
Potential Morbidity Reduction for Lung Stereotactic Body Radiation Therapy Using Respiratory Gating

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Data
2.2. Treatment Planning
2.3. Respiratory Gating Simulation
2.4. Statistical Analysis
2.5. Toxicity Risk Analysis
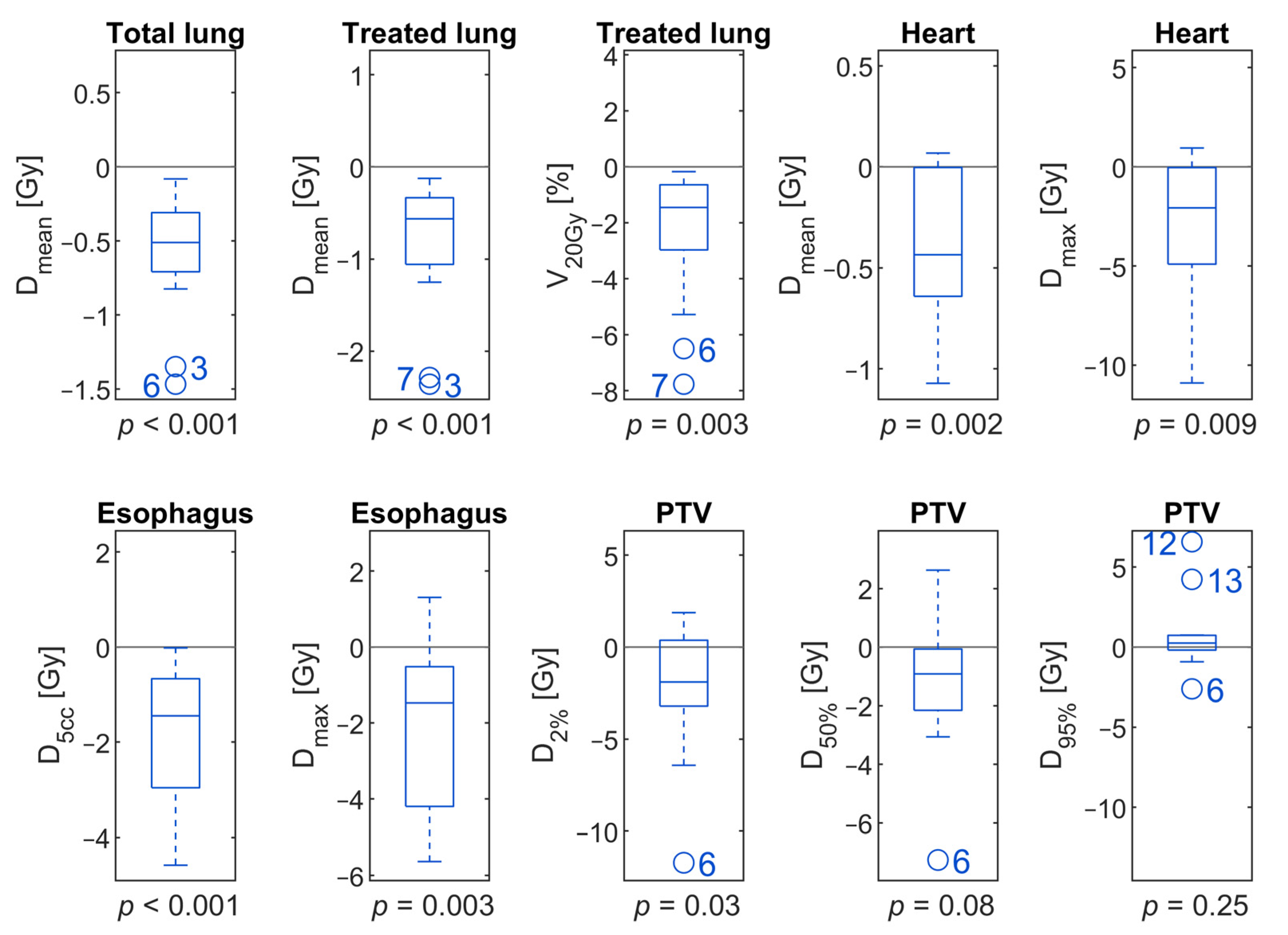
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Potters, L.; Kavanagh, B.; Galvin, J.M.; Hevezi, J.M.; Janjan, N.A.; Larson, D.A.; Mehta, M.P.; Ryu, S.; Steinberg, M.; Timmerman, R.; et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology (ACR) Practice Guideline for the Performance of Stereotactic Body Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Videtic, G.M.M.; Donington, J.; Giuliani, M.; Heinzerling, J.; Karas, T.Z.; Kelsey, C.R.; Lally, B.E.; Latzka, K.; Lo, S.S.; Moghanaki, D.; et al. Stereotactic Body Radiation Therapy for Early-Stage Non-Small Cell Lung Cancer: Executive Summary of an ASTRO Evidence-Based Guideline. Pract. Radiat. Oncol. 2017, 7, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S. ESMO Guidelines Committee Early and Locally Advanced Non-Small-Cell Lung Cancer (NSCLC): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.; Chirieac, L.R.; D’Amico, T.A.; DeCamp, M.M.; Dilling, T.J.; Dobelbower, M.; et al. Non-Small Cell Lung Cancer, Version 5.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2017, 15, 504–535. [Google Scholar] [CrossRef] [PubMed]
- Guckenberger, M.; Andratschke, N.; Alheit, H.; Holy, R.; Moustakis, C.; Nestle, U.; Sauer, O.; Deutschen Gesellschaft für Radioonkologie (DEGRO). Definition of Stereotactic Body Radiotherapy: Principles and Practice for the Treatment of Stage I Non-Small Cell Lung Cancer. Strahlenther. Onkol. 2014, 190, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Guckenberger, M.; Allgäuer, M.; Appold, S.; Dieckmann, K.; Ernst, I.; Ganswindt, U.; Holy, R.; Nestle, U.; Nevinny-Stickel, M.; Semrau, S.; et al. Safety and Efficacy of Stereotactic Body Radiotherapy for Stage 1 Non-Small-Cell Lung Cancer in Routine Clinical Practice: A Patterns-of-Care and Outcome Analysis. J. Thorac. Oncol. 2013, 8, 1050–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, D.R.; Tang, C.; Zhang, J.; Blumenschein, G.R.; Hernandez, M.; Lee, J.J.; Ye, R.; Palma, D.A.; Louie, A.V.; Camidge, D.R.; et al. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients With Oligometastatic Non-Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study. J. Clin. Oncol. 2019, 37, 1558–1565. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.A.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.A.; Lock, M.I.; Rodrigues, G.; Yaremko, B.P.; et al. Stereotactic Ablative Radiation Therapy for the Comprehensive Treatment of Oligometastatic Tumors (SABR-COMET): Results of a Randomized Trial. