
Site-Specific Variation in Radiomic Features of Head and Neck Squamous Cell Carcinoma and Its Impact on Machine Learning Models

 , , ,
, , ,  ,
, 

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients & Inclusion Criteria
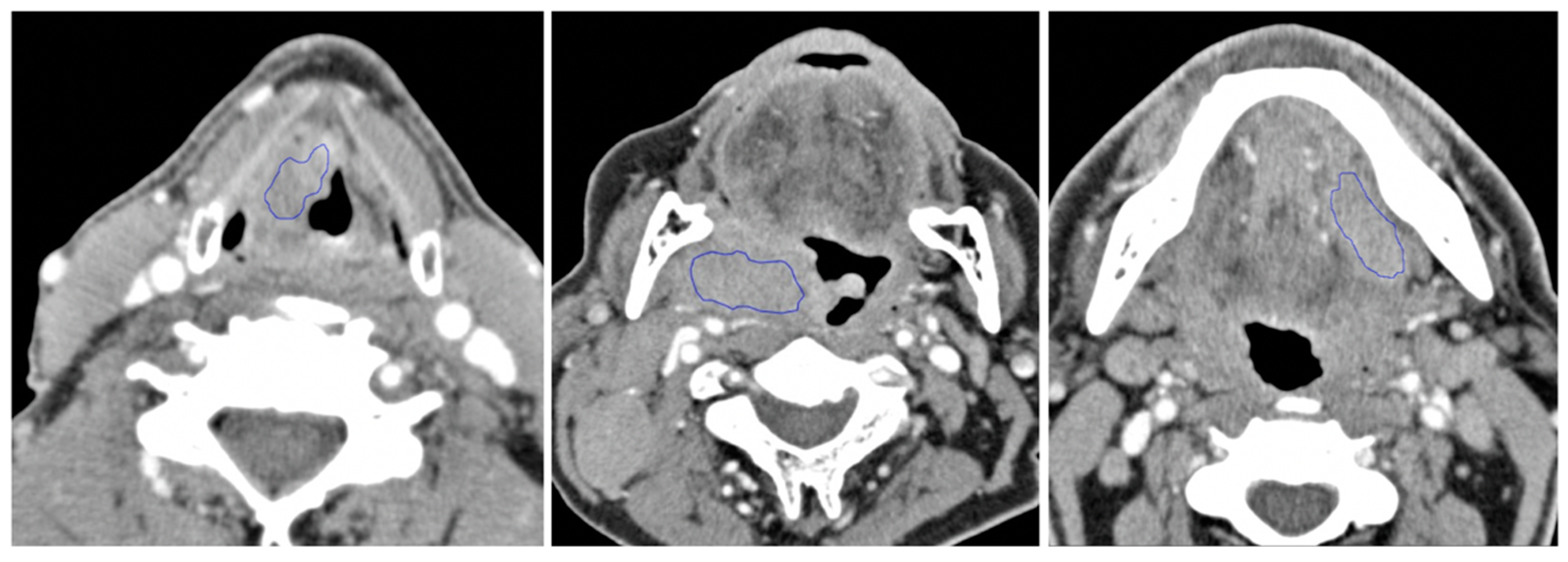
2.2. Image Acquisition
2.3. Statistical Analyses
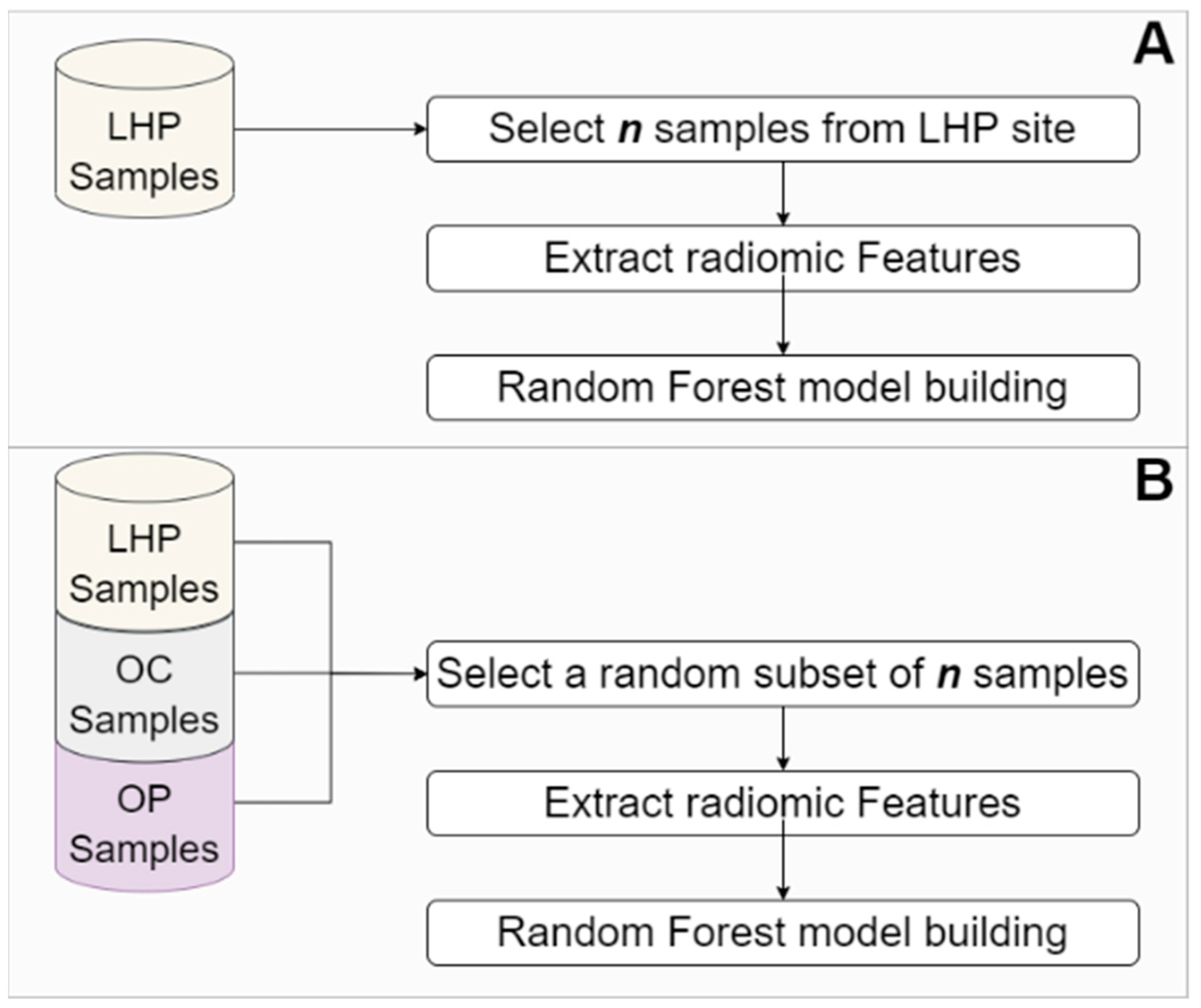
2.4. Predictive Modeling of Different Outcomes Using Machine Learning
3. Results
3.1. Association between Tumor Site and Lymph Node Metastasis and HPV Status
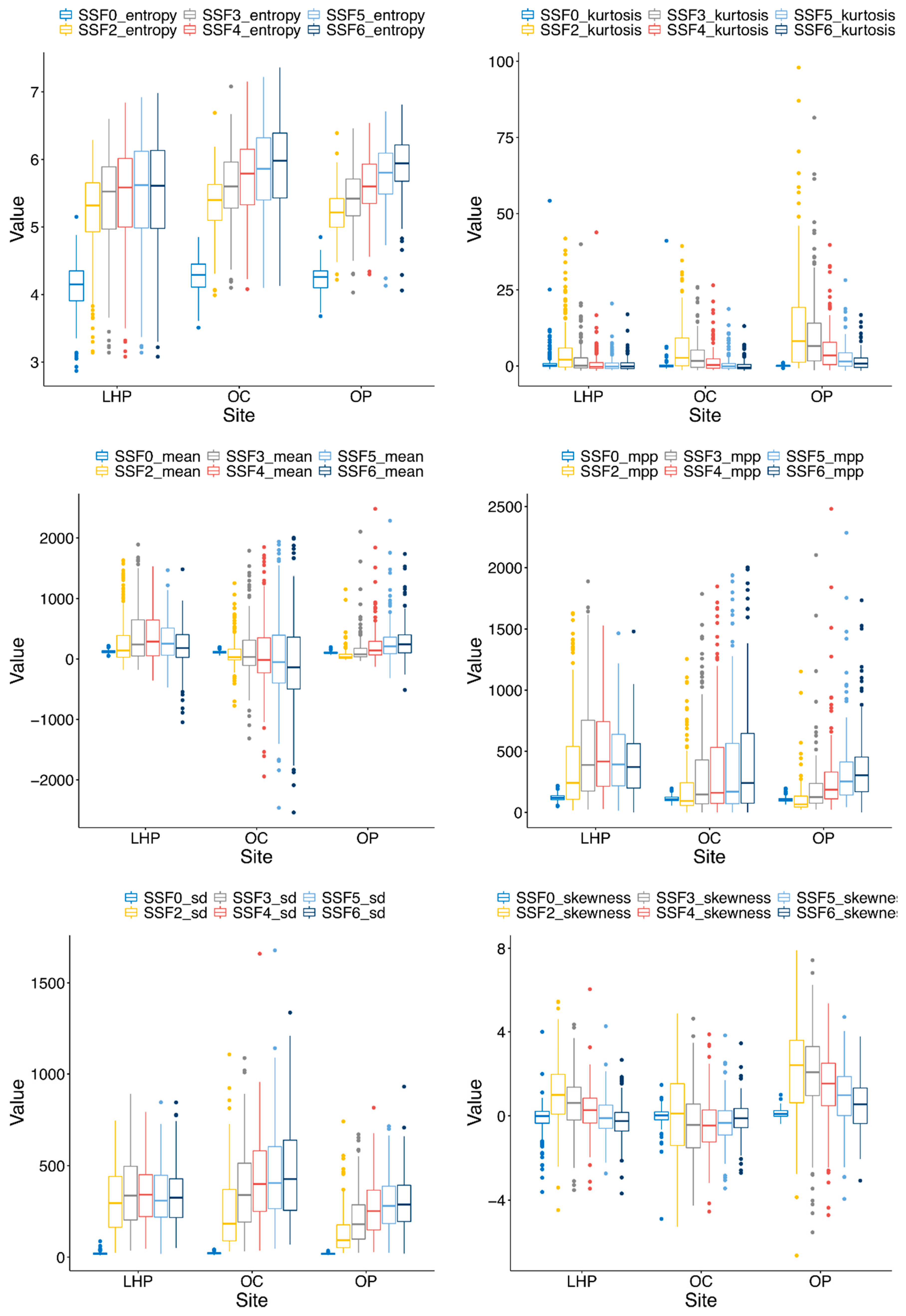
3.2. Site-Specific Variation and Differences in Radiomic Features between Different Tumor Anatomic Sites
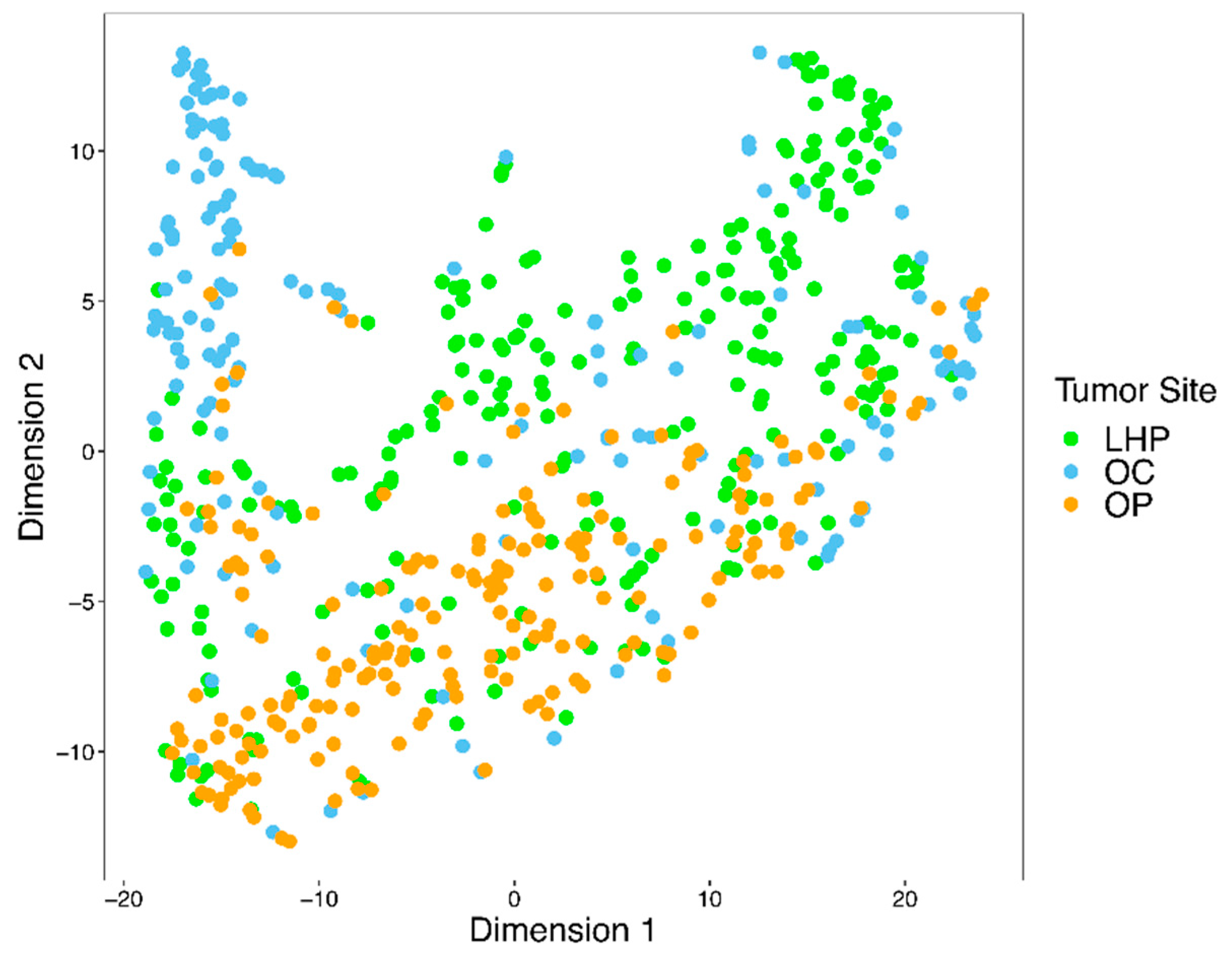
3.3. Radiomic Features Can Capture Tumor Site-Specific Information
3.4. Stratification According to Primary Tumor Site Affects Prediction Performance of Lymph Node Metastasis and HPV Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Adjusted p-Value |
|---|---|
| SSF0_entropy | 1.36 × 10−6 |
| SSF0_kurtosis | 4.02 × 10−2 |
| SSF0_mean | 7.99 × 10−11 |
| SSF0_mpp | 2.92 × 10−11 |
| SSF0_sd | 1.06 × 10−3 |
| SSF0_skewness | 1.97 × 10−4 |
| SSF2_entropy | 2.52 × 10−1 |
| SSF2_kurtosis | 3.01 × 10−14 |
| SSF2_mean | 2.64 × 10−14 |
| SSF2_mpp | 2.55 × 10−21 |
| SSF2_sd | 2.04 × 10−23 |
| SSF2_skewness | 9.41 × 10−23 |
| SSF3_entropy | 5.65 × 10−2 |
| SSF3_kurtosis | 2.57 × 10−23 |
| SSF3_mean | 8.38 × 10−12 |
| SSF3_mpp | 5.76 × 10−18 |
| SSF3_sd | 3.65 × 10−16 |
| SSF3_skewness | 6.04 × 10−33 |
| SSF4_entropy | 1.97 × 10−3 |
| SSF4_kurtosis | 6.90 × 10−19 |
| SSF4_mean | 4.38 × 10−9 |
| SSF4_mpp | 5.65 × 10−9 |
