
Phase I/II Study of LDE225 in Combination with Gemcitabine and Nab-Paclitaxel in Patients with Metastatic Pancreatic Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Population
2.2. Study Design and Treatment
2.3. Toxicity Assessment
2.4. Tumor Response Evaluation
2.5. Statistical Analysis
3. Results
3.1. Phase I
3.1.1. Characterization of the Study Cohort
3.1.2. MTD and DLT
3.2. Phase II
3.2.1. Characterization of the Study Cohort
3.2.2. Safety
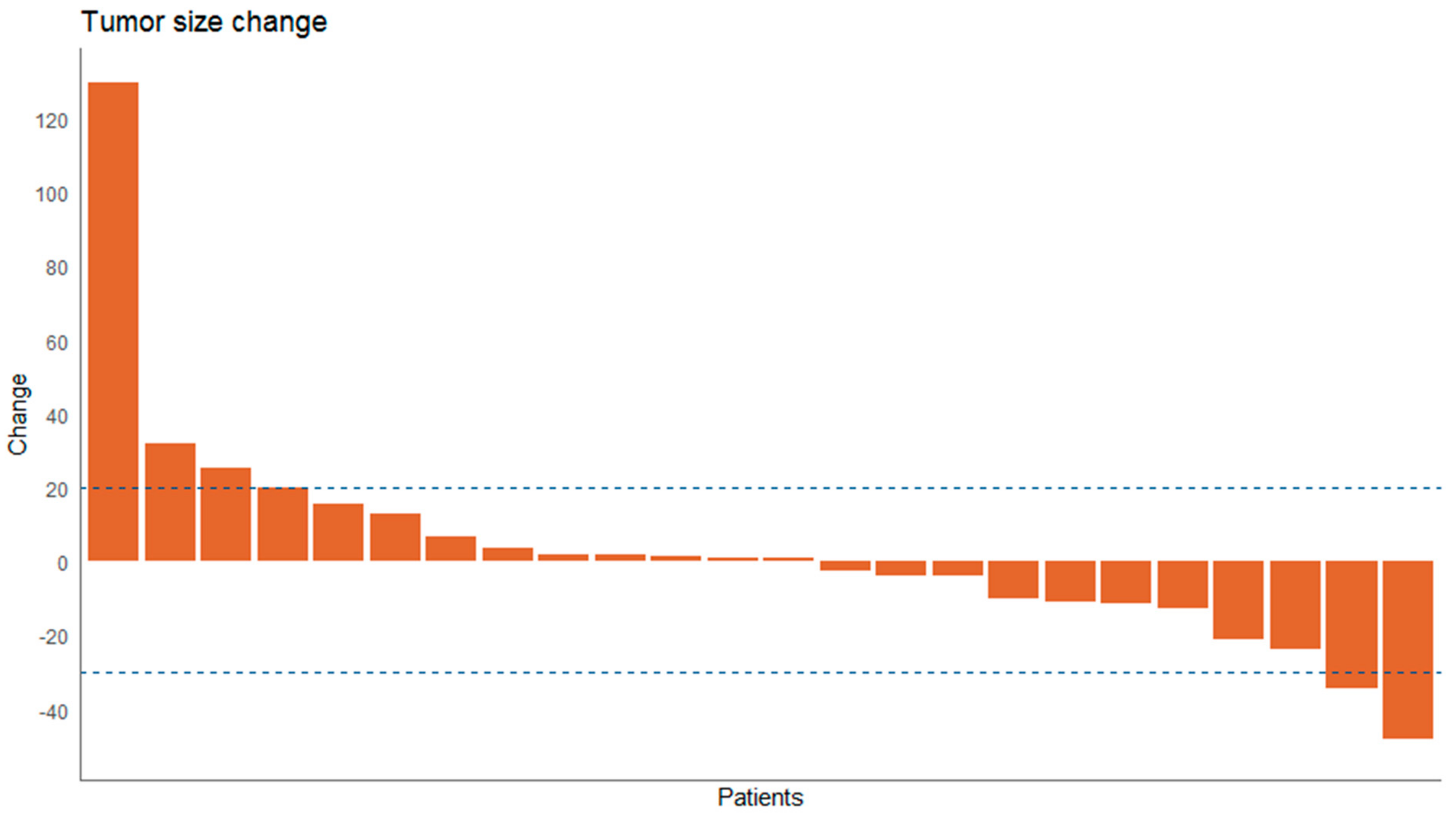
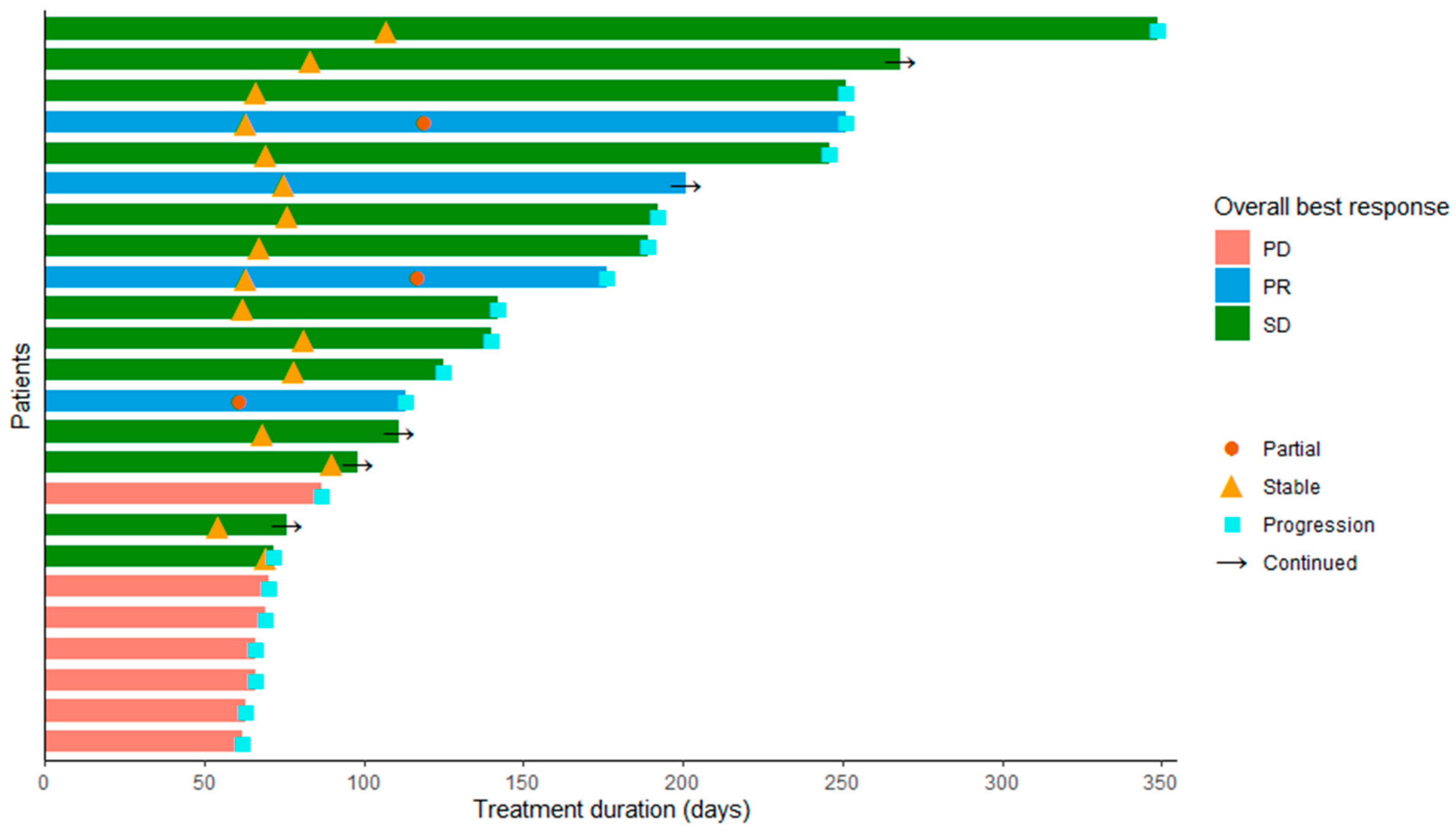
3.2.3. Tumor Response
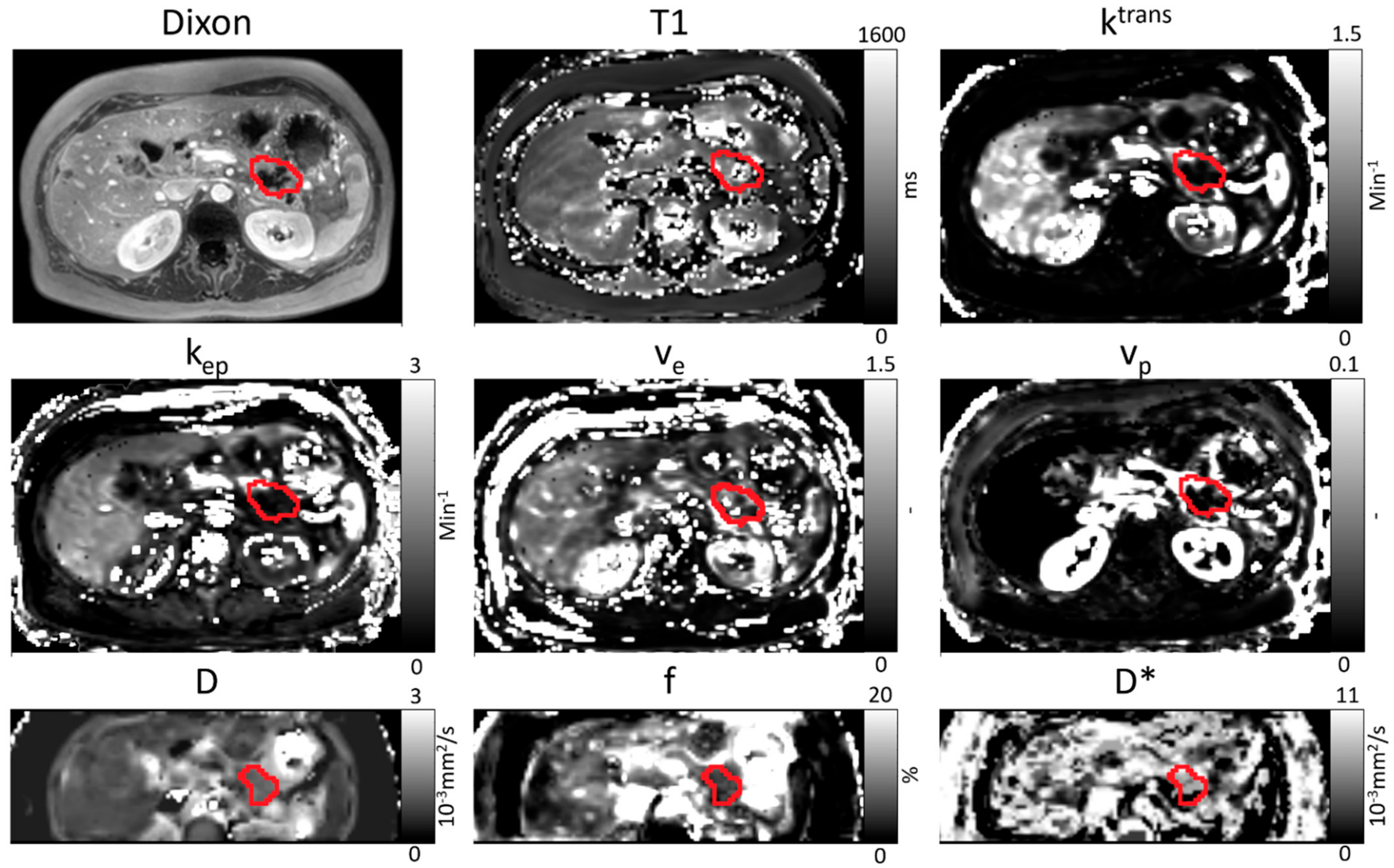
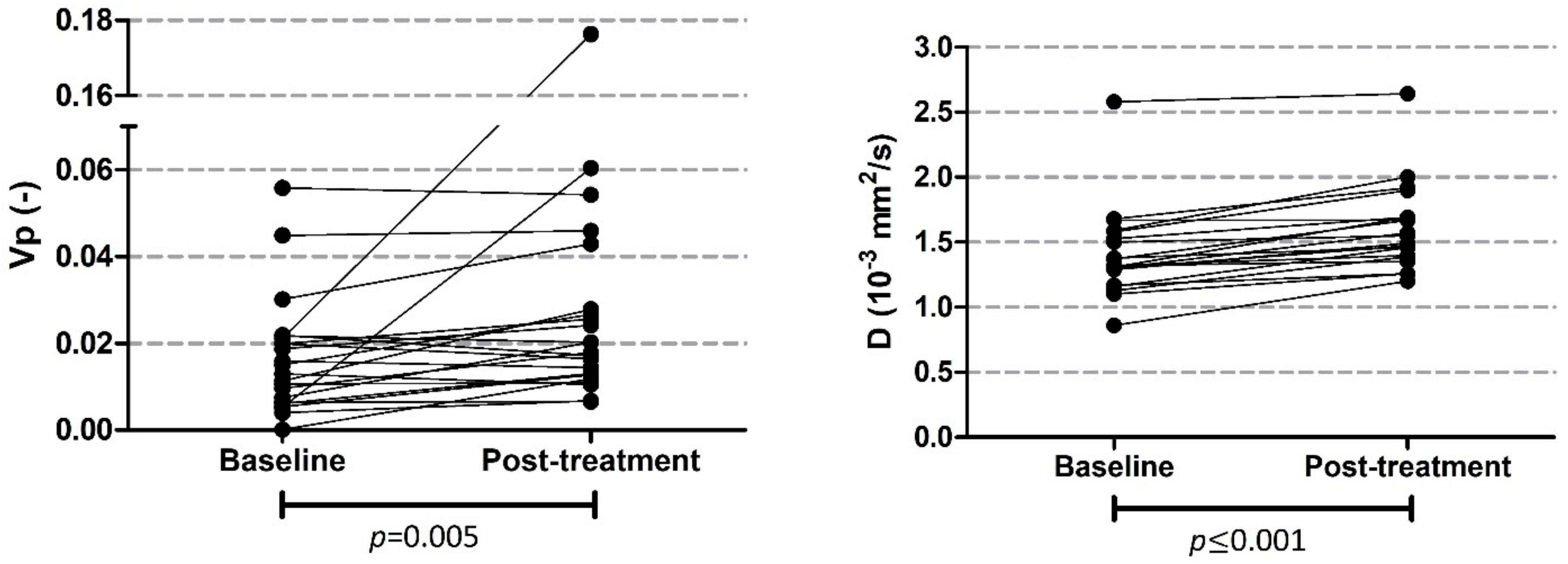
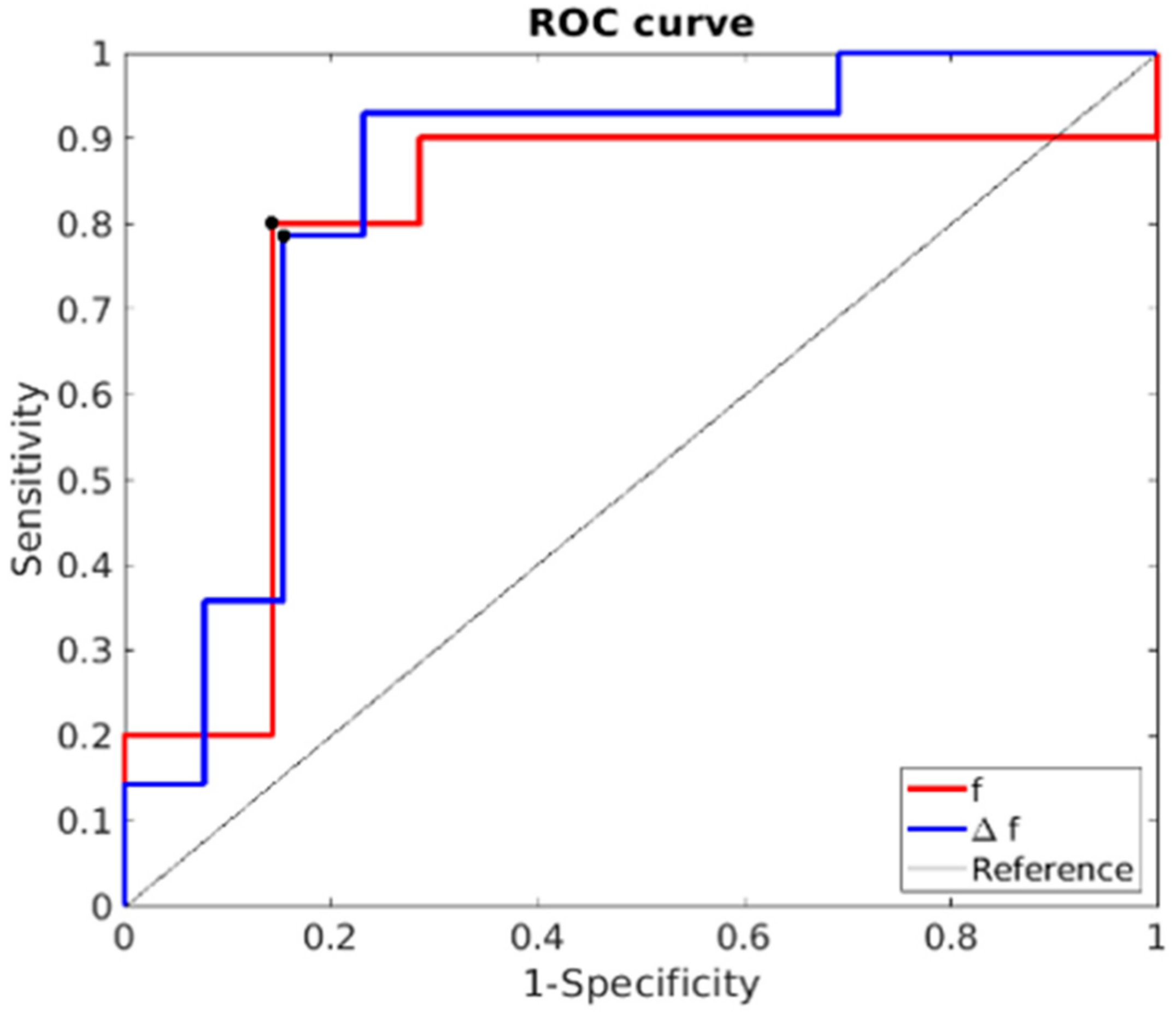
3.2.4. MRI Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-W.; Ma, Y.-X.; Sun, Y.; Cao, Y.-B.; Li, Q.; Xu, C.-A. Gemcitabine in combination with a second cytotoxic agent in the first-line treatment of locally advanced or metastatic pancreatic cancer: A systematic review and meta-analysis. Target. Oncol. 2017, 12, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Lambert, A.; Gavoille, C.; Conroy, T. Current status on the place of FOLFIRINOX in metastatic pancreatic cancer and future directions. Thrapeutic Adv. Gastroenterol. 2017, 10, 631–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; De La Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, A.H. FOLFIRINOX: A small step or a great leap forward? J. Clin. Oncol. 2011, 29, 3727–3729. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ramanathan, R.K.; Borad, M.J.; Laheru, D.A.; Smith, L.S.; Wood, T.E.; Korn, R.L.; Desai, N.; Trieu, V.; Iglesias, J.L.; et al. Gemcitabine plus nab-paclitaxel is an active regimen in patients with advanced pancreatic cancer: A phase I/II trial. J. Clin. Oncol. 2011, 29, 4548–4554. [Google Scholar] [CrossRef] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [Green Version]
- Latenstein, A.E.J.; Mackay, T.M.; Creemers, G.-J.; Van Eijck, C.H.J.; De Groot, J.W.B.; Mohammad, N.H.; Homs, M.Y.V.; Van Laarhoven, H.W.M.; Molenaar, I.Q.; Tije, B.-J.T.; et al. Implementation of contemporary chemotherapy for patients with metastatic pancreatic ductal adenocarcinoma: A population-based analysis. Acta Oncol. 2020, 59, 705–712. [Google Scholar] [CrossRef] [Green Version]
- Chin, V.; Nagrial, A.; Sjoquist, K.; O’Connor, A.C.; Chantrill, L.; Biankin, A.V.; Scholten, R.J.; Yip, D. Chemotherapy and radiotherapy for advanced pancreatic cancer. Cochrane Database Syst. Rev. 2018, 3, CD011044. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, M. Pancreatic cancer. N. Engl. J. Med. 2010, 362, 1605–1617. [Google Scholar] [CrossRef] [Green Version]
- Mahadevan, D.; Von Hoff, D.D. Tumor-stroma interactions in pancreatic ductal adenocarcinoma. Mol. Cancer Ther. 2007, 6, 1186–1197. [Google Scholar] [CrossRef] [Green Version]
