
Effect of Exercise Training on Quality of Life after Colorectal and Lung Cancer Surgery: A Meta-Analysis

 , ,
, ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Reporting
2.2. Eligibility Criteria
2.2.1. Types of Studies
2.2.2. Type of Participants
2.2.3. Type of Intervention
2.2.4. Type of Comparison
2.2.5. Type of Outcome
2.3. Information Sources
2.4. Search Strategy
2.5. Selection of Studies
2.6. Data Extraction
2.7. Quality Assessment
2.8. Data Synthesis and Analysis
2.9. Publication Bias
3. Results
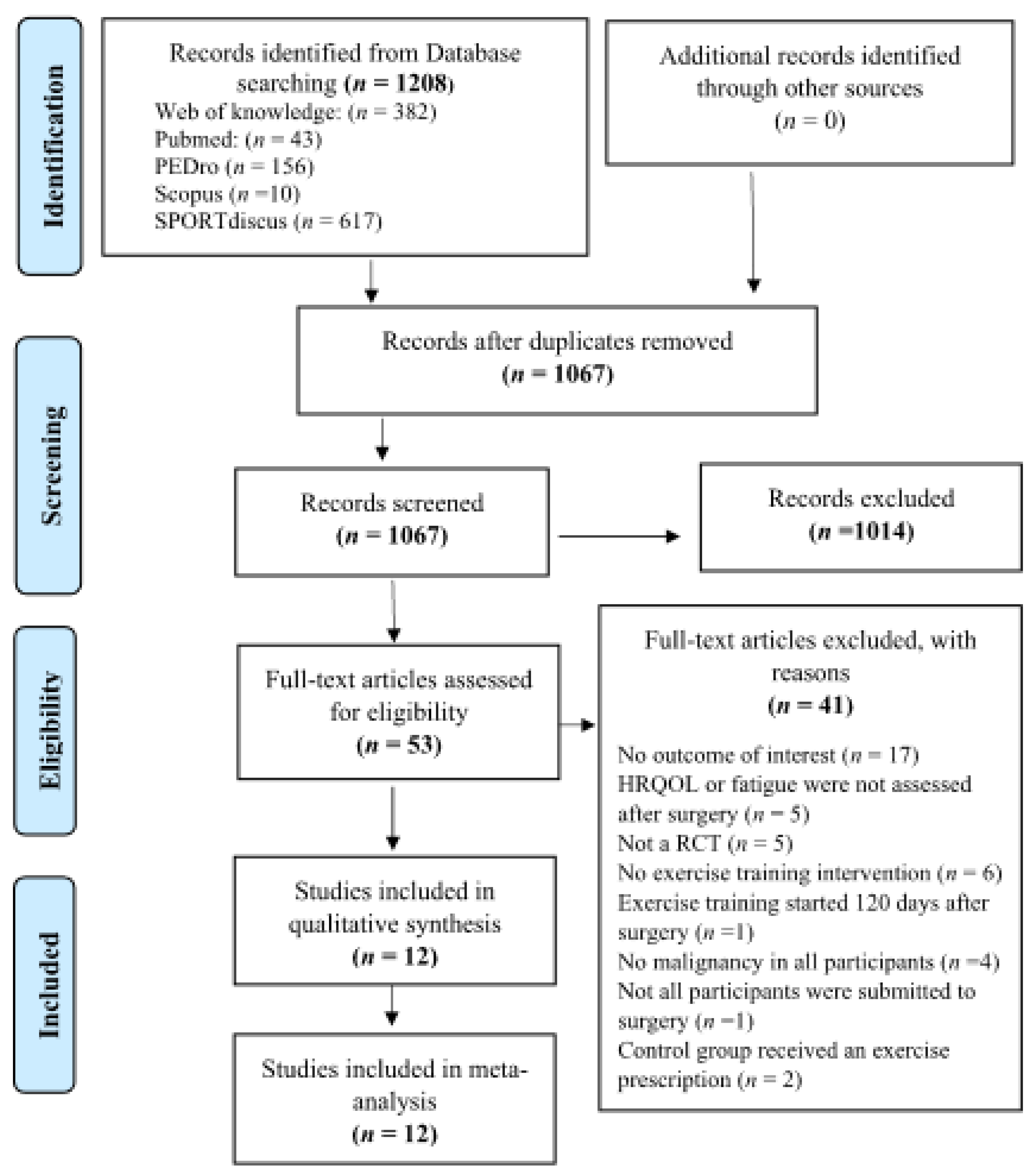
3.1. Search Results
3.2. Study Characteristics
3.3. Intervention Characteristics
3.4. Methodological Quality Assessment
3.5. Synthesis of the Results
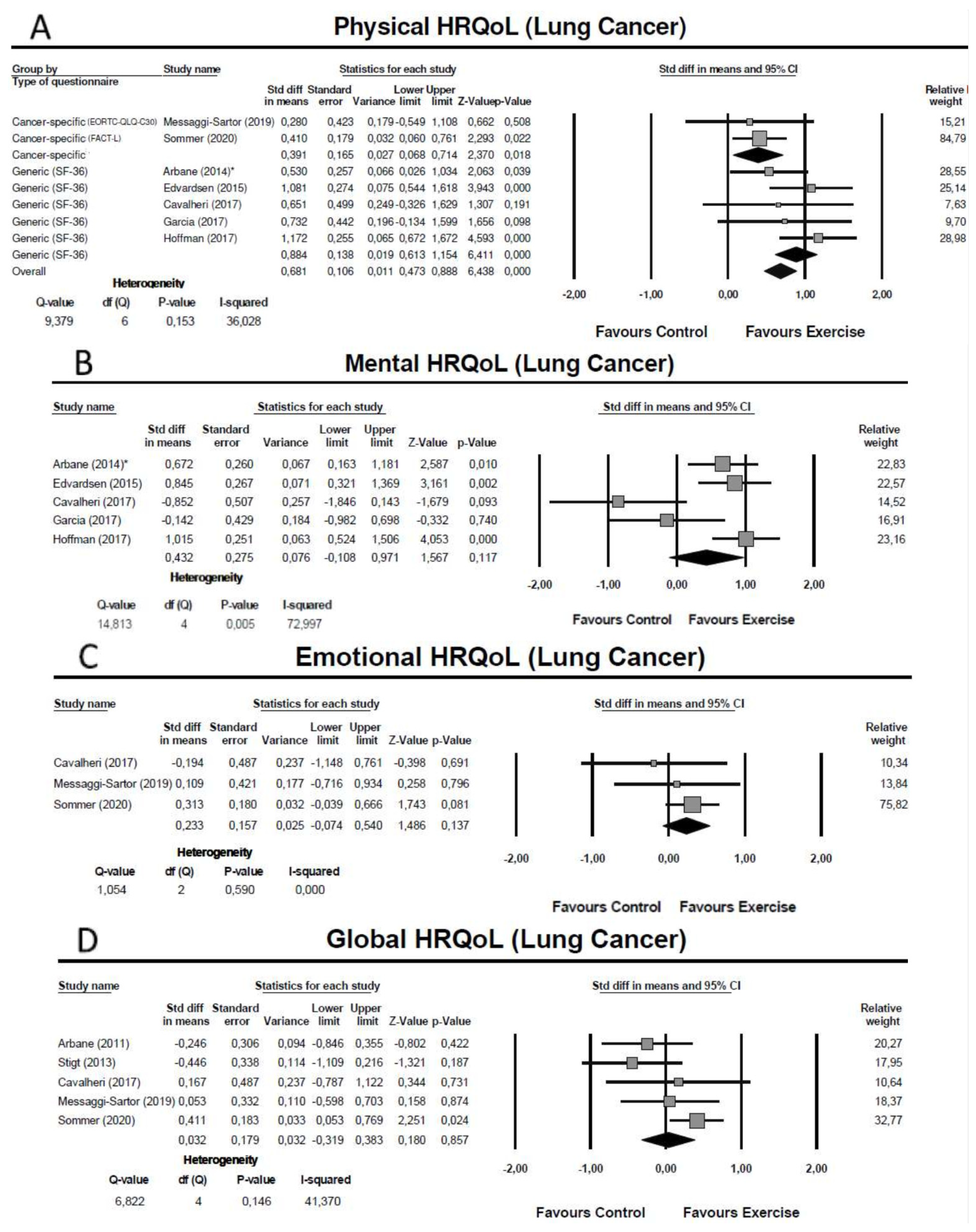
3.5.1. Lung Cancer Surgery: Effect of Exercise Training on HRQoL
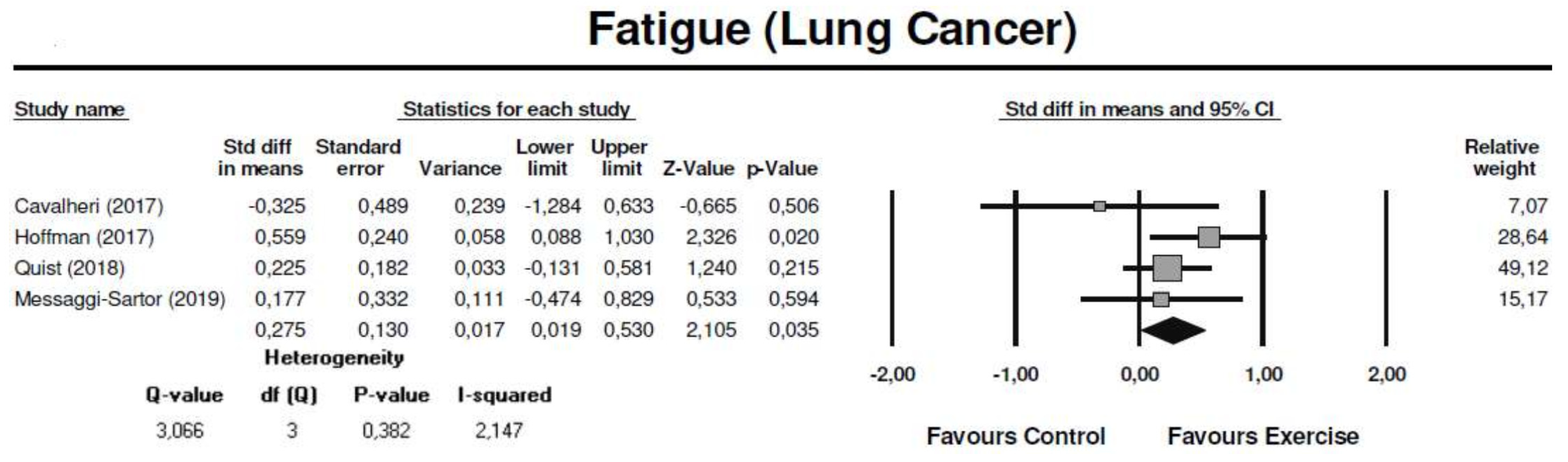
3.5.2. Lung Cancer Surgery: Effect of Exercise Training on Fatigue
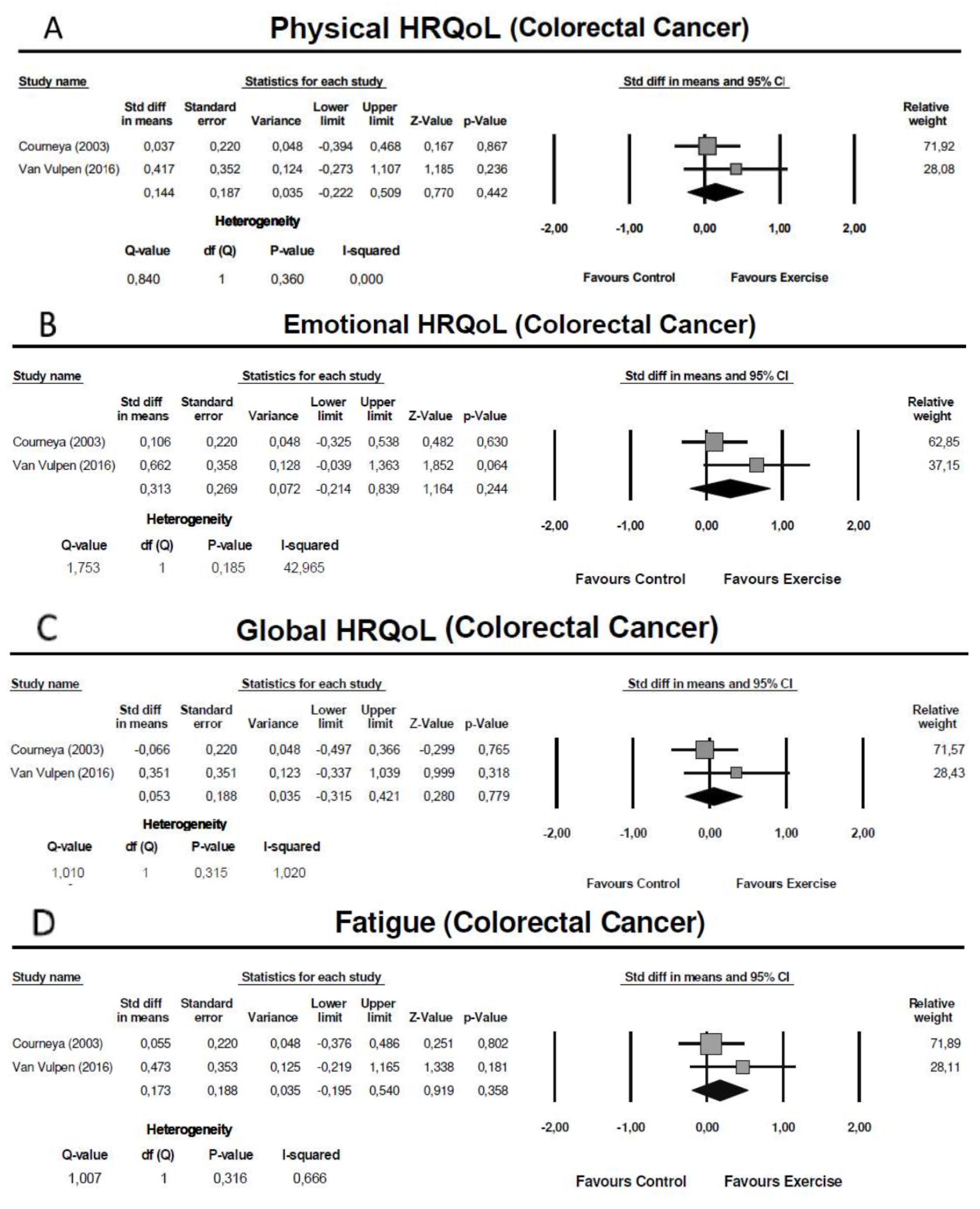
3.5.3. Colorectal Cancer Surgery: Effect of Exercise Training on HRQoL
3.5.4. Colorectal Cancer Surgery: Effect of Exercise Training on Fatigue
3.6. Publication Bias
4. Discussion
4.1. Implications for Future Research
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Bugge, A.S.; Kongerud, J.S.; Valberg, M.; Solberg, S.K.; Brustugun, O.T.; Lund, M.B. Long-term survival after surgical resection for non-small cell lung cancer. Eur. Respir. J. 2017, 50, PA4292. [Google Scholar]
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; Van de Velde, C.J.; Balmana, J.; Regula, J.; et al. Esmo consensus guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef] [PubMed]
- Avery, K.N.L.; Blazeby, J.M.; Chalmers, K.A.; Batchelor, T.J.P.; Casali, G.; Internullo, E.; Krishnadas, R.; Evans, C.; West, D. Impact on Health-Related Quality of Life of Video-Assisted Thoracoscopic Surgery for Lung Cancer. Ann. Surg. Oncol. 2020, 27, 1259–1271. [Google Scholar] [CrossRef] [PubMed]
- Nugent, S.M.; Golden, S.E.; Hooker, E.R.; Sullivan, D.R.; Thomas, C.R.; Deffebach, M.E.; Sukumar, M.S.; Schipper, P.H.; Tieu, B.H.; Moghanaki, D.; et al. Longitudinal Health-related Quality of Life among Individuals Considering Treatment for Stage i Non-Small-Cell Lung Cancer. Ann. Am. Thorac. Soc. 2020, 17, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, A.; Nakao, K.; Hiratsuka, K.; Tsunoda, Y.; Kusano, M. Prospective analysis of quality of life in the first year after colorectal cancer surgery. Acta Oncol. 2007, 46, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Kenny, P.M.; King, M.T.; Viney, R.C.; Boyer, M.J.; Pollicino, C.A.; McLean, J.M.; Fulham, M.J.; McCaughan, B.C. Quality of life and survival in the 2 years after surgery for non-small-cell lung cancer. J. Clin. Oncol. 2008, 26, 233–241. [Google Scholar] [CrossRef]
- Zieren, H.U.; Müller, J.M.; Hamberger, U.; Pichlmaier, H. Quality of life after surgical therapy of bronchogenic carcinoma. Eur. J. Cardio-Thorac. Surg. 1996, 10, 233–237. [Google Scholar] [CrossRef][Green Version]
- Win, T.; Sharples, L.; Wells, F.C.; Ritchie, A.J.; Munday, H.; Laroche, C.M. Effect of lung cancer surgery on quality of life. Thorax 2005, 60, 234–238. [Google Scholar] [CrossRef]
- Brown, L.M.; Gosdin, M.M.; Cooke, D.T.; Apesoa-Varano, E.C.; Kratz, A.L. Health-Related Quality of Life After Lobectomy for Lung Cancer: Conceptual Framework and Measurement. Ann. Thorac. Surg. 2020, 110, 1840–1846. [Google Scholar] [CrossRef]
- Poghosyan, H.; Sheldon, L.K.; Leveille, S.G.; Cooley, M.E. Health-related quality of life after surgical treatment in patients with non-small cell lung cancer: A systematic review. Lung Cancer 2013, 81, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Stamatis, G.; Leschber, G.; Schwarz, B.; Brintrup, D.L.; Ose, C.; Weinreich, G.; Passlick, B.; Hecker, E.; Kugler, C.; Dienemann, H.; et al. Perioperative course and quality of life in a prospective randomized multicenter phase III trial, comparing standard lobectomy versus anatomical segmentectomy in patients with non-small cell lung cancer up to 2 cm, stage IA (7th edition of TNM staging system). Lung Cancer 2019, 138, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Schulte, T.; Schniewind, B.; Dohrmann, P.; Küchler, T.; Kurdow, R. The extent of lung parenchyma resection significantly impacts long-term quality of life in patients with non-small cell lung cancer. Chest 2009, 135, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Wheelwright, S.; Permyakova, N.V.; Calman, L.; Din, A.; Fenlon, D.; Richardson, A.; Sodergren, S.; Smith, P.W.F.; Winter, J.; Foster, C. Does quality of life return to pre-treatment levels five years after curative intent surgery for colorectal cancer? Evidence from the ColoREctal Wellbeing (CREW) study. PLoS ONE 2020, 15, e0231332. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Mustian, K.M.; Alfano, C.M.; Heckler, C.; Kleckner, A.S.; Kleckner, I.R.; Leach, C.R.; Mohr, D.; Palesh, O.G.; Peppone, L.J.; Piper, B.F.; et al. Comparison of pharmaceutical, psychological, and exercise treatments for cancer-related fatigue: A meta-analysis. JAMA Oncol. 2017, 3, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, J.K.W.; Vincent, A.J.P.E. Exercise improves quality of life in patients with cancer: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 796–803. [Google Scholar] [CrossRef]
