
Prediction of Early Distant Recurrence in Upfront Resectable Pancreatic Adenocarcinoma: A Multidisciplinary, Machine Learning-Based Approach

 ,
,  , , ,
, , , 

Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
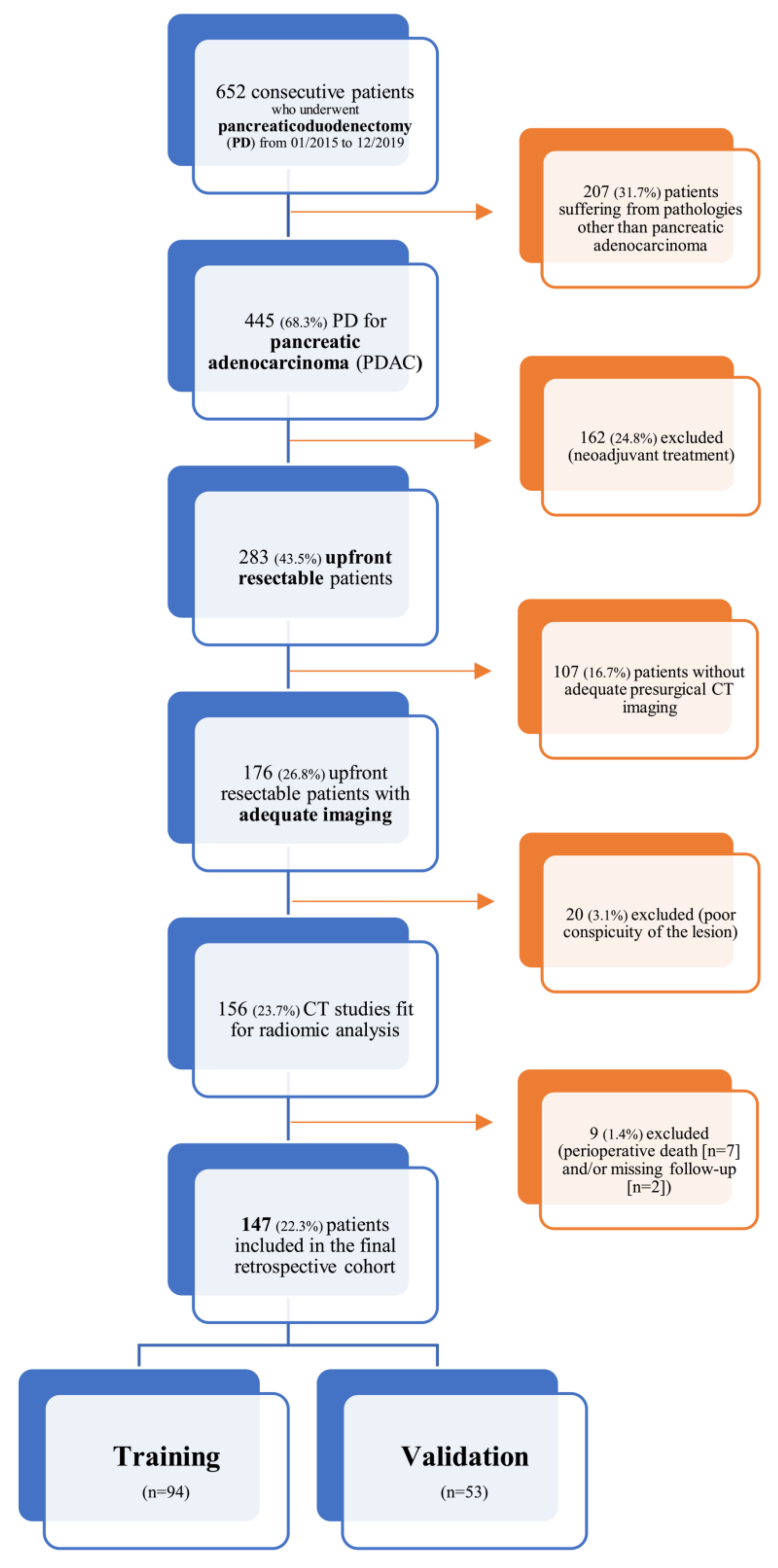
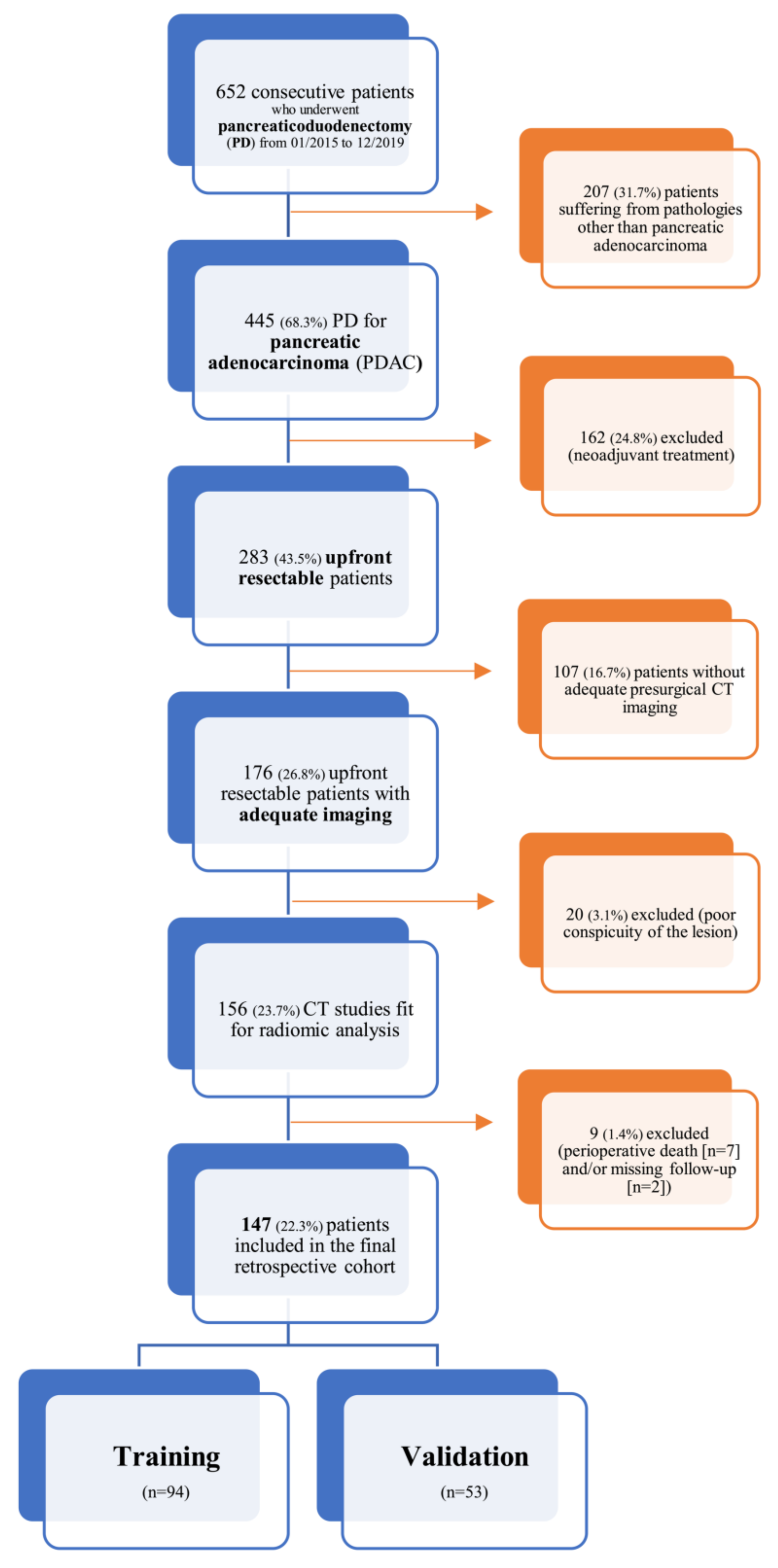
2.1. Patients’ Cohort
2.2. Surgical Technique, Pathology Protocol, Adjuvant Therapy and Follow-Up Data Collection
2.3. Clinical Variables
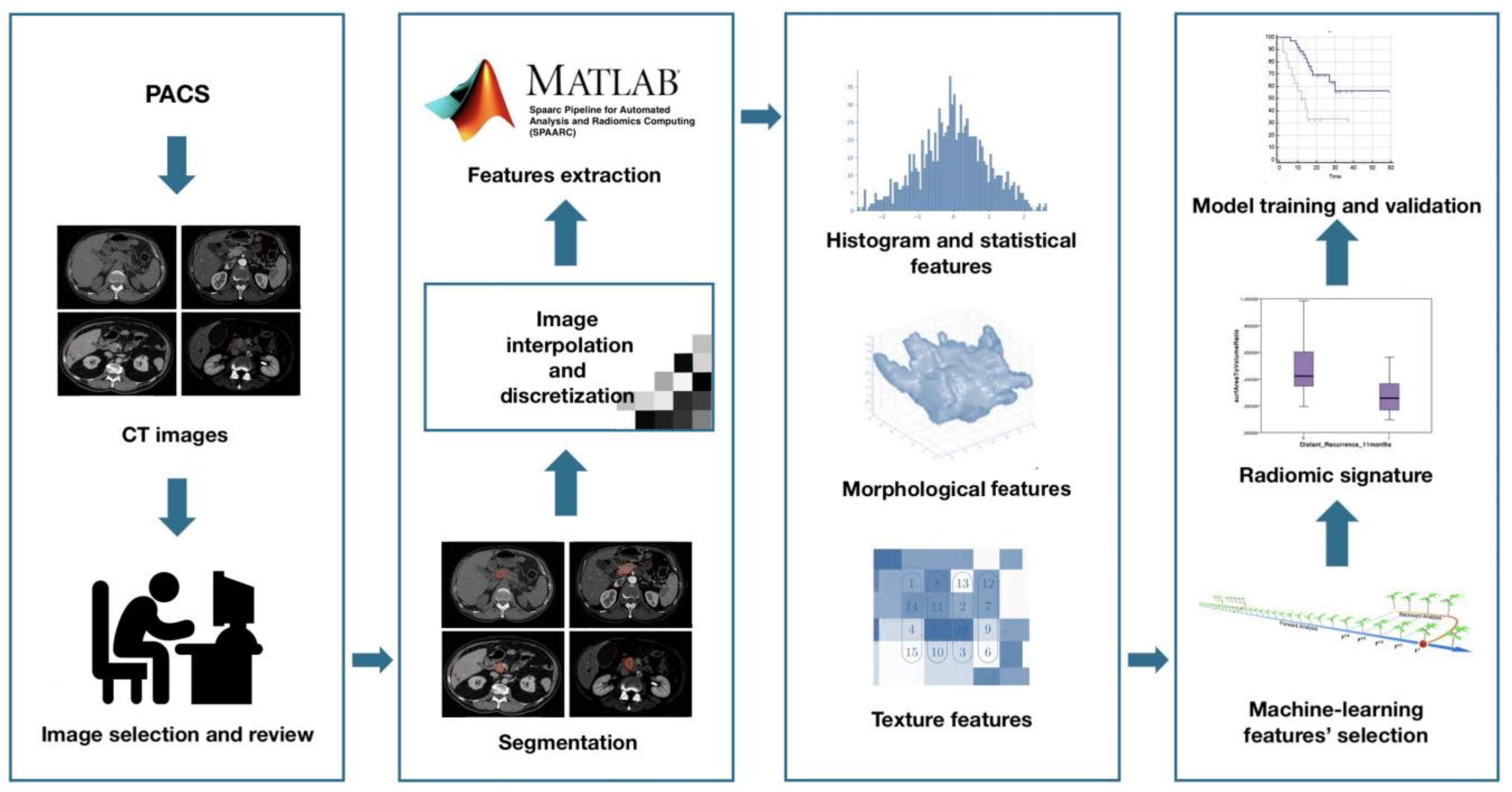
2.4. Radiological Variables and Radiomic Features
2.5. Statistical Analysis
3. Results
3.1. Patients’ Cohort
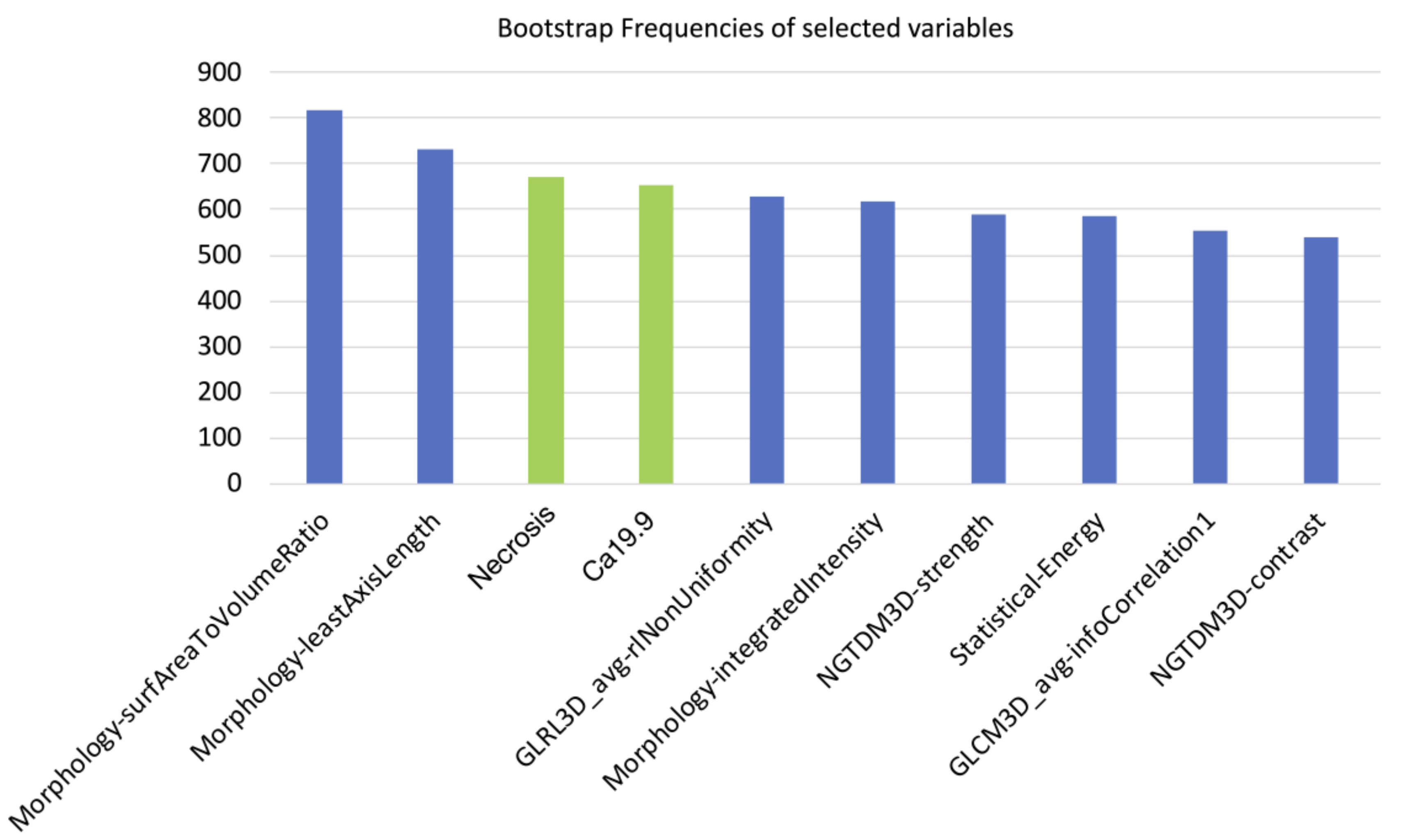
3.2. Variables Selection
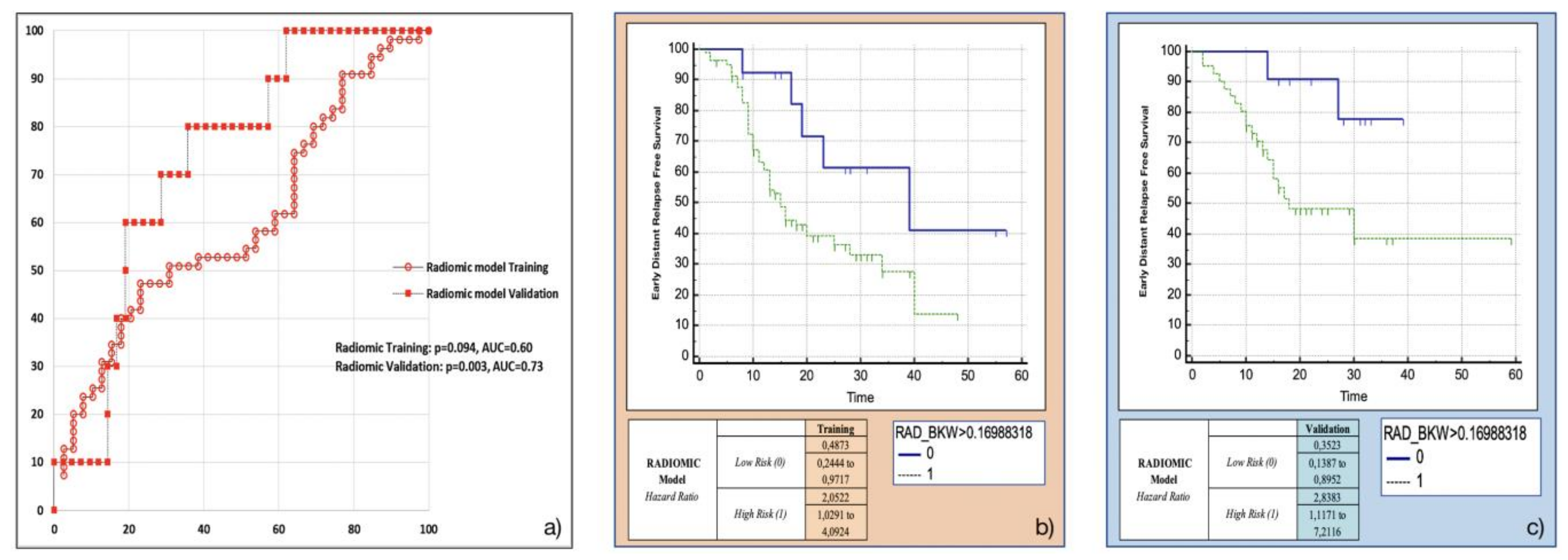
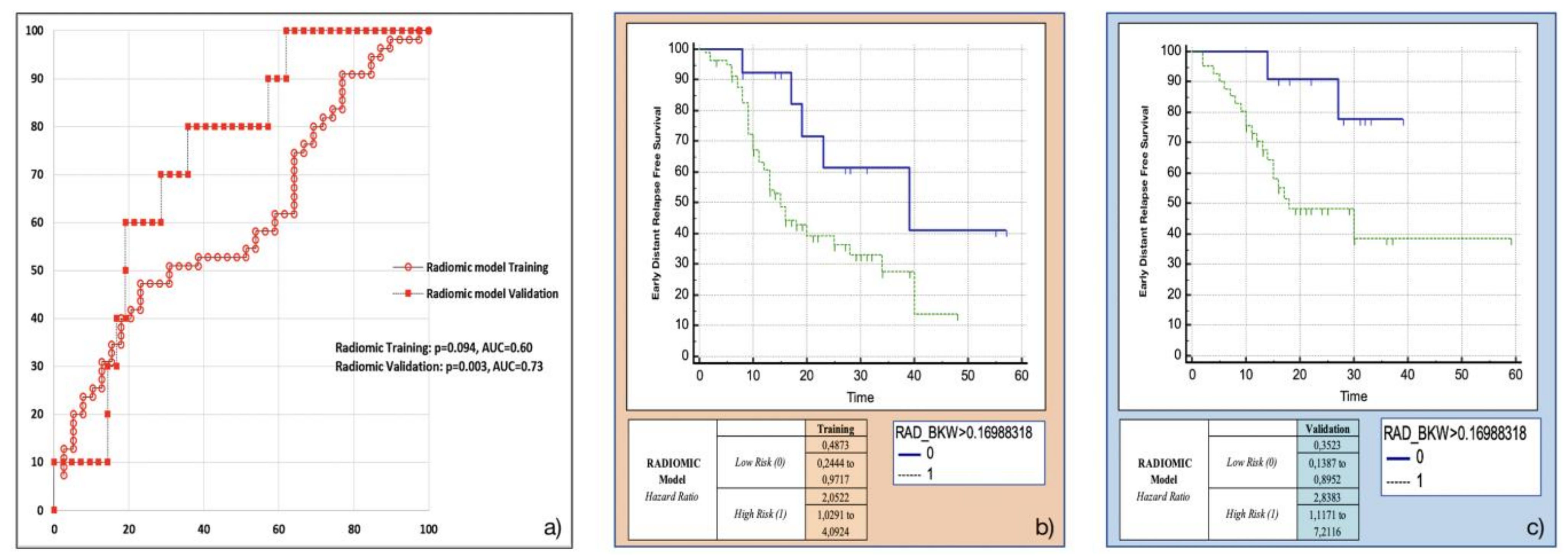
3.3. Training and Validation of the Radiomic Model
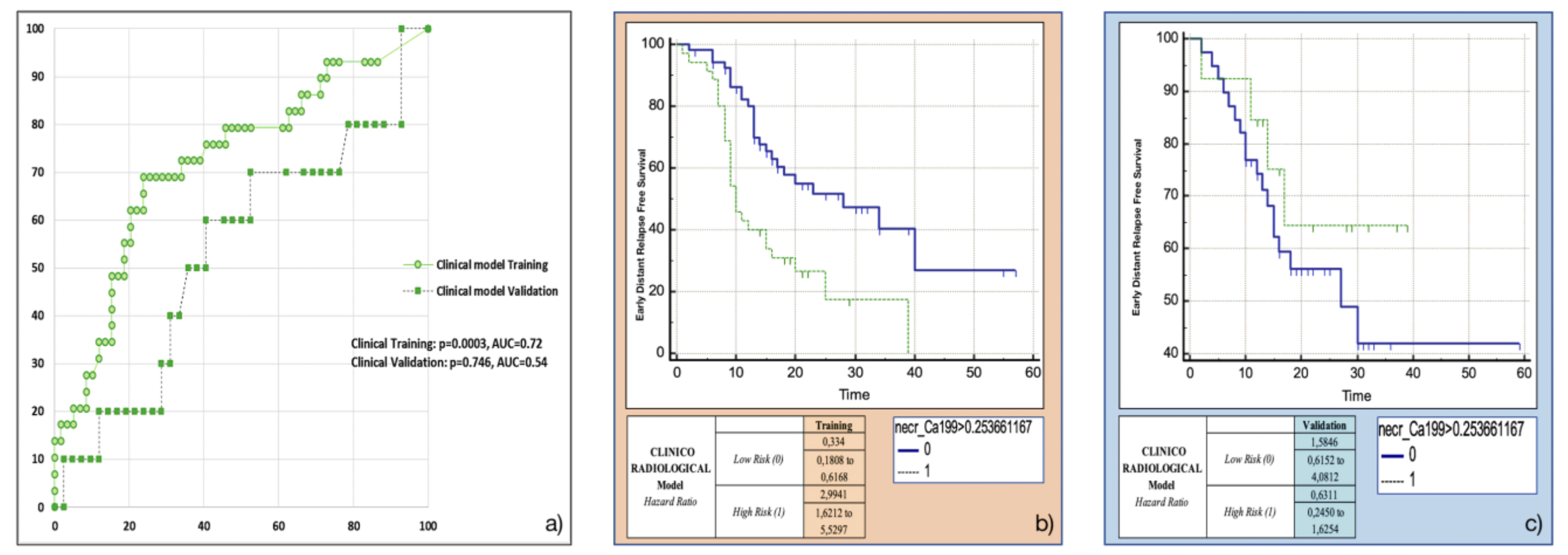
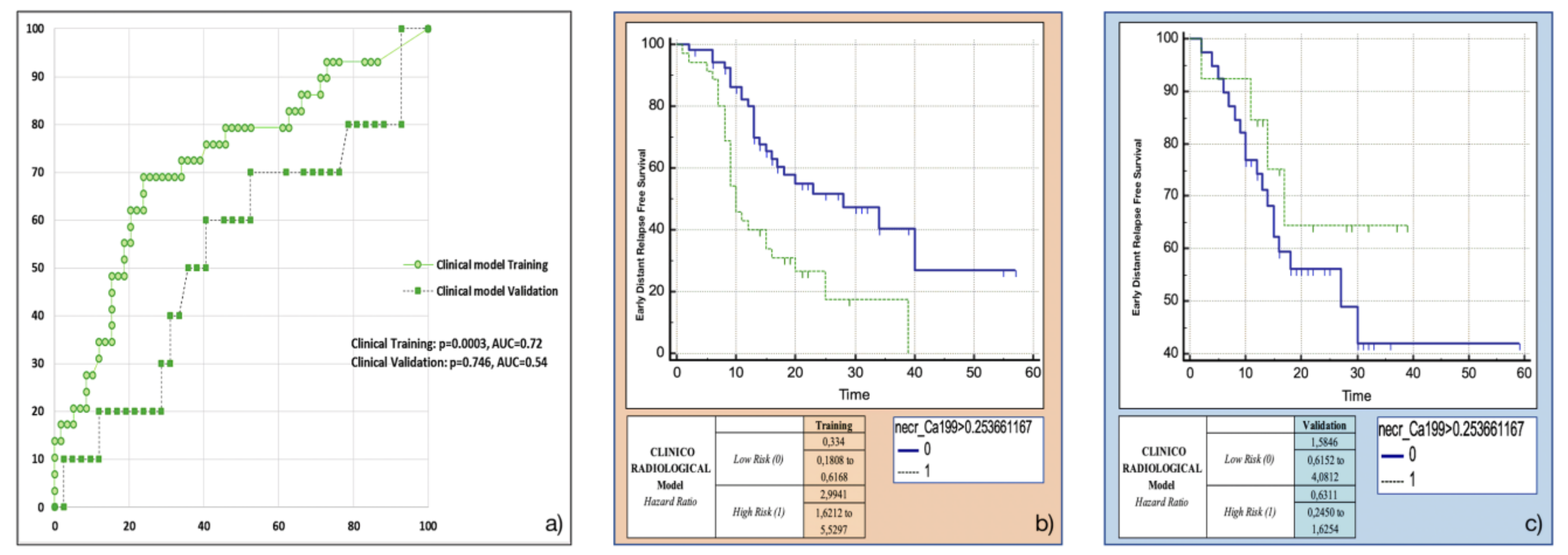
3.4. Training and Validation of the Clinicoradiological Model
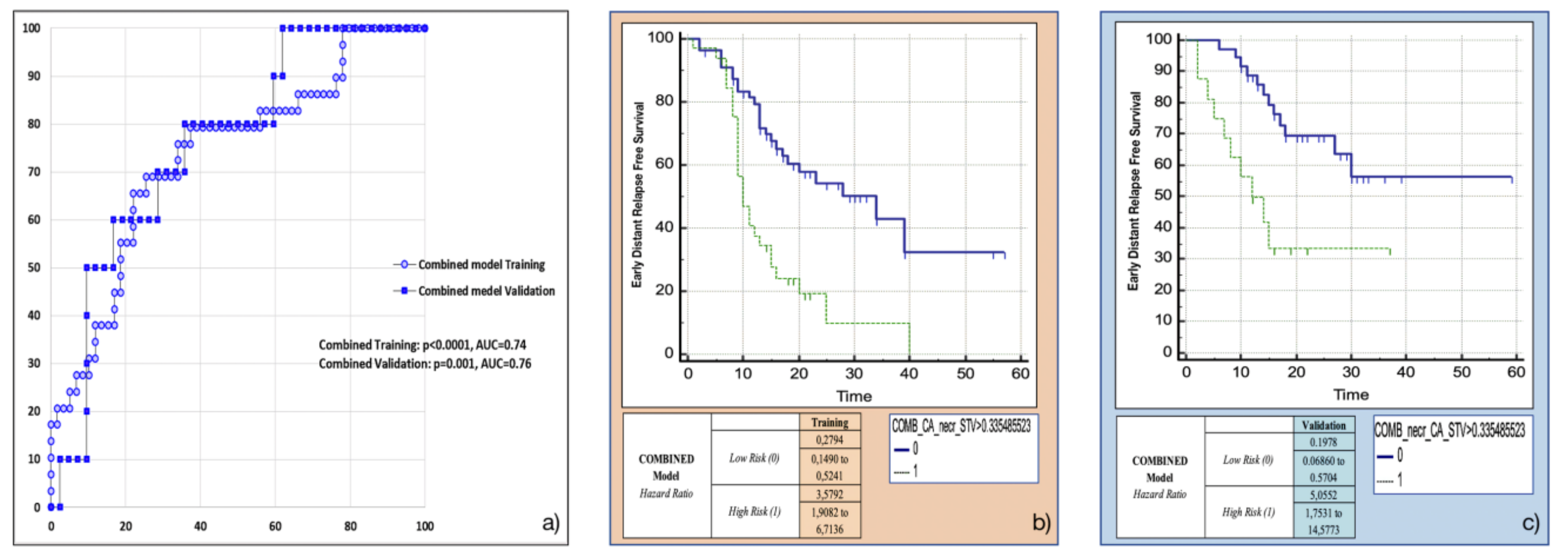
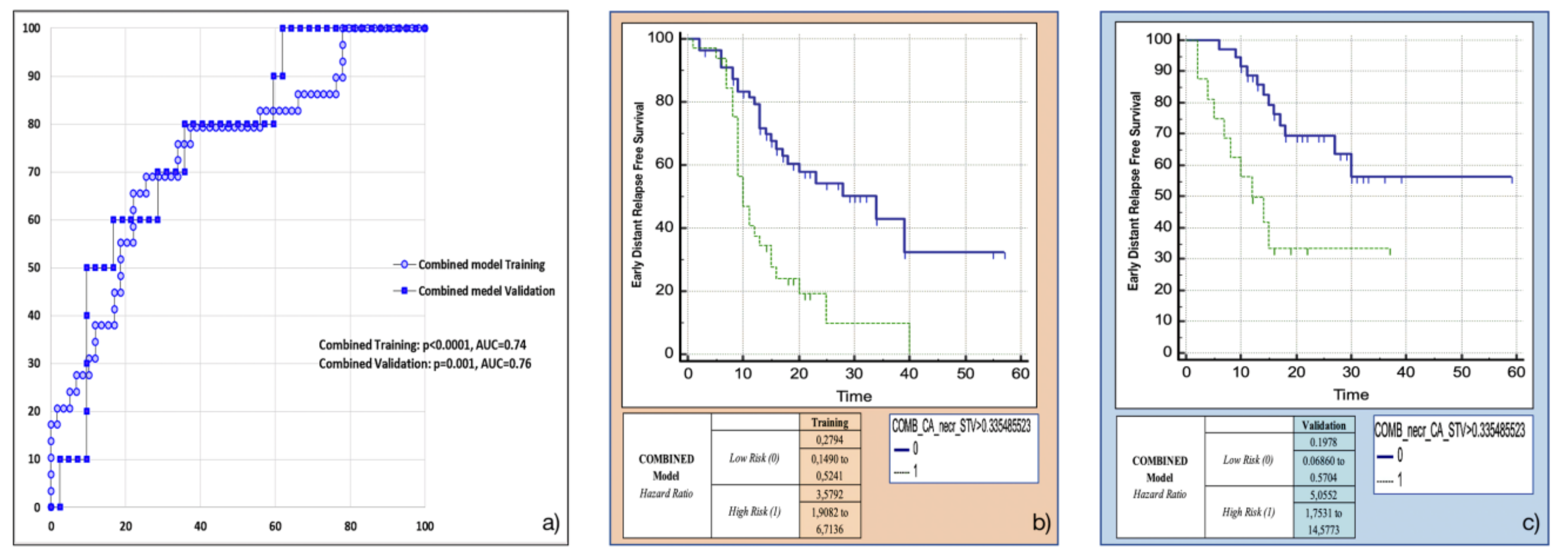
3.5. Training and Validation of the Combined Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zins, M.; Matos, C.; Cassinotto, C. Pancreatic Adenocarcinoma Staging in the Era of Preoperative Chemotherapy and Radiation Therapy. Radiology 2018, 287, 374–390. [Google Scholar] [CrossRef] [Green Version]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Pancreatic Adenocarcinoma; Version 1.2019; National Comprehensive Cancer Network: Fort Washington, PA, USA, 2019. [Google Scholar]
- Petrelli, F.; Inno, A.; Barni, S.; Ghidini, A.; Labianca, R.; Falconi, M.; Reni, M.; Cascinu, S. Borderline resectable pancreatic cancer: More than an anatomical concept. Dig. Liver Dis. 2017, 49, 223–226. [Google Scholar] [CrossRef]
- Matsumoto, I.; Murakami, Y.; Shinzeki, M.; Shinzeki, M.; Asari, S.; Goto, T.; Tani, M.; Motoi, F.; Uemura, K.; Sho, M.; et al. Proposed preoperative risk factors for early recurrence in patients with resectable pancreatic ductal adenocarcinoma after surgical resection: A multi-center retrospective study. Pancreatology 2015, 15, 674–680. [Google Scholar] [CrossRef]