- Erkan, M.; Reiser-Erkan, C.; Michalski, C.W.; Kong, B.; Esposito, I.; Friess, H.; Kleeff, J. The impact of the activated stroma on pancreatic ductal adenocarcinoma biology and therapy resistance. Curr. Mol. Med. 2012, 12, 288–303. [Google Scholar] [CrossRef]
- Jaster, R. Molecular regulation of pancreatic stellate cell function. Mol. Cancer 2004, 3, 26. [Google Scholar] [CrossRef] [Green Version]
- Bijlsma, M.F.; van Laarhoven, H.W. The conflicting roles of tumor stroma in pancreatic cancer and their contribution to the failure of clinical trials: A systematic review and critical appraisal. Cancer Metastasis Rev. 2015, 34, 97–114. [Google Scholar] [CrossRef]
- Hidalgo, M.; Maitra, A. The hedgehog pathway and pancreatic cancer. N. Engl. J. Med. 2009, 361, 2094–2096. [Google Scholar] [CrossRef] [PubMed]
- Hermann, P.C.; Huber, S.L.; Heeschen, C. Metastatic cancer stem cells: A new target for anti-cancer therapy? Cell Cycle 2008, 7, 188–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermann, P.C.; Huber, S.L.; Herrler, T.; Aicher, A.; Ellwart, J.W.; Guba, M.; Bruns, C.J.; Heeschen, C. Distinct populations of cancer stem cells determine tumor growth and metastatic activity in human pancreatic cancer. Cell Stem Cell 2007, 1, 313–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Heidt, D.G.; Dalerba, P.; Burant, C.F.; Zhang, L.; Adsay, V.; Wicha, M.; Clarke, M.F.; Simeone, D.M. Identification of pancreatic cancer stem cells. Cancer Res. 2007, 67, 1030–1037. [Google Scholar] [CrossRef] [Green Version]
- Olive, K.P.; Jacobetz, M.A.; Davidson, C.J.; Gopinathan, A.; McIntyre, D.; Honess, D.; Madhu, B.; Goldgraben, M.A.; Caldwell, M.E.; Allard, D.; et al. Inhibition of hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science 2009, 324, 1457–1461. [Google Scholar] [CrossRef] [Green Version]
- Kleeff, J.; Beckhove, P.; Esposito, I.; Herzig, S.; Huber, P.E.; Löhr, J.M.; Friess, H. Pancreatic cancer microenvironment. Int. J. Cancer 2007, 121, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Reni, M.; Cordio, S.; Milandri, C.; Passoni, P.; Bonetto, E.; Oliani, C.; Luppi, G.; Nicoletti, R.; Galli, L.; Bordonaro, R.; et al. Gemcitabine versus cisplatin, epirubicin, fluorouracil, and gemcitabine in advanced pancreatic cancer: A randomised controlled multicentre phase III trial. Lancet Oncol. 2005, 6, 369–376. [Google Scholar] [CrossRef]
- Ko, A.H.; LoConte, N.; Tempero, M.A.; Walker, E.J.; Kelley, R.K.; Lewis, S.; Chang, W.-C.; Kantoff, E.; Vannier, M.W.; Catenacci, D.V.; et al. A phase I study of FOLFIRINOX Plus IPI-926, a hedgehog pathway inhibitor, for advanced pancreatic adenocarcinoma. Pancreas 2016, 45, 370–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catenacci, D.V.T.; Junttila, M.R.; Karrison, T.; Bahary, N.; Horiba, M.N.; Nattam, S.R.; Marsh, R.; Wallace, J.; Kozloff, M.; Rajdev, L.; et al. Randomized Phase Ib/II study of gemcitabine Plus Placebo or Vismodegib, a hedgehog pathway inhibitor, in patients with metastatic pancreatic cancer. J. Clin. Oncol. 2015, 33, 4284–4292. [Google Scholar] [CrossRef] [PubMed]
