
Post-Vaccination Anti-SARS-CoV-2-Antibody Response in Patients with Multiple Myeloma Correlates with Low CD19+ B-Lymphocyte Count and Anti-CD38 Treatment

 , ,
, ,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
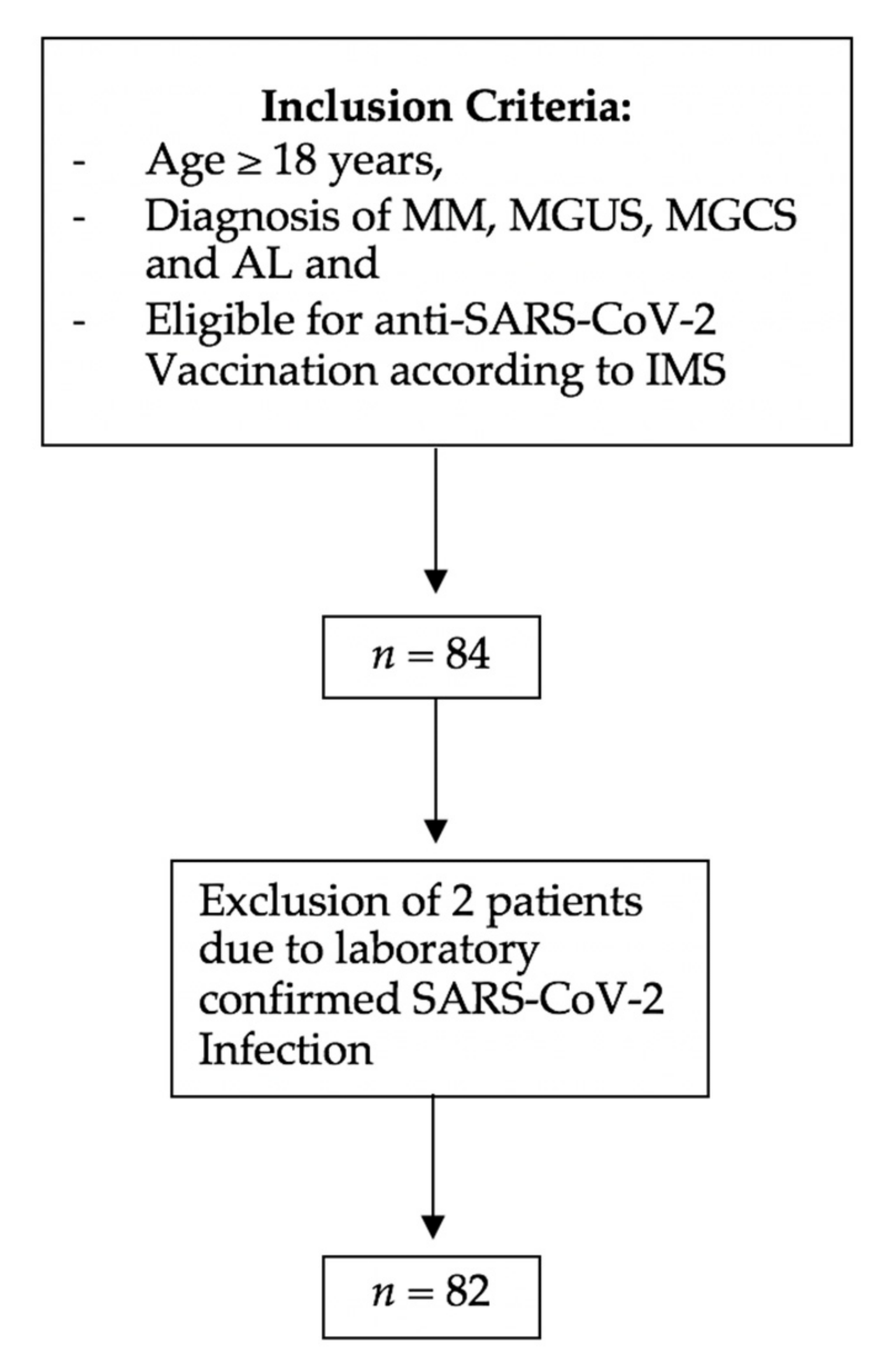
2.1. Study Design and Patients
2.2. Detection of Anti-SARS CoV-2 Antibodies
2.3. Flow Cytometry Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blimark, C.; Holmberg, E.; Mellqvist, U.H.; Landgren, O.; Bjorkholm, M.; Hultcrantz, M.; Kjellander, C.; Turesson, I.; Kristinsson, S.Y. Multiple myeloma and infections: A population-based study on 9253 multiple myeloma pa-tients. Haematologica 2015, 100, 107–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawstron, A.C.; Davies, F.E.; Owen, R.G.; English, A.; Pratt, G.; Child, J.A.; Jack, A.S.; Morgan, G.J. B-lymphocyte sup-pression in multiple myeloma is a reversible phenomenon specific to normal B-cell progen-itors and plasma cell precursors. Br. J. Haematol. 1998, 100, 176–183. [Google Scholar] [CrossRef]
- Chen, L.; Diao, L.; Yang, Y.; Yi, X.; Rodriguez, B.L.; Li, Y.; Villalobos, P.A.; Cascone, T.; Liu, X.; Tan, L.; et al. CD38-Mediated Immunosuppression as a Mechanism of Tumor Cell Escape from PD-1/PD-L1 Blockade. Cancer Discov. 2018, 8, 1156–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshua, D.; Suen, H.; Brown, R.; Bryant, C.; Ho, P.J.; Hart, D.; Gibson, J. The T Cell in Myeloma. Clin. Lymphoma Myeloma Leuk. 2016, 16, 537–542. [Google Scholar] [CrossRef]
- Pratt, G.; Goodyear, O.; Moss, P. Immunodeficiency and immunotherapy in multiple myeloma. Br. J. Haematol. 2007, 138, 563–579. [Google Scholar] [CrossRef] [PubMed]
