
Analyses of CNS Response to Osimertinib in Patients with T790M-Positive Advanced NSCLC from ASTRIS Korean Subset, Open-Label Real-World Study

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Overview
2.2. Participants
2.3. Ethical Approval
2.4. Assessments and Statistical Analyses
3. Results
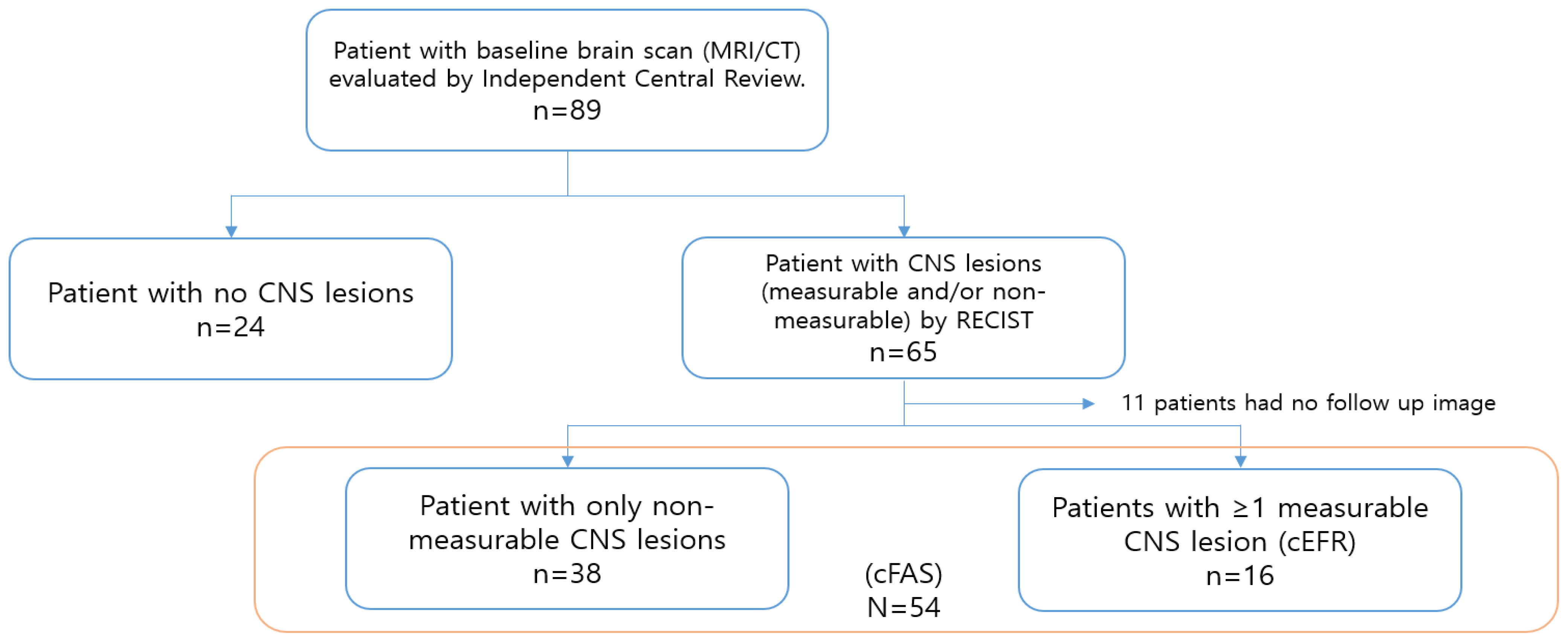
3.1. Patients
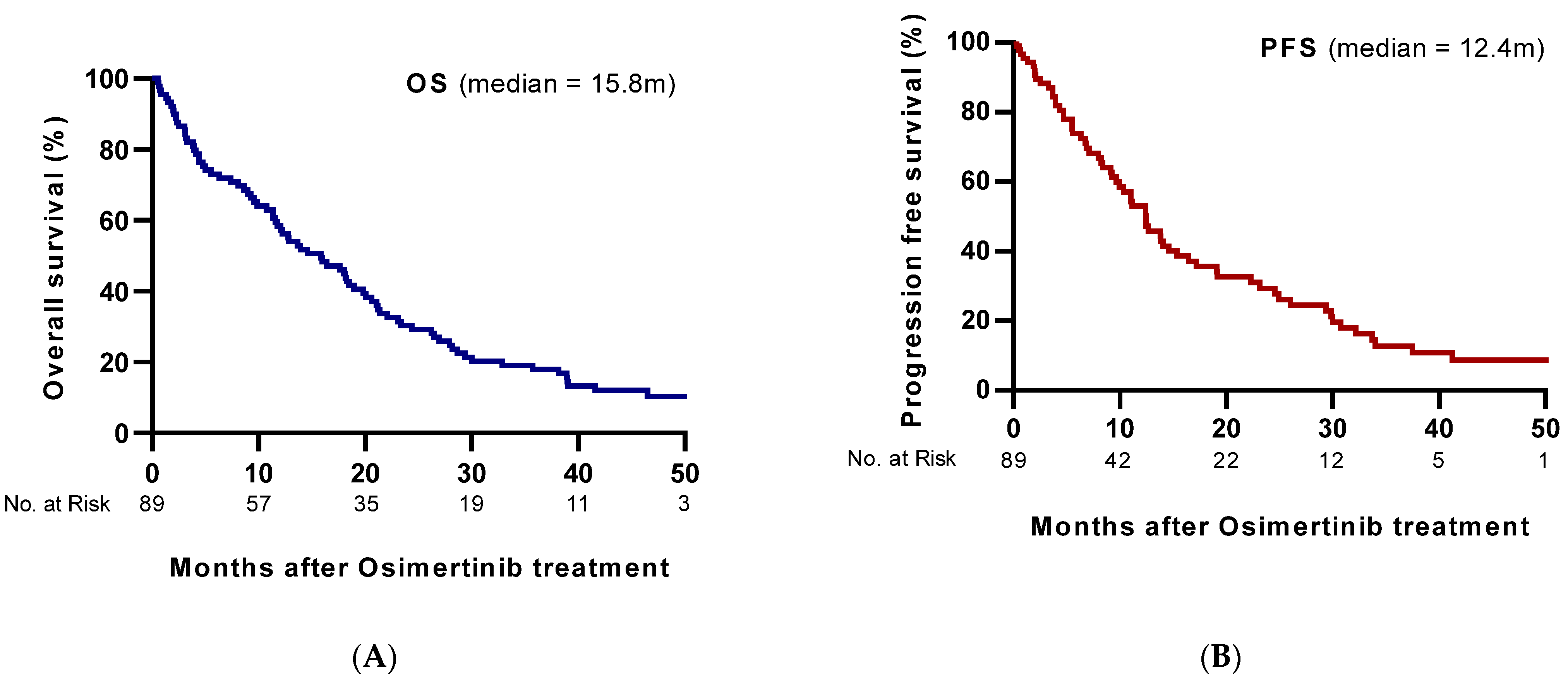
3.2. Osimertinib Efficacy
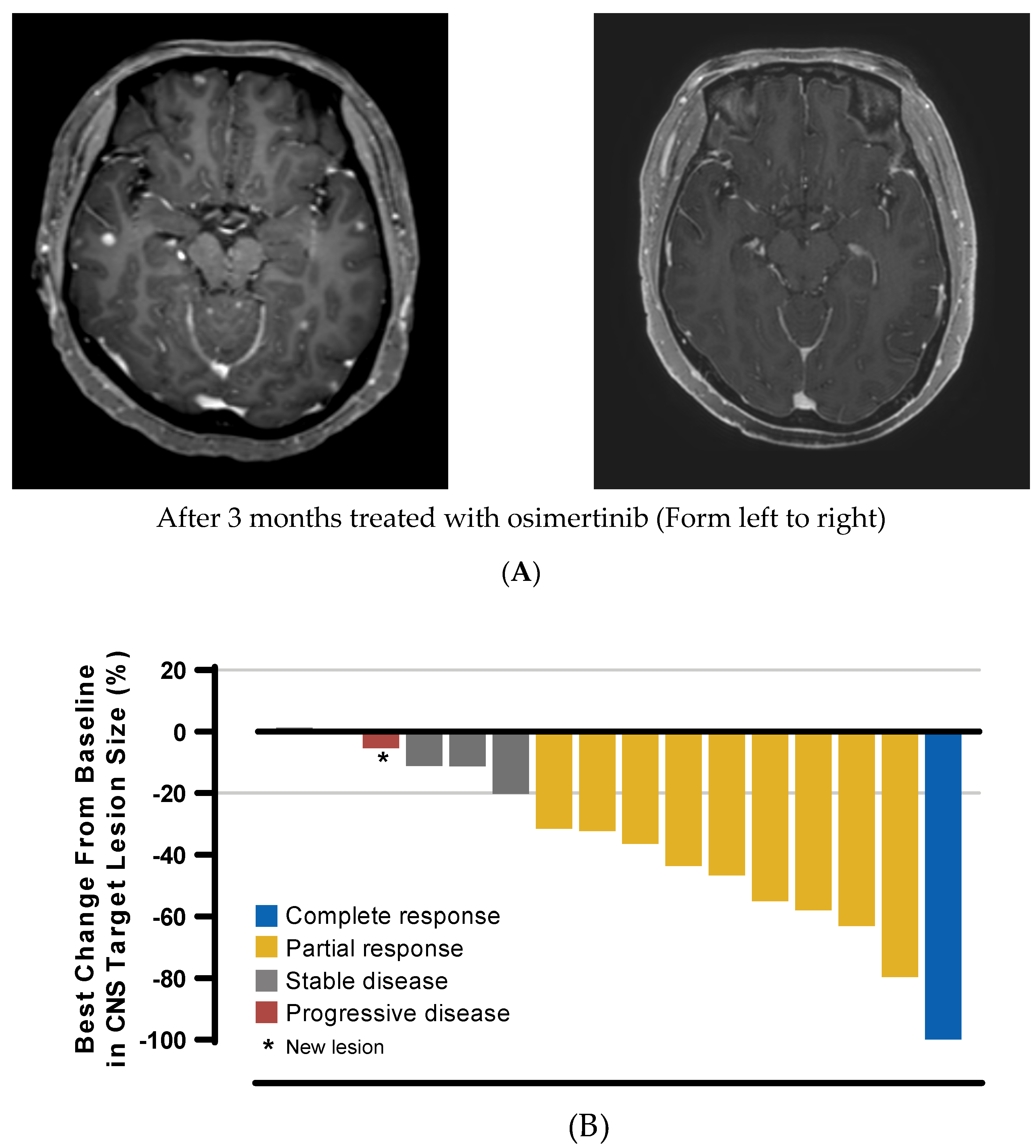
3.3. Concordance between CNS and Systemic Responses
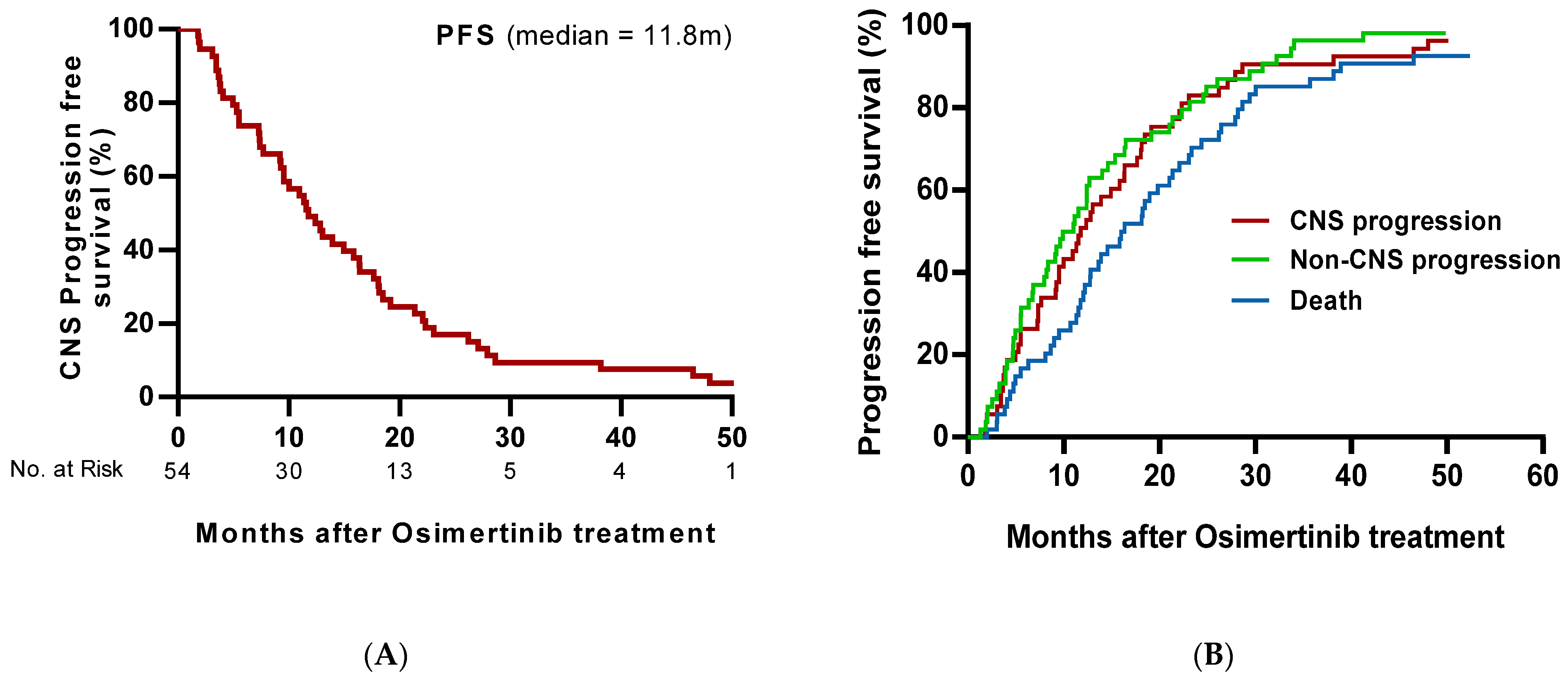
3.4. cPFS and Risk of CNS Progression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Peters, S.; Bexelius, C.; Munk, V.; Leighl, N. The impact of brain metastasis on quality of life, resource utilization and survival in patients with non-small-cell lung cancer. Cancer Treat. Rev. 2016, 45, 139–162. [Google Scholar] [CrossRef] [PubMed]
- Heon, S.; Yeap, B.Y.; Lindeman, N.I.; Joshi, V.A.; Butaney, M.; Britt, G.J.; Costa, D.B.; Rabin, M.S.; Jackman, D.M.; Johnson, B.E. The impact of initial gefitinib or erlotinib versus chemotherapy on central nervous system progression in advanced non-small cell lung cancer with EGFR mutations. Clin. Cancer Res. 2012, 18, 4406–4414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camidge, D.R.; Pao, W.; Sequist, L.V. Acquired resistance to TKIs in solid tumours: Learning from lung cancer. Nat. Rev. Clin. Oncol. 