- Lee, Y.S.; Lee, J.C.; Yang, S.Y.; Kim, J.; Hwang, J.H. Neoadjuvant therapy versus upfront surgery in resectable pancreatic cancer according to intention-to-treat and per-protocol analysis: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 15662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barugola, G.; Partelli, S.; Marcucci, S.; Sartori, N.; Capelli, P.; Bassi, C.; Pederzoli, P.; Falconi, M. Resectable pancreatic cancer: Who really benefits from resection? Ann. Surg. Oncol. 2009, 16, 3316–3322. [Google Scholar] [CrossRef]
- Bergquist, J.R.; Puig, C.A.; Shubert, C.R.; Groeschl, R.T.; Habermann, E.B.; Kendrick, M.L.; Nagorney, D.M.; Smoot, R.L.; Farnell, M.B.; Truty, M.J. Carbohydrate Antigen 19-9 Elevation in Anatomically Resectable, Early Stage Pancreatic Cancer Is Independently Associated with Decreased Overall Survival and an Indication for Neoadjuvant Therapy: A National Cancer Database Study. JACS 2016, 223, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Asano, T.; Okamura, K.; Tsuchikawa, T.; Murakami, S.; Kurashima, Y.; Ebihara, Y.; Noji, T.; Nakanishi, Y.; Tanaka, K.A. A Preoperative Prognostic Scoring System to Predict Prognosis for Resectable Pancreatic Cancer: Who Will Benefit from Upfront Surgery? J. Gastrointest. Surg. 2019, 23, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Groot, V.P.; Rezaee, N.; Wu, W.; Cameron, J.L.; Fishman, E.K.; Hruban, R.H.; Weiss, M.J.; Zheng, L.; Wolfgang, C.L.; He, J. Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2018, 267, 936–945. [Google Scholar] [CrossRef]
- Barugola, G.; Frulloni, L.; Salvia, R.; Falconi, M. Is CA 19-9 a screening marker? Dig. Liver Dis. 2009, 41, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Ballehaninna, U.K.; Chamberlain, R.S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 2012, 3, 105–119. [Google Scholar] [CrossRef]
- Crippa, S.; Pergolini, I.; Javed, A.A.; Honselmann, K.C.; Weiss, M.J.; Di Salvo, F.; Burkhart, R.; Zamboni, G.; Belfiori, G.; Ferrone, C.R. Implications of Perineural Invasion on Disease Recurrence and Survival After Pancreatectomy for Pancreatic Head Ductal Adenocarcinoma. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.; van Timmeren, J.; Sanduleanu, S.; Larue, R.; Even, A.; Jochems, A. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Abunahel, B.M.; Pontre, B.; Kumar, H.; Petrov, M.S. Pancreas image mining: A systematic review of radiomics. Eur. Radiol. 2021, 31, 3447–3467. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Loi, S.; Mori, M.; Benedetti, G.; Partelli, S.; Broggi, S.; Cattaneo, G.M.; Palumbo, D.; Muffatti, F.; Falconi, M.; De Cobelli, F. Robustness of CT radiomic features against image discretization and interpolation in characterizing pancreatic neuroendocrine neoplasms. Phys. Med. 2020, 76, 125–133. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, M.; De Robertis, R.; Aluffi, G.; Cadore, C.; Beleù, A.; Cardobi, N.; Malleo, G.; Manfrin, E.; Bassi, C. CT Simplified Radiomic Approach to Assess the Metastatic Ductal Adenocarcinoma of the Pancreas. Cancers (Basel) 2021, 13, 1843. [Google Scholar] [CrossRef]
- Mori, M.; Passoni, P.; Incerti, E.; Bettinardi, V.; Broggi, S.; Reni, M.; Whybra, P.; Spezi, E.; Vanoli, E.G.; Gianolli, L. Training and validation of a robust PET radiomic-based index to predict distant-relapse-free-survival after radio-chemotherapy for locally advanced pancreatic cancer. Radiother. Oncol. 2020, 153, 258–264. [Google Scholar] [CrossRef]
- Van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging-"how-to" guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef]
- Vallières, M.; Zwanenburg, A.; Badic, B.; Cheze Le Rest, C.; Visvikis, D.; Hatt, M. Responsible Radiomics Research for Faster Clinical Translation. J. Nucl. Med. 2018, 59, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Kim, H.J.; Kim, K.W.; An, S.; Hong, S.M.; Kim, S.C.; Kim, M.H. DPC4 gene expression in primary pancreatic ductal adenocarcinoma: Relationship with CT characteristics. Br. J. Radiol. 2017, 90, 20160403. [Google Scholar] [CrossRef] [Green Version]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groot, V.P.; Gemenetzis, G.; Blair, A.B.; Rivero-Soto, R.J.; Yu, J.; Javed, A.A.; Burkhart, R.A.; Rinkes, I.; Molenaar, I.Q.; Cameron, J.L. Defining and Predicting Early Recurrence in 957 Patients With Resected Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2019, 269, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Ikoma, H.; Morimura, R.; Konishi, H.; Murayama, Y.; Komatsu, S.; Shiozaki, A.; Kuriu, Y.; Kubota, T.; Nakanishi, M. Optimal duration of the early and late recurrence of pancreatic cancer after pancreatectomy based on the difference in the prognosis. Pancreatology 2014, 14, 524–529. [Google Scholar] [CrossRef]