- Heijmen, L.; Verstappen, M.C.; ter Voert, E.E.; Punt, C.J.; Oyen, W.J.; de Geus-Oei, L.-F.; Hermans, J.J.; Heerschap, A.; van Laarhoven, H.W. Tumour response prediction by diffusion-weighted MR imaging: Ready for clinical use? Crit. Rev. Oncol. 2012, 83, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.-M.; Collins, D. Diffusion-weighted MRI in the body: Applications and Challenges in oncology. Am. J. Roentgenol. 2007, 188, 1622–1635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klaassen, R.; Steins, A.; Gurney-Champion, O.J.; Bijlsma, M.F.; Van Tienhoven, G.; Engelbrecht, M.R.W.; Van Eijck, C.H.J.; Suker, M.; Wilmink, J.W.; Besselink, M.G.; et al. Pathological validation and prognostic potential of quantitative MRI in the characterization of pancreas cancer: Preliminary experience. Mol. Oncol. 2020, 14, 2176–2189. [Google Scholar] [CrossRef] [Green Version]
- Tofts, P.S.; Brix, G.; Buckley, D.; Evelhoch, J.L.; Henderson, E.; Knopp, M.V.; Larsson, H.B.; Lee, T.-Y.; Mayr, N.A.; Parker, G.; et al. Estimating kinetic parameters from dynamic contrast-enhanced t1-weighted MRI of a diffusable tracer: Standardized quantities and symbols. J. Magn. Reson. Imaging 1999, 10, 223–232. [Google Scholar] [CrossRef]
- Heid, I.; Steiger, K.; Trajkovic-Arsic, M.; Settles, M.; Eßwein, M.R.; Erkan, M.; Kleeff, J.; Jäger, C.; Friess, H.; Haller, B.; et al. Co-clinical assessment of tumor cellularity in pancreatic cancer. Clin. Cancer Res. 2016, 23, 1461–1470. [Google Scholar] [CrossRef] [Green Version]
- Mayer, P.; Jiang, Y.; Kuder, T.A.; Bergmann, F.; Khristenko, E.; Steinle, V.; Kaiser, J.; Hackert, T.; Kauczor, H.-U.; Klauß, M.; et al. Diffusion kurtosis imaging—A superior approach to assess tumor–stroma ratio in pancreatic ductal adenocarcinoma. Cancers 2020, 12, 1656. [Google Scholar] [CrossRef]
- Lee, H.-J.; Rha, S.Y.; Chung, Y.E.; Shim, H.S.; Kim, Y.J.; Hur, J.; Hong, Y.; Choi, B.W. Tumor perfusion-related parameter of diffusion-weighted magnetic resonance imaging: Correlation with histological microvessel density. Magn. Reson. Med. 2014, 71, 1554–1558. [Google Scholar] [CrossRef]
- Feig, C.; Gopinathan, A.; Neesse, A.; Chan, D.S.; Cook, N.; Tuveson, D.A. The Pancreas cancer microenvironment. Clin. Cancer Res. 2012, 18, 4266–4276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klaassen, R.; Gurney-Champion, O.; Wilmink, J.W.; Besselink, M.G.; Engelbrecht, M.R.; Stoker, J.; Nederveen, A.J.; van Laarhoven, H.W. Repeatability and correlations of dynamic contrast enhanced and T2* MRI in patients with advanced pancreatic ductal adenocarcinoma. Magn. Reson. Imaging 2018, 50, 1–9. [Google Scholar] [CrossRef]