- Minnella, E.M.; Carli, F. Prehabilitation and functional recovery for colorectal cancer patients. Eur. J. Surg. Oncol. 2018, 44, 919–926. [Google Scholar] [CrossRef]
- Lee, J.; Lee, M.; Hong, S.; Kim, J.Y.; Park, H.; Oh, M.; In Yang, H.; Kang, D.W.; Park, J.; Kim, D.I.; et al. Association between physical fitness, quality of life, and depression in stage II–III colorectal cancer survivors. Supportive Care Cancer 2015, 23, 2569–2577. [Google Scholar] [CrossRef]
- Soares-Miranda, L.; Lucia, A.; Silva, M.; Peixoto, A.; Ramalho, R.; Da Silva, P.C.; Mota, J.; Macedo, G.; Abreu, S. Physical Fitness and Health-related Quality of Life in Patients with Colorectal Cancer. Int. J. Sports Med. 2021, 42, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Bye, A.; Sjøblom, B.; Wentzel-Larsen, T.; Grønberg, B.H.; Baracos, V.E.; Hjermstad, M.J.; Aass, N.; Bremnes, R.M.; Fløtten, Ø.; Jordhøy, M. Muscle mass and association to quality of life in non-small cell lung cancer patients. J. Cachexia Sarcopenia Muscle 2017, 8, 759–767. [Google Scholar] [CrossRef]
- Ha, D.; Ries, A.L.; Mazzone, P.J.; Lippman, S.M.; Fuster, M.M. Exercise capacity and cancer-specific quality of life following curative intent treatment of stage I-IIIA lung cancer. Support. Care Cancer 2018, 26, 2459–2469. [Google Scholar] [CrossRef] [PubMed]
- West, M.A.; Loughney, L.; Lythgoe, D.; Barben, C.P.; Sripadam, R.; Kemp, G.J.; Grocott, M.P.W.; Jack, S. Effect of prehabilitation on objectively measured physical fitness after neoadjuvant treatment in preoperative rectal cancer patients: A blinded interventional pilot study. Br. J. Anaesth. 2015, 114, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Arbane, G.; Tropman, D.; Jackson, D.; Garrod, R. Evaluation of an early exercise intervention after thoracotomy for non-small cell lung cancer (NSCLC), effects on quality of life, muscle strength and exercise tolerance: Randomised controlled trial. Lung Cancer 2011, 71, 229–234. [Google Scholar] [CrossRef]
- Gillis, C.; Fenton, T.R.; Sajobi, T.T.; Minnella, E.M.; Awasthi, R.; Loiselle, S.È.; Liberman, A.S.; Stein, B.; Charlebois, P.; Carli, F. Trimodal prehabilitation for colorectal surgery attenuates post-surgical losses in lean body mass: A pooled analysis of randomized controlled trials. Clin. Nutr. 2019, 38, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Schricker, T.; Lattermann, R. Perioperative catabolism. Can. J. Anesth./J. Can. D’anesthésie 2015, 62, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.-J.; Pudasaini, B.; Yuan, X.-T.; Li, H.F.; Shi, L.; Yuan, P. Exercise Training for Patients Pre- and Postsurgically Treated for Non-Small Cell Lung Cancer: A Systematic Review and Meta-analysis. Integr. Cancer Ther. 2017, 16, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Boereboom, C.; Doleman, B.; Lund, J.N.; Williams, J.P. Systematic review of pre-operative exercise in colorectal cancer patients. Tech. Coloproctol. 2016, 20, 81–89. [Google Scholar] [CrossRef]
- Sebio Garcia, R.; Yáñez Brage, M.I.; Giménez Moolhuyzen, E.; Granger, C.L.; Denehy, L. Functional and postoperative outcomes after preoperative exercise training in patients with lung cancer: A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 486–497. [Google Scholar] [CrossRef] [PubMed]
- Rosero, I.D.; Ramírez-Vélez, R.; Lucia, A.; Martínez-Velilla, N.; Santos-Lozano, A.; Valenzuela, P.L.; Morilla, I.; Izquierdo, M. Systematic review and meta-analysis of randomized, controlled trials on preoperative physical exercise interventions in patients with non-small-cell lung cancer. Cancers 2019, 11, 944. [Google Scholar] [CrossRef] [PubMed]
- West, M.A.; Lythgoe, D.; Barben, C.P.; Noble, L.; Kemp, G.J.; Jack, S.; Grocott, M.P.W. Cardiopulmonary exercise variables are associated with postoperative morbidity after major colonic surgery: A prospective blinded observational study. Br. J. Anaesth. 2014, 112, 665–671. [Google Scholar] [CrossRef]
- Licker, M.; Schnyder, J.M.; Frey, J.G.; Diaper, J.; Cartier, V.; Inan, C.; Robert, J.; Bridevaux, P.O.; Tschoppe, J.M. Impact of aerobic exercise capacity and procedure-related factors in lung cancer surgery. Eur. Respir. J. 2011, 37, 1189–1198. [Google Scholar] [CrossRef]