| SSF4_sd | 3.10 × 10−13 |
| SSF4_skewness | 1.30 × 10−29 |
| SSF5_entropy | 3.28 × 10−6 |
| SSF5_kurtosis | 9.52 × 10−13 |
| SSF5_mean | 1.08 × 10−08 |
| SSF5_mpp | 9.34 × 10−02 |
| SSF5_sd | 1.07 × 10−13 |
| SSF5_skewness | 8.98 × 10−23 |
| SSF6_entropy | 1.01 × 10−9 |
| SSF6_kurtosis | 1.17 × 10−6 |
| SSF6_mean | 9.33 × 10−10 |
| SSF6_mpp | 1.00 |
| SSF6_sd | 4.04 × 10−14 |
| SSF6_skewness | 1.15 × 10−12 |
Appendix B
References
- Belcher, R.; Hayes, K.; Fedewa, S.; Chen, A.Y. Current treatment of head and neck squamous cell cancer. J. Surg. Oncol. 2014, 110, 551–574. [Google Scholar] [CrossRef]
- Guha, A.; Connor, S.; Anjari, M.; Naik, H.; Siddiqui, M.; Cook, G.; Goh, V. Radiomic analysis for response assessment in advanced head and neck cancers, a distant dream or an inevitable reality? A systematic review of the current level of evidence. Br. J. Radiol. 2020, 93, 20190496. [Google Scholar] [CrossRef]
- Huang, C.; Cintra, M.B.; Brennan, K.; Zhou, M.; Colevas, A.D.; Fischbein, N.; Zhu, S.; Gevaert, O. Development and validation of radiomic signatures of head and neck squamous cell carcinoma molecular features and subtypes. EBioMedicine 2019, 45, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Deschler, D.G.; Day, T. TNM Staging of Head and Neck Cancer and Neck Dissection Classification; American Academy of Otolaryngology–Head and Neck Surgery Foundation: Alexandria, VA, USA, 2008; pp. 10–23. [Google Scholar]
- Lassen, P.; Eriksen, J.G.; Hamilton-Dutoit, S.; Tramm, T.; Alsner, J.; Overgaard, J. Effect of HPV-associated p16INK4A expression on response to radiotherapy and survival in squamous cell carcinoma of the head and neck. J. Clin. Oncol. 2009, 27, 1992–1998. [Google Scholar] [CrossRef] [Green Version]
