
Survival Impact of Chronic Obstructive Pulmonary Disease or Acute Exacerbation on Patients with Rectal Adenocarcinoma Undergoing Curative Resection: A Propensity Score-Matched, Population-Based Cohort Study



Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
2.3. Propensity Score Matching and Covariates
2.4. Statistics
3. Results
3.1. Propensity Score Matching and Study Cohort
3.2. Prognostic Factors of All-Cause Mortality after Multivariate Cox Regression Analysis
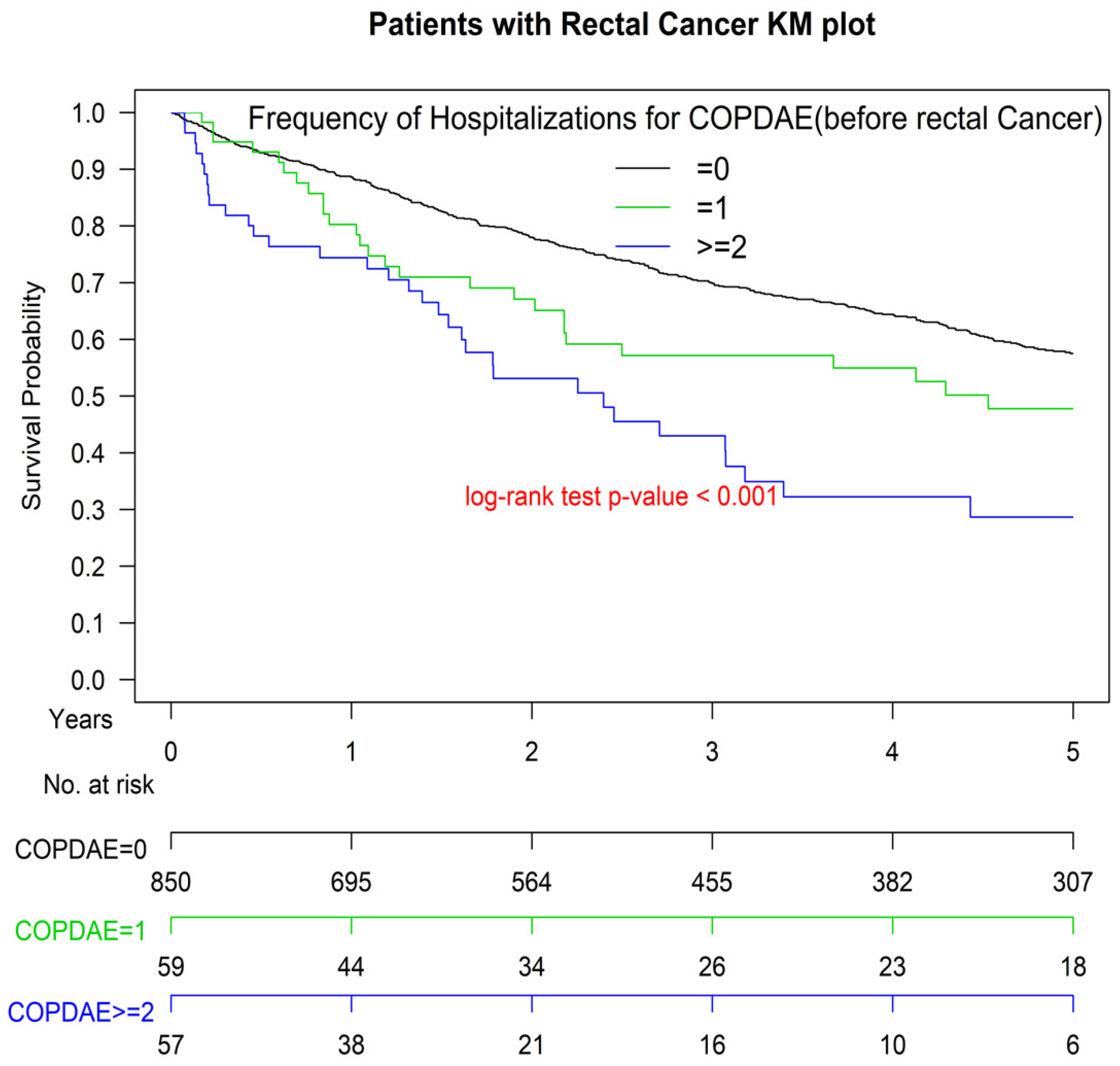
3.3. Kaplan–Meier OS among Non-COPD, COPD, and Hospitalization for COPDAE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Botteri, E.; Iodice, S.; Bagnardi, V.; Raimondi, S.; Lowenfels, A.B.; Maisonneuve, P. Smoking and colorectal cancer: A meta-analysis. JAMA 2008, 300, 2765–2778. [Google Scholar] [CrossRef]
- Botteri, E.; Iodice, S.; Raimondi, S.; Maisonneuve, P.; Lowenfels, A.B. Cigarette smoking and adenomatous polyps: A meta-analysis. Gastroenterology 2008, 134, 388–395. [Google Scholar] [CrossRef]
- Phipps, A.I.; Baron, J.; Newcomb, P.A. Prediagnostic smoking history, alcohol consumption, and colorectal cancer survival: The Seattle Colon Cancer Family Registry. Cancer 2011, 117, 4948–4957. [Google Scholar] [CrossRef]
- Phipps, A.I.; Shi, Q.; Newcomb, P.A.; Nelson, G.D.; Sargent, D.J.; Alberts, S.R.; Limburg, P.J. Associations between cigarette smoking status and colon cancer prognosis among participants in North Central Cancer Treatment Group Phase III Trial N0147. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 2016–2023. [Google Scholar] [CrossRef]
- Boyle, T.; Fritschi, L.; Platell, C.; Heyworth, J. Lifestyle factors associated with survival after colorectal cancer diagnosis. Br. J. Cancer 2013, 109, 814–822. [Google Scholar] [CrossRef]
- Yang, B.; Jacobs, E.J.; Gapstur, S.M.; Stevens, V.; Campbell, P.T. Active smoking and mortality among colorectal cancer survivors: The Cancer Prevention Study II nutrition cohort. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Walter, V.; Jansen, L.; Hoffmeister, M.; Ulrich, A.; Chang-Claude, J.; Brenner, H. Smoking and survival of colorectal cancer patients: Population-based study from Germany. Int. J. Cancer 2015, 137, 1433–1445. [Google Scholar] [CrossRef]
