
A Mass Spectrometry Imaging Based Approach for Prognosis Prediction in UICC Stage I/II Colon Cancer

 , ,
, ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Sample Collection
2.2. TMA-Construction
2.3. MALDI-MSI Measurement
2.4. Histological Tumor Annotation, Data Processing, and Extraction
2.5. MS/MS Measurements
2.6. Statistical Analysis
2.6.1. Supervised Classification
2.6.2. Unsupervised Analysis
2.6.3. Immunohistochemical Analysis
3. Results
3.1. Patient Characteristics
3.2. Prediction of Metastasis
3.2.1. Supervised Classification
3.2.2. Unsupervised Classification
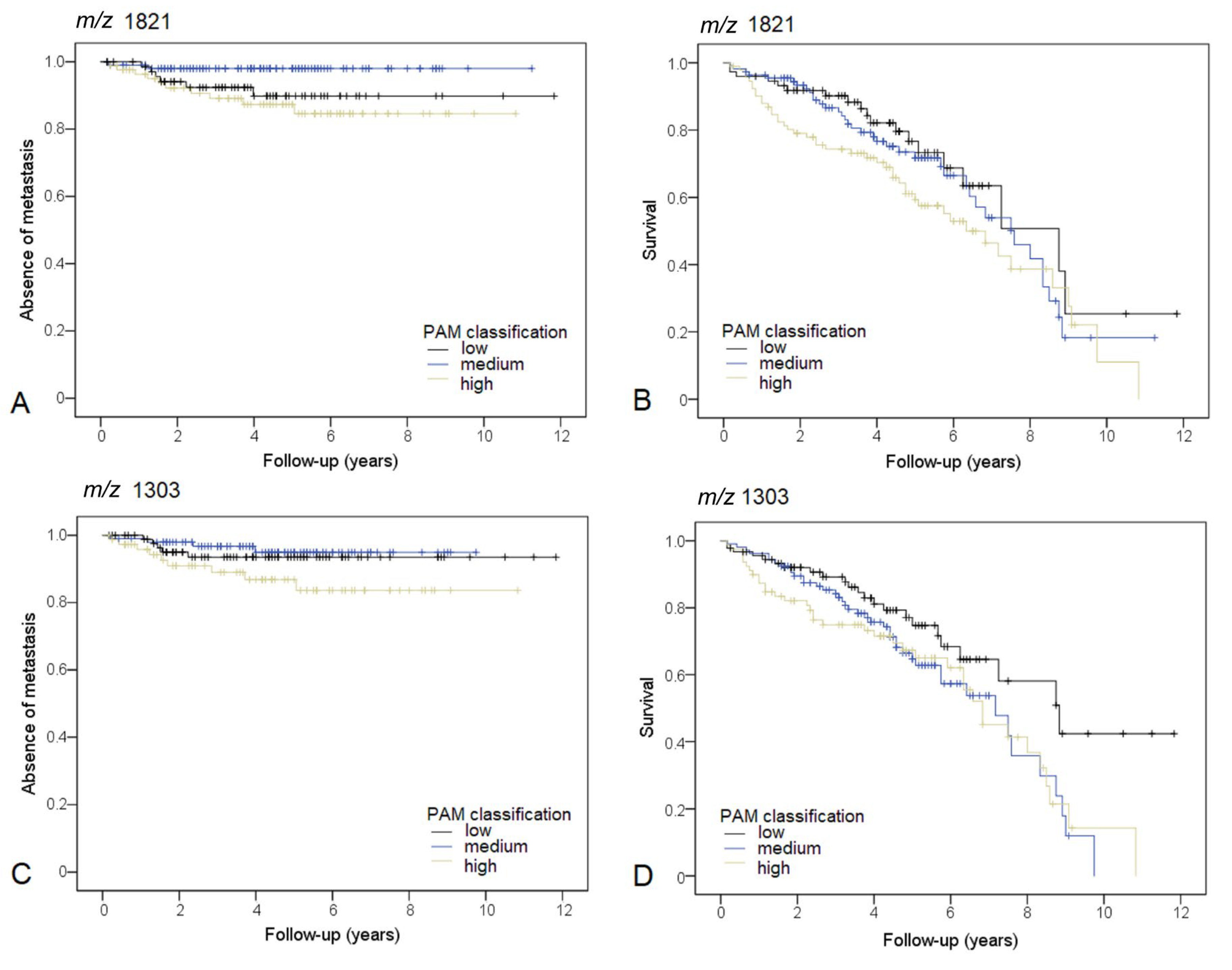
3.3. m/z 1821.8
3.4. m/z 1303.6
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, A.B.; Schrag, D.; Somerfield, M.R.; Cohen, A.M.; Figueredo, A.T.; Flynn, P.J.; Krzyzanowska, M.K.; Maroun, J.; McAllister, P.; Van Cutsem, E.; et al. American Society of Clinical Oncology Recommendations on Adjuvant Chemotherapy for Stage II Colon Cancer. J. Clin. Oncol. 2004, 22, 3408–3419. [Google Scholar] [CrossRef] [PubMed]
- Böckelman, C.; Engelmann, B.E.; Kaprio, T.; Hansen, T.F.; Glimelius, B. Risk of Recurrence in Patients with Colon Cancer Stage II and III: A Systematic Review and Meta-Analysis of Recent Literature. Acta Oncol. 2015, 54, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Dienstmann, R.; Villacampa, G.; Sveen, A.; Mason, M.J.; Niedzwiecki, D.; Nesbakken, A.; Moreno, V.; Warren, R.S.; Lothe, R.A.; Guinney, J. Relative Contribution of Clinicopathological Variables, Genomic Markers, Transcriptomic Subtyping and Microenvironment Features for Outcome Prediction in Stage II/III Colorectal Cancer. Ann. Oncol. 2019, 30, 1622–1629. [Google Scholar] [CrossRef] [Green Version]
- Pagès, F.; Taieb, J.; Laurent-Puig, P.; Galon, J. The Consensus Immunoscore in Phase 3 Clinical Trials; Potential Impact on Patient Management Decisions. Oncoimmunology 2020, 9, 1812221. [Google Scholar] [CrossRef]
- Shivji, S.; Conner, J.R.; Barresi, V.; Kirsch, R. Poorly Differentiated Clusters in Colorectal Cancer: A Current Review and Implications for Future Practice. Histopathology 2020, 77, 351–368. [Google Scholar] [CrossRef]
- Jin, Z.; Sinicrope, F.A. Prognostic and Predictive Values of Mismatch Repair Deficiency in Non-Metastatic Colorectal Cancer. Cancers 2021, 13, 300. [Google Scholar] [CrossRef]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.-F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for Reporting Tumor Budding in Colorectal Cancer Based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef]
