
Extracorporeal Shock Wave Enhances the Cisplatin Efficacy by Improving Tissue Infiltration and Cellular Uptake in an Upper Urinary Tract Cancer Animal and Human-Derived Organoid Model

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture and Reagents
2.2. Extracorporeal Shock Wave Exposure In Vitro
2.3. Xenograft Tumour Model and Treatment Protocol
2.4. Immunohistochemistry
2.5. Western Blotting Assays
2.6. RNA Isolation and Real-Time PCR
2.7. Tissue Dissociation and Organoid Culture
2.8. Organoid Drug Response Assay
2.9. Statistical Analysis
3. Results
3.1. Shock Waves Enhanced Cisplatin Cytotoxicity in UTUC Cells
3.2. Shock Waves Improved Antitumour Effects of Cisplatin in BFTC909 and UM-UC-14 Xenografts
3.3. Combination of Cisplatin and Shock Waves Additively Suppressed Tumour Cell Proliferation and Enhanced DNA Damage In Vivo
3.4. Shock Wave Treatment Enhanced Cisplatin Delivery into Tumour through Downregulation of E-Cadherin and ZO-1
3.5. Combination of Cisplatin and Shock Waves Repressed MDR1 Expression In Vivo
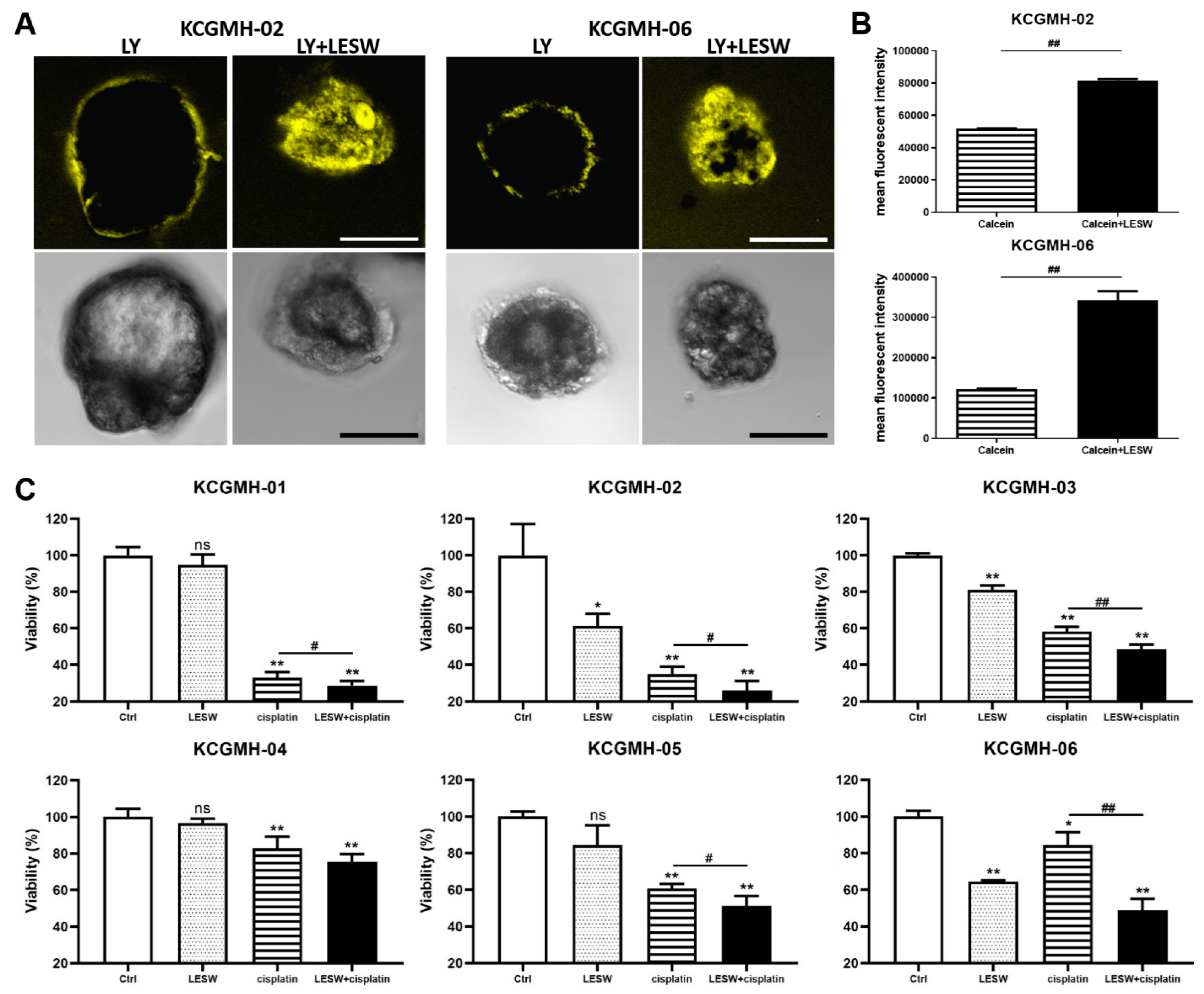
3.6. Shock Waves Improved Antitumour Effect of Cisplatin in Patient-Derived Organoid Model of UTUC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Margulis, V.; Shariat, S.F.; Matin, S.F.; Kamat, A.M.; Zigeuner, R.; Kikuchi, E.; Lotan, Y.; Weizer, A.; Raman, J.D.; Wood, C.G.; et al. Outcomes of radical nephroureterectomy: A series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer 2009, 115, 1224–1233. [Google Scholar] [CrossRef]
- Kaag, M.G.; O’Malley, R.L.; O’Malley, P.; Godoy, G.; Chen, M.; Smaldone, M.C.; Hrebinko, R.L.; Raman, J.D.; Bochner, B.; Dalbagni, G.; et al. Changes in renal function following nephroureterectomy may affect the use of perioperative chemotherapy. Eur. Urol. 2010, 58, 581–587. [Google Scholar] [CrossRef]
- Luo, H.L.; Ohyama, C.; Hatakeyama, S.; Wang, H.J.; Yoneyama, T.; Yang, W.C.; Chuang, Y.C.; Chen, Y.T.; Lee, W.C.; Cheng, Y.T.; et al. Unusual presentation of upper urinary tract urothelial carcinoma in Taiwan: Direct comparison from Taiwan-Japan UTUC Collaboration Cohort. Int. J. Urol. 2020, 27, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Tanji, N.; Fukumoto, T.; Miura, N.; Yanagihara, Y.; Shirato, A.; Azuma, K.; Miyauchi, Y.; Kikugawa, T.; Shimamoto, K.; Yokoyama, M. Combined chemotherapy with gemcitabine and carboplatin for metastatic urothelial carcinomas in patients with high renal insufficiency. Int. J. Clin. Oncol. 