- Ordonez-Mena, J.M.; Walter, V.; Schottker, B.; Jenab, M.; O’Doherty, M.G.; Kee, F.; Bueno-de-Mesquita, B.; Peeters, P.H.M.; Stricker, B.H.; Ruiter, R.; et al. Impact of prediagnostic smoking and smoking cessation on colorectal cancer prognosis: A meta-analysis of individual patient data from cohorts within the CHANCES consortium. Ann. Oncol. 2018, 29, 472–483. [Google Scholar] [CrossRef]
- Hawkes, A.L.; Chambers, S.K.; Pakenham, K.I.; Patrao, T.A.; Baade, P.D.; Lynch, B.M.; Aitken, J.F.; Meng, X.; Courneya, K.S. Effects of a telephone-delivered multiple health behavior change intervention (CanChange) on health and behavioral outcomes in survivors of colorectal cancer: A randomized controlled trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 2313–2321. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; Friedenreich, C.M.; Quinney, H.A.; Fields, A.L.; Jones, L.W.; Fairey, A.S. A randomized trial of exercise and quality of life in colorectal cancer survivors. Eur. J. Cancer Care 2003, 12, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Pinto, B.M.; Papandonatos, G.D.; Goldstein, M.G.; Marcus, B.H.; Farrell, N. Home-based physical activity intervention for colorectal cancer survivors. Psychooncology 2013, 22, 54–64. [Google Scholar] [CrossRef]
- Campbell, M.K.; Carr, C.; Devellis, B.; Switzer, B.; Biddle, A.; Amamoo, M.A.; Walsh, J.; Zhou, B.; Sandler, R. A randomized trial of tailoring and motivational interviewing to promote fruit and vegetable consumption for cancer prevention and control. Ann. Behav. Med. 2009, 38, 71–85. [Google Scholar] [CrossRef]
- Tager, I.B.; Speizer, F.E. Risk estimates for chronic bronchitis in smokers: A study of male-female differences. Am. Rev. Respir. Dis. 1976, 113, 619–625. [Google Scholar] [CrossRef]
- Xu, X.; Weiss, S.T.; Rijcken, B.; Schouten, J.P. Smoking, changes in smoking habits, and rate of decline in FEV1: New insight into gender differences. Eur. Respir. J. 1994, 7, 1056–1061. [Google Scholar] [PubMed]
- Doll, R.; Peto, R. Mortality in relation to smoking: 20 years’ observations on male British doctors. Br. Med. J. 1976, 2, 1525–1536. [Google Scholar] [CrossRef] [PubMed]
- Lokke, A.; Lange, P.; Scharling, H.; Fabricius, P.; Vestbo, J. Developing COPD: A 25 year follow up study of the general population. Thorax 2006, 61, 935–939. [Google Scholar] [CrossRef]
- Van Durme, Y.; Verhamme, K.M.C.; Stijnen, T.; van Rooij, F.J.A.; Van Pottelberge, G.R.; Hofman, A.; Joos, G.F.; Stricker, B.H.C.; Brusselle, G.G. Prevalence, incidence, and lifetime risk for the development of COPD in the elderly: The Rotterdam study. Chest 2009, 135, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xu, J.; Yang, L.; Xu, Y.; Zhang, X.; Bai, C.; Kang, J.; Ran, P.; Shen, H.; Wen, F.; et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): A national cross-sectional study. Lancet 2018, 391, 1706–1717. [Google Scholar] [CrossRef]