- Leemans, C.R.; Snijders, P.J.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat. Rev. Cancer 2018, 18, 269. [Google Scholar] [CrossRef]
- Pezzuto, F.; Buonaguro, L.; Caponigro, F.; Ionna, F.; Starita, N.; Annunziata, C.; Buonaguro, F.M.; Tornesello, M.L. Update on head and neck cancer: Current knowledge on epidemiology, risk factors, molecular features and novel therapies. Oncology 2015, 89, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Maleki, F.; Le, W.T.; Sananmuang, T.; Kadoury, S.; Forghani, R. Machine Learning Applications for Head and Neck Imaging. Neuroimaging Clin. N. Am. 2020, 30, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Diamant, A.; Chatterjee, A.; Vallières, M.; Shenouda, G.; Seuntjens, J. Deep learning in head & neck cancer outcome prediction. Sci. Rep. 2019, 9, 1–10. [Google Scholar]
- Leijenaar, R.T.; Bogowicz, M.; Jochems, A.; Hoebers, F.J.; Wesseling, F.W.; Huang, S.H.; Chan, B.; Waldron, J.N.; O’Sullivan, B.; Rietveld, D.; et al. Development and validation of a radiomic signature to predict HPV (p16) status from standard CT imaging: A multicenter study. Br. J. Radiol. 2018, 91, 20170498. [Google Scholar] [CrossRef]
- Head, M.A.C.C.; Neck Quantitative Imaging Working Group. Investigation of radiomic signatures for local recurrence using primary tumor texture analysis in oropharyngeal head and neck cancer patients. Sci. Rep. 2018, 8, 1524. [Google Scholar]
