C.; Maximo, V.; et al. Genetic Alterations in Poorly Differentiated and Undifferentiated Thyroid Carcinomas. Curr. Genom. 2011, 12, 609–617. [Google Scholar] [CrossRef]
- Tavares, C.; Melo, M.; Cameselle-Teijeiro, J.M.; Soares, P.; Sobrinho-Simões, M. Endocrine tumours: Genetic predictors of thyroid cancer outcome. Eur. J. Endocrinol. 2016, 174, R117–R126. [Google Scholar] [CrossRef]
- Wreesmann, V.B.; Ghossein, R.A.; Patel, S.G.; Harris, C.P.; Schnaser, E.; Shaha, A.R.; Tuttle, R.M.; Shah, J.; Rao, P.H.; Singh, B. Genome-Wide Appraisal of Thyroid Cancer Progression. Am. J. Pathol. 2002, 161, 1549–1556. [Google Scholar] [CrossRef]
- Sisdelli, L.; Cordioli, M.; Vaisman, F.; Monte, O.; Longui, C.; Cury, A.; Freitas, M.; Rangel-Pozzo, A.; Mai, S.; Cerutti, J. A Multifocal Pediatric Papillary Thyroid Carcinoma (PTC) Harboring the AGK-BRAF and RET/PTC3 Fusion in a Mutually Exclusive Pattern Reveals Distinct Levels of Genomic Instability and Nuclear Organization. Biology 2021, 10, 125. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Pacini, F.; Castagna, M.G.; Brilli, L.; Pentheroudakis, G. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23, 110–119. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedus, L.; Paschke, R.; Valcavi, R.; Vitti, P. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules—2016 Update Appendix. Endocr. Pract. 2016, 22, 1–60. [Google Scholar] [CrossRef] [PubMed]
- Fresilli, D.; David, E.; Pacini, P.; Del Gaudio, G.; Dolcetti, V.; Lucarelli, G.; Di Leo, N.; Bellini, M.; D’Andrea, V.; Sorrenti, S.; et al. Thyroid Nodule Characterization: How to Assess the Malignancy Risk. Update of the Literature. Diagnostics 2021, 11, 1374. [Google Scholar] [CrossRef]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef]
- Cosgrove, D.; Barr, R.; Bojunga, J.; Cantisani, V.; Chammas, M.C.; Dighe, M.; Vinayak, S.; Xu, J.-M.; Dietrich, C.F. WFUMB Guidelines and Recommendations on the Clinical Use of Ultrasound Elastography: Part 4. Thyroid. Ultrasound Med. Biol. 2017, 43, 4–26. [Google Scholar] [CrossRef]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.-M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Ultrasound Elastography. Part 1: Basic Principles and Technology. Ultraschall Med. Eur. J. Ultrasound 2013, 34, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Xing, Z.; Liu, J.; Peng, Y.; Zhu, J.; Su, A. Diagnostic reliability of elastography in thyroid nodules reported as indeterminate at prior fine-needle aspiration cytology (FNAC): A systematic review and Bayesian meta-analysis. Eur. Radiol. 2020, 30, 6624–6634. [Google Scholar] [CrossRef] [PubMed]
- Ulisse, S.; Bosco, D.; Nardi, F.; Nesca, A.; D’Armiento, E.; Guglielmino, V.; DE Vito, C.; Sorrenti, S.; Pironi, D.; Tartaglia, F.; et al. Thyroid Imaging Reporting and Data System Score Combined with the New Italian Classification for Thyroid Cytology Improves the Clinical Management of Indeterminate Nodules. Int. J. Endocrinol. 2017, 2017, 1–8. [Google Scholar] [CrossRef]
- Gharib, H. Fine-Needle Aspiration Biopsy of Thyroid Nodules: Advantages, Limitations, and Effect. Mayo Clin. Proc. 1994, 69, 44–49. [Google Scholar] [CrossRef]
- Hamburger, J.I. Diagnosis of thyroid nodules by fine needle biopsy: Use and abuse. J. Clin. Endocrinol. Metab. 1994, 79, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Baloch, Z.W.; Sack, M.J.; Yu, G.H.; Livolsi, V.A.; Gupta, P.K. Fine-Needle Aspiration of Thyroid: An Institutional Experience. Thyroid 1998, 8, 565–569. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The Bethesda System for Reporting Thyroid Cytopathology. Am. J. Clin. Pathol. 2009, 132, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Melillo, R.M.; Santoro, M. Molecular Biomarkers in Thyroid FNA Samples. J. Clin. Endocrinol. Metab. 2012, 97, 4370–4373. [Google Scholar] [CrossRef][Green Version]
- Papale, F.; Cafiero, G.; Grimaldi, A.; Marino, G.; Rosso, F.; Mian, C.; Barollo, S.; Pennelli, G.; Sorrenti, S.; De Antoni, E.; et al. Galectin-3 expression in thyroid fine needle cytology (t-FNAC) uncertain cases: Validation of molecular markers and technology innovation. J. Cell. Physiol. 2013, 228, 968–974. [Google Scholar] [CrossRef]
- Jameson, J.L. Minimizing Unnecessary Surgery for Thyroid Nodules. N. Engl. J. Med. 2012, 367, 765–767. [Google Scholar] [CrossRef]
- Nikiforov, Y.E.; Steward, D.L.; Robinson-Smith, T.M.; Haugen, B.R.; Klopper, J.P.; Zhu, Z.; Fagin, J.A.; Falciglia, M.; Weber, K.; Nikiforova, M.N. Molecular Testing for Mutations in Improving the Fine-Needle Aspiration Diagnosis of Thyroid Nodules. J. Clin. Endocrinol. Metab. 2009, 94, 2092–2098. [Google Scholar] [CrossRef]
- Nikiforov, Y.E.; Ohori, N.P.; Hodak, S.P.; Carty, S.E.; Lebeau, S.O.; Ferris, R.; Yip, L.; Seethala, R.R.; Tublin, M.E.; Stang, M.T.; et al. Impact of Mutational Testing on the Diagnosis and Management of Patients with Cytologically Indeterminate Thyroid Nodules: A Prospective Analysis of 1056 FNA Samples. J. Clin. Endocrinol. Metab. 2011, 96, 3390–3397. [Google Scholar] [CrossRef]
- Alexander, E.K.; Kennedy, G.C.; Baloch, Z.W.; Cibas, E.S.; Chudova, D.; Diggans, J.; Friedman, L.; Kloos, R.T.; Livolsi, V.A.; Mandel, S.J.; et al. Preoperative Diagnosis of Benign Thyroid Nodules with Indeterminate Cytology. N. Engl. J. Med. 2012, 367, 705–715. [Google Scholar] [CrossRef]
- Ohori, N.P. Molecular testing and thyroid nodule management in North America. Gland. Surg. 2020, 9, 1628–1638. [Google Scholar] [CrossRef] [PubMed]
- Schumm, M.A.; Nguyen, D.T.; Kim, J.; Tseng, C.-H.; Chow, A.Y.; Shen, N.; Livhits, M.J. Longitudinal Assessment of Quality of Life Following Molecular Testing for Indeterminate Thyroid Nodules. Ann. Surg. Oncol. 2021. [Google Scholar] [CrossRef]