2013, 18, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.H.; Yen, C.C.; Chang, Y.H.; Hsieh, R.K.; Liu, J.H.; Chiou, T.J.; Fan, F.S.; Lin, A.T.; Huang, W.J.; Wang, W.S.; et al. Single agent paclitaxel as a first-line therapy in advanced urothelial carcinoma: Its efficacy and safety in patients even with pretreatment renal insufficiency. Jpn. J. Clin. Oncol. 2000, 30, 547–552. [Google Scholar] [CrossRef][Green Version]
- Massari, F.; Santoni, M.; di Nunno, V.; Cheng, L.; Lopez-Beltran, A.; Cimadamore, A.; Gasparrini, S.; Scarpelli, M.; Battelli, N.; Montironi, R. Adjuvant and neoadjuvant approaches for urothelial cancer: Updated indications and controversies. Cancer Treat. Rev. 2018, 68, 80–85. [Google Scholar] [CrossRef]
- Bahílo Mateu, P.; Budía Alba, A.; Liatsikos, E.; Trassierra Villa, M.; López-Acón, J.D.; de Guzmán Ordaz, D.; Boronat Tormo, F. Is extracorporeal shock wave lithotripsy a current treatment for urolithiasis? A systematic review. Actas Urol. Esp. 2017, 41, 426–434. [Google Scholar] [CrossRef]
- Qi, B.; Yu, T.; Wang, C.; Wang, T.; Yao, J.; Zhang, X.; Deng, P.; Xia, Y.; Junger, W.G.; Sun, D. Shock wave-induced ATP release from osteosarcoma U2OS cells promotes cellular uptake and cytotoxicity of methotrexate. J. Exp. Clin. Cancer Res. 2016, 35, 161. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Pellegrino, A.; Hallack, A.; Petrinic, N.; Jérusalem, A.; Cleveland, R.O. Response of single cells to shock waves and numerically optimized waveforms for cancer therapy. Biophys. J. 2018, 114, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Gunti, S.; Hoke, A.T.; Vu, K.P.; London, N.R., Jr. Organoid and spheroid tumor models: Techniques and applications. Cancers 2021, 13, 874. [Google Scholar] [CrossRef] [PubMed]
- Vlachogiannis, G.; Hedayat, S.; Vatsiou, A.; Jamin, Y.; Fernández-Mateos, J.; Khan, K.; Lampis, A.; Eason, K.; Huntingford, I.; Burke, R.; et al. Patient-derived organoids model treatment response of metastatic gastrointestinal cancers. Science 2018, 359, 920–926. [Google Scholar] [CrossRef]
- Choi, S.Y.; Cho, Y.H.; Kim, D.S.; Ji, W.; Choi, C.M.; Lee, J.C.; Rho, J.K.; Jeong, G.S. Establishment and long-term expansion of small cell lung cancer patient-derived tumor organoids. Int. J. Mol. Sci. 2021, 22, 1349. [Google Scholar] [CrossRef] [PubMed]