- Frerichs, K.A.; Bosman, P.W.; Van Velzen, J.F.; Fraaij, P.L.; Koopmans, M.P.; Rimmelzwaan, G.F.; Nijhof, I.S.; Bloem, A.C.; Mutis, T.; Zweegman, S.; et al. Effect of daratumumab on normal plasma cells, polyclonal immunoglobulin levels, and vaccination responses in extensively pre-treated multiple myeloma patients. Haematologica 2019, 105, e302–e306. [Google Scholar] [CrossRef] [Green Version]
- Flores-Borja, F.; Bosma, A.; Ng, D.; Reddy, V.; Ehrenstein, M.R.; Isenberg, D.A.; Mauri, C. CD19+CD24hiCD38hi B cells maintain regulatory T cells while limiting TH1 and TH17 dif-ferentiation. Sci. Transl. Med. 2013, 5, 173ra23. [Google Scholar] [CrossRef]
- Krejcik, J.; Casneuf, T.; Nijhof, I.S.; Verbist, B.; Bald, J.; Plesner, T.; Syed, K.; Liu, K.; Van De Donk, N.W.C.J.; Weiss, B.M.; et al. Daratumumab depletes CD38+ immune regulatory cells, promotes T-cell expansion, and skews T-cell repertoire in multiple myeloma. Blood 2016, 128, 384–394. [Google Scholar] [CrossRef] [Green Version]
- Moreno, L.; Perez, C.; Zabaleta, A.; Manrique, I.; Alignani, D.; Ajona, D.; Blanco, L.; Lasa, M.; Maiso, P.; Rodriguez, I.; et al. The Mechanism of Action of the Anti-CD38 Monoclonal Antibody Isatuximab in Multiple Myeloma. Clin. Cancer Res. 2019, 25, 3176–3187. [Google Scholar] [CrossRef] [Green Version]
- Chari, A.; Samur, M.K.; Martinez-Lopez, J.; Cook, G.; Biran, N.; Yong, K.; Hungria, V.; Engelhardt, M.; Gay, F.; Feria, A.G.; et al. Clinical features associated with COVID-19 outcome in multiple myeloma: First results from the International Myeloma Society data set. Blood 2020, 136, 3033–3040. [Google Scholar] [CrossRef]
- European-Medicines-Agency. COVID-19 Vaccine Moderna. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/covid-19-vaccine-moderna (accessed on 14 June 2021).