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, S3–S4. [Google Scholar] [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic Body Radiation Therapy for Inoperable Early Stage Lung Cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Videtic, G.M.M.; Reddy, C.A.; Sorenson, L. A Prospective Study of Quality of Life Including Fatigue and Pulmonary Function after Stereotactic Body Radiotherapy for Medically Inoperable Early-Stage Lung Cancer. Support Care Cancer 2013, 21, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Liu, H.; Balter, P.; Komaki, R.; Liao, Z.; Welsh, J.; Mehran, R.J.; Roth, J.A.; Swisher, S.G. Clinical Outcome and Predictors of Survival and Pneumonitis after Stereotactic Ablative Radiotherapy for Stage I Non-Small Cell Lung Cancer. Radiat. Oncol. 2012, 7, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Yorke, E.D.; Li, L.; Kavanagh, B.D.; Li, X.A.; Das, S.; Miften, M.; Rimner, A.; Campbell, J.; Xue, J.; et al. Simple Factors Associated With Radiation-Induced Lung Toxicity After Stereotactic Body Radiation Therapy of the Thorax: A Pooled Analysis of 88 Studies. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1357–1366. [Google Scholar] [CrossRef] [Green Version]
- Barriger, R.B.; Forquer, J.A.; Brabham, J.G.; Andolino, D.L.; Shapiro, R.H.; Henderson, M.A.; Johnstone, P.A.S.; Fakiris, A.J. A Dose–Volume Analysis of Radiation Pneumonitis in Non–Small Cell Lung Cancer Patients Treated With Stereotactic Body Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.-M.S.; Moiseenko, V.; Zhao, J.; Milano, M.T.; Li, L.; Rimner, A.; Das, S.; Li, X.A.; Miften, M.; Liao, Z.; et al. Organs at Risk Considerations for Thoracic Stereotactic Body Radiation Therapy: What Is Safe for Lung Parenchyma? Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 172–187. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, R.; McGarry, R.; Yiannoutsos, C.; Papiez, L.; Tudor, K.; DeLuca, J.; Ewing, M.; Abdulrahman, R.; DesRosiers, C.; Williams, M.; et al. Excessive Toxicity When Treating Central Tumors in a Phase II Study of Stereotactic Body Radiation Therapy for Medically Inoperable Early-Stage Lung Cancer. J. Clin. Oncol. 2006, 24, 4833–4839. [Google Scholar] [CrossRef] [PubMed]
- Haseltine, J.M.; Rimner, A.; Gelblum, D.Y.; Modh, A.; Rosenzweig, K.E.; Jackson, A.; Yorke, E.D.; Wu, A.J. Fatal Complications after Stereotactic Body Radiation Therapy for Central Lung Tumors Abutting the Proximal Bronchial Tree. Pract. Radiat. Oncol. 2016, 6, e27–e33. [Google Scholar] [CrossRef] [Green Version]