- US Burden of Disease Collaborators; Mokdad, A.H.; Ballestros, K.; Echko, M.; Glenn, S.; Olsen, H.E.; Mullany, E.; Lee, A.; Khan, A.R.; Ahmadi, A.; et al. The State of US Health, 1990–2016: Burden of Diseases, Injuries, and Risk Factors Among US States. JAMA 2018, 319, 1444–1472. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.V.; Lee, E.; Park, B.; Jung, J.H.; Park, J.E.; Sheen, S.S.; Park, K.J.; Hwang, S.C.; Park, J.B.; Park, H.S.; et al. Cancer development in patients with COPD: A retrospective analysis of the National Health Insurance Service-National Sample Cohort in Korea. BMC Pulm. Med. 2020, 20, 170. [Google Scholar] [CrossRef] [PubMed]
- Bare, M.; Monton, C.; Mora, L.; Redondo, M.; Pont, M.; Escobar, A.; Sarasqueta, C.; Fernandez de Larrea, N.; Briones, E.; Quintana, J.M. COPD is a clear risk factor for increased use of resources and adverse outcomes in patients undergoing intervention for colorectal cancer: A nationwide study in Spain. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 1233–1241. [Google Scholar] [CrossRef]
- Platon, A.M.; Erichsen, R.; Christiansen, C.F.; Andersen, L.K.; Svaerke, C.; Montomoli, J.; Sorensen, H.T. The impact of chronic obstructive pulmonary disease on intensive care unit admission and 30-day mortality in patients undergoing colorectal cancer surgery: A Danish population-based cohort study. BMJ Open Respir. Res. 2014, 1, e000036. [Google Scholar] [CrossRef] [PubMed]
- Flynn, D.E.; Mao, D.; Yerkovich, S.T.; Franz, R.; Iswariah, H.; Hughes, A.; Shaw, I.M.; Tam, D.P.L.; Chandrasegaram, M.D. The impact of comorbidities on post-operative complications following colorectal cancer surgery. PLoS ONE 2020, 15, e0243995. [Google Scholar] [CrossRef]
- Paschke, S.; Jafarov, S.; Staib, L.; Kreuser, E.D.; Maulbecker-Armstrong, C.; Roitman, M.; Holm, T.; Harris, C.C.; Link, K.H.; Kornmann, M. Are Colon and Rectal Cancer Two Different Tumor Entities? A Proposal to Abandon the Term Colorectal Cancer. Int. J. Mol. Sci. 2018, 19, 2577. [Google Scholar] [CrossRef] [PubMed]
- Society, A.C. Cancer Facts and Figures 2015. Available online: http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf (accessed on 7 January 2015).