- Benzo, R.; Kelley, G.A.; Recchi, L.; Hofman, A.; Sciurba, F. Complications of lung resection and exercise capacity: A meta-analysis. Respir. Med. 2007, 101, 1790–1797. [Google Scholar] [CrossRef]
- Li, J.; Guo, N.-N.; Jin, H.-R.; Yu, H.; Wang, P.; Xu, G.G. Effects of exercise training on patients with lung cancer who underwent lung resection: A meta-analysis. World J. Surg. Oncol. 2017, 15, 158. [Google Scholar] [CrossRef] [PubMed]
- Osoba, D. Lessons learned from measuring health-related quality of life in oncology. J. Clin. Oncol. 1994, 12, 608–616. [Google Scholar] [CrossRef]
- Paull, D.E.; Thomas, M.L.; Meade, G.E.; Updyke, G.M.; Arocho, M.A.; Chin, H.W.; Adebonojo, S.A.; Little, A.G. Determinants of quality of life in patients following pulmonary resection for lung cancer. Am. J. Surg. 2006, 192, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Möller, A.; Sartipy, U. Predictors of postoperative quality of life after surgery for lung cancer. J. Thorac. Oncol. 2012, 7, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Dagnelie, P.C.; Pijls-Johannesma, M.C.G.; Lambin, P.; Beijer, S.; De Ruysscher, D.; Kempen, G.I.J.M. Impact of fatigue on overall quality of life in lung and breast cancer patients selected for high-dose radiotherapy. Ann. Oncol. 2007, 18, 940–944. [Google Scholar] [CrossRef] [PubMed]
- Vardy, J.L.; Dhillon, H.M.; Pond, G.R.; Renton, C.; Dodd, A.; Zhang, H.; Clarke, S.J.; Tannock, I.F. Fatigue in people with localized colorectal cancer who do and do not receive chemotherapy: A longitudinal prospective study. Ann. Oncol. 2016, 27, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Ichimura, H.; Kobayashi, K.; Gosho, M.; Nakaoka, K.; Yanagihara, T.; Ueda, S.; Saeki, Y.; Maki, N.; Kobayashi, N.; Kikuchi, S.; et al. Preoperative predictors of restoration in quality of life after surgery for lung cancer. Thorac. Cancer 2021, 12, 835–844. [Google Scholar] [CrossRef]
- Ihnát, P.; Martínek, L.; Mitták, M.; Vávra, P.; Rudinská, L.I.; Zonča, P. Quality of Life after Laparoscopic and Open Resection of Colorectal Cancer. Dig. Surg. 2014, 31, 161–168. [Google Scholar] [CrossRef]
- Kunz, R.; Vist, G.; Oxman, A.D. Randomisation to protect against selection bias in healthcare trials. Cochrane Database Syst. Rev. 2007, 2, MR000012. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G.; Grutsch, J.F. The Relationship Between Cancer-Related Fatigue and Patient Satisfaction with Quality of Life in Cancer. J. Pain Symptom Manag. 2007, 34, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform. Decis. Mak. 2007, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Swain, D.P.; Brawner, C.A. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- De van der Schueren, M.A.E.; Laviano, A.; Blanchard, H.; Jourdan, M.; Arends, J.; Baracos, V.E. Systematic review and meta-analysis of the evidence for oral nutritional intervention on nutritional and clinical outcomes during chemo(radio)therapy: Current evidence and guidance for design of future trials. Ann. Oncol. 2018, 29, 1141–1153. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Sherrington, C.; Herbert, R.D.; Maher, C.G.; Moseley, A.M. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man. Ther. 2000, 5, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Takeshima, N.; Sozu, T.; Tajika, A.; Ogawa, Y.; Hayasaka, Y.; Furukawa, T.A. Which is more generalizable, powerful and interpretable in meta-analyses, mean difference or standardized mean difference? BMC Med Res. Methodol. 2014, 14, 30. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Research synthesis methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Bmj 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis; Biostat: Engelwood, NJ, USA, 2005. [Google Scholar]
- Song, F.; Hooper, L.; Loke, Y.K. Publication bias: What is it? How do we measure it? How do we avoid it? Open Access J. Clin. Trials 2012, 5, 71–81. [Google Scholar] [CrossRef]
- Sebio García, R.; Yáñez-Brage, M.I.; Giménez Moolhuyzen, E.; Salorio Riobo, M.; Lista Paz, A.; Borro Mate, J.M. Preoperative exercise training prevents functional decline after lung resection surgery: A randomized, single-blind controlled trial. Clin. Rehabil. 2017, 31, 1057–1067. [Google Scholar] [CrossRef]
- Arbane, G.; Douiri, A.; Hart, N.; Hopkinson, N.S.; Singh, S.; Speed, C.; Valladares, B.; Garrod, R. Effect of postoperative physical training on activity after curative surgery for non-small cell lung cancer: A multicentre randomised controlled trial. Physiotherapy 2014, 100, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; Friedenreich, C.M.; Quinney, H.A.; Fields, A.L.A.; Jones, L.W.; Fairey, A.S. A randomized trial of exercise and quality of life in colorectal cancer survivors. Eur. J. Cancer Care 2003, 12, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Edvardsen, E.; Skjønsberg, O.H.; Holme, I.; Nordsletten, L.; Borchsenius, F.; Anderssen, S.A. High-intensity training following lung cancer surgery: A randomised controlled trial. Thorax 2015, 70, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.J.; Brintnall, R.A.; Given, B.A.; Von Eye, A.; Jones, L.W.; Brown, J.K. Using perceived self-efficacy to improve fatigue and fatigability in postsurgical lung cancer patients: A pilot randomized controlled trial. Cancer Nurs. 2017, 40, 1–12. [Google Scholar] [CrossRef]