- Braga, M.; Pecorelli, N.; Ariotti, R.; Capretti, G.; Greco, M.; Balzano, G.; Castoldi, R.; Beretta, L. Enhanced recovery after surgery pathway in patients undergoing pancreaticoduodenectomy. World J. Surg. 2014, 38, 2960–2966. [Google Scholar] [CrossRef]
- Crippa, S.; Belfiori, G.; Tamburrino, D.; Partelli, S.; Falconi, M. Indications to total pancreatectomy for positive neck margin after partial pancreatectomy: A review of a slippery ground. Updates Surg. 2021, 73, 1219–1229. [Google Scholar] [CrossRef] [PubMed]
- Van Roessel, S.; Kasumova, G.G.; Verheij, J.; Najarian, R.M.; Maggino, L.; de Pastena, M.; Malleo, G.; Marchegiani, G.; Salvia, R.; Ng, S.C. International Validation of the Eighth Edition of the American Joint Committee on Cancer (AJCC) TNM Staging System in Patients with Resected Pancreatic Cancer. JAMA Surg. 2018, 153, e183617. [Google Scholar] [CrossRef]
- Palumbo, D.; Tamburrino, D.; Partelli, S.; Gusmini, S.; Guazzarotti, G.; Cao, R.; Crippa, S.; Falconi, M.; De Cobelli, F. Before sentinel bleeding: Early prediction of postpancreatectomy hemorrhage (PPH) with a CT-based scoring system. Eur. Radiol. 2021, 31, 6879–6888. [Google Scholar] [CrossRef] [PubMed]
- Al-Hawary, M.M.; Francis, I.R.; Chari, S.T.; Fishman, E.K.; Hough, D.M.; Lu, D.S.; Macari, M.; Megibow, A.J.; Miller, F.H.; Mortele, K.J. Pancreatic ductal adenocarcinoma radiology reporting template: Consensus statement of the society of abdominal radiology and the american pancreatic association. Gastroenterology 2014, 146, 291–304.e1. [Google Scholar] [CrossRef]
- Benedetti, G.; Mori, M.; Panzeri, M.M.; Barbera, M.; Palumbo, D.; Sini, C.; Muffatti, F.; Andreasi, V.; Steidler, S.; Doglioni, C.; et al. CT-derived radiomic features to discriminate histologic characteristics of pancreatic neuroendocrine tumors. Radiol. Med. 2021, 126, 745–760. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Mori, M.; Benedetti, G.; Partelli, S.; Sini, C.; Andreasi, V.; Broggi, S.; Barbera, M.; Cattaneo, G.M.; Muffatti, F.; Panzeri, M. Ct radiomic features of pancreatic neuroendocrine neoplasms (panNEN) are robust against delineation uncertainty. Phys. Med. 2019, 57, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Reni, M.; Balzano, G.; Zanon, S.; Zerbi, A.; Rimassa, L.; Castoldi, R.; Pinelli, D.; Mosconi, S.; Doglioni, C.; Chiaravalli, M. Safety and efficacy of preoperative or postoperative chemotherapy for resectable pancreatic adenocarcinoma (PACT-15): A randomised, open-label, phase 2-3 trial. Lancet Gastroenterol. Hepatol. 2018, 3, 413–423. [Google Scholar] [CrossRef]