2014, 11, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Rangachari, D.; Yamaguchi, N.; VanderLaan, P.A.; Folch, E.; Mahadevan, A.; Floyd, S.R.; Uhlmann, E.J.; Wong, E.T.; Dahlberg, S.E.; Huberman, M.S.; et al. Brain metastases in patients with EGFR-mutated or ALK-rearranged non-small-cell lung cancers. Lung Cancer 2015, 88, 108–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballard, P.; Yates, J.W.; Yang, Z.; Kim, D.W.; Yang, J.C.; Cantarini, M.; Pickup, K.; Jordan, A.; Hickey, M.; Grist, M.; et al. Preclinical Comparison of Osimertinib with Other EGFR-TKIs in EGFR-Mutant NSCLC Brain Metastases Models, and Early Evidence of Clinical Brain Metastases Activity. Clin. Cancer Res. 2016, 22, 5130–5140. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Han, J.Y.; Katakami, N.; Kim, H.R.; Hodge, R.; Kaur, P.; Brown, A.P.; Ghiorghiu, D.; et al. CNS Efficacy of Osimertinib in Patients With T790M-Positive Advanced Non-Small-Cell Lung Cancer: Data from a Randomized Phase III Trial (AURA3). J. Clin. Oncol. 2018, 36, 2702–2709. [Google Scholar] [CrossRef] [PubMed]
- Reungwetwattana, T.; Nakagawa, K.; Cho, B.C.; Cobo, M.; Cho, E.K.; Bertolini, A.; Bohnet, S.; Zhou, C.; Lee, K.H.; Nogami, N.; et al. CNS Response to Osimertinib Versus Standard Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors in Patients With Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.C.; Kim, D.W.; Park, K.; Lee, J.S.; Yoo, S.S.; Kang, J.H.; Lee, S.Y.; Kim, C.H.; Jang, S.H.; Kim, Y.C.; et al. Real-world use of osimertinib in non-small cell lung cancer: ASTRIS study Korean subgroup analysis. Curr. Med. Res. Opin. 2020, 36, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Marinis, F.; Wu, Y.L.; de Castro, G., Jr.; Chang, G.C.; Chen, Y.M.; Cho, B.C.; Freitas, H.C.; Jiang, L.; Kim, S.W.; Martin, C.; et al. ASTRIS: A global real-world study of osimertinib in >3000 patients with EGFR T790M positive non-small-cell lung cancer. Future Oncol. 2019, 15, 3003–3014. [Google Scholar] [CrossRef] [PubMed]
- Goss, G.; Tsai, C.M.; Shepherd, F.A.; Ahn, M.J.; Bazhenova, L.; Crinò, L.; de Marinis, F.; Felip, E.; Morabito, A.; Hodge, R.; et al. CNS response to osimertinib in patients with T790M-positive advanced NSCLC: Pooled data from two phase II trials. Ann. Oncol. 2018, 29, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Khozin, S.; Blumenthal, G.M.; Pazdur, R. Real-world Data for Clinical Evidence Generation in Oncology. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, Y.-D.; Liao, H.; Qin, T.; Zhang, L.; Wei, W.-D.; Liang, J.-Z.; Xu, F.; Dinglin, X.-X.; Ma, S.-X.; Chen, L.-K. Blood-brain barrier permeability of gefitinib in patients with brain metastases from non-small-cell lung cancer before and during whole brain radiation therapy. Oncotarget 2015, 6, 8366–8376. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Sun, X.; Song, Y.; Zhang, Y.; Li, F.; Xu, Y.; Ma, S.; Lin, N. Whole-brain radiation fails to boost intracerebral gefitinib concentration in patients with brain metastatic non-small cell lung cancer: A self-controlled, pilot study. Cancer Chemother. Pharmacol. 2015, 76, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Grossman, S.A.; Krabak, M.J. Leptomeningeal carcinomatosis. Cancer Treat. Rev. 1999, 25, 103–119. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, M.; Soffietti, R.; Raizer, J.; Ruda, R.; Brandsma, D.; Boogerd, W.; Taillibert, S.; Groves, M.D.; Le Rhun, E.; Junck, L.; et al. Leptomeningeal metastasis: A Response Assessment in Neuro-Oncology critical review of endpoints and response criteria of published randomized clinical trials. Neuro Oncol 2014, 16, 1176–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.C.H.; Kim, S.-W.; Kim, D.-W.; Lee, J.-S.; Cho, B.C.; Ahn, J.-S.; Lee, D.H.; Kim, T.M.; Goldman, J.W.; Natale, R.B.; et al. Osimertinib in Patients With Epidermal Growth Factor Receptor Mutation–Positive Non–Small-Cell Lung Cancer and Leptomeningeal Metastases: The BLOOM Study. J. Clin. Oncol. 2020, 38, 538–547. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Age | (years) |