- Messaggi-Sartor, M.; Marco, E.; Martínez-Téllez, E.; Rodriguez-Fuster, A.; Palomares, C.; Chiarella, S.; Muniesa, J.M.; Orozco-Levi, M.; Barreiro, E.; Güell, M.R. Combined aerobic exercise and high-intensity respiratory muscle training in patients surgically treated for non-small cell lung cancer: A pilot randomized clinical trial. Eur. J. Phys. Rehabil. Med. 2019, 55, 113–122. [Google Scholar] [CrossRef]
- Quist, M.; Sommer, M.S.; Vibe-Petersen, J.; Stærkind, M.B.; Langer, S.W.; Larsen, K.R.; Trier, K.; Christensen, M.; Clementsen, P.F.; Missel, M.; et al. Early initiated postoperative rehabilitation reduces fatigue in patients with operable lung cancer: A randomized trial. Lung Cancer 2018, 126, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Stigt, J.A.; Uil, S.M.; Van Riesen, S.J.H.; Simons, F.J.N.A.; Denekamp, M.; Shahin, G.M.; Groen, H.J.M. A randomized controlled trial of postthoracotomy pulmonary rehabilitation in patients with resectable lung cancer. J. Thorac. Oncol. 2013, 8, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Van Vulpen, J.K.; Velthuis, M.J.; Bisschop, C.N.S.; Travier, N.; Van Den Buijs, B.J.W.; Backx, F.J.G.; Los, M.; Erdkamp, F.L.G.; Bloemendal, H.J.; Koopman, M.; et al. Effects of an exercise program in colon cancer patients undergoing chemotherapy. Med. Sci. Sports Exerc. 2016, 48, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Sommer, M.S.; Vibe-Petersen, J.; Stærkind, M.B.; Langer, S.W.; Larsen, K.R.; Trier, K.; Christensen, M.; Clementsen, P.F.; Missel, M.; Christensen, K.B.; et al. Early initiated postoperative rehabilitation enhances quality of life in patients with operable lung cancer: Secondary outcomes from a randomized trial. Lung Cancer 2020, 146, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Cavalheri, V.; Jenkins, S.; Cecins, N.; Gain, K.; Phillips, M.J.; Sanders, L.H.; Hill, K. Exercise training for people following curative intent treatment for non-small cell lung cancer: A randomized controlled trial. Braz. J. Phys. Ther. 2017, 21, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Cavalheri, V.; Burtin, C.; Formico, V.R.; Nonoyama, M.L.; Jenkins, S.; Spruit, M.A.; Hill, K. Exercise training undertaken by people within 12 months of lung resection for non-small cell lung cancer. Cochrane Database Syst. Rev. 2019, 6, CD009955. [Google Scholar] [CrossRef] [PubMed]
- Buffart, L.M.; Sweegers, M.G.; May, A.M.; Chinapaw, M.J.; van Vulpen, J.K.; Newton, R.U.; Galvão, D.A.; Aaronson, N.K.; Stuiver, M.M.; Jacobsen, P.B.; et al. Targeting Exercise Interventions to Patients With Cancer in Need: An Individual Patient Data Meta-Analysis. J. Natl. Cancer Inst. 2018, 110, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Pompili, C.; Brunelli, A.; Xiumé, F.; Refai, M.; Salati, M.; Socci, L.; Di Nunzio, L.; Sabbatini, A. Prospective external convergence evaluation of two different quality-of-life instruments in lung resection patients. Eur. J. Cardio-Thorac. Surg. 2011, 40, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Cykert, S.; Kissling, G.; Hansen, C.J. Patient preferences regarding possible outcomes of lung resection: What outcomes should preoperative evaluations target? Chest 2000, 117, 1551–1559. [Google Scholar] [CrossRef] [PubMed]
- Schulte, T.; Schniewind, B.; Walter, J.; Dohrmann, P.; Küchler, T.; Kurdow, R. Age-related impairment of quality of life after lung resection for non-small cell lung cancer. Lung Cancer 2010, 68, 115–120. [Google Scholar] [CrossRef]
- Steffens, D.; Beckenkamp, P.R.; Young, J.; Solomon, M.; da Silva, T.M.; Hancock, M.J. Is preoperative physical activity level of patients undergoing cancer surgery associated with postoperative outcomes? A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2019, 45, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Fresard, I.; Licker, M.; Adler, D.; Lovis, A.; Robert, J.; Karenovics, W.; Diaper, J.; Janssens, J.P.; Triponez, F.; Lador, F.; et al. Preoperative Peak Oxygen Uptake in Lung Cancer Subjects With Neoadjuvant Chemotherapy: A Cross-Sectional Study. Respir. Care 2016, 61, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, A.; Belardinelli, R.; Refai, M.; Salati, M.; Socci, L.; Pompili, C.; Sabbatini, A. Peak oxygen consumption during cardiopulmonary exercise test improves risk stratification in candidates to major lung resection. Chest 2009, 135, 1260–1267. [Google Scholar] [CrossRef] [PubMed]