- Medas, F.; Canu, G.L.; Cappellacci, F.; Boi, F.; Lai, M.L.; Erdas, E.; Calò, P.G. Predictive Factors of Lymph Node Metastasis in Patients with Papillary Microcarcinoma of the Thyroid: Retrospective Analysis on 293 Cases. Front. Endocrinol. 2020, 11, 551. [Google Scholar] [CrossRef] [PubMed]
- Stack, B.C.; Ferris, R.L.; Goldenberg, D.; Haymart, M.; Shaha, A.; Sheth, S.; Sosa, J.A.; Ralph, P. Tufano, for the American Thyroid Association Surgical Affairs Committee. American Thyroid Association Consensus Review and Statement Regarding the Anatomy, Terminology, and Rationale for Lateral Neck Dissection in Differentiated Thyroid Cancer. Thyroid 2012, 22, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Florentine, B.D.; Staymates, B.; Rabadi, M.; Barstis, J.; Black, A. Cancer Committee of the Henry Mayo Newhall Memorial Hospital: The reliability of fine-needle aspiration biopsy as the initial diagnostic procedure for palpable masses: A 4-year expe-rience of 730 patients from a community hospital-based outpatient aspiration biopsy clinic. Cancer 2006, 107, 406–416. [Google Scholar]
- Cignarelli, M.; Triggiani, V.; Ciampolillo, A.; Ambrosi, A.; Giorgino, F.; Liso, V.; Giorgino, R. High Frequency of Incidental Diagnosis of Extrathyroidal Neoplastic Diseases at the Fine-Needle Aspiration Biopsy of Laterocervical Lymph Nodes in Patients with Thyroid Nodules. Thyroid 2001, 11, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Üstün, M.; Risberg, B.; Davidson, B.; Berner, A. Cystic change in metastatic lymph nodes: A common diagnostic pitfall in fine-needle aspiration cytology. Diagn. Cytopathol. 2002, 27, 387–392. [Google Scholar] [CrossRef]
- Kessler, A.; Rappaport, Y.; Blank, A.; Marmor, S.; Weiss, J.; Graif, M. Cystic appearance of cervical lymph nodes is characteristic of metastatic papillary thyroid carcinoma. J. Clin. Ultrasound 2003, 1, 21–25. [Google Scholar] [CrossRef]
- Pacini, F.; Fugazzola, L.; Lippi, F.; Ceccarelli, C.; Centoni, R.; Miccoli, P.; Elisei, R.; Pinchera, A. Detection of thyroglobulin in fine needle aspirates of nonthyroidal neck masses: A clue to the diagnosis of metastatic differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 1992, 74, 1401–1404. [Google Scholar] [CrossRef] [PubMed]
- Frasoldati, A.; Toschi, E.; Zini, M.; Flora, M.; Caroggio, A.; Dotti, C.; Valcavi, R. Role of Thyroglobulin Measurement in Fine-Needle Aspiration Biopsies of Cervical Lymph Nodes in Patients with Differentiated Thyroid Cancer. Thyroid 1999, 9, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Cignarelli, M.; Ambrosi, A.; Marino, A.; Lamacchia, O.; Campo, M.; Picca, G.; Giorgino, F. Diagnostic Utility of Thyroglobulin Detection in Fine-Needle Aspiration of Cervical Cystic Metastatic Lymph Nodes from Papillary Thyroid Cancer with Negative Cytology. Thyroid 2003, 13, 1163–1167. [Google Scholar] [CrossRef] [PubMed]
- Borel, A.-L.; Boizel, R.; Faure, P.; Barbe, G.; Boutonnat, J.; Sturm, N.; Seigneurin, D.; Bricault, I.; Caravel, J.-P.; Chaffanjon, P.; et al. Significance of low levels of thyroglobulin in fine needle aspirates from cervical lymph nodes of patients with a history of differentiated thyroid cancer. Eur. J. Endocrinol. 2008, 158, 691–698. [Google Scholar] [CrossRef]
- Cunha, N.; Rodrigues, F.; Curado, F.; Ilhéu, O.; Cruz, C.; Naidenov, P.; Rascão, M.J.; Ganho, J.; Gomes, I.; Pereira, H.; et al. Thyroglobulin detection in fine-needle aspirates of cervical lymph nodes: A technique for the diagnosis of metastatic differentiated thyroid cancer. Eur. J. Endocrinol. 2007, 157, 101–107. [Google Scholar] [CrossRef]
- Kim, D.W.; Jeon, S.J.; Kim, C.G. Usefulness of thyroglobulin measurement in needle-washout of fine-needle aspiration biopsy for the diagnosis of cervical lymph node metastases from papillary thyroid cancer before thyroidectomy. Endocrine 2012, 42, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Baldini, E.; Sorrenti, S.; Di Gioia, C.; De Vito, C.; Antonelli, A.; Gnessi, L.; Carbotta, G.; D’Armiento, E.; Miccoli, P.; De Antoni, E.; et al. Cervical lymph node metastases from thyroid cancer: Does thyroglobulin and calcitonin measurement in fine needle aspirates improve the diagnostic value of cytology? BMC Clin. Pathol. 2013, 13, 7. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Materazzi, G.; Bakkar, S.; Miccoli, P. Recent Trends in Surgical Approach to Thyroid Cancer. Front. Endocrinol. 2021, 12, 699805. [Google Scholar] [CrossRef]
- Medas, F.; Canu, G.L.; Cappellacci, F.; Anedda, G.; Conzo, G.; Erdas, E.; Calò, P.G. Prophylactic Central Lymph Node Dissection Improves Disease-Free Survival in Patients with Intermediate and High Risk Differentiated Thyroid Carcinoma: A Retrospective Analysis on 399 Patients. Cancers 2020, 12, 1658. [Google Scholar] [CrossRef]
- Canu, G.L.; Medas, F.; Podda, F.; Tatti, A.; Pisano, G.; Erdas, E.; Calò, P.G. Thyroidectomy with energy-based devices: Surgical outcomes and complications—Comparison between Harmonic Focus, LigaSure Small Jaw and Thunderbeat Open Fine Jaw. Gland. Surg. 2020, 9, 721–726. [Google Scholar] [CrossRef]
- Miccoli, P.; Berti, P.; Conte, M.; Bendinelli, C.; Marcocci, C. Minimally invasive surgery for thyroid small nodules: Preliminary report. J. Endocrinol. Investig. 1999, 22, 849–851. [Google Scholar] [CrossRef]