- Giovannucci, E.; Ascherio, A.; Rimm, E.B.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C. Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann. Intern. Med. 1995, 122, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Gerhardsson de Verdier, M.; Steineck, G.; Hagman, U.; Rieger, A.; Norell, S.E. Physical activity and colon cancer: A case-referent study in Stockholm. Int. J. Cancer 1990, 46, 985–989. [Google Scholar] [CrossRef]
- Halle, M.; Schoenberg, M.H. Physical activity in the prevention and treatment of colorectal carcinoma. Dtsch. Arztebl. Int. 2009, 106, 722–727. [Google Scholar] [CrossRef]
- Lynch, H.T.; Smyrk, T.C. Classification of familial adenomatous polyposis: A diagnostic nightmare. Am. J. Hum. Genet. 1998, 62, 1288–1289. [Google Scholar] [CrossRef]
- Konishi, K.; Fujii, T.; Boku, N.; Kato, S.; Koba, I.; Ohtsu, A.; Tajiri, H.; Ochiai, A.; Yoshida, S. Clinicopathological differences between colonic and rectal carcinomas: Are they based on the same mechanism of carcinogenesis? Gut 1999, 45, 818–821. [Google Scholar] [CrossRef]
- Lehnert, T.; Methner, M.; Pollok, A.; Schaible, A.; Hinz, U.; Herfarth, C. Multivisceral resection for locally advanced primary colon and rectal cancer: An analysis of prognostic factors in 201 patients. Ann. Surg. 2002, 235, 217–225. [Google Scholar] [CrossRef]
- Kornmann, M.; Staib, L.; Wiegel, T.; Kron, M.; Henne-Bruns, D.; Link, K.H.; Formentini, A.; Study Group Oncology of Gastrointestinal Tumors (FOGT). Long-term results of 2 adjuvant trials reveal differences in chemosensitivity and the pattern of metastases between colon cancer and rectal cancer. Clin. Colorectal Cancer 2013, 12, 54–61. [Google Scholar] [CrossRef]
- Kornmann, M.; Staib, L.; Wiegel, T.; Kreuser, E.D.; Kron, M.; Baumann, W.; Henne-Bruns, D.; Link, K.H. Adjuvant chemoradiotherapy of advanced resectable rectal cancer: Results of a randomised trial comparing modulation of 5-fluorouracil with folinic acid or with interferon-alpha. Br. J. Cancer 2010, 103, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, C.Y.; Chen, H.M.; Wu, S.Y. Neoadjuvant Chemotherapy or Endocrine Therapy for Invasive Ductal Carcinoma of the Breast with High Hormone Receptor Positivity and Human Epidermal Growth Factor Receptor 2 Negativity. JAMA Netw. Open 2021, 4, e211785. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Hsu, C.H.; Lin, Y.C.; Wu, S.Y. Effects of 1-Year Hospital Volume on Surgical Margin and Biochemical-Failure-Free Survival in Patients Undergoing Robotic versus Nonrobotic Radical Prostatectomy: A Nationwide Cohort Study from the National Taiwan Cancer Database. Cancers 2021, 13, 488. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, C.Y.; Qin, L.; Chen, H.M.; Wu, S.Y. Breast-conserving surgery with or without irradiation in women with invasive ductal carcinoma of the breast receiving preoperative systemic therapy: A cohort study. Breast 2020, 54, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.C.; Liu, H.E.; Kao, Y.W.; Qin, L.; Lin, K.C.; Fang, C.Y.; Tsai, L.L.; Shia, B.C.; Wu, S.Y. Definitive radiotherapy or surgery for early oral squamous cell carcinoma in old and very old patients: A propensity-score-matched, nationwide, population-based cohort study. Radiother. Oncol. 2020, 151, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.C.; Chen, T.M.; Yuan, K.S.; Wu, A.T.H.; Wu, S.Y. Assessment of Predictive Scoring System for 90-Day Mortality Among Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma Who Have Completed Concurrent Chemoradiotherapy. JAMA Netw. Open 2020, 3, e1920671. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology. Available online: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp (accessed on 18 June 2021).