- European-Medicines-Agency. Comirnaty. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty (accessed on 14 June 2021).
- US FDA. Moderna COVID-19 Vaccine|FDA: @US_FDA. 2021. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/moderna-covid-19-vaccine (accessed on 14 June 2021).
- US FDA. Pfizer-BioNTech COVID-19 Vaccine. 2021. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccine (accessed on 14 June 2021).
- European-Medicines-Agency. Vaxzevria (Previously COVID-19 Vaccine AstraZeneca). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria-previously-covid-19-vaccine-astrazeneca (accessed on 14 June 2021).
- Association TEH. Expert Opinions for COVID-19 Vaccination in Patients with Hematologic Cancer: Eha_Hematology. 2021. Available online: https://ehaweb.org/covid-19/eha-statement-on-covid-19-vaccines/recommendations-for-covid-19-vaccination-in-patients-with-hematologic-cancer/ (accessed on 14 June 2021).
- ASH-ASTCT COVID-19 and Vaccines: Frequently Asked Questions—Hematology.org. 2021. Available online: https://www.hematology.org:443/covid-19/ash-astct-covid-19-and-vaccines (accessed on 14 June 2021).
- International-Myeloma-Society. Recommendations for anti-Covid-19 Vaccination in Patients with Multiple Myeloma (MM) and Related Conditions, AL Amyloidosis and Other Monoclonal Gammopathies of Clinical Significance. Available online: https://myelomasociety.org/wp-content/uploads/2021/03/PM-COVID-vaccination-in-MM-guidelines-The-Final.pdf (accessed on 14 June 2021).
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. Interna-tional Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kumar, S.; Paiva, B.; Anderson, K.C.; Durie, B.; Landgren, O.; Moreau, P.; Munshi, N.; Lonial, S.; Blade, J.; Mateos, M.-V.; et al. International Mye-loma Working Group consensus criteria for response and minimal residual disease assess-ment in multiple myeloma. Lancet Oncol. 2016, 17, e328–e346. [Google Scholar] [CrossRef]