- Miccoli, P.; Fregoli, L.; Rossi, L.; Papini, P.; Ambrosini, C.E.; Bakkar, S.; De Napoli, L.; Aghababyan, A.; Matteucci, V.; Materazzi, G. Minimally invasive video-assisted thyroidectomy (MIVAT). Gland. Surg. 2020, 9, S1–S5. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-W.; Jeong, J.J.; Yun, J.-S.; Sung, T.Y.; Lee, S.C.; Lee, Y.S.; Nam, K.-H.; Chang, H.-S.; Chung, W.Y.; Park, C.S. Gasless Endoscopic Thyroidectomy Using Trans-axillary Approach; Surgical Outcome of 581 Patients. Endocr. J. 2009, 56, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Jongekkasit, I.; Jitpratoom, P.; Sasanakietkul, T.; Anuwong, A. Transoral Endoscopic Thyroidectomy for Thyroid Cancer. Endocrinol. Metab. Clin. N. Am. 2019, 48, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Haddad, R.I.; Nasr, C.; Bischoff, L.; Busaidy, N.L.; Byrd, D.; Callender, G.; Dickson, P.; Duh, Q.-Y.; Ehya, H.; Goldner, W.; et al. NCCN Guidelines Insights: Thyroid Carcinoma, Version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 1429–1440. [Google Scholar] [CrossRef]
- American Thyroid Association Guidelines Taskforce on Thyroid; Cooper, D.S.; Doherty, G.; Haugen, B.R.; Kloos, R.T.; Lee, S.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; et al. Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef]
- Cocuzza, S.; Di Luca, M.; Maniaci, A.; Russo, M.; Di Mauro, P.; Migliore, M.; Serra, A.; Spinato, G. Precision treatment of post pneumonectomy unilateral laryngeal paralysis due to cancer. Future Oncol. 2020, 16, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Grani, G.; Durante, C.; Borget, I.; Filetti, S.; Schlumberger, M. Follow-up of differentiated thyroid cancer—What should (and what should not) be done. Nat. Rev. Endocrinol. 2018, 14, 538–551. [Google Scholar] [CrossRef] [PubMed]
- Fullmer, T.; Cabanillas, M.E.; Zafereo, M. Novel Therapeutics in Radioactive Iodine-Resistant Thyroid Cancer. Front. Endocrinol. 2021, 12, 720723. [Google Scholar] [CrossRef]
- Al-Jundi, M.; Thakur, S.; Gubbi, S.; Klubo-Gwiezdzinska, J. Novel Targeted Therapies for Metastatic Thyroid Cancer—A Comprehensive Review. Cancers 2020, 12, 2104. [Google Scholar] [CrossRef]
- Fallahi, P.; Ruffilli, I.; Elia, G.; Ragusa, F.; Ulisse, S.; Baldini, E.; Miccoli, M.; Materazzi, G.; Antonelli, A.; Ferrari, S.M. Novel treatment options for anaplastic thyroid cancer. Expert Rev. Endocrinol. Metab. 2017, 12, 279–288. [Google Scholar] [CrossRef]
- Ferrari, S.M.; Bocci, G.; Di Desidero, T.; Ruffilli, I.; Elia, G.; Ragusa, F.; Fioravanti, A.; Orlandi, P.; Paparo, S.R.; Patrizio, A.; et al. Vandetanib has antineoplastic activity in anaplastic thyroid cancer, in vitro and in vivo. Oncol. Rep. 2018, 39, 2306–2314. [Google Scholar] [CrossRef]
- Ferrari, S.M.; Bocci, G.; Di Desidero, T.; Elia, G.; Ruffilli, I.; Ragusa, F.; Orlandi, P.; Paparo, S.R.; Patrizio, A.; Piaggi, S.; et al. Lenvatinib exhibits antineoplastic activity in anaplastic thyroid cancer in vitro and in vivo. Oncol. Rep. 2018, 39, 2225–2234. [Google Scholar] [CrossRef]
- Ferrari, S.M.; La Motta, C.; Elia, G.; Ragusa, F.; Ruffilli, I.; Quattrini, L.; Paparo, S.R.; Piaggi, S.; Patrizio, A.; Ulisse, S.; et al. Antineoplastic Effect of Lenvatinib and Vandetanib in Primary Anaplastic Thyroid Cancer Cells Obtained from Biopsy or Fine Needle Aspiration. Front. Endocrinol. 2018, 9, 764. [Google Scholar] [CrossRef]
- Ferrari, S.M.; Politti, U.; Spisni, R.; Materazzi, G.; Baldini, E.; Ulisse, S.; Miccoli, P.; Antonelli, A.; Fallahi, P. Sorafenib in the treatment of thyroid cancer. Expert Rev. Anticancer Ther. 2015, 15, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Asghar, M.Y.; Lassila, T.; Paatero, I.; Nguyen, V.D.; Kronqvist, P.; Zhang, J.; Slita, A.; Löf, C.; Zhou, Y.; Rosenholm, J.; et al. Stromal interaction molecule 1 (STIM1) knock down attenuates invasion and proliferation and enhances the expression of thyroid-specific proteins in human follicular thyroid cancer cells. Cell. Mol. Life Sci. 2021, 78, 5827–5846. [Google Scholar] [CrossRef]
- Lang, B.; Lo, C.-Y.; Chan, W.-F.; Lam, A.; Wan, K.-Y. Staging Systems for Papillary Thyroid Carcinoma. Ann. Surg. 2007, 245, 366–378. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Alzahrani, A.S. Risk Stratification in Differentiated Thyroid Cancer: From Detection to Final Follow-Up. J. Clin. Endocrinol. Metab. 2019, 104, 4087–4100. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Sorrenti, S.; Carbotta, G.; Di Matteo, F.M.; Catania, A.; Pironi, D.; Tartaglia, F.; Tarroni, D.; Gagliardi, F.; Tripodi, D.; Watanabe, M.; et al. Evaluation of Clinicopathological and Molecular Parameters on Disease Recurrence of Papillary Thyroid Cancer Patient: A Retrospective Observational Study. Cancers 2020, 12, 3637. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Tala, H.; Shah, J.; Leboeuf, R.; Ghossein, R.; Gonen, M.; Brokhin, M.; Omry, G.; Fagin, J.A.; Shaha, A. Estimating Risk of Recurrence in Differentiated Thyroid Cancer After Total Thyroidectomy and Radioactive Iodine Remnant Ablation: Using Response to Therapy Variables to Modify the Initial Risk Estimates Predicted by the New American Thyroid Association Staging System. Thyroid 2010, 20, 1341–1349. [Google Scholar] [CrossRef]
- Castagna, M.G.; Maino, F.; Cipri, C.; Belardini, V.; Theodoropoulou, A.; Cevenini, G.; Pacini, F. Delayed risk stratification, to include the response to initial treatment (surgery and radioiodine ablation), has better outcome predictivity in differentiated thyroid cancer patients. Eur. J. Endocrinol. 2011, 165, 441–446. [Google Scholar] [CrossRef]
- Lamartina, L.; Grani, G.; Arvat, E.; Nervo, A.; Zatelli, M.C.; Rossi, R.; Puxeddu, E.; Morelli, S.; Torlontano, M.; Massa, M.; et al. 8th edition of the AJCC/TNM staging system of thyroid cancer: What to expect (ITCO#2). Endocr. Relat. Cancer 2018, 25, L7–L11. [Google Scholar] [CrossRef]
- Grani, G.; Zatelli, M.C.; Alfò, M.; Montesano, T.; Torlontano, M.; Morelli, S.; Deandrea, M.; Antonelli, A.; Francese, C.; Ceresini, G.; et al. Real-World Performance of the American Thyroid Association Risk Estimates in Predicting 1-Year Differentiated Thyroid Cancer Outcomes: A Prospective Multicenter Study of 2000 Patients. Thyroid 2021, 31, 264–271. [Google Scholar] [CrossRef]