- Ger, R.B.; Zhou, S.; Elgohari, B.; Elhalawani, H.; Mackin, D.M.; Meier, J.; Nguyen, C.M.; Anderson, B.M.; Gay, C.; Ning, J.; et al. Radiomics features of the primary tumor fail to improve prediction of overall survival in large cohorts of CT- and PET-imaged head and neck cancer patients. PLoS ONE 2019, 14, e0222509. [Google Scholar] [CrossRef]
- Wu, W.; Ye, J.; Wang, Q.; Luo, J.; Xu, S. CT-based radiomics signature for the preoperative discrimination between head and neck squamous cell carcinoma grades. Front. Oncol. 2019, 9, 821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, T.-T.; Langendijk, J.A.; van Dijk, L.V.; Halmos, G.B.; Witjes, M.J.; Oosting, S.F.; Noordzij, W.; Sijtsema, N.M.; Steenbakkers, R.J. The prognostic value of CT-based image-biomarkers for head and neck cancer patients treated with definitive (chemo-)radiation. Oral Oncol. 2019, 95, 178–186. [Google Scholar] [CrossRef]
- Cozzi, L.; Franzese, C.; Fogliata, A.; Franceschini, D.; Navarria, P.; Tomatis, S.; Scorsetti, M. Predicting survival and local control after radiochemotherapy in locally advanced head and neck cancer by means of computed tomography based radiomics. Strahlenther. Onkol. 2019, 195, 805–818. [Google Scholar] [CrossRef] [PubMed]
- Giraud, P.; Giraud, P.; Gasnier, A.; El Ayachy, R.; Kreps, S.; Foy, J.P.; Durdux, C.; Huguet, F.; Burgun, A.; Bibault, J.E. Radiomics and machine learning for radiotherapy in head and neck cancers. Front. Oncol. 2019, 9, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo, X.; Wu, X.; Dong, D.; Guo, B.; Liang, C.; Luo, X.; Zhang, B.; Zhang, L.; Dong, Y.; Lian, Z.; et al. Prognostic value of the radiomics-based model in progression-free survival of hypopharyngeal cancer treated with chemoradiation. Eur. Radiol. 2020, 30, 833–843. [Google Scholar] [CrossRef]