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; van de Velde, C.J.; Balmana, J.; Regula, J.; et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef] [PubMed]
- Valentini, V.; Aristei, C.; Glimelius, B.; Minsky, B.D.; Beets-Tan, R.; Borras, J.M.; Haustermans, K.; Maingon, P.; Overgaard, J.; Pahlman, L.; et al. Multidisciplinary Rectal Cancer Management: 2nd European Rectal Cancer Consensus Conference (EURECA-CC2). Radiother. Oncol. 2009, 92, 148–163. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Chen, J.H.; Yen, Y.C.; Yang, H.C.; Liu, S.H.; Yuan, S.P.; Wu, L.L.; Lee, F.P.; Lin, K.C.; Lai, M.T.; Wu, C.C.; et al. Curative-Intent Aggressive Treatment Improves Survival in Elderly Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma and High Comorbidity Index. Medicine 2016, 95, e3268. [Google Scholar] [CrossRef]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. The performance of different propensity score methods for estimating marginal hazard ratios. Stat. Med. 2013, 32, 2837–2849. [Google Scholar] [CrossRef]
- Austin, P.C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2014, 33, 1242–1258. [Google Scholar] [CrossRef] [PubMed]
- Hisada, H.; Takahashi, Y.; Kubota, M.; Shimura, H.; Itobayashi, E.; Shimura, K.; Nakamura, A. Clinical and therapeutic features and prognostic factors of metastatic colorectal cancer over age 80: A retrospective study. BMC Gastroenterol. 2021, 21, 199. [Google Scholar] [CrossRef]
- Laohavinij, S.; Maneechavakajorn, J.; Techatanol, P. Prognostic factors for survival in colorectal cancer patients. J. Med. Assoc. Thai. 2010, 93, 1156–1166. [Google Scholar]
- Pule, M.L.; Buckley, E.; Niyonsenga, T.; Roder, D. The effects of comorbidity on colorectal cancer mortality in an Australian cancer population. Sci. Rep. 2019, 9, 8580. [Google Scholar] [CrossRef] [PubMed]
- Jm, J.; Rm, G.; Ea, A. Colon and Rectum. In AJCC Cancer Staging Manual, 8th ed.; Mb, A., Ed.; American Joint Commitee on Cancer: Chicago, IL, USA, 2018. [Google Scholar]
- Liebig, C.; Ayala, G.; Wilks, J.; Verstovsek, G.; Liu, H.; Agarwal, N.; Berger, D.H.; Albo, D. Perineural invasion is an independent predictor of outcome in colorectal cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 5131–5137. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, A.M.; Lee, J.L.; Kim, J.; Lim, S.B.; Yu, C.S.; Kim, T.W.; Kim, J.H.; Kim, J.C. Prognostic and Oncologic Significance of Perineural Invasion in Sporadic Colorectal Cancer. Ann. Surg. Oncol. 2017, 24, 1626–1634. [Google Scholar] [CrossRef]
- Hogan, J.; Chang, K.H.; Duff, G.; Samaha, G.; Kelly, N.; Burton, M.; Burton, E.; Coffey, J.C. Lymphovascular invasion: A comprehensive appraisal in colon and rectal adenocarcinoma. Dis. Colon Rectum 2015, 58, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, D.; Paty, P.B.; Picon, A.I.; Guillem, J.G.; Klimstra, D.S.; Minsky, B.D.; Quan, S.H.; Cohen, A.M. Stage I rectal cancer: Identification of high-risk patients. J. Am. Coll. Surg. 1998, 186, 574–579, discussion 579–580. [Google Scholar] [CrossRef]
- Willett, C.G.; Badizadegan, K.; Ancukiewicz, M.; Shellito, P.C. Prognostic factors in stage T3N0 rectal cancer: Do all patients require postoperative pelvic irradiation and chemotherapy? Dis. Colon Rectum 1999, 42, 167–173. [Google Scholar] [CrossRef]
- Kodner, I.J.; Shemesh, E.I.; Fry, R.D.; Walz, B.J.; Myerson, R.; Fleshman, J.W.; Schechtman, K.B. Preoperative irradiation for rectal cancer. Improved local control and long-term survival. Ann. Surg. 1989, 209, 194–199. [Google Scholar] [CrossRef]
- Gosens, M.J.; Klaassen, R.A.; Tan-Go, I.; Rutten, H.J.; Martijn, H.; van den Brule, A.J.; Nieuwenhuijzen, G.A.; van Krieken, J.H.; Nagtegaal, I.D. Circumferential margin involvement is the crucial prognostic factor after multimodality treatment in patients with locally advanced rectal carcinoma. Clin. Cancer Res. 2007, 13, 6617–6623. [Google Scholar] [CrossRef]
- Compton, C.C.; Fielding, L.P.; Burgart, L.J.; Conley, B.; Cooper, H.S.; Hamilton, S.R.; Hammond, M.E.; Henson, D.E.; Hutter, R.V.; Nagle, R.B.; et al. Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch. Pathol. Lab. Med. 2000, 124, 979–994. [Google Scholar] [CrossRef]
- Le, H.; Ziogas, A.; Lipkin, S.M.; Zell, J.A. Effects of socioeconomic status and treatment disparities in colorectal cancer survival. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1950–1962. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, D.Y.; Boyer, M.J.; Hong, J.C.; Williams, C.D.; Kelley, M.J.; Salama, J.K.; Palta, M. Survival Advantage with Adjuvant Chemotherapy for Locoregionally Advanced Rectal Cancer: A Veterans Health Administration Analysis. J. Natl. Compr. Cancer Netw. 2020, 18, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.; Gao, P.; Wang, H.; Xu, Q.; Song, Y.; Huang, X.; Sun, J.; Zhao, J.; Luo, J.; Sun, Y.; et al. What has preoperative radio(chemo)therapy brought to localized rectal cancer patients in terms of perioperative and long-term outcomes over the past decades? A systematic review and meta-analysis based on 41,121 patients. Int. J. Cancer 2017, 141, 1052–1065. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease. In Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2018 Report); Global Initiative for Chronic Obstructive Lung Disease: Delavan, WI, USA, 2018.