- Lindenmann, J.; Fink-Neuboeck, N.; Fediuk, M.; Maier, A.; Kovacs, G.G.; Balic, M.; Smolle, J.; Smolle-Juettner, F.M. Preoperative peak oxygen consumption: A predictor of survival in resected lung cancer. Cancers 2020, 12, 836. [Google Scholar] [CrossRef]
- Adams, S.C.; DeLorey, D.S.; Davenport, M.H.; Fairey, A.S.; North, S.; Courneya, K.S. Effects of high-intensity interval training on fatigue and quality of life in testicular cancer survivors. Br. J. Cancer 2018, 118, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Lorente, D.; Navarro-Ripoll, R.; Guzman, R.; Moises, J.; Gimeno, E.; Boada, M.; Molins, L. Prehabilitation in thoracic surgery. J. Thorac. Dis. 2018, 10, S2593–S2600. [Google Scholar] [CrossRef] [PubMed]
- Murias, J.M.; Kowalchuk, J.M.; Paterson, D.H. Time course and mechanisms of adaptations in cardiorespiratory fitness with endurance training in older and young men. J. Appl. Physiol. 2010, 108, 621–627. [Google Scholar] [CrossRef] [PubMed]
- West, M.A.; Jack, S.; Grocott, M.P.W. Prehabilitation before surgery: Is it for all patients? Best Pract. Res. Clin. Anaesthesiol. 2021. [Google Scholar] [CrossRef]
- Schauer, T.; Mazzoni, A.S.; Henriksson, A.; Demmelmaier, I.; Berntsen, S.; Raastad, T.; Nordin, K.; Pedersen, B.K.; Christensen, J.F. Exercise intensity and markers of inflammation during and after (neo-) adjuvant cancer treatment. Endocr.-Relat. Cancer 2021, 28, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Chu, S.; Gao, Y.; Ai, Q.; Liu, Y.; Li, X.; Chen, N. A Narrative Review of Cancer-Related Fatigue (CRF) and Its Possible Pathogenesis. Cells 2019, 8, 738. [Google Scholar] [CrossRef]
- Demmelmaier, I.; Brooke, H.L.; Henriksson, A.; Mazzoni, A.S.; Bjørke, A.C.H.; Igelström, H.; Ax, A.K.; Sjövall, K.; Hellbom, M.; Pingel, R.; et al. Does exercise intensity matter for fatigue during (neo-)adjuvant cancer treatment? The Phys-Can randomized clinical trial. Scand. J. Med. Sci. Sports 2021, 31, 1144–1159. [Google Scholar] [CrossRef]
- Van Zutphen, M.; Winkels, R.M.; van Duijnhoven, F.J.B.; van Harten-Gerritsen, S.A.; Kok, D.E.G.; van Duijvendijk, P.; van Halteren, H.K.; Hansson, B.M.E.; Kruyt, F.M.; Bilgen, E.J.S.; et al. An increase in physical activity after colorectal cancer surgery is associated with improved recovery of physical functioning: A prospective cohort study. BMC Cancer 2017, 17, 74. [Google Scholar] [CrossRef]
- Brown, J.C.; Huedo-Medina, T.B.; Pescatello, L.S.; Pescatello, S.M.; Ferrer, R.A.; Johnson, B.T. Efficacy of exercise interventions in modulating cancer-related fatigue among adult cancer survivors: A meta-analysis. Cancer Epidemiol. Biomark. Prev. 2011, 20, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Saltaji, H.; Da Costa, B.R.; Fuentes, J.; Ha, C.; Cummings, G.G. What is the influence of randomization sequence generation and allocation concealment on treatment effects of physical therapy trials? A meta-epidemiological study. BMJ Open 2015, 5, e008562. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Huang, D.; Wen, J.; Wang, Y.; Rosman, L.; Chen, Q.; Robinson, K.A.; Gagnier, J.J.; Ehrhardt, S.; Celentano, D.D. Assessment of Language and Indexing Biases among Chinese-Sponsored Randomized Clinical Trials. JAMA Netw. Open 2020, 3, 205894. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Sample Size/Sex/Age (Mean) | Type of Cancer/Stage | Surgical Approach | Timing of Intervention | Exercise Group | Control Group | Primary Outcome | Assessment (HRQoL/ Fatigue) | Key Findings (HRQoL/Fatigue) |
|---|---|---|---|---|---|---|---|---|---|
| Courneya et al., 2003 [59] | E.G (n = 62) M = 34; F = 28 59.9 years C.G (n = 31) M = 20; F = 11 61.1 years | CRC Stage III-IV (82.4%) Node stage 0 (60%) Metastatic (3.5%) | Not reported (19.4% of patients submitted to colostomy) | Post-surgery (mean of 73 days) | Home-based Aerobic exercise | Usual care (no exercise training) | HRQoL | FACT-G and FACT-F | No between-group differences observed in HRQoL and fatigue |
| Arbane et al., 2011 [24] | E.G. (n = 26) Sex not reported 62.6 years C.G. (n = 25) Sex not reported: 65.4 years | NSCLC Stage I–IV | VATS (n = 2) Open Thoracotomy (n = 49) | Post-Surgery (1st postoperative day) | Aerobic exercise + Resistance exercise + Mobility exercises | Usual care (Routine physiotherapy treatments, airway clearance techniques, mobilization and upper limb activities) | Exercise capacity | EORTC-QLQ-C30 | No between-group differences observed in HRQoL |
| Stigt et al., 2013 [64] | E.G (n = 23) M = 21; F = 2 63.6 years C.G (n = 26) M = 19; F = 7 63.2 years | NSCLC Stage not reported | Open Thoracotomy (n = 49) | Post-surgery (4 weeks after hospital discharge) | Aerobic exercise + Resistance exercise | Usual care (routine outpatient appointments after discharge, pain medication) | HRQoL | SGRQ | No between-group differences observed in HRQoL |