- Ou, D.; Blanchard, P.; Rosellini, S.; Levy, A.; Nguyen, F.; Leijenaar, R.T.; Garberis, I.; Gorphe, P.; Bidault, F.; Ferté, C.; et al. Predictive and prognostic value of CT based radiomics signature in locally advanced head and neck cancers patients treated with concurrent chemoradiotherapy or bioradiotherapy and its added value to Human Papillomavirus status. Oral Oncol. 2017, 71, 150–155. [Google Scholar] [CrossRef]
- Bahig, H.; Lapointe, A.; Bedwani, S.; De Guise, J.; Lambert, L.; Filion, E.; Roberge, D.; Letourneau-Guillon, L.; Blais, D.; Ng, S.P.; et al. Dual-energy computed tomography for prediction of loco-regional recurrence after radiotherapy in larynx and hypopharynx squamous cell carcinoma. Eur. J. Radiol. 2019, 110, 1–6. [Google Scholar] [CrossRef]
- Forghani, R.; Chatterjee, A.; Reinhold, C.; Lara, A.E.P.; Romero-Sanchez, G.; Ueno, Y.; Bayat, M.; Alexander, J.W.M.; Kadi, L.; Chankowsky, J.; et al. Head and neck squamous cell carcinoma: Prediction of cervical lymph node metastasis by dual-energy CT texture analysis with machine learning. Eur. Radiol. 2019, 29, 6172–6181. [Google Scholar] [CrossRef]
- Chen, L.; Zhou, Z.; Sher, D.; Zhang, Q.; Shah, J.; Pham, N.-L.; Jiang, S.; Wang, J. Combining many-objective radiomics and 3D convolutional neural network through evidential reasoning to predict lymph node metastasis in head and neck cancer. Phys. Med. Biol. 2019, 64, 075011. [Google Scholar] [CrossRef]
- Park, B.W.; Kim, J.K.; Heo, C.; Park, K.J. Reliability of CT radiomic features reflecting tumour heterogeneity according to image quality and image processing parameters. Sci. Rep. 2020, 10, 3852. [Google Scholar] [CrossRef]