- Portegies, M.L.; Lahousse, L.; Joos, G.F.; Hofman, A.; Koudstaal, P.J.; Stricker, B.H.; Brusselle, G.G.; Ikram, M.A. Chronic Obstructive Pulmonary Disease and the Risk of Stroke. The Rotterdam Study. Am. J. Respir. Crit. Care Med. 2016, 193, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Takagi, H.; Umemoto, T.; Group, A. A Meta-Analysis of the Association of Chronic Obstructive Pulmonary Disease with Abdominal Aortic Aneurysm Presence. Ann. Vasc. Surg. 2016, 34, 84–94. [Google Scholar] [CrossRef]
- Meteran, H.; Backer, V.; Kyvik, K.O.; Skytthe, A.; Thomsen, S.F. Comorbidity between chronic obstructive pulmonary disease and type 2 diabetes: A nation-wide cohort twin study. Respir. Med. 2015, 109, 1026–1030. [Google Scholar] [CrossRef]
- Incalzi, R.A.; Corsonello, A.; Pedone, C.; Battaglia, S.; Paglino, G.; Bellia, V.; Extrapulmonary Consequences of, C.i.t.E.S.I. Chronic renal failure: A neglected comorbidity of COPD. Chest 2010, 137, 831–837. [Google Scholar] [CrossRef]
- Vespasiani-Gentilucci, U.; Pedone, C.; Muley-Vilamu, M.; Antonelli-Incalzi, R. The pharmacological treatment of chronic comorbidities in COPD: Mind the gap! Pulm. Pharmacol. Ther. 2018, 51, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Dong, W.; Du, Y.; Ma, S. Impact of chemotherapy in the prognosis of non-small-cell lung cancer patients with severe to very severe COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 3805–3812. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.P.; McAvay, G.J.; Guo, Z.; Tinetti, M.E. The impact of chronic illnesses on the use and effectiveness of adjuvant chemotherapy for colon cancer. Cancer 2007, 109, 2410–2419. [Google Scholar] [CrossRef] [PubMed]
- Riesco, J.A.; Alcazar, B.; Trigueros, J.A.; Campuzano, A.; Perez, J.; Lorenzo, J.L. Active smoking and COPD phenotype: Distribution and impact on prognostic factors. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 1989–1999. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Non-COPD Patients | COPD Patients | p-Value | ||
|---|---|---|---|---|---|
| N = 644 | (100%) | N = 322 | (100%) | ||
| Age (mean ± SD) | (71.96 ± 10.10) | (71.51 ± 9.72) | 0.821 | ||
| Age (years) | 0.372 | ||||
| ≤65 | 153 | 23.76% | 74 | 22.98% | |
| 65–75 | 224 | 34.78% | 109 | 33.85% | |
| 75–85 | 221 | 34.32% | 110 | 34.16% | |
| >85 | 46 | 7.14% | 29 | 9.00% | |
| Sex | 0.788 | ||||
| Female | 205 | 31.83% | 99 | 30.75% | |
| Male | 439 | 68.17% | 223 | 69.25% | |
| Diabetes | 0.306 | ||||
| No | 462 | 71.74% | 220 | 68.32% | |
| Yes | 182 | 28.26% | 102 | 31.68% | |
| Hyperlipidemia | 0.588 | ||||
| No | 470 | 72.98% | 241 | 74.84% | |
| Yes | 174 | 27.02% | 81 | 25.16% | |
| Hypertension | 0.769 | ||||
| No | 587 | 91.15% | 292 | 90.68% | |
| Yes | 57 | 8.85% | 30 | 9.32% | |
| CKD | 0.998 | ||||
| No | 633 | 98.29% | 316 | 98.14% | |
| Yes | 11 | 1.71% | 6 | 1.86% | |