- Gertz, M.A.; Comenzo, R.; Falk, R.H.; Fermand, J.P.; Hazenberg, B.P.; Hawkins, P.N.; Merlini, G.; Moreau, P.; Ronco, P.; Sanchorawala, V.; et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): A consensus opinion from the 10th International Symposium on Amyloid and Amy-loidosis, Tours, France, 18–22 April 2004. Am. J. Hematol. 2005, 79, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Palladini, G.; Dispenzieri, A.; Gertz, M.A.; Kumar, S.; Wechalekar, A.; Hawkins, P.N.; Schönland, S.; Hegenbart, U.; Comenzo, R.; Kastritis, E.; et al. New Criteria for Response to Treatment in Immunoglobulin Light Chain Amyloidosis Based on Free Light Chain Measurement and Cardiac Biomarkers: Impact on Survival Outcomes. J. Clin. Oncol. 2012, 30, 4541–4549. [Google Scholar] [CrossRef]
- Rajkumar, S.V.; Richardson, P.; Miguel, J.S. Guidelines for determination of the number of prior lines of therapy in multiple myeloma. Blood 2015, 126, 921–922. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, U.H.; Cornell, R.F.; Lakshman, A.; Gahvari, Z.J.; McGehee, E.; Jagosky, M.H.; Gupta, R.; Varnado, W.; Fiala, M.A.; Chhabra, S.; et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia 2019, 33, 2266–2275. [Google Scholar] [CrossRef] [PubMed]
- Monin-Aldama, L.; Laing, A.G.; Munoz-Ruiz, M.; McKenzie, D.R.; del Barrio, I.D.M.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Interim results of the safety and immune-efficacy of 1 versus 2 doses of COVID-19 vaccine BNT162b2 for cancer patients in the context of the UK vaccine priority guidelines. medRxiv 2021. [Google Scholar] [CrossRef]
- Favresse, J.; Bayart, J.L.; Mullier, F.; Dogne, J.M.; Closset, M.; Douxfils, J. Early antibody response in health-care professionals after two doses of SARS-CoV-2 mRNA vaccine (BNT162b2). Clin. Microbiol. Infect. 2021. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1-2a Trial of Ad26.COV2.S Covid-19 Vaccine. N. Engl. J. Med. 2021, 384, 1824–1835. [Google Scholar] [CrossRef] [PubMed]