- Sanchez, L.E.; Rundo, L.; Gill, A.B.; Hoare, M.; Serrao, E.M.; Sala, E. Robustness of radiomic features in CT images with different slice thickness, comparing liver tumour and muscle. Sci. Rep. 2021, 11, 1–15. [Google Scholar]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and Reproducibility of Radiomic Features: A Systematic Review. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1143–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, B. Understanding Sources of Variation to Improve the Reproducibility of Radiomics. Front. Oncol. 2021, 11, 826. [Google Scholar]
- Ueno, Y.; Forghani, B.; Forghani, R.; Dohan, A.; Zeng, X.Z.; Chamming’S, F.; Arseneau, J.; Fu, L.; Gilbert, L.; Gallix, B.; et al. Endometrial Carcinoma: MR Imaging–based Texture Model for Preoperative Risk Stratification—A Preliminary Analysis. Radiol. 2017, 284, 748–757. [Google Scholar] [CrossRef] [Green Version]
- Bretz, F.; Hothorn, T.; Westfall, P. Multiple Comparisons Using R; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Ho, T.Y.; Chao, C.H.; Chin, S.C.; Ng, S.H.; Kang, C.J.; Tsang, N.M. Classifying Neck Lymph Nodes of Head and Neck Squamous Cell Carcinoma in MRI Images with Radiomic Features. J. Digit. Imaging 2020, 33, 613–618. [Google Scholar] [CrossRef]
- Maleki, F.; Muthukrishnan, N.; Ovens, K.; Reinhold, C.; Forghani, R. Machine Learning Algorithm Validation: From Essentials to Advanced Applications and Implications for Regulatory Certification and Deployment. Neuroimaging Clin. N. Am. 2020, 30, 433–445. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Feliciani, G.; Fioroni, F.; Grassi, E.; Bertolini, M.; Rosca, A.; Timon, G.; Galaverni, M.; Iotti, C.; Versari, A.; Iori, M.; et al. Radiomic Profiling of Head and Neck Cancer: 18F-FDG PET Texture Analysis as Predictor of Patient Survival. Contrast Media Mol. Imaging 2018, 2018, 3574310. [Google Scholar] [CrossRef] [Green Version]
- Shur, J.; Orton, M.; Connor, A.; Fischer, S.; Moulton, C.; Gallinger, S.; Koh, D.; Jhaveri, K.S. A clinical-radiomic model for improved prognostication of surgical candidates with colorectal liver metastases. J. Surg. Oncol. 2019, 121, 357–364. [Google Scholar] [CrossRef] [PubMed]




| OC | OP | LHP | Total | |
|---|---|---|---|---|
| Number of cases | 164 | 200 | 241 | 605 |
| Age | 64 (24–90) | 61 (33–87) | 65 (27–88) | 64 (24–90) |
| Sex (Male:Female) | 111:53 | 161:39 | 201:40 | 473:132 |
| LN (+/−) | 93:70 | 175:25 | 78:163 | 346:258 |
| HPV (+/−) | 0:9 | 134:63 | 11:55 | 145:127 |
| Sites | Nonmetastatic | Metastatic |
|---|---|---|
| LHP | 0.676 | 0.324 |
| OC | 0.429 | 0.571 |
| OP | 0.125 | 0.875 |
| Sites | Negative | Positive |
|---|---|---|
| LHP | 0.833 | 0.167 |
| OC | 1.00 | 0.00 |
| OP | 0.320 | 0.680 |
| Endpoint-Site | Statistics | Accuracy | Precision | Recall | F1 | AUC |
|---|---|---|---|---|---|---|
| LN-LHP (N = 241) | statistic | 8.34 | 12.22 | 10.17 | 12.09 | 9.71 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| LN-OC (N = 163) | statistic | 11.54 | 9.96 | 7.13 | 8.40 | 11.97 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| HPV-OP (N = 197) | statistic | 11.12 | 0.32 | 7.73 | 4.06 | 11.67 