- Tekatli, H.; Haasbeek, N.; Dahele, M.; De Haan, P.; Verbakel, W.; Bongers, E.; Hashemi, S.; Nossent, E.; Spoelstra, F.; de Langen, A.J.; et al. Outcomes of Hypofractionated High-Dose Radiotherapy in Poor-Risk Patients with “Ultracentral” Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2016, 11, 1081–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regnery, S.; Eichkorn, T.; Weykamp, F.; Held, T.; Dinges, L.-A.; Schunn, F.; Winter, H.; Thomas, M.; Debus, J.; El Shafie, R.A.; et al. Progression of Pulmonary Function and Correlation with Survival Following Stereotactic Body Radiotherapy of Central and Ultracentral Lung Tumors. Cancers 2020, 12, 2862. [Google Scholar] [CrossRef] [PubMed]
- Duijm, M.; van der Voort van Zyp, N.C.; van de Vaart, P.; Oomen-de Hoop, E.; Mast, M.E.; Hoogeman, M.S.; Nuyttens, J.J. Predicting High-Grade Esophagus Toxicity After Treating Central Lung Tumors With Stereotactic Radiation Therapy Using a Normal Tissue Complication Probability Model. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.Y.; Li, Q.-Q.; Xu, Q.-Y.; Allen, P.K.; Rebueno, N.; Gomez, D.R.; Balter, P.; Komaki, R.; Mehran, R.; Swisher, S.G.; et al. Stereotactic Ablative Radiation Therapy for Centrally Located Early Stage or Isolated Parenchymal Recurrences of Non-Small Cell Lung Cancer: How to Fly in a “No Fly Zone”. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1120–1128. [Google Scholar] [CrossRef]
- Murrell, D.H.; Laba, J.M.; Erickson, A.; Millman, B.; Palma, D.A.; Louie, A.V. Stereotactic Ablative Radiotherapy for Ultra-Central Lung Tumors: Prioritize Target Coverage or Organs at Risk? Radiat. Oncol. 2018, 13, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagerwaard, F.J.; Haasbeek, C.J.A.; Smit, E.F.; Slotman, B.J.; Senan, S. Outcomes of Risk-Adapted Fractionated Stereotactic Radiotherapy for Stage I Non-Small-Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Bezjak, A.; Paulus, R.; Gaspar, L.E.; Timmerman, R.D.; Straube, W.L.; Ryan, W.F.; Garces, Y.I.; Pu, A.T.; Singh, A.K.; Videtic, G.M.; et al. Safety and Efficacy of a Five-Fraction Stereotactic Body Radiotherapy Schedule for Centrally Located Non-Small-Cell Lung Cancer: NRG Oncology/RTOG 0813 Trial. J. Clin. Oncol. 2019, 37, 1316–1325. [Google Scholar] [CrossRef]
- Aridgides, P.; Nsouli, T.; Chaudhari, R.; Kincaid, R.; Rosenbaum, P.F.; Tanny, S.; Mix, M.; Bogart, J. Clinical Outcomes Following Advanced Respiratory Motion Management (Respiratory Gating or Dynamic Tumor Tracking) with Stereotactic Body Radiation Therapy for Stage I Non-Small-Cell Lung Cancer. Lung Cancer 2018, 9, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Prunaretty, J.; Boisselier, P.; Aillères, N.; Riou, O.; Simeon, S.; Bedos, L.; Azria, D.; Fenoglietto, P. Tracking, Gating, Free-Breathing, Which Technique to Use for Lung Stereotactic Treatments? A Dosimetric Comparison. Rep. Pract. Oncol. Radiother. 2019, 24, 97–104. [Google Scholar] [CrossRef]