- Collier, D.A.; Ferreira, I.A.; Kotagiri, P.; Datir, R.; Lim, E.; Touizer, E.; Meng, B.; Abdullahi, A.; Elmer, A.; Kingston, N.; et al. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2020, 396, 1979–1993. [Google Scholar] [CrossRef]
- Pimpinelli, F.; Marchesi, F.; Piaggio, G.; Giannarelli, D.; Papa, E.; Falcucci, P.; Pontone, M.; Martino, S.D.; Laquintana, V.; Malfa, A.L.; et al. Fifth-week immunogenicity and safety of anti-SARS-CoV-2 BNT162b2 vaccine in patients with multiple myeloma and myeloproliferative malignancies on active treatment: Preliminary data from a single institution. J. Hematol. Oncol. 2021, 14, 81. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.; Panopoulou, A.; Shea, R.L.; Tsui, M.; Saso, R.; Sud, A.; West, S.; Smith, K.; Barwood, J.; Kaczmarek, E.; et al. Response to first vaccination against SARS-CoV-2 in patients with multiple myeloma. Lancet Haematol. 2021, 8, e389–e392. [Google Scholar] [CrossRef]
- Terpos, E.; Trougakos, I.P.; Gavriatopoulou, M.; Papassotiriou, I.; Sklirou, A.D.; Ntana-sis-Stathopoulos, I.; Papanagnou, E.D.; Fotiou, D.; Kastritis, E.; Dimopoulos, M.A. Low Neutralizing Antibody Responses Against SARS-CoV-2 in Elderly Myeloma Patients After the First BNT162b2 Vaccine Dose. Blood J. Am. Soc. Hematol. 2021, 137, 3674–3676. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Variable | SP-AbT Negative | SP-AbT Positive | SP-AbT Missing | p-Value | Total |
|---|---|---|---|---|---|
| Age, median age in years (range) | 68.54 | 58.65 | 68.5 | <0.01 | 67.5 (40–85) |
| Sex, n (%) | |||||
| Male | 33 | 12 | 4 | 0.41 | 49 (59.8) |
| Female | 24 | 5 | 4 | 33 (40.2) | |
| Charlson Comorbidity Index (mean; range) | 2.94 | 2.56 | 2.75 | 0.01 | 2.72 (2–6) |
| Plasma-cell-related neoplasia, n (%) | |||||
| MM | 78 (95.1) | ||||
| Smoldering MM | 0 | ||||
| MGCS | 2 (2.4) | ||||
| MGUS | 0 | ||||
| AL | 2 (2.4) | ||||
| Newly diagnosed | 25 | 11 | 0.17 | 40 (48.8) | |
| R/R Disease | 32 | 6 | 42 (51.2) | ||
| Triple-refractory | 10 | 0 | 10 (12.2) | ||