- André, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Oxaliplatin, Fluorouracil, and Leucovorin as Adjuvant Treatment for Colon Cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef] [Green Version]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; et al. Improved Overall Survival with Oxaliplatin, Fluorouracil, and Leucovorin as Adjuvant Treatment in Stage II or III Colon Cancer in the MOSAIC Trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef] [Green Version]
- Arentz, G.; Mittal, P.; Zhang, C.; Ho, Y.-Y.; Briggs, M.; Winderbaum, L.; Hoffmann, M.K.; Hoffmann, P. Applications of Mass Spectrometry Imaging to Cancer. Adv. Cancer Res. 2017, 134, 27–66. [Google Scholar] [CrossRef]
- Lopes Gonçalves, J.P.; Bollwein, C.; Weichert, W.; Schwamborn, K. Implementation of Mass Spectrometry Imaging in Pathology: Advances and Challenges. Clin. Lab. Med. 2021, 41, 173–184. [Google Scholar] [CrossRef]
- Ryan, D.J.; Spraggins, J.M.; Caprioli, R.M. Protein Identification Strategies in MALDI Imaging Mass Spectrometry: A Brief Review. Curr. Opin. Chem. Biol. 2019, 48, 64–72. [Google Scholar] [CrossRef]
- Vaysse, P.-M.; Heeren, R.M.A.; Porta, T.; Balluff, B. Mass Spectrometry Imaging for Clinical Research—Latest Developments, Applications, and Current Limitations. Analyst 2017, 142, 2690–2712. [Google Scholar] [CrossRef]
- Angel, P.M.; Norris-Caneda, K.; Drake, R.R. In Situ Imaging of Tryptic Peptides by MALDI Imaging Mass Spectrometry Using Fresh-Frozen or Formalin-Fixed, Paraffin-Embedded Tissue. Curr. Protoc. Protein Sci. 2018, 94, e65. [Google Scholar] [CrossRef]
- Kriegsmann, K.; Longuespée, R.; Hundemer, M.; Zgorzelski, C.; Casadonte, R.; Schwamborn, K.; Weichert, W.; Schirmacher, P.; Harms, A.; Kazdal, D.; et al. Combined Immunohistochemistry after Mass Spectrometry Imaging for Superior Spatial Information. Proteom. Clin. Appl. 2019, 13, e1800035. [Google Scholar] [CrossRef] [Green Version]
- Neumann, E.K.; Djambazova, K.V.; Caprioli, R.M.; Spraggins, J.M. Multimodal Imaging Mass Spectrometry: Next Generation Molecular Mapping in Biology and Medicine. J. Am. Soc. Mass Spectrom. 2020, 31, 2401–2415. [Google Scholar] [CrossRef]
- Angel, P.M.; Mehta, A.; Norris-Caneda, K.; Drake, R.R. MALDI Imaging Mass Spectrometry of N-Glycans and Tryptic Peptides from the Same Formalin-Fixed, Paraffin-Embedded Tissue Section. Methods Mol. Biol. 2018, 1788, 225–241. [Google Scholar] [CrossRef]
- Heijs, B.; Holst, S.; Briaire-de Bruijn, I.H.; van Pelt, G.W.; de Ru, A.H.; van Veelen, P.A.; Drake, R.R.; Mehta, A.S.; Mesker, W.E.; Tollenaar, R.A.; et al. Multimodal Mass Spectrometry Imaging of N-Glycans and Proteins from the Same Tissue Section. Anal. Chem. 2016, 88, 7745–7753. [Google Scholar] [CrossRef]