- Saito, T.; Sakamoto, T.; Oya, N. Comparison of Gating around End-Expiration and End-Inspiration in Radiotherapy for Lung Cancer. Radiother. Oncol. 2009, 93, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Cole, A.J.; Hanna, G.G.; Jain, S.; O’Sullivan, J.M. Motion Management for Radical Radiotherapy in Non-Small Cell Lung Cancer. Clin. Oncol. 2014, 26, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Rouabhi, O.; Gross, B.; Bayouth, J.; Xia, J. The Dosimetric and Temporal Effects of Respiratory-Gated, High-Dose-Rate Radiation Therapy in Patients with Lung Cancer. Technol. Cancer Res. Treat. 2019, 18, 1533033818816072. [Google Scholar] [CrossRef]
- Brierley, J.; Gospodarowicz, M.K.; Wittekind, C.; Union for International Cancer Control. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2017; ISBN 978-1-119-26357-9. [Google Scholar]
- Hanna, G.G.; Murray, L.; Patel, R.; Jain, S.; Aitken, K.L.; Franks, K.N.; van As, N.; Tree, A.; Hatfield, P.; Harrow, S.; et al. UK Consensus on Normal Tissue Dose Constraints for Stereotactic Radiotherapy. Clin. Oncol. 2018, 30, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rit, S.; van Herk, M.; Zijp, L.; Sonke, J.-J. Quantification of the Variability of Diaphragm Motion and Implications for Treatment Margin Construction. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e399–e407. [Google Scholar] [CrossRef]
- Heerkens, H.D.; van Vulpen, M.; van den Berg, C.A.T.; Tijssen, R.H.N.; Crijns, S.P.M.; Molenaar, I.Q.; van Santvoort, H.C.; Reerink, O.; Meijer, G.J. MRI-Based Tumor Motion Characterization and Gating Schemes for Radiation Therapy of Pancreatic Cancer. Radiother. Oncol. 2014, 111, 252–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lujan, A.E.; Larsen, E.W.; Balter, J.M.; Ten Haken, R.K. A Method for Incorporating Organ Motion Due to Breathing into 3D Dose Calculations. Med Phys. 1999, 26, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Ryckman, J.M.; Baine, M.; Carmicheal, J.; Osayande, F.; Sleightholm, R.; Samson, K.; Zheng, D.; Zhen, W.; Lin, C.; Zhang, C. Correlation of Dosimetric Factors with the Development of Symptomatic Radiation Pneumonitis in Stereotactic Body Radiotherapy. Radiat. Oncol. 2020, 15, 33. [Google Scholar] [CrossRef]
- Wu, A.J.; Williams, E.; Modh, A.; Foster, A.; Yorke, E.; Rimner, A.; Jackson, A. Dosimetric Predictors of Esophageal Toxicity after Stereotactic Body Radiotherapy for Central Lung Tumors. Radiother. Oncol. 2014, 112, 267–271. [Google Scholar] [CrossRef] [Green Version]