- Kopper, O.; de Witte, C.J.; Lõhmussaar, K.; Valle-Inclan, J.E.; Hami, N.; Kester, L.; Balgobind, A.V.; Korving, J.; Proost, N.; Begthel, H.; et al. An organoid platform for ovarian cancer captures intra- and interpatient heterogeneity. Nat. Med. 2019, 25, 838–849. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Hu, W.; Matulay, J.T.; Silva, M.V.; Owczarek, T.B.; Kim, K.; Chua, C.W.; Barlow, L.J.; Kandoth, C.; Williams, A.B.; et al. Tumor evolution and drug response in patient-derived organoid models of bladder cancer. Cell 2018, 173, 515–528. [Google Scholar] [CrossRef] [PubMed]
- Calandrini, C.; Schutgens, F.; Oka, R.; Margaritis, T.; Candelli, T.; Mathijsen, L.; Ammerlaan, C.; van Ineveld, R.L.; Derakhshan, S.; de Haan, S.; et al. An organoid biobank for childhood kidney cancers that captures disease and tissue heterogeneity. Nat. Commun. 2020, 11, 1310. [Google Scholar] [CrossRef]
- Ganesh, K.; Wu, C.; O’Rourke, K.P.; Szeglin, B.C.; Zheng, Y.; Sauvé, C.G.; Adileh, M.; Wasserman, I.; Marco, M.R.; Kim, A.S.; et al. A rectal cancer organoid platform to study individual responses to chemoradiation. Nat. Med. 2019, 25, 1607–1614. [Google Scholar] [CrossRef]
- Yao, Y.; Xu, X.; Yang, L.; Zhu, J.; Wan, J.; Shen, L.; Xia, F.; Fu, G.; Deng, Y.; Pan, M.; et al. Patient-derived organoids predict chemoradiation responses of locally advanced rectal cancer. Cell. Stem Cell. 2020, 26, 17–26. [Google Scholar] [CrossRef]
- Luo, H.L.; Chiang, P.H.; Huang, C.C.; Su, Y.L.; Sung, M.T.; Tsai, E.M.; Lin, C.S.; Chiang, P.H. Methylation of SPARCL1 is associated with oncologic outcome of advanced upper urinary tract urothelial carcinoma. Int. J. Mol. Sci. 2019, 20, 1653. [Google Scholar] [CrossRef]
- Shu, J.; Dolman, G.E.; Duan, J.; Qiu, G.; Ilyas, M. Statistical colour models: An automated digital image analysis method for quantification of histological biomarkers. Biomed. Eng. Online 2016, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.C.; Huang, T.L.; Tyagi, P.; Huang, C.C. Urodynamic and immunohistochemical evaluation of intravesical Botulinum Toxin A delivery using low energy shock waves. J. Urol. 2016, 196, 599–608. [Google Scholar] [CrossRef]
- Weiss, N.; Delius, M.; Gambihler, S.; Eichholtz-Wirth, H.; Dirschedl, P.; Brendel, W. Effect of shock waves and cisplatin on cisplatin-sensitive and -resistant rodent tumors in vivo. Int. J. Cancer 1994, 58, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Vinette, V.; Placet, M.; Arguin, G.; Gendron, G.P. Multidrug resistance-associated protein 2 expression is upregulated by Adenosine 5′-Triphosphate in colorectal cancer cells and enhances their survival to chemotherapeutic drugs. PLoS ONE 2015, 10, e0136080. [Google Scholar] [CrossRef]