- Märkl, B.; Märkl, M.; Schaller, T.; Mayr, P.; Schenkirsch, G.; Kriening, B.; Anthuber, M. A New Simple Morphology-Based Risk Score Is Prognostic in Stage I/II Colon Cancers. Cancer Med. 2016, 5, 1492–1501. [Google Scholar] [CrossRef] [Green Version]
- Ly, A.; Longuespée, R.; Casadonte, R.; Wandernoth, P.; Schwamborn, K.; Bollwein, C.; Marsching, C.; Kriegsmann, K.; Hopf, C.; Weichert, W.; et al. Site-to-Site Reproducibility and Spatial Resolution in MALDI-MSI of Peptides from Formalin-Fixed Paraffin-Embedded Samples. Proteom. Clin. Appl. 2019, 13, e1800029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, D.N.; Pappin, D.J.; Creasy, D.M.; Cottrell, J.S. Probability-Based Protein Identification by Searching Sequence Databases Using Mass Spectrometry Data. Electrophoresis 1999, 20, 3551–3567. [Google Scholar] [CrossRef]
- Buck, A.; Heijs, B.; Beine, B.; Schepers, J.; Cassese, A.; Heeren, R.M.A.; McDonnell, L.A.; Henkel, C.; Walch, A.; Balluff, B. Round Robin Study of Formalin-Fixed Paraffin-Embedded Tissues in Mass Spectrometry Imaging. Anal. Bioanal. Chem. 2018, 410, 5969–5980. [Google Scholar] [CrossRef] [Green Version]
- Römpp, A.; Both, J.-P.; Brunelle, A.; Heeren, R.M.A.; Laprévote, O.; Prideaux, B.; Seyer, A.; Spengler, B.; Stoeckli, M.; Smith, D.F. Mass Spectrometry Imaging of Biological Tissue: An Approach for Multicenter Studies. Anal. Bioanal. Chem. 2015, 407, 2329–2335. [Google Scholar] [CrossRef]
- Porcari, A.M.; Zhang, J.; Garza, K.Y.; Rodrigues-Peres, R.M.; Lin, J.Q.; Young, J.H.; Tibshirani, R.; Nagi, C.; Paiva, G.R.; Carter, S.A.; et al. Multicenter Study Using Desorption-Electrospray-Ionization-Mass-Spectrometry Imaging for Breast-Cancer Diagnosis. Anal. Chem. 2018, 90, 11324–11332. [Google Scholar] [CrossRef]
- Boskamp, T.; Casadonte, R.; Hauberg-Lotte, L.; Deininger, S.; Kriegsmann, J.; Maass, P. Cross-Normalization of MALDI Mass Spectrometry Imaging Data Improves Site-to-Site Reproducibility. Anal. Chem. 2021, 93, 10584–10592. [Google Scholar] [CrossRef]
- Boskamp, T.; Lachmund, D.; Casadonte, R.; Hauberg-Lotte, L.; Kobarg, J.H.; Kriegsmann, J.; Maass, P. Using the Chemical Noise Background in MALDI Mass Spectrometry Imaging for Mass Alignment and Calibration. Anal. Chem. 2020, 92, 1301–1308. [Google Scholar] [CrossRef]
- Kuhn, M. Building Predictive Models in R Using the Caret Package. J. Stat. Softw. 2008, 28, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Maechler, M.; Rousseeuw, P.; Struyf, A.; Hubert, M.; Hornik, K. cluster: Cluster Analysis Basics and Extensions. R Package Version 2.1.0. 2019. Available online: https://cran.r-project.org/web/packages/cluster/index.html (accessed on 31 August 2021).