| Arbane et al., 2014 [58] | E.G. (n = 64) M = 29; F = 35 67 years C.G. (n = 67) M = 43; F = 24 68 years | NSCLC Stage I-IV | VATS (n = 38) Open Thoracotomy (n = 90) Unknown (n = 3) | Post-Surgery (1st postoperative day) | Aerobic exercise + Resistance exercise (In-hospital) + Home-based walking Program | Usual care (Routine physiotherapy treatments, airway clearance techniques, mobilization, and upper limb activities) | Physical activity levels | SF-36 |  Significant difference between groups in PCS and MCS in patients with airflow obstruction |
| Edvardsen et al. 2015 [60] | E.G. (n = 30) M = 13; F = 17 64.4 years C.G. (n = 31) M = 15; F = 16 65.9 years | NSCLC Stage I-IV | VATS (n = 10) Open Thoracotomy (n = 51) | Post-surgery (5 to 7 weeks after surgery) | HIIT + Resistance exercise + daily inspiratory muscle training | Standard postoperative care (no advice about exercise training) | Exercise capacity | SF-36 and EORTC-QLQ-C30 | Significant difference between groups in PCS, MCS and dyspnea, favoring the exercise group |
| Van Vulpen et al., 2016 [65] | E.G. (n = 17) M= 10; F= 7 58.1 years C.G. (n = 16) M= 11; F= 5 58.1 years | Colon cancer Stage M0 | Laparoscopic (n = 13) Open surgery (n = 18) Unknown (n = 2) | Post-surgery (10 weeks after surgery, during adjuvant chemotherapy) | Aerobic exercise (Interval training) + Resistance Exercise | Usual Care (no exercise intervention and instruction for the continuation of the usual activities) | Fatigue | EORTC-QLQ-C30, MFI | Significant difference between groups in physical function and both physical and general fatigue, favoring the exercise group. |
| Cavalheri et al., 2017 [67] | E.G. (n = 9) M= 3; F= 6 66 years C.G. (n = 8) M= 2; F= 6 68 years | NSCLC Stage I-IIIA | VATS (n = 9) Open Thoracotomy (n = 8) | Post-surgery (6 to 10 weeks after lobectomy or 4 to 8 weeks after last chemotherapy cycle) | Aerobic exercise (Continuous training and HIIT) + Resistance Exercise | General Instructions on daily activities + weekly phone calls | Exercise capacity | SF-36, EORTC-QLQ-C30, FACT-L and FACIT-F | No between-group differences observed in HRQoL and fatigue |
| Garcia et al., 2017 [57] | E.G (n = 10) M = 9; F = 1 70.9 years C.G (n = 12) M = 11; F = 1 69.4 years | NSCLC Stage not reported | VATS (n = 22) | Pre-surgery (baseline assessment was 54.5 days before surgery) | HIIT + Resistance Exercise + Breathing exercises (incentive spirometer) | Usual care (no exercise training) | Exercise capacity | SF-36 | Significant difference between groups in PCS, favoring the exercise group |
| Hoffman et al., 2017 [61] | E.G (n = 37) M = 17; F = 20 64.4 years C.G (n = 35) M = 15; F = 20 65.6 years | NSCLC Stage I-IV | VATS (n = 13) Open Thoracotomy (n = 59) | Post-surgery (mean of 4 days after hospital discharge) | Home-based aerobic exercise + balance Training | Usual care from health providers plus a pedometer with instructions on how to record the total number of steps per day | Feasibility and acceptability | SF-36 and BFI | Significant difference between groups in the PCS 3 months after surgery, favoring the preoperative exercise group |
| Quist et al., 2018 [63] and Sommer et al. 2020 [66] | E.G (n = 110) M = 46; F = 64 66 years C.G (n = 101) M = 48; F = 53 65 years | NSCLC Stage IA-IIIB | VATS (n = 110) Open Thoracotomy (n = 101) | Post-surgery (14 days after surgery: early intervention) | HIIT + Resistance exercise + breathing exercises combined with stretching and tension-release techniques | Usual care (postoperative exercise initiated 14 weeks after surgery: late intervention) | Exercise capacity * | EORTC-QLQ-C30 and FACT-L | Significant difference between groups in fatigue and HRQoL 14 weeks after surgery favoring the early initiated intervention |
| Messaggi-Sartor et al., 2019 [62] | E.G (n = 16) M = 8; F = 8 64.2 years C.G (n = 21) M = 18; F = 3 64.8 years | NSCLC Stage I-II | VATS (n = 3) Open Thoracotomy (n = 34) | Post-surgery (6–8 weeks after lung resection) | Aerobic exercise + Resistance exercise + Respiratory muscle training | Advice to perform physical activity, following WHO recommendations. | Exercise capacity | EORTC-QLQ-C30 | No between-group differences observed in HRQoL |