- Nuyttens, J.J.; Moiseenko, V.; McLaughlin, M.; Jain, S.; Herbert, S.; Grimm, J. Esophageal Dose Tolerance in Patients Treated with Stereotactic Body Radiation Therapy. Semin. Radiat. Oncol. 2016, 26, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Wu, Q.; Zhao, B.; Wen, N.; Ajlouni, M.; Movsas, B.; Chetty, I.J. To Gate or Not to Gate-Dosimetric Evaluation Comparing Gated vs. ITV-Based Methodologies in Stereotactic Ablative Body Radiotherapy (SABR) Treatment of Lung Cancer. Radiat. Oncol. 2016, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muirhead, R.; Featherstone, C.; Duffton, A.; Moore, K.; McNee, S. The Potential Clinical Benefit of Respiratory Gated Radiotherapy (RGRT) in Non-Small Cell Lung Cancer (NSCLC). Radiother. Oncol. 2010, 95, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.S.; Huh, G.J.; Park, S.Y.; Yang, P.S.; Cho, E.Y. The Impact of Respiratory Gating on Lung Dosimetry in Stereotactic Body Radiotherapy for Lung Cancer. Phys. Med. 2014, 30, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Kraus, K.M.; Oechsner, M.; Wilkens, J.J.; Kessel, K.A.; Münch, S.; Combs, S.E. Patient Individual Phase Gating for Stereotactic Radiation Therapy of Early Stage Non-Small Cell Lung Cancer (NSCLC). Sci. Rep. 2021, 11, 5870. [Google Scholar] [CrossRef]
- Eppenhof, K.A.J.; Pluim, J.P.W. Error Estimation of Deformable Image Registration of Pulmonary CT Scans Using Convolutional Neural Networks. JMI 2018, 5, 024003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanley, J.; Debois, M.M.; Mah, D.; Mageras, G.S.; Raben, A.; Rosenzweig, K.; Mychalczak, B.; Schwartz, L.H.; Gloeggler, P.J.; Lutz, W.; et al. Deep Inspiration Breath-Hold Technique for Lung Tumors: The Potential Value of Target Immobilization and Reduced Lung Density in Dose Escalation. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 603–611. [Google Scholar] [CrossRef]
- Lee, D.; Greer, P.B.; Lapuz, C.; Ludbrook, J.; Hunter, P.; Arm, J.; Pollock, S.; Makhija, K.; O’Brien, R.T.; Kim, T.; et al. Audiovisual Biofeedback Guided Breath-Hold Improves Lung Tumor Position Reproducibility and Volume Consistency. Adv. Radiat. Oncol. 2017, 2, 354–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Underberg, R.W.M.; Lagerwaard, F.J.; Slotman, B.J.; Cuijpers, J.P.; Senan, S. Benefit of Respiration-Gated Stereotactic Radiotherapy for Stage I Lung Cancer: An Analysis of 4DCT Datasets. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 554–560. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Case Location Peripheral | Age | Smoking Status | TNM | Pulmonary Comorbidity |