| Penta-refractory | 3 | 0 | 3 (3.7) | ||
| Anti-myeloma therapy, n (%) | 69 (84.1) | ||||
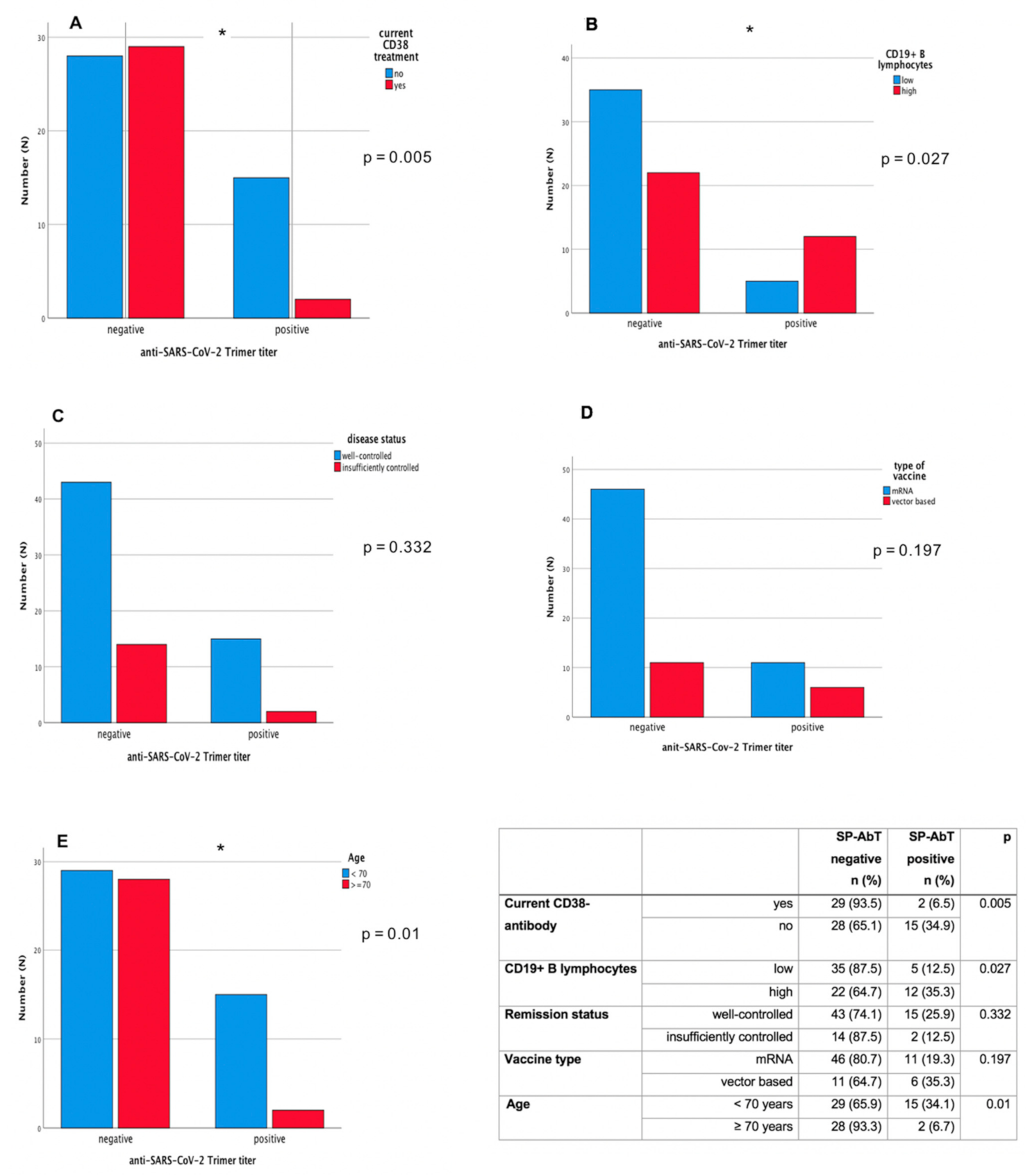
| Anti-CD38 monoclonal antibody in total | 29 | 2 | 3 | 0.005 | 34 (41.5) |
| Daratumumab-based | 25 (30.5) | ||||
| Isatuximab-based | 9 (11.0) | ||||
| Mean duration of CD38-based therapy in months (range) | 9.5 (0–50) | ||||
| Anti-SLAMF7-monoclonal antibody (elotuzumab)-based | 3 (3.7) | ||||
| IMiD-based therapies in total | 39 | 8 | 52 (63.4) | ||
| Thalidomide | 1 | 0 | 1 (1.2) | ||
| Lenalidomide | 32 | 8 | 45 (54.9) | ||
| Pomalidomide | 6 | 0 | 6 (7.3) | ||
| Proteasome inhibitors in total | 13 | 2 | 16 (19.5) | ||
| Bortezomib-based | 0 | 1 | 2 (2.4) | ||
| Carfilzomib-based | 13 | 1 | 14 (17.1) | ||
| No current therapy | 7 | 6 | 13 (15.8) | ||
| Therapy lines, median number of therapy lines in total (range) | 1 (0–10) | ||||
| untreated | 6 (7.3) | ||||
| 1st line, n (%) | 42 (51.8) | ||||
| 2nd line, n (%) | 11 (13.4) | ||||
| 3rd line, n (%) | 12 (14.6) | ||||
| >3rd line, n (%) | 11 (13.4) | ||||
| Remission status at time of vaccination | |||||
| Well-controlled disease | 38 | 12 | 7 | 57 (69.5) | |
| Complete remission | 16 (19.5) | ||||
| Very good partial response | 41 (50) | ||||
| Insufficiently controlled disease | 14 | 2 | 0 | 16 (19.5) | |
| Partial remission | 7 (8.5) | ||||
| Stable disease | 3 (3.7) | ||||
| Progressive disease | 6 (7.3) | ||||
| Not assessable * | 9 (10.9) | ||||
| TOTAL § | 57 | 17 | 8 | 82 |
| Variable | Total |
|---|---|
| Type of anti-SARS-CoV-2 vaccine, n (%) | |
| mRNA-based vaccine | 63 (76.8) |
| Vector-based vaccine | 19 (23.2) |
| Time between first vaccination and Anti-SARS-CoV-2 spike protein titer measurement, days (mean, ± SD) | 25.2 (±11.8) |
| Distribution of lymphocytes detected by flow cytometry | |
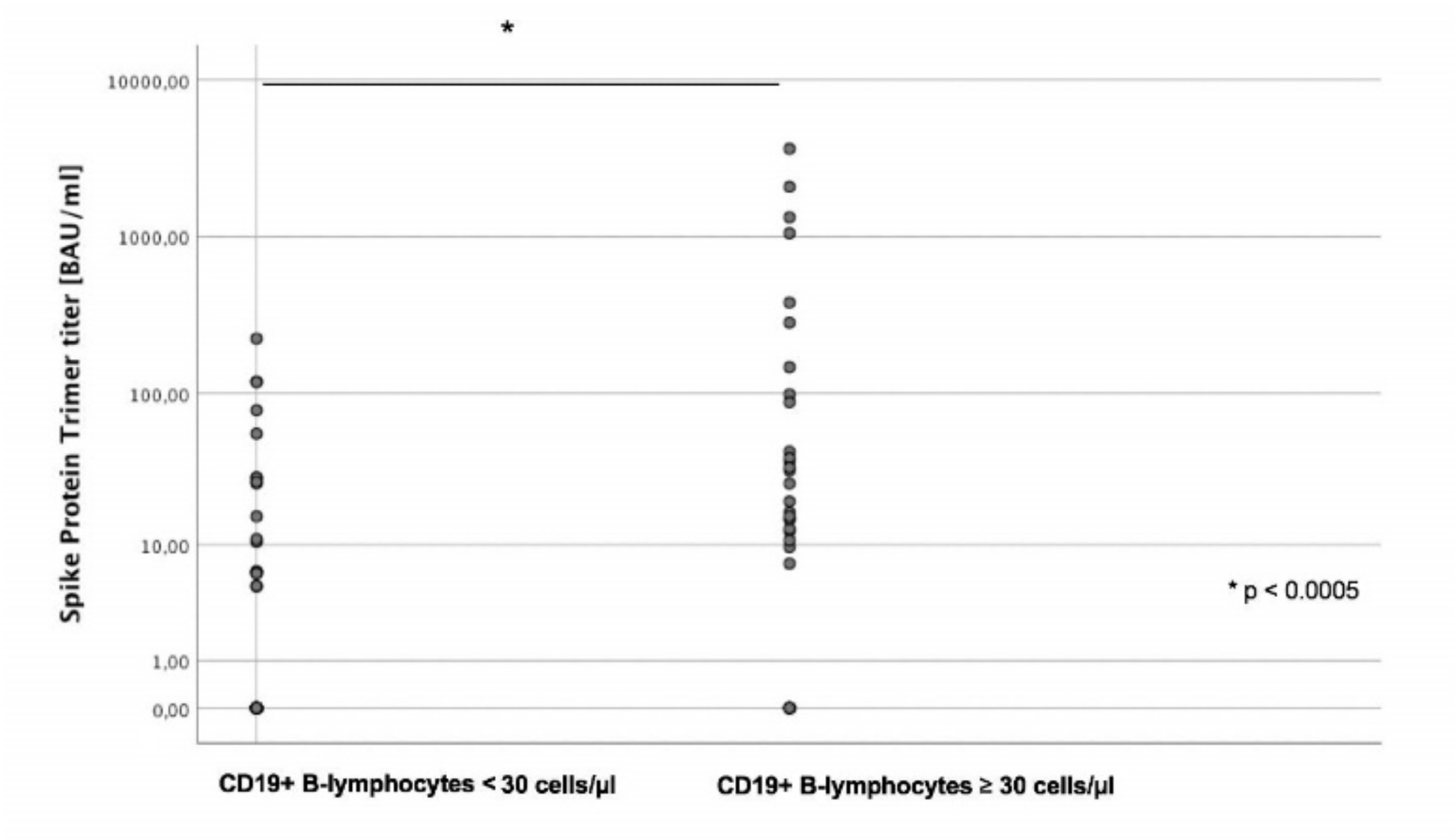
| Mean CD19+ cells/µL (range) | 88.5 (1–642) |
| Mean CD4+ cells/µL (range) | 442.7 (39–1730) |
| Mean CD8+ cells/µL (range) | 553.4 (27–2261) |