| Cardiovascular diseases | 0.822 | ||||
| No | 551 | 85.56% | 273 | 84.78% | |
| Yes | 93 | 14.44% | 49 | 15.22% | |
| CCI score | 0.876 | ||||
| 0 | 394 | 61.18% | 200 | 62.11% | |
| ≥1 | 250 | 38.82% | 122 | 37.89% | |
| AJCC pathologic stages | 0.950 | ||||
| I | 27 | 4.19% | 16 | 4.97% | |
| II | 180 | 27.95% | 90 | 27.95% | |
| IIIA | 177 | 27.48% | 87 | 27.02% | |
| IIIB | 216 | 33.54% | 106 | 32.92% | |
| IIIC | 44 | 6.83% | 23 | 7.14% | |
| Grade of differentiation | 0.881 | ||||
| Low | 201 | 31.21% | 107 | 33.23% | |
| Moderate | 315 | 48.91% | 154 | 47.83% | |
| High | 128 | 19.88% | 61 | 18.94% | |
| Lymphovascular invasion | 0.726 | ||||
| No | 401 | 62.27% | 196 | 60.87% | |
| Yes | 243 | 37.73% | 126 | 39.13% | |
| Perineural invasion | 0.741 | ||||
| No | 440 | 68.32% | 223 | 69.25% | |
| Yes | 204 | 31.68% | 99 | 30.75% | |
| Margin (distal and circumferential margin) | 0.212 | ||||
| Negative | 619 | 96.12% | 308 | 95.65% | |
| Positive | 25 | 3.88% | 14 | 4.35% | |
| Neoadjuvant CCRT | 0.601 | ||||
| No | 307 | 47.67% | 160 | 49.69% | |
| Yes | 337 | 52.33% | 162 | 50.31% | |
| Adjuvant chemotherapy | 0.855 | ||||
| No | 295 | 45.81% | 149 | 46.63% | |
| Yes | 349 | 54.19% | 173 | 53.73% | |
| Incomes Levels | 0.811 | ||||
| Low (<20,000 NTD) | 330 | 51.24% | 168 | 52.17% | |
| Middle (20,000–30,000 NTD) | 229 | 35.56% | 116 | 36.02% | |
| High (>30,000 NTD) | 85 | 13.20% | 38 | 11.81% | |
| Frequency of Hospitalizations for COPDAE (1 year before rectal cancer) | <0.001 | ||||
| 0 | 644 | 100.00% | 206 | 63.98% | |
| 1 | 0 | 0.00% | 59 | 18.32% | |
| ≥2 | 0 | 0.00% | 57 | 17.70% | |
| Follow up (Death) | <0.001 | ||||
| Years, Median (IQR, Q1, Q3) | 4.64 (1.53, 7.04) | 3.40 (1.11, 5.53) | |||
| Follow up (Death) | <0.001 | ||||
| Years (mean ± SD) | 5.74 ± 4.06 | 3.95 ± 3.45 | |||
| Death | 0.039 | ||||
| No | 346 | 53.73% | 148 | 45.96% | |
| Yes | 298 | 46.27% | 174 | 54.04% | |
| Variables | Crude HR (95% CI) | Adjusted HR * (95% CI) | p-Value | ||
|---|---|---|---|---|---|
| COPD status (ref: non-COPD) | |||||
| COPD | 1.41 | (1.17, 1.71) | 1.25 | (1.04, 1.51) | 0.019 |
| Frequency of hospitalization for COPDAE before rectal cancer (ref: 0) | |||||
| 1 | 1.42 | (1.01, 1.93) | 1.17 | (1.05, 1.51) | 0.021 |
| ≥2 | 2.33 | (1.63, 3.36) | 1.48 | (1.03, 2.41) | 0.024 |
| Sex (ref: Female) | |||||
| Male | 0.95 | (0.79, 1.16) | 1.09 | (0.87, 1.31) | 0.432 |
| Age (years; ref: ≤65 y) | |||||
| 65–75 | 1.71 | (1.27, 2.25) | 1.37 | (1.02, 1.84) | 0.023 |
| 75–85 | 2.44 | (1.75, 3.33) | 2.23 | (1.70, 3.01) | <0.001 |
| >85 | 4.62 | (3.30, 6.91) | 3.94 | (2.61, 5.90) | <0.001 |
| CCI Score (ref: 0) | |||||
| ≥1 | 1.61 | (1.34, 1.93) | 1.49 | (1.19, 1.86) | <0.001 |
| Diabetes (ref: No) | |||||
| Yes | 1.46 | (1.15, 1.86) | 1.16 | (0.86, 1.57) | 0.284 |
| Hyperlipidemia (ref: No) | |||||