- Hoffmann, A.C.; Wild, P.; Leicht, C.; Bertz, S.; Danenberg, K.D.; Danenberg, P.V.; Stöhr, R.; Stöckle, M.; Lehmann, J.; Schuler, M.; et al. MDR1 and ERCC1 expression predict outcome of patients with locally advanced bladder cancer receiving adjuvant chemotherapy. Neoplasia 2010, 12, 628–636. [Google Scholar] [CrossRef]
- Cheng, J.H.; Wang, C.J. Biological mechanism of shockwave in bone. Int. J. Surg. 2015, 24, 143–146. [Google Scholar] [CrossRef]
- Wang, C.J. An overview of shock wave therapy in musculoskeletal disorders. Chang. Gung Med. J. 2003, 26, 220–232. [Google Scholar]
- Adeldaeim, H.M.; Abouyoussif, T.; Gebaly, O.E.; Assem, A.; Abdel Wahab, M.M.; Rashad, H.; Sakr, M.; Zahran, A.R. Prognostic indicators for successful low-intensity extracorporeal shock wave therapy treatment of erectile dysfunction. Urology 2021, 149, 133–139. [Google Scholar] [CrossRef]
- Hsiao, C.C.; Lin, C.C.; Hou, Y.S.; Ko, J.Y.; Wang, C.J. Low-energy extracorporeal shock wave ameliorates streptozotocin induced diabetes and promotes pancreatic beta cells regeneration in a rat model. Int. J. Mol. Sci. 2019, 20, 4934. [Google Scholar] [CrossRef]
- Zeman, J.; Benes, J.; Pouckova, P.; Zadinova, M.; Lukes, P. Effect of shock waves combined with cytostatics on the growths of tumors in vivo. Physiol. Res. 2019, 68, 475–481. [Google Scholar] [CrossRef]
- Peña, M.; Delgado-Gonzalez, E.; López-Marín, L.M.; Millán-Chiu, B.E.; Fernández, F.; Rodriguez-Castelan, J.; Muñoz-Torres, C.; Carrasco, G.; Anguiano, B.; Loske, A.M.; et al. Shock wave application increases the antineoplastic effect of molecular iodine supplement in breast cancer xenografts. Ultrasound Med. Biol. 2020, 46, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Gose, J.W.; Arruda, E.M.; Liu, A.P.; Merajver, S.D.; Young, Y.L. Shock wave impact on the viability of MDA-MB-231 cells. PLoS ONE 2020, 15, e0234138. [Google Scholar] [CrossRef]
- Ha, C.H.; Lee, S.C.; Kim, S.; Chung, J.; Bae, H.; Kwon, K. Novel mechanism of gene transfection by low-energy shock wave. Sci. Rep. 2015, 5, 12843. [Google Scholar] [CrossRef] [PubMed]
- Delius, M.; Adams, G. Shock wave permeabilization with ribosome inactivating proteins: A new approach to tumor therapy. Cancer Res. 1999, 59, 5227–5232. [Google Scholar] [PubMed]