Significant differences between the exercise group and the control group; No between-group differences. * Measurement at 14 weeks after surgery (end of the early initiated exercise intervention), BFI (Brief fatigue inventory); C.G (Control Group); CRC (Colorectal cancer); E.G (Exercise Group); EORTC-QLQ-C30 (European Organization for Research and Treatment of Cancer questionnaire); FACIT-F (Functional Assessment of Chronic Illness Therapy—Fatigue); FACT-F (Functional assessment of cancer therapy—Fatigue); FACT-G (Functional assessment of cancer therapy—General); FACT-L (Functional assessment of cancer therapy—Lung); HIIT (High Intensity Interval Training); HRQOL (Health-related quality of life); M (Male); MCS (Mental Component Summary); MFI (Multidimensional Fatigue Inventory); NSCLC (Non-small cell lung cancer); F (Female); PCS (Physical Component Summary); SF-36 (Short-Form 36-Item Health Survey; VATS (Video-assisted thoracoscopic surgery); WHO (Word Health Organization).| Reference | Type of Supervision | Type/Mode of Exercise | Time (min/sets)/Intensity (MET; % HRmax; %HRR;% Wpeak; % 1- RM) | Progression (Time/Sets/Intensity) | Session Time (min) | Frequency (Sessions Per Week) | Program Duration (Weeks/Sessions) | Adverse Events (A.E) Attrition/Adhrence Rates |
|---|---|---|---|---|---|---|---|---|
| Aerobic Exercise | ||||||||
| Courneya et al., 2003 [59] | Telephone (weekly telephone calls) | Aerobic: Swimming, cycling or walking | Aerobic: 20–30 min 65–75% of predicted HRmax. | Aerobic: Varied depending on motivation and capability | 20–30 min | 3–5 times per week | 16 weeks | A.E: NR Adherence: 76% Attrition: 10% |
| Hoffman et al., 2017 [61] | Mixed supervision: presential (two home visits) and by telephone | Aerobic: Continuous walking in place with Wii Fit Plus exercise equipment Balance exercises: Wii balance exercises | Aerobic: 5 min each day for 5 days during week 1 Light intensity (less than 3.0 METs) | Aerobic: The walking time was increased by 5 min each week with the goal of 30 min per day during week 6 | 5 min (1st week) to 30 min (6th week) | 5 times per week | 6 weeks | A.E: No adverse events Adhrence:93% Attrition:3% |
| Aerobic + Resistance Exercise | ||||||||
| Arbane et al., 2011 [24] | Presential in hospital and three home visits during the home-based program | Aerobic: Walking Resistance: Seated leg raises and unspecified home resistance exercises | Aerobic: 60% to 80% HRmax (220-age formula) Resistance (in-hospital): Ankle weights of 2 lb. | Resistance (in-hospital): Progress to ankle weights of 4 lb | NR | In hospital: 5 times per week/twice daily Home-based: NR | In-Hospital: 5 days Home-based: 12 weeks | A.E: NR Adherence: NR Attrition: 17% |
| Stigt et al., 2013 [64] | Presential | Aerobic: Continuous training on a cyclo-ergometer Resistance: Dose not reported | Aerobic: 60% to 80% of peak workload | NR | 60 min | 2 times per week | 12 weeks | A.E: NR Adherence: NR Attrition:26.5% |
| Arbane et al., 2014 [58] | Mixed supervision: Presential (In hospital program) and weekly telephone calls (home program) | Aerobic: Cycling (in hospital) and home-based walking program (SPACE) Resistance: NR | Aerobic: 30 min 60% to 90% of HRR 3 or 4 on the Borg CR10 13 to 15 on the Borg RPE Pedalling rate was held between 50 and 60 rpm Resistance: 10-RM (number of. Sets NR) | NR | NR | NR | In Hospital: 5 days Home-based: 20 weeks | A.E: NR Adherence: NR Attrition: 31% |
| Van Vulpen et al., 2016 [65] | Presential (In-hospital) | Aerobic: Interval training on a cycle-ergometer Resistance: Exercises for major muscle groups (arms, legs, shoulder and trunk) | Aerobic High intensity: 3 sets x 2 min at the first VT measured by CPET Low intensity: 3 sets x 4 min below the first VT Resistance: 2 sets x 10 reps at 65% of 1-RM | Aerobic High intensity: 2 sets x 7 min at the first VT Low intensity: 1 set x 7 min at the first VT Resistance: 1 set x 10 reps (75% 1-RM) and 2 sets x 20 reps (45% 1-RM) | 60 min | 2 sessions per week | 18 weeks | A.E: No serious adverse events Adherence: 89% Attrition:15% |
| Cavalheri et al., 2017 [67] | Presential (In-hospital) | Aerobic: Continuous walking on treadmill or 100-m corridor + HIIT on a cycle-ergometer Resistance: Exercises for upper and lower limbs using hand weights (step-ups, elbow flexion and shoulder abduction) | Walking on corridor—20 min at 80% of the average 6MWT speed Treadmill walking—20 min at 70% of the average 6MWT speed Cycling (HIIT): 14 min High intensity (2 × 2 min at 80% of the peak workload) Low intensity (10 min at 60% of the peak workload) Resistance training: 2–3 sets of 10 reps; Initial hand weights: 1.5 kg for women and 2 kg for men | Aerobic: Walking speed was increased if the patients were able to walk for 20 min continuously providing symptoms and SpO2 were within acceptable limits (≥88%) | 60 min | 3 sessions per week | 8 weeks | A.E: NR Adherence: 44% Attrition: 0% |
| Garcia et al., 2017 [57] | Presential (In-Hospital) | Aerobic: HIIT on a cycle-ergometer Resistance: 6 exercises using elastic bands and body weight, targeting the main muscle groups. | Aerobic: 30 min High intensity (1 min at 80% of peak workload) Low intensity (4 min at 50% of peak workload) Resistance: 3 sets of 15 reps (45” rest) Moderate perceived rate of exhaustion (OMNI Scale) | Aerobic: Peak workload adjusted based on an incremental cycle test (10th session) Resistance: Number of sets was increased to four if tolerated (10th session) | 60 min | 3–5 times per week depending on the surgery date | 16 sessions (range 8–25) | A.E: No adverse Events Adherence: NR Attrition: 14% |