|---|---|---|---|---|---|
| 1 | Right lower lobe | 81 | Current | cT1c cN0 M0 | No |
| 2 | Left lower lobe | 72 | Former | cT1c cN0 cM0 | Yes |
| 3 | Left upper lobe | 79 | Former | cT1 cN0 cM0 | Yes |
| 4 | Right lower lobe | 83 | Former | cT1b cN0 M0 | Yes |
| Case Location Central | |||||
| 5 | Right hilar | 74 | Current | cT1b2 cN0 M0 | Yes |
| 6 | Left hilar | 63 | Former | cT1c cN0 cM0 | Yes |
| 7 | Right hilar | 80 | Former | pT2a pN0 cM0 | Yes |
| 8 | Left hilar | 83 | Former | rcT0 rcN1 rcM1 | No |
| 9 | Right hilar | 50 | Former | cT4 cN+ cM1 | No |
| 10 | Right hilar | 55 | Current | cT2 cN2 M1b | No |
| 11 | Left hilar | 70 | Former | cT2 cN0 cMX | Yes |
| 12 | Left hilar | 66 | Current | cT3 cN1 cM1 | No |
| 13 | Right hilar | 70 | no | rcT1a pN1 M0 | No |
| 14 | Right upper lobe | 51 | no | cT1b cN1 cM1b | No |
| Dosimetric Parameter | Gating Window GW40–60 | No Gating | ||
|---|---|---|---|---|
| Mean | Std. Dev. | Mean | Std. Dev. | |
| Total lung Dmean (Gy) | 3.5 | 1.5 | 4.1 | 1.6 |
| Treated lung Dmean (Gy) | 5.8 | 2.7 | 6.6 | 3.0 |
| Treated lung V20Gy (%) | 8.0 | 5.0 | 10.4 | 6.7 |
| Heart Dmean (Gy) | 1.7 | 1.4 | 2.1 | 1.8 |
| Heart Dmax (Gy) | 16.0 | 15.0 | 19.2 | 16.2 |
| Esophagus D5cc (Gy) | 8.3 | 7.2 | 10.1 | 7.3 |
| Esophagus Dmax (Gy) | 18.8 | 12.0 | 20.8 | 11.6 |
| PTV D2% (Gy) | 64.3 | 2.9 | 66.5 | 5.0 |
| PTV D50% (Gy) | 54.1 | 1.5 | 55.3 | 3.2 |
| PTV D95% (Gy) | 45.1 | 1.0 | 44.4 | 2.5 |
| Pneumonitis risk (%) | 7.4 | 8.9 | 11.4 | 12.1 |
| Esophagitis risk (%) | 9.3 | 12.3 | 12.2 | 13.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kraus, K.M.; Simonetto, C.; Kundrát, P.; Waitz, V.; Borm, K.J.; Combs, S.E. Potential Morbidity Reduction for Lung Stereotactic Body Radiation Therapy Using Respiratory Gating. Cancers 2021, 13, 5092. https://doi.org/10.3390/cancers13205092
Kraus KM, Simonetto C, Kundrát P, Waitz V, Borm KJ, Combs SE. Potential Morbidity Reduction for Lung Stereotactic Body Radiation Therapy Using Respiratory Gating. Cancers. 2021; 13(20):5092. https://doi.org/10.3390/cancers13205092
Chicago/Turabian StyleKraus, Kim Melanie, Cristoforo Simonetto, Pavel Kundrát, Vanessa Waitz, Kai Joachim Borm, and Stephanie Elisabeth Combs. 2021. "Potential Morbidity Reduction for Lung Stereotactic Body Radiation Therapy Using Respiratory Gating" Cancers 13, no. 20: 5092. https://doi.org/10.3390/cancers13205092
APA StyleKraus, K. M., Simonetto, C., Kundrát, P., Waitz, V., Borm, K. J., & Combs, S. E. (2021). Potential Morbidity Reduction for Lung Stereotactic Body Radiation Therapy Using Respiratory Gating. Cancers, 13(20), 5092. https://doi.org/10.3390/cancers13205092