- Elkashef, A.; Barakat, N.; Khater, S.M.; Awadalla, A.; Belal, F.; El-Assmy, A.M.; Sheir, K.Z.; Shokeir, A.A. Effect of low-energy shock wave therapy on intravesical epirubicin delivery in a rat model of bladder cancer. BJU Int. 2021, 127, 80–89. [Google Scholar] [CrossRef]
- Saltsman, J.A.; Hammond, W.J.; Narayan, N.J.; Requena, D.; Gehart, H.; Lalazar, G.; LaQuaglia, M.P.; Clevers, H.; Simon, S. A human organoid model of aggressive hepatoblastoma for disease modeling and drug testing. Cancers 2020, 12, 2668. [Google Scholar] [CrossRef]
- Green, E.A.; Li, R.; Albiges, L.; Choueiri, T.K.; Freedman, M.; Pal, S.; Dyrskjøt, L.; Kamat, A.M. Clinical Utility of Cell-free and Circulating Tumor DNA in Kidney and Bladder Cancer: A Critical Review of Current Literature. Eur. Urol. Oncol. 2021, 8. S2588-9311(21)00079-1. [Google Scholar] [CrossRef]
- Ng, M.; Brown, E.; Williams, A.; Chao, M.; Lawrentschuk, N.; Chee, R. Fiducial markers and spacers in prostate radiotherapy: Current applications. BJU Int. 2014, 113 (Suppl. S2), 13–20. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, H.-L.; Liu, H.-Y.; Chang, Y.-L.; Su, Y.-L.; Huang, C.-C.; Lin, X.-J.; Chuang, Y.-C. Extracorporeal Shock Wave Enhances the Cisplatin Efficacy by Improving Tissue Infiltration and Cellular Uptake in an Upper Urinary Tract Cancer Animal and Human-Derived Organoid Model. Cancers 2021, 13, 4558. https://doi.org/10.3390/cancers13184558
Luo H-L, Liu H-Y, Chang Y-L, Su Y-L, Huang C-C, Lin X-J, Chuang Y-C. Extracorporeal Shock Wave Enhances the Cisplatin Efficacy by Improving Tissue Infiltration and Cellular Uptake in an Upper Urinary Tract Cancer Animal and Human-Derived Organoid Model. Cancers. 2021; 13(18):4558. https://doi.org/10.3390/cancers13184558
Chicago/Turabian StyleLuo, Hao-Lun, Hui-Ying Liu, Yin-Lun Chang, Yu-Li Su, Chun-Chieh Huang, Xin-Jie Lin, and Yao-Chi Chuang. 2021. "Extracorporeal Shock Wave Enhances the Cisplatin Efficacy by Improving Tissue Infiltration and Cellular Uptake in an Upper Urinary Tract Cancer Animal and Human-Derived Organoid Model" Cancers 13, no. 18: 4558. https://doi.org/10.3390/cancers13184558
APA StyleLuo, H.-L., Liu, H.-Y., Chang, Y.-L., Su, Y.-L., Huang, C.-C., Lin, X.-J., & Chuang, Y.-C. (2021). Extracorporeal Shock Wave Enhances the Cisplatin Efficacy by Improving Tissue Infiltration and Cellular Uptake in an Upper Urinary Tract Cancer Animal and Human-Derived Organoid Model. Cancers, 13(18), 4558. https://doi.org/10.3390/cancers13184558