| Variables | All Observations | Observations with Positive Antibody Titer | ||
|---|---|---|---|---|
| Estimate | p-Value | |||
| Intercept | 2.86 | 0.088 | 4.58 | 0.068 |
| Log (CD19 count) L | 0.43 | 0.001 | 0.39 | 0.008 |
| Time since first vaccination (days) | 0.049 | 0.008 | 0.022 | 0.21 |
| Age at vaccination (years) | −0.047 | 0.027 | −0.045 | 0.03 |
| Insufficiently controlled disease | −1.18 | 0.024 | −0.50 | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghandili, S.; Schönlein, M.; Lütgehetmann, M.; Schulze zur Wiesch, J.; Becher, H.; Bokemeyer, C.; Sinn, M.; Weisel, K.C.; Leypoldt, L.B. Post-Vaccination Anti-SARS-CoV-2-Antibody Response in Patients with Multiple Myeloma Correlates with Low CD19+ B-Lymphocyte Count and Anti-CD38 Treatment. Cancers 2021, 13, 3800. https://doi.org/10.3390/cancers13153800
Ghandili S, Schönlein M, Lütgehetmann M, Schulze zur Wiesch J, Becher H, Bokemeyer C, Sinn M, Weisel KC, Leypoldt LB. Post-Vaccination Anti-SARS-CoV-2-Antibody Response in Patients with Multiple Myeloma Correlates with Low CD19+ B-Lymphocyte Count and Anti-CD38 Treatment. Cancers. 2021; 13(15):3800. https://doi.org/10.3390/cancers13153800
Chicago/Turabian StyleGhandili, Susanne, Martin Schönlein, Marc Lütgehetmann, Julian Schulze zur Wiesch, Heiko Becher, Carsten Bokemeyer, Marianne Sinn, Katja C. Weisel, and Lisa B. Leypoldt. 2021. "Post-Vaccination Anti-SARS-CoV-2-Antibody Response in Patients with Multiple Myeloma Correlates with Low CD19+ B-Lymphocyte Count and Anti-CD38 Treatment" Cancers 13, no. 15: 3800. https://doi.org/10.3390/cancers13153800
APA StyleGhandili, S., Schönlein, M., Lütgehetmann, M., Schulze zur Wiesch, J., Becher, H., Bokemeyer, C., Sinn, M., Weisel, K. C., & Leypoldt, L. B. (2021). Post-Vaccination Anti-SARS-CoV-2-Antibody Response in Patients with Multiple Myeloma Correlates with Low CD19+ B-Lymphocyte Count and Anti-CD38 Treatment. Cancers, 13(15), 3800. https://doi.org/10.3390/cancers13153800