- Gurney-Champion, O.J.; Klaassen, R.; Froeling, M.; Barbieri, S.; Stoker, J.; Engelbrecht, M.R.W.; Wilmink, J.W.; Besselink, M.G.; Bel, A.; Van Laarhoven, H.W.M.; et al. Comparison of six fit algorithms for the intra-voxel incoherent motion model of diffusion-weighted magnetic resonance imaging data of pancreatic cancer patients. PLoS ONE 2018, 13, e0194590. [Google Scholar] [CrossRef]
- Klaassen, R.; Gurney-Champion, O.J.; Engelbrecht, M.R.; Stoker, J.; Wilmink, J.W.; Besselink, M.G.; Bel, A.; van Tienhoven, G.; van Laarhoven, H.W.; Nederveen, A.J. Evaluation of six diffusion-weighted MRI models for assessing effects of neoadjuvant chemoradiation in pancreatic cancer patients. Int. J. Radiat. Oncol. 2018, 102, 1052–1062. [Google Scholar] [CrossRef] [PubMed]
- Portal, A.; Pernot, S.; Tougeron, D.; Arbaud, C.; Bidault, A.T.; De La Fouchardière, C.; Hammel, P.; Lecomte, T.; Dréanic, J.; Coriat, R.; et al. Nab-paclitaxel plus gemcitabine for metastatic pancreatic adenocarcinoma after Folfirinox failure: An AGEO prospective multicentre cohort. Br. J. Cancer 2015, 113, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Rodon, J.; Tawbi, H.A.; Thomas, A.L.; Stoller, R.G.; Turtschi, C.P.; Baselga, J.; Sarantopoulos, J.; Mahalingam, D.; Shou, Y.; Moles, M.A.; et al. A phase I, multicenter, open-label, first-in-human, dose-escalation study of the oral smoothened inhibitor Sonidegib (LDE225) in patients with advanced solid tumors. Clin. Cancer Res. 2014, 20, 1900–1909. [Google Scholar] [CrossRef] [Green Version]
- Parker, G.J.; Roberts, C.; Macdonald, A.; Buonaccorsi, G.A.; Cheung, S.; Buckley, D.L.; Jackson, A.; Watson, Y.; Davies, K.; Jayson, G.C. Experimentally-derived functional form for a population-averaged high-temporal-resolution arterial input function for dynamic contrast-enhanced MRI. Magn. Reson. Med. 2006, 56, 993–1000. [Google Scholar] [CrossRef]
- Tofts, P. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J. Magn. Reson. Imaging 1997, 7, 91–101. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Wang-Gillam, A.; Hubner, R.A.; Siveke, J.T.; Von Hoff, D.D.; Belanger, B.; de Jong, F.A.; Mirakhur, B.; Chen, L.-T. NAPOLI-1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: Final overall survival analysis and characteristics of long-term survivors. Eur. J. Cancer 2019, 108, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Hochster, H.; Stein, S.; Lacy, J. Gemcitabine plus nab-paclitaxel for advanced pancreatic cancer after first-line FOLFIRINOX: Single institution retrospective review of efficacy and toxicity. Exp. Hematol. Oncol. 2015, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Caparello, C.; Vivaldi, C.; Fornaro, L.; Musettini, G.; Pasquini, G.; Catanese, S.; Masi, G.; Lencioni, M.; Falcone, A.; Vasile, E. Second-line therapy for advanced pancreatic cancer: Evaluation of prognostic factors and review of current literature. Futur. Oncol. 2016, 12, 901–908. [Google Scholar] [CrossRef] [PubMed]