- Paniccia, A.; Hosokawa, P.; Henderson, W.; Schulick, R.D.; Edil, B.H.; McCarter, M.D.; Gajdos, C. Characteristics of 10-Year Survivors of Pancreatic Ductal Adenocarcinoma. JAMA Surg. 2015, 150, 701–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudo, M.; Kobayashi, T.; Gotohda, N.; Konishi, M.; Takahashi, S.; Kobayashi, S.; Sugimoto, M.; Okubo, S.; Martin, J.; Cabral, H. Clinical Utility of Histological and Radiological Evaluations of Tumor Necrosis for Predicting Prognosis in Pancreatic Cancer. Pancreas 2020, 49, 634–641. [Google Scholar] [CrossRef]
- Brennan, M.F.; Kattan, M.W.; Klimstra, D.; Conlon, K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann. Surg. 2004, 240, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Adamu, M.; Nitschke, P.; Petrov, P.; Rentsch, A.; Distler, M.; Reissfelder, C.; Welsch, T.; Saeger, H.D.; Weitz, J.; Rahbari, N.N. Validation of prognostic risk scores for patients undergoing resection for pancreatic cancer. Pancreatology 2018, 18, 585–591. [Google Scholar] [CrossRef]
- Strijker, M.; Chen, J.W.; Mungroop, T.H.; Jamieson, N.B.; van Eijck, C.H.; Steyerberg, E.W.; Wilmink, J.W.; Groot Koerkamp, B.; van Laarhoven, H.W.; Besselink, M.G. Systematic review of clinical prediction models for survival after surgery for resectable pancreatic cancer. Br. J. Surg. 2019, 106, 342–354. [Google Scholar] [CrossRef]
- Kim, D.W.; Lee, S.S.; Kim, S.O.; Kim, J.H.; Kim, H.J.; Byun, J.H.; Yoo, C.; Kim, K.P.; Song, K.B.; Kim, S.C. Estimating Recurrence after Upfront Surgery in Patients with Resectable Pancreatic Ductal Adenocarcinoma by Using Pancreatic CT: Development and Validation of a Risk Score. Radiology 2020, 296, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Eilaghi, A.; Baig, S.; Zhang, Y.; Zhang, J.; Karanicolas, P.; Gallinger, S.; Khalvati, F.; Haider, M.A. CT texture features are associated with overall survival in pancreatic ductal adenocarcinoma—A quantitative analysis. BMC Med. Imaging 2017, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Kim, H.J.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Shin, J.H. Can preoperative CA19-9 and CEA levels predict the resectability of patients with pancreatic adenocarcinoma? J. Gastroenterol. Hepatol. 