- Kim, M.; Kim, W.B.; Oh, H.-S.; Park, S.; Kwon, H.; Song, D.E.; Kim, T.Y.; Shong, Y.K.; Sung, T.-Y.; Jeon, M.J. Comparison of the Seventh and Eighth Editions of the American Joint Committee on Cancer/Union for International Cancer Control Tumor-Node-Metastasis Staging System for Differentiated Thyroid Cancer. Thyroid 2017, 27, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, H.I.; Jeon, M.J.; Kim, H.K.; Kim, E.H.; Yi, H.-S.; Kim, E.S.; Kim, H.; Kim, B.H.; Kim, T.Y.; et al. Eighth edition of tumor-node-metastasis staging system improve survival predictability for papillary, but not follicular thyroid carcinoma: A multicenter cohort study. Oral Oncol. 2018, 87, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Medas, F.; Canu, G.L.; Boi, F.; Lai, M.L.; Erdas, E.; Calò, P.G. Predictive Factors of Recurrence in Patients with Differentiated Thyroid Carcinoma: A Retrospective Analysis on 579 Patients. Cancers 2019, 11, 1230. [Google Scholar] [CrossRef]
- Shteinshnaider, M.; Kalmovich, L.M.; Koren, S.; Limor, M.K.; Cantrell, D.; Benbassat, C. Reassessment of Differentiated Thyroid Cancer Patients Using the Eighth TNM/AJCC Classification System: A Comparative Study. Thyroid 2018, 28, 201–209. [Google Scholar] [CrossRef]
- Zheng, D.; Trynda, J.; Williams, C.; Vold, J.A.; Nguyen, J.H.; Harnois, D.M.; Bagaria, S.P.; McLaughlin, S.A.; Li, Z. Sexual dimorphism in the incidence of human cancers. BMC Cancer 2019, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Radkiewicz, C.; Johansson, A.L.; Dickman, P.W.; Lambe, M.; Edgren, G. Sex differences in cancer risk and survival: A Swedish cohort study. Eur. J. Cancer 2017, 84, 130–140. [Google Scholar] [CrossRef]
- Micheli, A.; Ciampichini, R.; Oberaigner, W.; Ciccolallo, L.; de Vries, E.; Izarzugaza, I.; Zambon, P.; Gatta, G.; De Angelis, R. The advantage of women in cancer survival: An analysis of EUROCARE-4 data. Eur. J. Cancer 2009, 45, 1017–1027. [Google Scholar] [CrossRef]
- Guo, K.; Wang, Z. Risk factors influencing the recurrence of papillary thyroid carcinoma: A systematic review and meta-analysis. Int. J. Clin. Exp. Pathol. 2014, 7, 5393–5403. [Google Scholar]
- Ding, J.; Wu, W.; Fang, J.; Zhao, J.; Jiang, L. Male sex is associated with aggressive behaviour and poor prognosis in Chinese papillary thyroid carcinoma. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Kim, M.J.; Lee, S.G.; Kim, K.; Lee, C.R.; Kang, S.-W.; Lee, J.; Nam, K.-H.; Chung, W.Y.; Jeong, J.J. Current trends in the features of male thyroid cancer. Medicine 2019, 98, e15559. [Google Scholar] [CrossRef] [PubMed]
- De Castro, T.P.; Waissmann, W.; Simões, T.C.; De Mello, R.C.R.; Carvalho, D.P. Predictors for papillary thyroid cancer persistence and recurrence: A retrospective analysis with a 10-year follow-up cohort study. Clin. Endocrinol. 2016, 85, 466–474. [Google Scholar] [CrossRef]
- Elisei, R.; Molinaro, E.; Agate, L.; Bottici, V.; Masserini, L.; Ceccarelli, C.; Lippi, F.; Grasso, L.; Basolo, F.; Bevilacqua, G.; et al. Are the Clinical and Pathological Features of Differentiated Thyroid Carcinoma Really Changed over the Last 35 Years? Study on 4187 Patients from a Single Italian Institution to Answer this Question. J. Clin. Endocrinol. Metab. 2010, 95, 1516–1527. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Lim, J.A.; Ahn, H.Y.; Cho, S.W.; Lee, K.E.; Kim, K.W.; Yi, K.H.; Sung, M.-W.; Youn, Y.-K.; Chung, J.-K.; et al. Secular trends in the prognostic factors for papillary thyroid cancer. Eur. J. Endocrinol. 2014, 171, 667–675. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lee, Y.H.; Sung, T.Y.; Yoon, J.H.; Song, D.E.; Kim, T.Y.; Baek, J.H.; Ryu, J.S.; Chung, K.W.; Hong, S.J. Is Male Gender a Prognostic Factor for Papillary Thyroid Microcarcinoma? Ann. Surg. Oncol. 2017, 24, 1958–1964. [Google Scholar] [CrossRef]
- Park, J.; Kim, K.; Lim, D.-J.; Bae, J.S.; Kim, J.S. Male sex is not an independent risk factor for recurrence of differentiated thyroid cancer: A propensity score-matching study. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Falvo, L.; Catania, A.; Sorrenti, S.; D’Andrea, V.; Berni, A.; De Stefano, M.; De Antoni, E. Prognostic significance of the age factor in the thyroid cancer: Statistical analysis. J. Surg. Oncol. 2004, 88, 217–222. [Google Scholar] [CrossRef]
- Boi, F.; Lai, M.L.; Marziani, B.; Minerba, L.; Faa, G.; Mariotti, S. High prevalence of suspicious cytology in thyroid nodules associated with positive thyroid autoantibodies. Eur. J. Endocrinol. 2005, 153, 637–642. [Google Scholar] [CrossRef]
- Fiore, E.; Rago, T.; Latrofa, F.; Provenzale, M.A.; Piaggi, P.; Delitala, A.; Scutari, M.; Basolo, F.; Di Coscio, G.; Grasso, L.; et al. Hashimoto’s thyroiditis is associated with papillary thyroid carcinoma: Role of TSH and of treatment with l-thyroxine. Endocr. Relat. Cancer 2011, 18, 429–437. [Google Scholar] [CrossRef]
- Boi, F.; Minerba, L.; Lai, M.L.; Marziani, B.; Figus, B.; Spanu, F.; Borghero, A.; Mariotti, S. Both thyroid autoimmunity and increased serum TSH are independent risk factors for malignancy in patients with thyroid nodules. J. Endocrinol. Investig. 2013, 36, 313–320. [Google Scholar] [CrossRef]
- Antonelli, A.; Ferrari, S.M.; Corrado, A.; Di Domenicantonio, A.; Fallahi, P. Autoimmune thyroid disorders. Autoimmun. Rev. 2015, 14, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Chung, H.S.; Yu, J.M.; Yoo, H.J.; Park, J.H.; Kim, D.S.; Park, Y.J. Associations between Hashimoto Thyroiditis and Clinical Outcomes of Papillary Thyroid Cancer: A Meta-Analysis of Observational Studies. Endocrinol. Metab. 2018, 33, 473–484. [Google Scholar] [CrossRef]