| Median (range) | 60 (31–85) |
| Sex | n (%) |
| Male | 27 (30.3) |
| Female | 62 (69.7) |
| Histology | |
| Adenocarcinoma | 89 (100) |
| EGFR mutation | |
| T790M | 89 (100) |
| E19del | 39 (43.8) |
| L858R | 49 (55.1) |
| G719X | 1 (1.1) |
| ECOG PS score | |
| 0 | 36 (40.4) |
| 1 | 41 (46.1) |
| 2 | 21 (13.5) |
| Prior brain therapy | |
| Yes | 38 (42.7) |
| No | 27 (30.3) |
| No brain lesion | 24 (27.0) |
| Baseline brain lesion * | |
| No metastasis | 24 (27.0) |
| Brain metastasis only | 46 (51.7) |
| Brain metastasis with LM | 19 (21.3) |
| Analysis Set/Response | cFAS (N = 54) n (%)(95% CI) | cEFR (N = 16) n (%) (95% CI) |
|---|---|---|
| CNS ORR, n (%) (95% CI) | 21 (38.9) (26.7–52.2) | 10 (62.5) (38.3–82.6) |
| Complete response (CR) | 11 (20.4) | 0 (0) |
| Partial response (PR) | 10 (18.5) | 10 (62.5) |
| Stable disease (SD) | 5 (9.3) | 5 (31.3) |
| Progressive disease | 2 (3.7) | 1 (6.2) |
| non-CR, non-PD † | 26 (48.1) | - |
| CNS DCR n (%) (95% CI) | 52 (96.3) (88.6–99.2) | 15 (93.8) (74.3–99.3) |
| CNS DoR § | ||
| Median, months (95% CI) | 12.1 (8.5–15.8) | 7.6 (NC–17.8) |
| Time to onset of response | ||
| Median, weeks (interquartile range) | 8.6 (7.7–26.0) | 7.7 (7.0–8.6) |
| ≤9 weeks, No. (%) | 12 (57.1) | 8 (80.0) |
| Treatment | Patients with a Response * n (%) (95% CI) | p |
|---|---|---|
| Prior radiotherapy before randomization (n = 30) ** | 8 (26.7) (13.5–44.1) | 0.039 |