| Yes | 1.02 | (0.73, 1.13) | 1.01 | (0.63, 1.04) | 0.183 |
| Hypertension (ref: No) | |||||
| Yes | 1.07 | (0.78, 1.19) | 1.01 | (0.71, 1.14) | 0.691 |
| Cardiovascular diseases (ref: No) | |||||
| Yes | 1.91 | (1.21, 2.44) | 1.17 | (0.88, 1.81) | 0.277 |
| CKD (ref: No) | |||||
| Yes | 1.07 | (0.80, 1.19) | 1.04 | (0.73, 1.16) | 0.505 |
| Lymphovascular invasion (ref: No) | |||||
| Yes | 1.41 | (1.10, 1.81) | 1.12 | (0.81, 1.57) | 0.288 |
| Perineural invasion (ref: No) | |||||
| Yes | 1.82 | (1.36, 2.42) | 1.16 | (0.78, 1.69) | 0.295 |
| Pathologic stage (ref: Stage I) | |||||
| II | 1.72 | (1.02, 3.11) | 1.21 | (0.81, 2.19) | 0.462 |
| IIIA | 2.13 | (1.55, 2.90) | 1.55 | (1.12, 2.77) | 0.021 |
| IIIB | 2.85 | (1.70, 3.71) | 1.85 | (1.18, 3.27) | 0.019 |
| IIIC | 3.26 | (1.80, 6.19) | 1.97 | (1.07, 3.58) | 0.031 |
| Grade of differentiation (ref: Low grade) | |||||
| Moderate | 1.37 | (1.12, 1.68) | 1.14 | (1.07, 1.52) | 0.009 |
| High | 1.44 | (1.18, 1.71) | 1.23 | (1.03, 1.41) | 0.017 |
| Neoadjuvant CCRT (ref: No) | |||||
| Yes | 0.71 | (0.60, 1.04) | 0.81 | (0.63, 1.03) | 0.213 |
| Adjuvant chemotherapy (ref: No) | |||||
| Yes | 0.88 | (0.75, 1.19) | 0.86 | (0.73, 1.15) | 0.534 |
| Incomes Levels (ref: low) | |||||
| Middle (20,000–30,000 NTD) | 1.11 | (1.01, 1.27) | 1.03 | (0.97, 1.21) | 0.059 |
| High (>30,000 NTD) | 1.24 | (1.03, 1.39) | 1.13 | (0.83, 1.30) | 0.066 |
| Margin status (ref: Negative) | |||||
| Positive | 1.09 | (0.91, 1.32) | 1.04 | (0.90, 1.30) | 0.057 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Chiu, K.-C.; Lin, W.-C.; Wu, S.-Y. Survival Impact of Chronic Obstructive Pulmonary Disease or Acute Exacerbation on Patients with Rectal Adenocarcinoma Undergoing Curative Resection: A Propensity Score-Matched, Population-Based Cohort Study. Cancers 2021, 13, 4221. https://doi.org/10.3390/cancers13164221
Zhang J, Chiu K-C, Lin W-C, Wu S-Y. Survival Impact of Chronic Obstructive Pulmonary Disease or Acute Exacerbation on Patients with Rectal Adenocarcinoma Undergoing Curative Resection: A Propensity Score-Matched, Population-Based Cohort Study. Cancers. 2021; 13(16):4221. https://doi.org/10.3390/cancers13164221
Chicago/Turabian StyleZhang, Jiaqiang, Kuo-Chin Chiu, Wei-Chun Lin, and Szu-Yuan Wu. 2021. "Survival Impact of Chronic Obstructive Pulmonary Disease or Acute Exacerbation on Patients with Rectal Adenocarcinoma Undergoing Curative Resection: A Propensity Score-Matched, Population-Based Cohort Study" Cancers 13, no. 16: 4221. https://doi.org/10.3390/cancers13164221
APA StyleZhang, J., Chiu, K.-C., Lin, W.-C., & Wu, S.-Y. (2021). Survival Impact of Chronic Obstructive Pulmonary Disease or Acute Exacerbation on Patients with Rectal Adenocarcinoma Undergoing Curative Resection: A Propensity Score-Matched, Population-Based Cohort Study. Cancers, 13(16), 4221. https://doi.org/10.3390/cancers13164221