- Lee, I.; Kim, H.K.; Soh, E.Y.; Lee, J. The Association Between Chronic Lymphocytic Thyroiditis and the Progress of Papillary Thyroid Cancer. World J. Surg. 2020, 44, 1506–1513. [Google Scholar] [CrossRef]
- Ragusa, F.; Fallahi, P.; Elia, G.; Gonnella, D.; Paparo, S.R.; Giusti, C.; Churilov, L.P.; Ferrari, S.M.; Antonelli, A. Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101367. [Google Scholar] [CrossRef] [PubMed]
- Song, E.; Oh, H.-S.; Jeon, M.J.; Chung, K.W.; Hong, S.J.; Ryu, J.S.; Baek, J.H.; Lee, J.H.; Kim, W.G.; Kim, W.B.; et al. The value of preoperative antithyroidperoxidase antibody as a novel predictor of recurrence in papillary thyroid carcinoma. Int. J. Cancer 2018, 144, 1414–1420. [Google Scholar] [CrossRef] [PubMed]
- Myshunina, T.M.; Guda, B.D.; Bolgov, M.Y.; Mikhailenko, N.I.; Tronko, N.D. Differentiated Thyroid Carcinomas Associated with Chronic Thyroiditis: Biological and Clinical Properties. Exp. Oncol. 2018, 40, 128–131. [Google Scholar] [CrossRef]
- Zitvogel, L.; Perreault, C.; Finn, O.J.; Kroemer, G. Beneficial autoimmunity improves cancer prognosis. Nat. Rev. Clin. Oncol. 2021, 18, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Prinzi, N.; Sorrenti, S.; Baldini, E.; DE Vito, C.; Tuccilli, C.; Catania, A.; Coccaro, C.; Bianchini, M.; Nesca, A.; Grani, G.; et al. Association of Thyroid Diseases with Primary Extra-Thyroidal Malignancies in Women: Results of a Cross-Sectional Study of 6,386 Patients. PLoS ONE 2015, 10, e0122958. [Google Scholar] [CrossRef] [PubMed]
- Prinzi, N.; Baldini, E.; Sorrenti, S.; DE Vito, C.; Tuccilli, C.; Catania, A.; Carbotta, S.; Mocini, R.; Coccaro, C.; Nesca, A.; et al. Prevalence of breast cancer in thyroid diseases: Results of a cross-sectional study of 3,921 patients. Breast Cancer Res. Treat. 2014, 144, 683–688. [Google Scholar] [CrossRef]
- Shi, X.; Liu, R.; Basolo, F.; Giannini, R.; Shen, X.; Teng, D.; Guan, H.; Shan, Z.; Teng, W.; Musholt, T.J.; et al. Differential Clinicopathological Risk and Prognosis of Major Papillary Thyroid Cancer Variants. J. Clin. Endocrinol. Metab. 2016, 101, 264–274. [Google Scholar] [CrossRef]
- Choi, W.R.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Multifocality of papillary thyroid carcinoma as a risk factor for disease recurrence. Oral Oncol. 2019, 94, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Ryu, Y.J.; Cho, J.S.; Yoon, J.H.; Park, M.H. Identifying risk factors for recurrence of papillary thyroid cancer in patients who underwent modified radical neck dissection. World J. Surg. Oncol. 2018, 16, 205. [Google Scholar] [CrossRef]
- Nam, S.H.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Nodal Factors Predictive of Recurrence After Thyroidectomy and Neck Dissection for Papillary Thyroid Carcinoma. Thyroid 2018, 28, 88–95. [Google Scholar] [CrossRef]
- Kim, Y.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Risk Factors for Lateral Neck Recurrence of N0/N1a Papillary Thyroid Cancer. Ann. Surg. Oncol. 2017, 24, 3609–3616. [Google Scholar] [CrossRef]
- Khan, M.; Syed, A.A.; Khan, A.I.; Hussain, S.R.; Urooj, N. Association of tumor size and focality with recurrence/persistence in papillary thyroid cancer patients treated with total thyroidectomy along with radioactive-iodine ablation and TSH suppression. Updates Surg. 2017, 70, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Li, D.; Wang, H.; Yang, X.; Yu, Y.; Gao, M. Multifocality predicts poor outcome of patients with insular thyroid cancer: A clinicopathological study. Int. J. Clin. Exp. Pathol. 2015, 8, 11212–11217. [Google Scholar]
- Geron, Y.; Benbassat, C.; Shteinshneider, M.; Or, K.; Markus, E.; Hirsch, D.; Levy, S.; Ziv-Baran, T.; Muallem-Kalmovich, L. Multifocality Is not an Independent Prognostic Factor in Papillary Thyroid Cancer: A Propensity Score–Matching Analysis. Thyroid 2019, 29, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Yu, X.; Shen, X.; Zhu, G.; Huang, Y.; Liu, R.; Viola, D.; Elisei, R.; Puxeddu, E.; Fugazzola, L.; et al. The Prognostic Value of Tumor Multifocality in Clinical Outcomes of Papillary Thyroid Cancer. J. Clin. Endocrinol. Metab. 2017, 102, 3241–3250. [Google Scholar] [CrossRef]
- Li, L.Q.; Hey, S.Y.; Andreeva, D.; Tornari, C.; Sawant, R.; Harding, N.E.; Adamson, R.; Hay, A.; Simo, R.; Nixon, I.J. A UK based two-centre review of multifocality and its role in the treatment of papillary thyroid cancer. Eur. J. Surg. Oncol. (EJSO) 2021. [Google Scholar] [CrossRef] [PubMed]
- Shaha, A.R.; Poorten, V.V.; Tuttle, R.M. Multifocality in papillary thyroid carcinoma—An unresolved controversy. Eur. J. Surg. Oncol. (EJSO) 2020, 46, 1777–1778. [Google Scholar] [CrossRef]
- Cao, J.; Hu, J.-L.; Chen, C.; Wang, Q.-L.; Fang, X.-H.; Zhang, Y.; Ge, M.-H. Vascular invasion is an independent prognostic factor for distant recurrence-free survival in papillary thyroid carcinoma: A matched-case comparative study. J. Clin. Pathol. 2016, 69, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Furlan, J.C.; Bedard, Y.C.; Rosen, I.B. Clinicopathologic significance of histologic vascular invasion in papillary and follicular thyroid carcinomas1 1No competing interests declared. J. Am. Coll. Surg. 2004, 198, 341–348. [Google Scholar] [CrossRef]
- Kim, H.J.; Sung, J.-Y.; Oh, Y.L.; Kim, J.H.; Son, Y.-I.; Min, Y.-K.; Kim, S.W.; Chung, J.H. Association of vascular invasion with increased mortality in patients with minimally invasive follicular thyroid carcinoma but not widely invasive follicular thyroid carcinoma. Head Neck 2014, 36, 1695–1700. [Google Scholar] [CrossRef]
- Collini, P.; Sampietro, G.; Pilotti, S. Extensive vascular invasion is a marker of risk of relapse in encapsulated non-Hurthle cell follicular carcinoma of the thyroid gland: A clinicopathological study of 18 consecutive cases from a single institution with a 11-year median follow-up. Histopathology 2004, 44, 35–39. [Google Scholar] [CrossRef]