2009, 24, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.R.; Finkelstein, D.M.; Thayer, S.P.; Muzikansky, A.; Fernandez del Castillo, C.; Warshaw, A.L. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J. Clin. Oncol. 2006, 24, 2897–2902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiura, T.; Uesaka, K.; Kanemoto, H.; Mizuno, T.; Sasaki, K.; Furukawa, H.; Matsunaga, K.; Maeda, A. Serum CA19-9 is a significant predictor among preoperative parameters for early recurrence after resection of pancreatic adenocarcinoma. J. Gastrointest. Surg. 2012, 16, 977–985. [Google Scholar] [CrossRef]
- Limkin, E.J.; Reuzé, S.; Carré, A.; Sun, R.; Schernberg, A.; Alexis, A.; Deutsch, E.; Ferté, C.; Robert, C. The complexity of tumor shape, spiculatedness, correlates with tumor radiomic shape features. Sci. Rep. 2019, 9, 4329. [Google Scholar] [CrossRef] [Green Version]
- Bribiesca, E. Measure of compactness for 3D shapes. Comput. Math. Appl. 2000, 40, 1275–1284. [Google Scholar] [CrossRef] [Green Version]
- Harris, L.K.; Theriot, J.A. Surface Area to Volume Ratio: A Natural Variable for Bacterial Morphogenesis. Trends Microbiol. 2018, 26, 815–832. [Google Scholar] [CrossRef] [Green Version]
- Xie, T.; Wang, X.; Li, M.; Tong, T.; Yu, X.; Zhou, Z. Pancreatic ductal adenocarcinoma: A radiomics nomogram outperforms clinical model and TNM staging for survival estimation after curative resection. Eur. Radiol. 2020, 30, 2513–2524. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 147) | Training (n = 94) | Validation (n = 53) | p-Value | ||
|---|---|---|---|---|---|
| Clinical Variables | Age at diagnosis (year) * | 69.94 (44–88) | 70.06 (43–87) | 69.73 (43–88) | 0.84 |
| Sex | 0.13 | ||||
| Female | 61 (41.6%) | 35 (37.6%) | 27 (50.5%) | ||
| Male | 86 (58.4%) | 59 (63.4%) | 26 (49.5%) | ||
| Ca 19.9 (U/mL) * | 40 (14–150) | 48.5 (13.25–191) | 35 (14.5–77.5) | 0.21 | |
| Adjuvant Treatment | 111 (75%) | 69 (73.2%) | 42 (78.6%) | 0.38 | |
| Adjuvant Chemoterapy | 107 (73.0%) | 68 (73.0%) | 39 (73.2%) | 0.45 | |
| Adjuvant Radioteraphy | 31 (21%) | 21 (22.3%) | 10 (19.6%) | 0.11 | |
| Pathological Data | Tumor Size (mm) ^ | 27.33 (+/− 0.78) | 28.36 (+/− 0.97) | 25.48 (+/− 1.29) | 0.78 |
| Final R status | 0.08 | ||||