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Maleki, F.; Muthukrishnan, N.; Ovens, K.; Huang, S.H.; Pérez-Lara, A.; Romero-Sanchez, G.; Bhatnagar, S.R.; Chatterjee, A.; Pusztaszeri, M.P.; et al. Site-Specific Variation in Radiomic Features of Head and Neck Squamous Cell Carcinoma and Its Impact on Machine Learning Models. Cancers 2021, 13, 3723. https://doi.org/10.3390/cancers13153723
Liu X, Maleki F, Muthukrishnan N, Ovens K, Huang SH, Pérez-Lara A, Romero-Sanchez G, Bhatnagar SR, Chatterjee A, Pusztaszeri MP, et al. Site-Specific Variation in Radiomic Features of Head and Neck Squamous Cell Carcinoma and Its Impact on Machine Learning Models. Cancers. 2021; 13(15):3723. https://doi.org/10.3390/cancers13153723
Chicago/Turabian StyleLiu, Xiaoyang, Farhad Maleki, Nikesh Muthukrishnan, Katie Ovens, Shao Hui Huang, Almudena Pérez-Lara, Griselda Romero-Sanchez, Sahir Rai Bhatnagar, Avishek Chatterjee, Marc Philippe Pusztaszeri, and et al. 2021. "Site-Specific Variation in Radiomic Features of Head and Neck Squamous Cell Carcinoma and Its Impact on Machine Learning Models" Cancers 13, no. 15: 3723. https://doi.org/10.3390/cancers13153723
APA StyleLiu, X., Maleki, F., Muthukrishnan, N., Ovens, K., Huang, S. H., Pérez-Lara, A., Romero-Sanchez, G., Bhatnagar, S. R., Chatterjee, A., Pusztaszeri, M. P., Spatz, A., Batist, G., Payabvash, S., Haider, S. P., Mahajan, A., Reinhold, C., Forghani, B., O’Sullivan, B., Yu, E., & Forghani, R. (2021). Site-Specific Variation in Radiomic Features of Head and Neck Squamous Cell Carcinoma and Its Impact on Machine Learning Models. Cancers, 13(15), 3723. https://doi.org/10.3390/cancers13153723