- Falvo, L.; Catania, A.; D’Andrea, V.; Marzullo, A.; Giustiniani, M.C.; De Antoni, E. Prognostic Importance of Histologic Vascular Invasion in Papillary Thyroid Carcinoma. Ann. Surg. 2005, 241, 640–646. [Google Scholar] [CrossRef]
- Vuong, H.G.; Kondo, T.; Duong, U.N.; Pham, T.Q.; Oishi, N.; Mochizuki, K.; Nakazawa, T.; Hassell, L.; Katoh, R. Prognostic impact of vascular invasion in differentiated thyroid carcinoma: A systematic review and meta-analysis. Eur. J. Endocrinol. 2017, 177, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.-K.; Lee, S.; Kim, S.-J.; Jee, H.-G.; Kim, B.-A.; Cho, H.; Song, Y.S.; Cho, S.W.; Won, J.-K.; Shin, J.-Y.; et al. Comprehensive Analysis of the Transcriptional and Mutational Landscape of Follicular and Papillary Thyroid Cancers. PLoS Genet. 2016, 12, e1006239. [Google Scholar] [CrossRef]
- Soares, P.; Póvoa, A.A.; Melo, M.; Vinagre, J.; Máximo, V.; Eloy, C.; Cameselle-Teijeiro, J.M.; Sobrinho-Simões, M. Molecular Pathology of Non-familial Follicular Epithelial–Derived Thyroid Cancer in Adults: From RAS/BRAF-like Tumor Designations to Molecular Risk Stratification. Endocr. Pathol. 2021, 32, 44–62. [Google Scholar] [CrossRef] [PubMed]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio Cancer Genomics Portal: An Open Platform for Exploring Multidimensional Cancer Genomics Data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative Analysis of Complex Cancer Genomics and Clinical Profiles Using the cBioPortal. Sci. Signal. 2013, 6, 11. [Google Scholar] [CrossRef]
- Xing, M. BRAF Mutation in Papillary Thyroid Cancer: Pathogenic Role, Molecular Bases, and Clinical Implications. Endocr. Rev. 2007, 28, 742–762. [Google Scholar] [CrossRef]
- Handkiewicz-Junak, D.; Czarniecka, A.; Jarząb, B. Molecular prognostic markers in papillary and follicular thyroid cancer: Current status and future directions. Mol. Cell. Endocrinol. 2010, 322, 8–28. [Google Scholar] [CrossRef]
- Shibru, D.; Chung, K.-W.; Kebebew, E. Recent developments in the clinical application of thyroid cancer biomarkers. Curr. Opin. Oncol. 2008, 20, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.N.; Yip, L.; Lubitz, C.C.; Grubbs, E.G.; Miller, B.S.; Shen, W.; Angelos, P.; Chen, H.; Doherty, G.M.; Fahey, T.J.; et al. The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults. Ann. Surg. 2020, 271, e21–e93. [Google Scholar] [CrossRef]
- Melo, M.; da Rocha, A.G.; Vinagre, J.; Sobrinho-Simões, M.; Soares, P. Coexistence of TERT Promoter and BRAF Mutations in Papillary Thyroid Carcinoma: Added Value in Patient Prognosis? J. Clin. Oncol. 2015, 33, 667–668. [Google Scholar] [CrossRef]
- Huang, Y.; Qu, S.; Zhu, G.; Wang, F.; Liu, R.; Shen, X.; Viola, D.; Elisei, R.; Puxeddu, E.; Fugazzola, L.; et al. BRAF V600E Mutation-Assisted Risk Stratification of Solitary Intrathyroidal Papillary Thyroid Cancer for Precision Treatment. J. Natl. Cancer Inst. 2018, 110, 362–370. [Google Scholar] [CrossRef]
- Li, F.; Chen, G.; Sheng, C.; Gusdon, A.M.; Huang, Y.; Lv, Z.; Xu, H.; Xing, M.; Qu, S. BRAFV600E mutation in papillary thyroid microcarcinoma: A meta-analysis. Endocr. Relat. Cancer 2015, 22, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Shong, Y.K.; Kim, T.Y.; Viola, D.; Elisei, R.; Bendlová, B.; Yip, L.; Mian, C.; et al. Association Between BRAF V600E Mutation and Recurrence of Papillary Thyroid Cancer. J. Clin. Oncol. 2015, 33, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Ulisse, S.; Baldini, E.; Sorrenti, S.; Barollo, S.; Prinzi, N.; Catania, A.; Nesca, A.; Gnessi, L.; Pelizzo, M.R.; Mian, C.; et al. In papillary thyroid carcinoma BRAFV600Eis associated with increased expression of the urokinase plasminogen activator and its cognate receptor, but not with disease-free interval. Clin. Endocrinol. 2012, 77, 780–786. [Google Scholar] [CrossRef]
- Vuong, H.G.; Duong, U.N.; Altibi, A.M.; Ngo, H.T.; Pham, T.Q.; Tran, H.M.; Gandolfi, G.; Hassell, L. A meta-analysis of prognostic roles of molecular markers in papillary thyroid carcinoma. Endocr. Connect. 2017, 6, R8–R17. [Google Scholar] [CrossRef]
- Ito, Y.; Yoshida, H.; Maruo, R.; Morita, S.; Takano, T.; Hirokawa, M.; Yabuta, T.; Fukushima, M.; Inoue, H.; Tomoda, C.; et al. BRAF Mutation in Papillary Thyroid Carcinoma in a Japanese Population: Its Lack of Correlation with High-Risk Clinicopathological Features and Disease-Free Survival of Patients. Endocr. J. 2009, 56, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Soares, P.; Celestino, R.; Melo, M.; Fonseca, E.; Sobrinho-Simões, M. Prognostic biomarkers in thyroid cancer. Virchows Archiv 2014, 464, 333–346. [Google Scholar] [CrossRef]
- Czarniecka, A.; Oczko-Wojciechowska, M.; Barczyński, M. BRAF V600E mutation in prognostication of papillary thyroid cancer (PTC) recurrence. Gland. Surg. 2016, 5, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Pacini, F.; Cantara, S.; Capezzone, M.; Marchisotta, S. Telomerase and the endocrine system. Nat. Rev. Endocrinol. 2011, 7, 420–430. [Google Scholar] [CrossRef]
- Vinagre, J.; Almeida, A.; Pópulo, H.; Batista, R.; Lyra, J.; Pinto, V.; Coelho, R.; Celestino, R.; Prazeres, H.; Lima, L.; et al. Frequency of TERT promoter mutations in human cancers. Nat. Commun. 2013, 4, 2185. [Google Scholar] [CrossRef]
- Heidenreich, B.; Rachakonda, S.; Hemminki, K.; Kumar, R. TERT promoter mutations in cancer development. Curr. Opin. Genet. Dev. 2014, 24, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Xing, M. Genetic-guided Risk Assessment and Management of Thyroid Cancer. Endocrinol. Metab. Clin. N. Am. 2019, 48, 109–124. [Google Scholar] [CrossRef]