- El Rassy, E.; Assi, T.; El Karak, F.; Ghosn, M.; Kattan, J. Could the combination of Nab-paclitaxel plus gemcitabine salvage metastatic pancreatic adenocarcinoma after folfirinox failure? A single institutional retrospective analysis. Clin. Res. Hepatol. Gastroenterol. 2017, 41, e26–e28. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.T.; Kalyan, A.; Beasley, H.S.; Singhi, A.D.; Sun, W.; Zeh, H.J.; Normolle, D.; Bahary, N. Gemcitabine/nab-paclitaxel as second-line therapy following FOLFIRINOX in metastatic/advanced pancreatic cancer—retrospective analysis of response. J. Gastrointest. Oncol. 2017, 8, 556–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mita, N.; Iwashita, T.; Uemura, S.; Yoshida, K.; Iwasa, Y.; Ando, N.; Iwata, K.; Okuno, M.; Mukai, T.; Shimizu, M. Second-Line Gemcitabine Plus Nab-Paclitaxel for Patients with Unresectable Advanced Pancreatic Cancer after First-Line FOLFIRINOX Failure. J. Clin. Med. 2019, 8, 761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oettle, H.; Riess, H.; Stieler, J.M.; Heil, G.; Schwaner, I.; Seraphin, J.; Görner, M.; Mölle, M.; Greten, T.F.; Lakner, V.; et al. Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: Outcomes from the CONKO-003 trial. J. Clin. Oncol. 2014, 32, 2423–2429. [Google Scholar] [CrossRef]
- Gill, S.; Ko, Y.-J.; Cripps, C.; Beaudoin, A.; Dhesy-Thind, S.; Zulfiqar, M.; Zalewski, P.; Do, T.; Cano, P.; Lam, W.Y.H.; et al. PANCREOX: A randomized phase III study of fluorouracil/leucovorin with or without oxaliplatin for second-line advanced pancreatic cancer in patients who have received gemcitabine-based chemotherapy. J. Clin. Oncol. 2016, 34, 3914–3920. [Google Scholar] [CrossRef]
- Yoo, C.; Hwang, J.Y.; Kim, J.-E.; Kim, T.W.; Lee, J.S.; Park, D.H.; Lee, S.S.; Seo, D.W.; Kim, M.-H.; Han, D.J.; et al. A randomised phase II study of modified FOLFIRI.3 vs modified FOLFOX as second-line therapy in patients with gemcitabine-refractory advanced pancreatic cancer. Br. J. Cancer 2009, 101, 1658–1663. [Google Scholar] [CrossRef]
- Pijnappel, E.; Dijksterhuis, W.; Van Der Geest, L.; De Vos-Geelen, J.; De Groot, J.; Tije, A.T.; Homs, M.; Creemers, G.-J.; Mohammad, N.H.; Van Laarhoven, H.; et al. 1526P First and second-line palliative systemic treatment outcomes in a real-world metastatic pancreatic cancer cohort. Ann. Oncol. 2020, 31, S939–S940. [Google Scholar] [CrossRef]
- Minami, H.; Ando, Y.; Ma, B.; Lee, J.-H.; Momota, H.; Fujiwara, Y.; Li, L.; Fukino, K.; Ito, K.; Tajima, T.; et al. Phase I, multicenter, open-label, dose-escalation study of sonidegib in Asian patients with advanced solid tumors. Cancer Sci. 2016, 107, 1477–1483. [Google Scholar] [CrossRef] [Green Version]