| R1 | 65 (44.2%) | 44 (46.8%) | 21 (39.6%) | ||
| R0 | 82 (55.8%) | 50 (53.2%) | 32 (60.4%) | ||
| Lymph-vascular Invasion | 129 (87.8%) | 88 (93.6%) | 41 (76.8%) | 0.015 | |
| Perineural Invasion | 130 (87.1%) | 86 (91.4%) | 44 (82.1%) | 0.06 | |
| Peripancreatic Fat Invasion | 135 (91%) | 92 (97.8%) | 43 (80.3%) | 0.72 | |
| Grading | 0.42 | ||||
| G1 | 3 (2.0%) | 3 (3.1%) | 0 (0%) | ||
| G2 | 66 (45.0%) | 45 (47.8%) | 26 (48.2%) | ||
| G3 | 78 (53.0%) | 46 (49.1%) | 27 (51.8%) | ||
| TNM | |||||
| T | 0.75 | ||||
| T1 | 34 (22.7%) | 20 (20.3%) | 14 (26.8%) | ||
| T2 | 102 (69.2%) | 68 (72.3%) | 34 (64.3%) | ||
| T3 | 11 (7.7%) | 7 (7.4%) | 5 (8.9%) | ||
| N | 0.065 | ||||
| N0 | 23 (16.1%) | 15 (15.0%) | 9 (17.8%) | ||
| N1 | 50 (33.9%) | 26 (27.6%) | 24 (44.6%) | ||
| N2 | 74 (50%) | 54 (57.4%) | 20 (37.5%) | ||
| Lymphnode Ratio * | 0.136 (0.04–0.25) | 0.16 (0.06–0.26) | 0.10 (0.03–0.2) | 0.11 | |
| Radiological Data | Dimension (mm) ^ | 24.5 (+/− 7.2) | 25.79 (+/− 6.8) | 23.23 (+/− 7.8) | 0.07 |
| Necrosis | 0.34 | ||||
| Present | 27 (18.2%) | 18 (19.1%) | 9 (16.9%) | ||
| Absent | 120 (81.6%) | 76 (85.2%) | 44 (83.0%) | ||
| Hypodense on pancreatic phase | 116 (74.4%) | 77 (81.9%) | 39 (73.5%) | 0.48 | |
| Hypodense on venous phase | 93 (57.1%) | 91 (96.8%) | 2 (3.5%) | 0.50 | |
| Isodense on pancreatic phase | 23 (21.8%) | 21 (23.4%) | 2 (3.5%) | 0.58 | |
| Outcome Variables | Early distant recurrence (EDR) | 0.54 | |||
| EDR | 39 (25.6%) | 25 (26.5%) | 14 (26.3%) | ||
| non-EDR | 108 (74.4%) | 69 (73.5%) | 39 (73.7%) | ||
| Time to recurrence (months) * | 15 (10–22) | 15 (9–22) | 16 (11–26) | 0.55 | |
| Overall survival (months) * | 20 (15–28) | 20 (15–28) | 20 (16–28.5) | 0.98 | |
| Length of follow-up (months) * | 19 (14–27) | 19 (14–27) | 19.5 (13.25–27.75) | 0.94 |
| Radomic Model | Coefficient | p-value | OR | 95%CI | Overall Fit Model | AUC | 95%CI | Sensivity | Specifity | PPP | NPP | ||||||||
| Surface To Volume Ratio | −3.82224 | 0.0183 | 0.0219 | 0.0009 to 0.5237 | 0.0097 | 0.0244 | 0.599 | 0.733 | 0.493 to 0.699 | 0.593 to 0.846 | 90.9 | 100.0 | 23.08 | 26.2 | 62.5 | 24.4 | 64.3 | 100.0 | |
| Clinico Radiological Model | Coefficient | p-value | OR | 95%CI | Overall Fit Model | AUC | 95%CI | Sensivity | Specifity | PPP | NPP | ||||||||