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000; ISBN 0-387-98784-3. [Google Scholar]
- Groseclose, M.R.; Massion, P.P.; Chaurand, P.; Caprioli, R.M. High-Throughput Proteomic Analysis of Formalin-Fixed Paraffin-Embedded Tissue Microarrays Using MALDI Imaging Mass Spectrometry. Proteomics 2008, 8, 3715–3724. [Google Scholar] [CrossRef]
- Jih, D.M.; Lyle, S.; Elenitsas, R.; Elder, D.E.; Cotsarelis, G. Cytokeratin 15 Expression in Trichoepitheliomas and a Subset of Basal Cell Carcinomas Suggests They Originate from Hair Follicle Stem Cells. J. Cutan. Pathol. 1999, 26, 113–118. [Google Scholar] [CrossRef]
- Ohyama, M.; Terunuma, A.; Tock, C.L.; Radonovich, M.F.; Pise-Masison, C.A.; Hopping, S.B.; Brady, J.N.; Udey, M.C.; Vogel, J.C. Characterization and Isolation of Stem Cell-Enriched Human Hair Follicle Bulge Cells. J. Clin. Investig. 2006, 116, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.; Li, A.; Kaur, P. Location and Phenotype of Human Adult Keratinocyte Stem Cells of the Skin. Differentiation 2004, 72, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Figueira, E.C.; Di Girolamo, N.; Coroneo, M.T.; Wakefield, D. The Phenotype of Limbal Epithelial Stem Cells. Investig. Ophthalmol. Vis. Sci. 2007, 48, 144–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Y.-H.; Xu, C.-P.; Shi, Z.-M.; Zhang, Y.-J.; Qiao, Y.-G.; Zhao, H.-P. Cytokeratin 15 Is an Effective Indicator for Progression and Malignancy of Esophageal Squamous Cell Carcinomas. Asian Pac. J. Cancer Prev. 2016, 17, 4217–4222. [Google Scholar]
- Hanley, C.J.; Noble, F.; Ward, M.; Bullock, M.; Drifka, C.; Mellone, M.; Manousopoulou, A.; Johnston, H.E.; Hayden, A.; Thirdborough, S.; et al. A Subset of Myofibroblastic Cancer-Associated Fibroblasts Regulate Collagen Fiber Elongation, Which is Prognostic in Multiple Cancers. Oncotarget 2015, 7, 6159–6174. [Google Scholar] [CrossRef] [Green Version]
- Mesker, W.E.; Junggeburt, J.M.C.; Szuhai, K.; de Heer, P.; Morreau, H.; Tanke, H.J.; Tollenaar, R.A.E.M. The Carcinoma-Stromal Ratio of Colon Carcinoma Is an Independent Factor for Survival Compared to Lymph Node Status and Tumor Stage. Cell. Oncol. 2007, 29, 387–398. [Google Scholar]
- Van Pelt, G.W.; Kjær-Frifeldt, S.; van Krieken, J.H.J.M.; Al Dieri, R.; Morreau, H.; Tollenaar, R.A.E.M.; Sørensen, F.B.; Mesker, W.E. Scoring the Tumor-Stroma Ratio in Colon Cancer: Procedure and Recommendations. Virchows Arch. 2018, 473, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.; Banner, B.M.; Schäfer, E.-M.; Mayr, P.; Anthuber, M.; Schenkirsch, G.; Märkl, B. Tumor Proportion in Colon Cancer: Results from a Semiautomatic Image Analysis Approach. Virchows Arch. 2020, 477, 185–193. [Google Scholar] [CrossRef]
- Wang, X.-Q.; Tang, Z.-X.; Yu, D.; Cui, S.-J.; Jiang, Y.-H.; Zhang, Q.; Wang, J.; Yang, P.-Y.; Liu, F. Epithelial but Not Stromal Expression of Collagen Alpha-1(III) Is a Diagnostic and Prognostic Indicator of Colorectal Carcinoma. Oncotarget 2016, 7, 8823–8838. [Google Scholar] [CrossRef] [Green Version]