- Migden, M.R.; Guminski, A.; Gutzmer, R.; Dirix, L.; Lewis, K.D.; Combemale, P.; Herd, R.M.; Kudchadkar, R.; Trefzer, U.; Gogov, S.; et al. Treatment with two different doses of sonidegib in patients with locally advanced or metastatic basal cell carcinoma (BOLT): A multicentre, randomised, double-blind phase 2 trial. Lancet Oncol. 2015, 16, 716–728. [Google Scholar] [CrossRef]
- Thoeny, H.C.; Ross, B.D. Predicting and monitoring cancer treatment response with diffusion-weighted MRI. J. Magn. Reson. Imaging 2010, 32, 2–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Li, J.; Fu, C.; Kühn, B.; Wang, X. Chemotherapy response of pancreatic cancer by diffusion-weighted imaging (DWI) and intravoxel incoherent motion DWI (IVIM-DWI) in an orthotopic mouse model. Magma 2019, 32, 501–509. [Google Scholar] [CrossRef]
- Galbán, C.J.; Hoff, B.A.; Chenevert, T.L.; Ross, B.D. Diffusion MRI in early cancer therapeutic response assessment. NMR Biomed. 2017, 30, e3458. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Toxicity | DLT Criteria |
|---|---|
| Toxicity leading to skipped/delayed dose | An AE (except for alopecia) of any grade, considered to be related to the study drug, leading to a dose interruption of more than 7 consecutive days, despite supportive treatment, will be considered to be a DLT. |
| Re-occurred toxicity | If the 2nd occurrence of an initially non-dose limiting toxicity (e.g., grade 1 neutropenia that resolved within 7 days at 1st occurrence) leads to a dose reduction within 42 days of the first dose of LDE225, this will be considered a DLT |
| Hematologic a | CTCAE grade 4 neutropenia for >5 consecutive days |
| CTCAE grade 4 thrombocytopenia CTCAE grade 3 with CTCAE grade > 2 bleeding | |
| CTCAE grade > 3 neutropenia with fever > 38.5 °C (non axillary) | |
| Renal | ≥CTCAE grade 3 serum creatinine |
| Hepatic | Total bilirubin ≥ 2.0× ULN to ≤ 3.0× ULN for >7 consecutive days. AST or ALT CTCAE grade ≥ 3 in conjunction with blood bilirubin CTCAE grade ≥ 2 of any duration. If not related to biliary obstruction/biliary stent dysfunction. |
| ≥CTCAE grade 3 total bilirubin. If not related to biliary obstruction/biliary stent dysfunction. | |
| CTCAE grade 3 AST or ALT for >7 consecutive days | |
| CTCAE grade 4 AST or ALT | |
| Metabolic/Laboratory | CTCAE grade 3 asymptomatic amylase and/or lipase > 7 consecutive days |
| CTCAE grade 4 asymptomatic amylase and/or lipase | |
| Pancreatitis | ≥CTCAE grade 2, if not related to biliary obstruction/stent dysfunction |
| Cardiac | Cardiac toxicity ≥ CTCAE grade 3 or cardiac event that is symptomatic or requires medical intervention |
| QTcF > 500 ms confirmed by at least one ECG | |