- Liu, R.; Xing, M. TERT promoter mutations in thyroid cancer. Endocr. Relat. Cancer 2016, 23, R143–R155. [Google Scholar] [CrossRef] [PubMed]
- Sohn, S.Y.; Park, W.-Y.; Shin, H.T.; Bae, J.S.; Ki, C.-S.; Oh, Y.L.; Kim, S.W.; Chung, J.H. Highly Concordant Key Genetic Alterations in Primary Tumors and Matched Distant Metastases in Differentiated Thyroid Cancer. Thyroid 2016, 26, 672–682. [Google Scholar] [CrossRef]
- Bu, R.; Siraj, A.K.; Divya, S.P.; Kong, Y.; Parvathareddy, S.K.; Al-Rasheed, M.; Al Obaisi, K.A.S.; Victoria, I.G.; Al-Sobhi, S.S.; Al-Dawish, M.; et al. Telomerase reverse transcriptase mutations are independent predictor of disease-free survival in Middle Eastern papillary thyroid cancer. Int. J. Cancer 2017, 142, 2028–2039. [Google Scholar] [CrossRef]
- Xing, M.; Liu, R.; Liu, X.; Murugan, A.K.; Zhu, G.; Zeiger, M.A.; Pai, S.; Bishop, J. BRAF V600E and TERT Promoter Mutations Cooperatively Identify the Most Aggressive Papillary Thyroid Cancer with Highest Recurrence. J. Clin. Oncol. 2014, 32, 2718–2726. [Google Scholar] [CrossRef]
- Jin, L.; Chen, E.; Dong, S.; Cai, Y.; Zhang, X.; Zhou, Y.; Zeng, R.; Yang, F.; Pan, C.; Liu, Y.; et al. BRAF and TERT promoter mutations in the aggressiveness of papillary thyroid carcinoma: A study of 653 patients. Oncotarget 2016, 7, 18346–18355. [Google Scholar] [CrossRef] [PubMed]
- Landa, I.; Ganly, I.; Chan, T.A.; Mitsutake, N.; Matsuse, M.; Ibrahimpasic, T.; Ghossein, R.A.; Fagin, J.A. Frequent Somatic TERT Promoter Mutations in Thyroid Cancer: Higher Prevalence in Advanced Forms of the Disease. J. Clin. Endocrinol. Metab. 2013, 98, E1562–E1566. [Google Scholar] [CrossRef]
- Liu, R.; Bishop, J.; Zhu, G.; Zhang, T.; Ladenson, P.W.; Xing, M. Mortality Risk Stratification by Combining BRAF V600E and TERT Promoter Mutations in Papillary Thyroid Cancer. JAMA Oncol. 2017, 3, 202–208. [Google Scholar] [CrossRef]
- Shen, X.; Liu, R.; Xing, M. A six-genotype genetic prognostic model for papillary thyroid cancer. Endocr.-Relat. Cancer 2017, 24, 41–52. [Google Scholar] [CrossRef]
- Shi, X.; Liu, R.; Qu, S.; Zhu, G.; Bishop, J.; Liu, X.; Sun, H.; Shan, Z.; Wang, E.; Luo, Y.; et al. Association of TERT promoter mutation 1,295,228 C>T with BRAF V600E mutation, older patient age, and distant metastasis in anaplastic thyroid cancer. J. Clin. Endocrinol. Metab. 2015, 100, E632–E637. [Google Scholar] [CrossRef] [PubMed]
- Yates, L.; Norbury, C.J.; Gilbert, R. The Long and Short of MicroRNA. Cell 2013, 153, 516–519. [Google Scholar] [CrossRef]
- Di Leva, G.; Croce, C.M. miRNA profiling of cancer. Curr. Opin. Genet. Dev. 2013, 23, 3–11. [Google Scholar] [CrossRef]
- Zhang, B.; Pan, X.; Cobb, G.; Anderson, T. microRNAs as oncogenes and tumor suppressors. Dev. Biol. 2007, 302, 1–12. [Google Scholar] [CrossRef]
- Cao, J.; Zhang, M.; Zhang, L.; Lou, J.; Zhou, F.; Fang, M. Non-coding RNA in thyroid cancer—Functions and mechanisms. Cancer Lett. 2020, 496, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-K.; Yang, K.D.; Chou, F.-F.; Huang, C.-C.; Lan, Y.-W.; Lee, Y.-F.; Kang, H.-Y.; Liu, R.-T. Prognostic Implications of miR-146b Expression and Its Functional Role in Papillary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2013, 98, E196–E205. [Google Scholar] [CrossRef] [PubMed]
- Mardente, S.; Mari, E.; Consorti, F.; Di Gioia, C.; Negri, R.; Etna, M.P.; Zicari, A.; Antonaci, A. HMGB1 induces the overexpression of miR-222 and miR-221 and increases growth and motility in papillary thyroid cancer cells. Oncol. Rep. 2012, 28, 2285–2289. [Google Scholar] [CrossRef]
- Ravegnini, G.; Cargnin, S.; Sammarini, G.; Zanotti, F.; Bermejo, J.L.; Hrelia, P.; Terrazzino, S.; Angelini, S. Prognostic Role of miR-221 and miR-222 Expression in Cancer Patients: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 970. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, H.; He, L.; Dong, W.; Li, J.; Shan, Z.; Teng, W. Association between the expression of four upregulated miRNAs and extrathyroidal invasion in papillary thyroid carcinoma. OncoTargets Ther. 2013, 6, 281–287. [Google Scholar] [CrossRef]
- Akyay, O.Z.; Gov, E.; Kenar, H.; Arga, K.Y.; Selek, A.; Tarkun, I.; Canturk, Z.; Cetinarslan, B.; Gurbuz, Y.; Sahin, B. Mapping the Molecular Basis and Markers of Papillary Thyroid Carcinoma Progression and Metastasis Using Global Transcriptome and microRNA Profiling. OMICS J. Integr. Biol. 2020, 24, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Ulisse, S.; Baldini, E.; Sorrenti, S.; D’Armiento, M. The Urokinase Plasminogen Activator System: A Target for Anti-Cancer Therapy. Curr. Cancer Drug Targets 2009, 9, 32–71. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J. Urokinase-type plasminogen activator: A potent marker of metastatic potential in human cancer. Biochem. Soc. Trans. 2002, 30, 207–210. [Google Scholar] [CrossRef]
- Look, M.P.; Van Putten, W.L.J.; Duffy, M.J.; Harbeck, N.; Christensen, I.J.; Thomssen, C.; Kates, R.; Spyratos, F.; Ferno, M.; Eppenberger-Castori, S.; et al. Pooled Analysis of Prognostic Impact of Urokinase-Type Plasminogen Activator and Its Inhibitor PAI-1 in 8377 Breast Cancer Patients. J. Natl. Cancer Inst. 2002, 94, 116–128. [Google Scholar] [CrossRef]
- Barzaman, K.; Karami, J.; Zarei, Z.; Hosseinzadeh, A.; Kazemi, M.H.; Moradi-Kalbolandi, S.; Safari, E.; Farahmand, L. Breast cancer: Biology, biomarkers, and treatments. Int. Immunopharmacol. 2020, 84, 106535. [Google Scholar] [CrossRef]
- Baldini, E.; Sorrenti, S.; D’Armiento, E.; DI Matteo, F.M.; Catania, A.; Ulisse, S. The urokinase plasminogen activating system in thyroid cancer: Clinical implications. G. Chir. 2012, 33, 305–310. [Google Scholar]