| Ca19.9 | 0.001128 | 0.049 | 1.0011 | 1.0000 to 1.0023 | 0.0018 | 0.9529 | 0.72 | 0.536 | 0.614 to 0.811 | 0.392 to 0.675 | 68.9 | 20.0 | 76.27 | 73.8 | 58.8 | 15.4 | 83.3 | 79.5 | |
| Necrosis | 1.10839 | 0.0633 | 3.0295 | 0.9402 to 9.7611 | |||||||||||||||
| Combined Model | Coefficient | p-value | OR | 95%CI | Overall Fit Model | AUC | 95%CI | Sensivity | Specifity | PPP | NPP | ||||||||
| Ca19.9 | 0.000964 | 0.0946 | 1.011 | 0.9998 to 1.0021 | 0.0015 | 0.0178 | 0.736 | 0.76 | 0.648 to 0.838 | 0.618 to 0.865 | 58.6 | 60.0 | 86.44 | 78.5 | 68.0 | 40.0 | 81.0 | 89.2 | |
| Necrosis | 0.86465 | 0.1594 | 2.3742 | 0.7120 to 7.9167 | |||||||||||||||
| Surface To Volume Ratio | −2.8972 | 0.1171 | 0.0552 | 0.0015 to 2.0684 | |||||||||||||||
| Training | |||||||||||||||||||
| Validation | |||||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palumbo, D.; Mori, M.; Prato, F.; Crippa, S.; Belfiori, G.; Reni, M.; Mushtaq, J.; Aleotti, F.; Guazzarotti, G.; Cao, R.; et al. Prediction of Early Distant Recurrence in Upfront Resectable Pancreatic Adenocarcinoma: A Multidisciplinary, Machine Learning-Based Approach. Cancers 2021, 13, 4938. https://doi.org/10.3390/cancers13194938
Palumbo D, Mori M, Prato F, Crippa S, Belfiori G, Reni M, Mushtaq J, Aleotti F, Guazzarotti G, Cao R, et al. Prediction of Early Distant Recurrence in Upfront Resectable Pancreatic Adenocarcinoma: A Multidisciplinary, Machine Learning-Based Approach. Cancers. 2021; 13(19):4938. https://doi.org/10.3390/cancers13194938
Chicago/Turabian StylePalumbo, Diego, Martina Mori, Francesco Prato, Stefano Crippa, Giulio Belfiori, Michele Reni, Junaid Mushtaq, Francesca Aleotti, Giorgia Guazzarotti, Roberta Cao, and et al. 2021. "Prediction of Early Distant Recurrence in Upfront Resectable Pancreatic Adenocarcinoma: A Multidisciplinary, Machine Learning-Based Approach" Cancers 13, no. 19: 4938. https://doi.org/10.3390/cancers13194938
APA StylePalumbo, D., Mori, M., Prato, F., Crippa, S., Belfiori, G., Reni, M., Mushtaq, J., Aleotti, F., Guazzarotti, G., Cao, R., Steidler, S., Tamburrino, D., Spezi, E., Del Vecchio, A., Cascinu, S., Falconi, M., Fiorino, C., & De Cobelli, F. (2021). Prediction of Early Distant Recurrence in Upfront Resectable Pancreatic Adenocarcinoma: A Multidisciplinary, Machine Learning-Based Approach. Cancers, 13(19), 4938. https://doi.org/10.3390/cancers13194938