| Clinical signs of cardiac disease, such as unstable angina or myocardial infarction, or Troponin ≥ CTCAE grade 3 | |
| Neurotoxicity | ≥1 CTCAE grade level increase |
| Dematologic | ≥CTCAE Grade 2 photosensitivity |
| CTCAE Grade 3 rash for >7 consecutive days despite skin toxicity treatment | |
| CTCAE Grade 4 rash | |
| Fatigue | ≥CTCAE grade 3 for >7 consecutive days |
| CTCAE grade 4 | |
| Other adverse events | ≥CTCAE grade 3 adverse events (excluding ≥ CTCAE grade 3 lymphopenia or ≥ CTCAE grade 3 elevations in alkaline phosphatase |
| ≥CTCAE grade 3 vomiting/nausea ≥ 48 h, despite the use of anti-emetic therapy | |
| ≥CTCAE grade 3 diarrhea ≥ 48 h, despite the use of anti-diarrheal therapy | |
| CK elevation | ≥CTCAE grade 3 |
| Exception to DLT criteria | CTCAE grade 3 or 4 hypersensitivity or signs of allergic reaction |
| Dose Level | LDE225 | Gemcitabine | Nab-Paclitaxel | Minimum Number of Patients |
|---|---|---|---|---|
| −1 | 200 mg | 1000 mg/m2 | 125 mg/m2 | -- |
| 1 (starting) | 400 mg | 1000 mg/m2 | 125 mg/m2 | 3 |
| 2 | 600 mg | 1000 mg/m2 | 125 mg/m2 | 3 |
| 3 | 800 mg | 1000 mg/m2 | 125 mg/m2 | 3 |
| Variable | n = 30 |
|---|---|
| Gender | |
| Male | 17 (57%) |
| Female | 13 (43%) |
| Age at start of study | 62.1 (6.7) |
| WHO performance status at start study | |
| 0 | 12 (40%) |
| 1 | 16 (53%) |
| 2 | 2 (7%) |
| Prior chemotherapy | 30 (100%) |
| Prior surgery | 11 (37%) |
| Median number of cycles | 2 (2–6) |
| Median survival | 6.0 months (3.9–8.1) |
| Adverse Event | n (%) |
|---|---|
| Alopecia | 17 (6) |
| Anemia | 7 (2) |
| Anorexia | 12 (4) |
| Bacterial infection | 2 (1) |
| Chills | 7 (3) |
| Constipation | 1 (0.3) |
| Diarrhea | 28 (8) |
| Dysgeusia | 3 (1) |
| Edema limb | 6 (2) |
| Epistaxis | 2 (1) |
| Erythema multiform | 1 (0.3) |
| Eye disorder other: decreased vision | 1 (0.3) |
| Fatigue | 43 (14) |
| Febrile neutropenia | 2 (1) |
| Fever | 26 (8) |
| Flu-like symptoms | 4 (1) |
| Hematoma hands | 1 (0.3) |
| Infection | 1 (0.3) |
| Infusion related infection | 6 (2) |
| Leukocytopenia | 1 (0.3) |
| Malaise | 3 (1) |
| Mucositis oral | 11 (4) |
| Myalgia | 3 (1) |
| Nail loss | 1 (0.3) |
| Nausea | 23 (7) |
| Neuropathy | 11 (4) |
| Neutropenic fever | 1 (0.3) |
| Neutropenia | 15 (5) |
| Papulopustular rash | 1 (0.3) |
| Rash | 3 (1) |
| Rash acneiform | 1 (0.3) |
| Rash, maculo popular | 1 (0.3) |
| Sepsis | 2 (1) |
| Stomatitis | 1 (0.3) |
| Thrombocytopenia | 35 (11) |
| Vomiting | 25 (8) |
| Median (IQR 25–75%) | Wilcoxon p-Value | ||
|---|---|---|---|
| Ktrans (min−1) | Baseline | 0.172 (0.113–0.295) | 0.101 |
| Post | 0.179 (0.113–0.301) | ||
| kep (min−1) | Baseline | 0.375 (0.287–0.469) | 0.527 |
| Post | 0.343 (0.261–0.427) | ||
| ve (-) | Baseline | 0.581 (0.435–0.768) | 0.961 |
| Post | 0.623 (0.403–0.797) | ||
| vp (-) | Baseline | 0.0159 (0.0075–0.0304) | 0.005 |