- Kehlet, S.N.; Sanz-Pamplona, R.; Brix, S.; Leeming, D.J.; Karsdal, M.A.; Moreno, V. Excessive Collagen Turnover Products Are Released during Colorectal Cancer Progression and Elevated in Serum from Metastatic Colorectal Cancer Patients. Sci. Rep. 2016, 6, 30599. [Google Scholar] [CrossRef] [Green Version]
- Meding, S.; Balluff, B.; Elsner, M.; Schöne, C.; Rauser, S.; Nitsche, U.; Maak, M.; Schäfer, A.; Hauck, S.M.; Ueffing, M.; et al. Tissue-based Proteomics Reveals FXYD3, S100A11 and GSTM3 as Novel Markers for Regional Lymph Node Metastasis in Colon Cancer. J. Pathol. 2012, 228, 459–470. [Google Scholar] [CrossRef]
- Hinsch, A.; Buchholz, M.; Odinga, S.; Borkowski, C.; Koop, C.; Izbicki, J.R.; Wurlitzer, M.; Krech, T.; Wilczak, W.; Steurer, S.; et al. MALDI Imaging Mass Spectrometry Reveals Multiple Clinically Relevant Masses in Colorectal Cancer Using Large-Scale Tissue Microarrays. J. Mass Spectrom. 2017, 52, 165–173. [Google Scholar] [CrossRef]
- Boyaval, F.; Van Zeijl, R.; Dalebout, H.; Holst, S.; van Pelt, G.; Fariña-Sarasqueta, A.; Mesker, W.; Tollenaar, R.; Morreau, H.; Wuhrer, M.; et al. N-Glycomic Signature of Stage II Colorectal Cancer and Its Association with the Tumor Microenvironment. Mol. Cell. Proteom. 2021, 20, 100057. [Google Scholar] [CrossRef]
- Alexander, J.; Gildea, L.; Balog, J.; Speller, A.; McKenzie, J.; Muirhead, L.; Scott, A.; Kontovounisios, C.; Rasheed, S.; Teare, J.; et al. A Novel Methodology for in Vivo Endoscopic Phenotyping of Colorectal Cancer Based on Real-Time Analysis of the Mucosal Lipidome: A Prospective Observational Study of the IKnife. Surg. Endosc. 2017, 31, 1361–1370. [Google Scholar] [CrossRef] [Green Version]
- Mason, S.E.; Manoli, E.; Alexander, J.L.; Poynter, L.; Ford, L.; Paizs, P.; Adebesin, A.; McKenzie, J.S.; Rosini, F.; Goldin, R.; et al. Lipidomic Profiling of Colorectal Lesions for Real-Time Tissue Recognition and Risk-Stratification Using Rapid Evaporative Ionisation Mass Spectrometry. Ann. Surg. 2021. [Google Scholar] [CrossRef]
- Veselkov, K.A.; Mirnezami, R.; Strittmatter, N.; Goldin, R.D.; Kinross, J.; Speller, A.V.M.; Abramov, T.; Jones, E.A.; Darzi, A.; Holmes, E.; et al. Chemo-Informatic Strategy for Imaging Mass Spectrometry-Based Hyperspectral Profiling of Lipid Signatures in Colorectal Cancer. Proc. Natl. Acad. Sci. USA 2014, 111, 1216–1221. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Characteristics | All Patients | Exploration Set (n = 138) | Test Set (n = 138) | p-Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age (years ± SD) | 69.9 ± 10.4 | 69.9 ± 10.9 | 70.1 ± 10.0 | NS | |||
| Follow-up (years ± SD) | 4.2 ± 2.39 | 4.0 ± 2.4 | 4.4 ± 2.4 | NS | |||
| Sex | NS | ||||||
| Female | 114 | 41.3% | 54 | 39.1% | 60 | 43.5% | |