- Ito, Y.; Takeda, T.; Kobayashi, T.; Wakasugi, E.; Tamaki, Y.; Umeshita, K.; Monden, T.; Shimano, T.; Monden, M. Plasminogen activation system in active even in thyroid tumors; an immunohistochemical study. Anticancer Res. 1996, 16, 81–89. [Google Scholar]
- Herceg, G.H.; Herceg, D.; Kralik, M.; Bence-Zigman, Z.; Tomić-Brzac, H.; Kulić, A. Urokinase-type plasminogen acti-vator and its inhibitor in thyroid neoplasms: A cytosol study. Wien. Klin. Wochenschr. 2006, 118, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Ulisse, S.; Baldini, E.; Toller, M.; Marchioni, E.; Giacomelli, L.; De Antoni, E.; Ferretti, E.; Marzullo, A.; Graziano, F.; Trimboli, P.; et al. Differential expression of the components of the plasminogen activating system in human thyroid tumour derived cell lines and papillary carcinomas. Eur. J. Cancer 2006, 42, 2631–2638. [Google Scholar] [CrossRef]
- Buergy, D.; Weber, T.; Maurer, G.D.; Mudduluru, G.; Medved, F.; Leupold, J.H.; Brauckhoff, M.; Post, S.; Dralle, H.; Allgayer, H. Urokinase receptor, MMP-1 and MMP-9 are markers to differentiate prognosis, adenoma and carcinoma in thyroid malignancies. Int. J. Cancer 2009, 125, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Ulisse, S.; Baldini, E.; Sorrenti, S.; Barollo, S.; Gnessi, L.; Catania, A.; Pellizzo, M.R.; Nardi, F.; Mian, C.; De Antoni, E.; et al. High Expression of the Urokinase Plasminogen Activator and Its Cognate Receptor Associates with Advanced Stages and Reduced Disease-Free Interval in Papillary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2011, 96, 504–508. [Google Scholar] [CrossRef]
- Baldini, E.; Sorrenti, S.; Tuccilli, C.; Prinzi, N.; Coccaro, C.; Catania, A.; Filippini, A.; Bononi, M.; De Antoni, E.; D’Armiento, M.; et al. Emerging molecular markers for the prognosis of differentiated thyroid cancer patients. Int. J. Surg. 2014, 12, S52–S56. [Google Scholar] [CrossRef]
- Sun, J.; Shi, R.; Zhang, X.; Fang, D.; Rauch, J.; Lu, S.; Wang, X.; Käsmann, L.; Ma, J.; Belka, C.; et al. Characterization of immune landscape in papillary thyroid cancer reveals distinct tumor immunogenicity and implications for immunotherapy. OncoImmunology 2021, 10, 1964189. [Google Scholar] [CrossRef] [PubMed]
- Wan, B.; Deng, P.; Dai, W.; Wang, P.; Dong, Z.; Yang, C.; Tian, J.; Hu, T.; Yan, K. Association between programmed cell death ligand 1 expression and thyroid cancer. Medicine 2021, 100, e25315. [Google Scholar] [CrossRef]
- Tuccilli, C.; Baldini, E.; Sorrenti, S.; Catania, A.; Antonelli, A.; Fallahi, P.; Tartaglia, F.; Barollo, S.; Mian, C.; Palmieri, A.; et al. CTLA-4 and PD-1 Ligand Gene Expression in Epithelial Thyroid Cancers. Int. J. Endocrinol. 2018, 2018, 1–10. [Google Scholar] [CrossRef]
- Ulisse, S.; Tuccilli, C.; Sorrenti, S.; Antonelli, A.; Fallahi, P.; D’Armiento, E.; Catania, A.; Tartaglia, F.; Amabile, M.I.; Giacomelli, L.; et al. PD-1 Ligand Expression in Epithelial Thyroid Cancers: Potential Clinical Implications. Int. J. Mol. Sci. 2019, 20, 1405. [Google Scholar] [CrossRef] [PubMed]
- Heikkilä, A.; Hagström, J.; Mäenpää, H.; Louhimo, J.; Siironen, P.; Heiskanen, I.; Haglund, C.; Arola, J. Loss of Estrogen Receptor Beta Expression in Follicular Thyroid Carcinoma Predicts Poor Outcome. Thyroid 2013, 23, 456–465. [Google Scholar] [CrossRef]
- Bains, A.; Mur, T.; Wallace, N.; Noordzij, J. The Role of Vitamin D as a Prognostic Marker in Papillary Thyroid Cancer. Cancers 2021, 13, 3516. [Google Scholar] [CrossRef]
- Melaccio, A.; Sgaramella, L.; Pasculli, A.; Di Meo, G.; Gurrado, A.; Prete, F.; Vacca, A.; Ria, R.; Testini, M. Prognostic and Therapeutic Role of Angiogenic Microenvironment in Thyroid Cancer. Cancers 2021, 13, 2775. [Google Scholar] [CrossRef] [PubMed]
- Xia, F.; Zhang, Z.; Li, X. Emerging Roles of Circular RNAs in Thyroid Cancer. Front. Cell Dev. Biol. 2021, 9, 636838. [Google Scholar] [CrossRef]
- Sedaghati, M.; Kebebew, E. Long noncoding RNAs in thyroid cancer. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 275–281. [Google Scholar] [CrossRef]
- Dong, X.; Jin, C.; Chen, D.; Chen, Y.; Ye, Z.-Q.; Zhang, X.; Huang, X.; Zhang, W.; Gu, D.-N. Genomic Instability-Related LncRNA Signature Predicts the Prognosis and Highlights LINC01614 Is a Tumor Microenvironment-Related Oncogenic lncRNA of Papillary Thyroid Carcinoma. Front. Oncol. 2021, 11, 737867. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.S.; Lorenz, K.; Ukkat, J.; Hoang-Vu, C.; Trojanowicz, B. Angiotensin converting enzymes ACE and ACE2 in thyroid cancer progression. Neoplasma 2020, 67, 402–409. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulisse, S.; Baldini, E.; Lauro, A.; Pironi, D.; Tripodi, D.; Lori, E.; Ferent, I.C.; Amabile, M.I.; Catania, A.; Di Matteo, F.M.; et al. Papillary Thyroid Cancer Prognosis: An Evolving Field. Cancers 2021, 13, 5567. https://doi.org/10.3390/cancers13215567
Ulisse S, Baldini E, Lauro A, Pironi D, Tripodi D, Lori E, Ferent IC, Amabile MI, Catania A, Di Matteo FM, et al. Papillary Thyroid Cancer Prognosis: An Evolving Field. Cancers. 2021; 13(21):5567. https://doi.org/10.3390/cancers13215567
Chicago/Turabian StyleUlisse, Salvatore, Enke Baldini, Augusto Lauro, Daniele Pironi, Domenico Tripodi, Eleonora Lori, Iulia Catalina Ferent, Maria Ida Amabile, Antonio Catania, Filippo Maria Di Matteo, and et al. 2021. "Papillary Thyroid Cancer Prognosis: An Evolving Field" Cancers 13, no. 21: 5567. https://doi.org/10.3390/cancers13215567
APA StyleUlisse, S., Baldini, E., Lauro, A., Pironi, D., Tripodi, D., Lori, E., Ferent, I. C., Amabile, M. I., Catania, A., Di Matteo, F. M., Forte, F., Santoro, A., Palumbo, P., D’Andrea, V., & Sorrenti, S. (2021). Papillary Thyroid Cancer Prognosis: An Evolving Field. Cancers, 13(21), 5567. https://doi.org/10.3390/cancers13215567