| Post | 0.0190 (0.0125–0.0317) | ||
| T1 (ms) | Baseline | 674 (554–877) | 0.987 |
| Post | 695 (590–871) | ||
| D (10−3 mm2/s) | Baseline | 1.35 (1.22–1.50) | <0.001 |
| Post | 1.52 (1.39–1.69) | ||
| f (%) | Baseline | 5.1 (3.0–7.1) | 0.279 |
| Post | 5.1 (3.8–6.5) | ||
| D* (10−3 mm2/s) | Baseline | 24.0 (10.6–71.5) | 0.165 |
| Post | 45.4 (24.1–108.3) | ||
| Parameter | Cut Off Value | Sensitivity | Specificity | AUC |
|---|---|---|---|---|
| Baseline | ||||
| Ktrans (min−1) | ≥0.181 | 62% | 60% | 0.600 |
| kep (min−1) | ≤0.345 | 67% | 46% | 0.508 |
| ve (−) | ≥0.544 | 54% | 60% | 0.569 |
| vp (−) | ≥0.0155 | 69% | 60% | 0.600 |
| T1 (ms) | ≤834 | 47% | 85% | 0.528 |
| D (10−3 mm2/s) | ≥1.32 | 69% | 47% | 0.574 |
| f (%) | ≤5.1 | 80% | 85% | 0.846 |
| D* (10−3 mm2/s) | ≤22.9 | 73% | 77% | 0.779 |
| Parameter change | ||||
| ΔKtrans (%) | ≤14 | 71% | 70% | 0.614 |
| Δkep (%) | ≤−8 | 71% | 70% | 0.714 |
| Δve (%) | ≥4 | 60% | 71% | 0.571 |
| Δvp (%) | ≤60 | 86% | 80% | 0.743 |
| ΔT1 (%) | ≥−18 | 80% | 43% | 0.614 |
| ΔD (%) | ≤9 | 86% | 50% | 0.586 |
| Δf (%) | ≥16 | 80% | 86% | 0.786 |
| ΔD* (%) | ≥35 | 80% | 57% | 0.586 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pijnappel, E.N.; Wassenaar, N.P.M.; Gurney-Champion, O.J.; Klaassen, R.; van der Lee, K.; Pleunis-van Empel, M.C.H.; Richel, D.J.; Legdeur, M.C.; Nederveen, A.J.; van Laarhoven, H.W.M.; et al. Phase I/II Study of LDE225 in Combination with Gemcitabine and Nab-Paclitaxel in Patients with Metastatic Pancreatic Cancer. Cancers 2021, 13, 4869. https://doi.org/10.3390/cancers13194869
Pijnappel EN, Wassenaar NPM, Gurney-Champion OJ, Klaassen R, van der Lee K, Pleunis-van Empel MCH, Richel DJ, Legdeur MC, Nederveen AJ, van Laarhoven HWM, et al. Phase I/II Study of LDE225 in Combination with Gemcitabine and Nab-Paclitaxel in Patients with Metastatic Pancreatic Cancer. Cancers. 2021; 13(19):4869. https://doi.org/10.3390/cancers13194869
Chicago/Turabian StylePijnappel, Esther N., Nienke P. M. Wassenaar, Oliver J. Gurney-Champion, Remy Klaassen, Koen van der Lee, Marjolein C. H. Pleunis-van Empel, Dick J. Richel, Marie C. Legdeur, Aart J. Nederveen, Hanneke W. M. van Laarhoven, and et al. 2021. "Phase I/II Study of LDE225 in Combination with Gemcitabine and Nab-Paclitaxel in Patients with Metastatic Pancreatic Cancer" Cancers 13, no. 19: 4869. https://doi.org/10.3390/cancers13194869
APA StylePijnappel, E. N., Wassenaar, N. P. M., Gurney-Champion, O. J., Klaassen, R., van der Lee, K., Pleunis-van Empel, M. C. H., Richel, D. J., Legdeur, M. C., Nederveen, A. J., van Laarhoven, H. W. M., & Wilmink, J. W. (2021). Phase I/II Study of LDE225 in Combination with Gemcitabine and Nab-Paclitaxel in Patients with Metastatic Pancreatic Cancer. Cancers, 13(19), 4869. https://doi.org/10.3390/cancers13194869