| Quist et al., 2018 [63] and Sommer et al. [66] | Presential (Rehabilitation center) | Aerobic: HIIT on a cycle-ergometer Resistance: 5 exercises using weight machines (leg press, chest press, leg extension, pull to chest, and pull down) | Aerobic: 25 min High intensity (1–2 min at 85%–100% of HRmax) Low intensity: (1-min pauses) Resistance: 3 sets of 5 to12 reps at 60–80% of 1-RM | Aerobic: 50–60% of HRmax. (first 4 weeks) and 70–90% of HRmax (last 8 weeks) Resistance: Every two weeks, the load was increased and the number of repetitions reduced to a final of 3 sets of 8 reps | 60 min | 2 times per week | 12 weeks (24 sessions on nonconsecutive days) | A.E: NR Adherence: NR Attrition: 40% |
| Aerobic + Resistance + Respiratory Muscle Exercise | ||||||||
| Edvardsen et al., 2015 [60] | Presential (Fitness center) | Aerobic: HIIT (walking uphill on treadmill) Resistance: Leg press, leg extension, back extension, seat row, bicep curls, chest-and-shoulder press Inspiratory muscle training | Aerobic: HIIT achieving 80–95% of the HRmax. Resistance training: 3 sets of 6–12 RM Inspiratory muscle training: NR | Aerobic: The intensity and duration of each interval was individually increased based on the patient’s improvement and symptoms of fatigue and dyspnoea | 60 min | 3 times per week | 20 weeks | A.E: Hip fracture during balance training Adherence: 88% Attrition: 12% |
| Messaggi-Sartor et al., 2019 [62] | Presential (In-Hospital) | Aerobic: Continuous training on a cycle-ergometer IEMT: Using a respiratory muscle trainer at a rate of 15–20 breaths/min Resistance: 3 exercises (bicep curl, chest and shoulder press | Aerobic: 30 min 60% of peak workload IEMT: 5 sets of 10 repetitions followed by 1–2 min of unloaded recovery breathing (off the device) 50% of PImax and PEmax; Resistance: 3 sets with a constant load of 0.5 kg. | Aerobic: Increased in workload by 5 watts weekly if the patient was able to tolerate the set load for 30 min IEMT: Load was adjusted weekly by 10 cmH2O if tolerated | 60 min | 3 times per week (IEMT: twice a day) | 8 weeks (24 sessions) | A.E: No adverse events Adherence: >80% Attrition: 35% |
| Reference | Eligibility Criteria * | Randomized Allocation | Hidden Allocation | Baseline Comparison Between Groups | Blind Participants | Blind Physical Therapists | Blind Assessors | Proper Follow-Up | Intention to Treat Analysis | Comparison Between Groups | Point Estimate and Variability | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Courneya et al., 2003 [59] | √ | √ | × | √ | × | × | √ | √ | √ | √ | √ | 7/10 |
| Arbane et al., 2011 [24] | √ | √ | √ | √ | × | × | √ | √ | × | √ | √ | 7/10 |
| Stigt et al., 2013 [64] | √ | √ | × | √ | × | × | × | × | √ | √ | √ | 5/10 |
| Arbane et al., 2014 [58] | √ | √ | √ | √ | × | × | × | × | √ | √ | √ | 6/10 |
| Edvardsen et al. 2015 [60] | √ | √ | √ | √ | × | × | × | √ | √ | √ | √ | 7/10 |
| Van Vulpen et al., 2016 [65] | √ | √ | √ | √ | × | × | × | √ | √ | √ | √ | 7/10 |
| Cavalheri et al., 2017 [67] | √ | √ | √ | √ | × | × | √ | × | √ | √ | √ | 7/10 |
| Garcia et al., 2017 [57] | √ | √ | √ | √ | × | × | √ | × | × | √ | √ | 6/10 |
| Hoffman et al., 2017 [61] | √ | √ | × | √ | × | × | × | × | √ | √ | √ | 5/10 |
| Quist et al., 2018 [63] | √ | √ | × | √ | × | × | √ | × | √ | √ | √ | 6/10 |
| Messaggi-Sartor et al., 2019 [62] | √ | √ | √ | √ | × | × | √ | × | × | √ | √ | 6/10 |
| Sommer et al., 2020 [66] | √ | √ | × | √ | × | × | √ | × | √ | √ | √ | 6/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, P.; Pimenta, S.; Oliveiros, B.; Ferreira, J.P.; Martins, R.A.; Cruz, J. Effect of Exercise Training on Quality of Life after Colorectal and Lung Cancer Surgery: A Meta-Analysis. Cancers 2021, 13, 4975. https://doi.org/10.3390/cancers13194975
Machado P, Pimenta S, Oliveiros B, Ferreira JP, Martins RA, Cruz J. Effect of Exercise Training on Quality of Life after Colorectal and Lung Cancer Surgery: A Meta-Analysis. Cancers. 2021; 13(19):4975. https://doi.org/10.3390/cancers13194975
Chicago/Turabian StyleMachado, Pedro, Sara Pimenta, Bárbara Oliveiros, José Pedro Ferreira, Raul A. Martins, and Joana Cruz. 2021. "Effect of Exercise Training on Quality of Life after Colorectal and Lung Cancer Surgery: A Meta-Analysis" Cancers 13, no. 19: 4975. https://doi.org/10.3390/cancers13194975
APA StyleMachado, P., Pimenta, S., Oliveiros, B., Ferreira, J. P., Martins, R. A., & Cruz, J. (2021). Effect of Exercise Training on Quality of Life after Colorectal and Lung Cancer Surgery: A Meta-Analysis. Cancers, 13(19), 4975. https://doi.org/10.3390/cancers13194975