| Male | 162 | 58.7% | 84 | 60.9% | 78 | 56.5% | |
| UICC | NS | ||||||
| I | 112 (40.5%) | 40.6% | 54 | 39.1% | 58 | 42.0% | |
| II | 164 (59.4%) | 59.4% | 84 | 60.9% | 80 | 58.0% | |
| pT | NS | ||||||
| 1 | 12 | 4.3% | 6 | 4.3% | 6 | 4.3% | |
| 2 | 100 | 36.2% | 48 | 34.8% | 52 | 37.7% | |
| 3 | 155 | 56.2% | 80 | 58.0% | 75 | 54.3% | |
| 4 | 9 | 3.3% | 4 | 2.9% | 5 | 3.6% | |
| Grading | NS | ||||||
| Low | 218 | 79.0% | 109 | 79.0% | 109 | 79.0% | |
| High | 58 | 21.0% | 29 | 21.0% | 29 | 21.0% | |
| Differentiation | 0.019 | ||||||
| Adenocarcinoma, NOS | 241 | 87.3% | 114 | 82.6% | 127 | 92.0% | |
| Specific Subtype | 35 | 12.7% | 24 | 17.4% | 11 | 8.0% | |
| Death | |||||||
| All causes | 102 | 37.0% | 48 | 34.8% | 54 | 39.1% | NS |
| Colon Cancer specific | 26 | 9.4% | 11 | 8.0% | 15 | 10.9% | NS |
| Distant Metastasis | NS | ||||||
| No | 245 | 88.8% | 126 | 91.3% | 119 | 86.2% | |
| Yes | 31 | 11.2% | 12 | 8.7% | 19 | 13.8% | |
| Supervised Classification Results | RF (n = 500) | kNN | SVM | LDA |
|---|---|---|---|---|
| Balanced accuracy | 0.9731 | 0.9828 | 0.9217 | 0.5700 |
| Sensitivity | 0.9991 | 0.9963 | 0.9992 | 0.9887 |
| Specificity | 0.9471 | 0.9693 | 0.8442 | 0.1513 |
| m/z Features | Low Intensity | Medium Intensity | High Intensity |
|---|---|---|---|
| m/z 1821.8 | |||
| n = 276 | 27% | 40% | 33% |
| Mean intensity | 1.23 | 1.77 | 2.39 |
| Intensity range | 0.790–1.526 | 1.532–2.015 | 2.016–6.80 |
| m/z 1303.6 | |||
| n = 276 | 33% | 38% | 29% |
| Mean intensity | 5.73 | 9.16 | 13.78 |
| Intensity range | 1.58–7.52 | 9.16–10.84 | 11.17–21.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, B.; Gonçalves, J.P.L.; Bollwein, C.; Sommer, F.; Schenkirsch, G.; Jacob, A.; Seibert, A.; Weichert, W.; Märkl, B.; Schwamborn, K. A Mass Spectrometry Imaging Based Approach for Prognosis Prediction in UICC Stage I/II Colon Cancer. Cancers 2021, 13, 5371. https://doi.org/10.3390/cancers13215371
Martin B, Gonçalves JPL, Bollwein C, Sommer F, Schenkirsch G, Jacob A, Seibert A, Weichert W, Märkl B, Schwamborn K. A Mass Spectrometry Imaging Based Approach for Prognosis Prediction in UICC Stage I/II Colon Cancer. Cancers. 2021; 13(21):5371. https://doi.org/10.3390/cancers13215371
Chicago/Turabian StyleMartin, Benedikt, Juliana P. L. Gonçalves, Christine Bollwein, Florian Sommer, Gerhard Schenkirsch, Anne Jacob, Armin Seibert, Wilko Weichert, Bruno Märkl, and Kristina Schwamborn. 2021. "A Mass Spectrometry Imaging Based Approach for Prognosis Prediction in UICC Stage I/II Colon Cancer" Cancers 13, no. 21: 5371. https://doi.org/10.3390/cancers13215371
APA StyleMartin, B., Gonçalves, J. P. L., Bollwein, C., Sommer, F., Schenkirsch, G., Jacob, A., Seibert, A., Weichert, W., Märkl, B., & Schwamborn, K. (2021). A Mass Spectrometry Imaging Based Approach for Prognosis Prediction in UICC Stage I/II Colon Cancer. Cancers, 13(21), 5371. https://doi.org/10.3390/cancers13215371