| No prior radiotherapy before randomization (n = 24) | 13 (54.2) (34.7–72.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, B.-C.; Kim, J.H.; Pyo, K.-H.; Lim, S.M.; Hong, M.H.; Kim, H.R.; Cho, B.C. Analyses of CNS Response to Osimertinib in Patients with T790M-Positive Advanced NSCLC from ASTRIS Korean Subset, Open-Label Real-World Study. Cancers 2021, 13, 3681. https://doi.org/10.3390/cancers13153681
Ahn B-C, Kim JH, Pyo K-H, Lim SM, Hong MH, Kim HR, Cho BC. Analyses of CNS Response to Osimertinib in Patients with T790M-Positive Advanced NSCLC from ASTRIS Korean Subset, Open-Label Real-World Study. Cancers. 2021; 13(15):3681. https://doi.org/10.3390/cancers13153681
Chicago/Turabian StyleAhn, Beung-Chul, Jee Hung Kim, Kyoung-Ho Pyo, Sun Min Lim, Min Hee Hong, Hye Ryun Kim, and Byoung Chul Cho. 2021. "Analyses of CNS Response to Osimertinib in Patients with T790M-Positive Advanced NSCLC from ASTRIS Korean Subset, Open-Label Real-World Study" Cancers 13, no. 15: 3681. https://doi.org/10.3390/cancers13153681
APA StyleAhn, B.-C., Kim, J. H., Pyo, K.-H., Lim, S. M., Hong, M. H., Kim, H. R., & Cho, B. C. (2021). Analyses of CNS Response to Osimertinib in Patients with T790M-Positive Advanced NSCLC from ASTRIS Korean Subset, Open-Label Real-World Study. Cancers, 13(15), 3681. https://doi.org/10.3390/cancers13153681