
Drug Holidays and Overall Survival of Patients with Metastatic Colorectal Cancer

 ,
,  , ,
, ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Descriptive Analysis
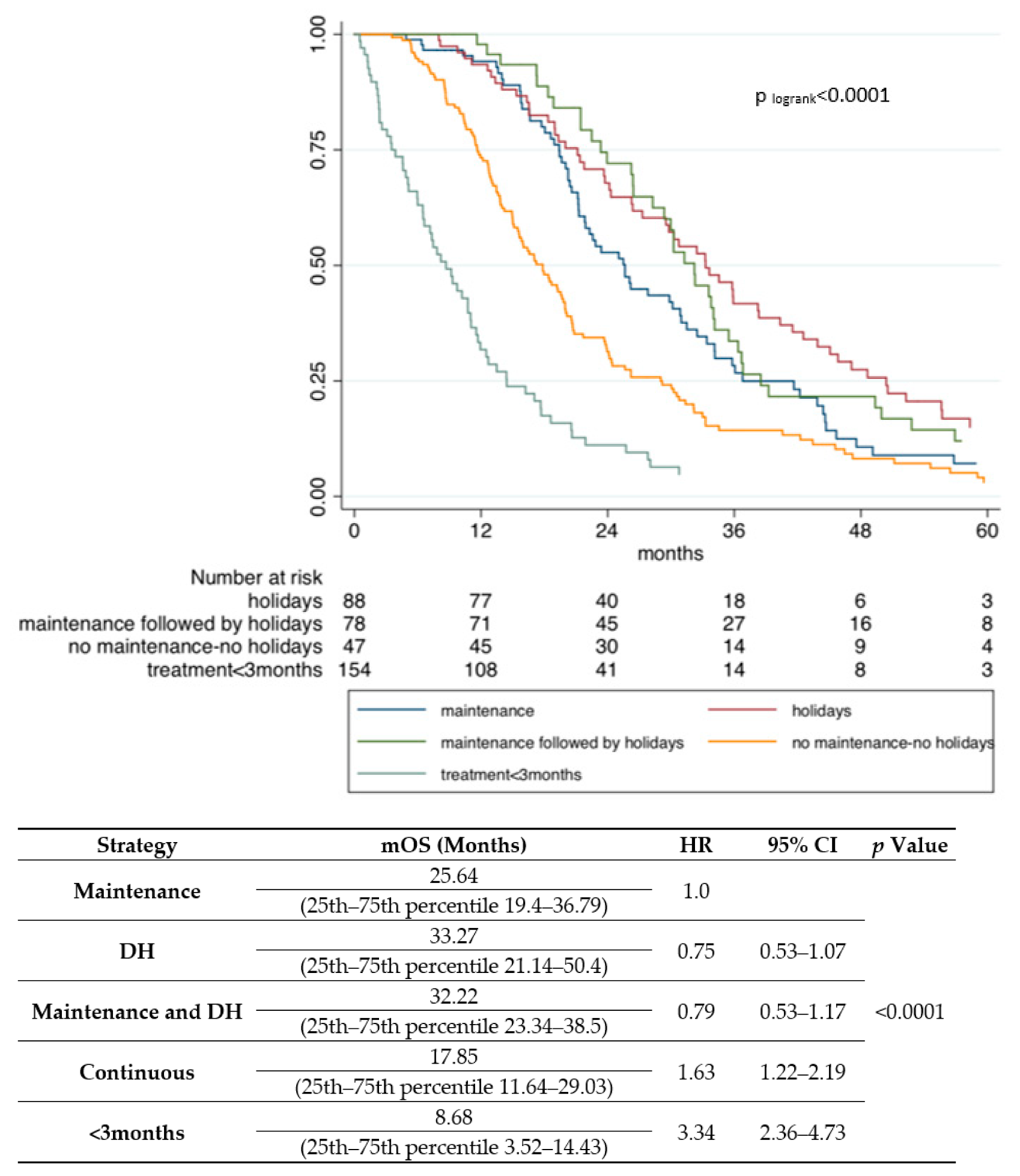
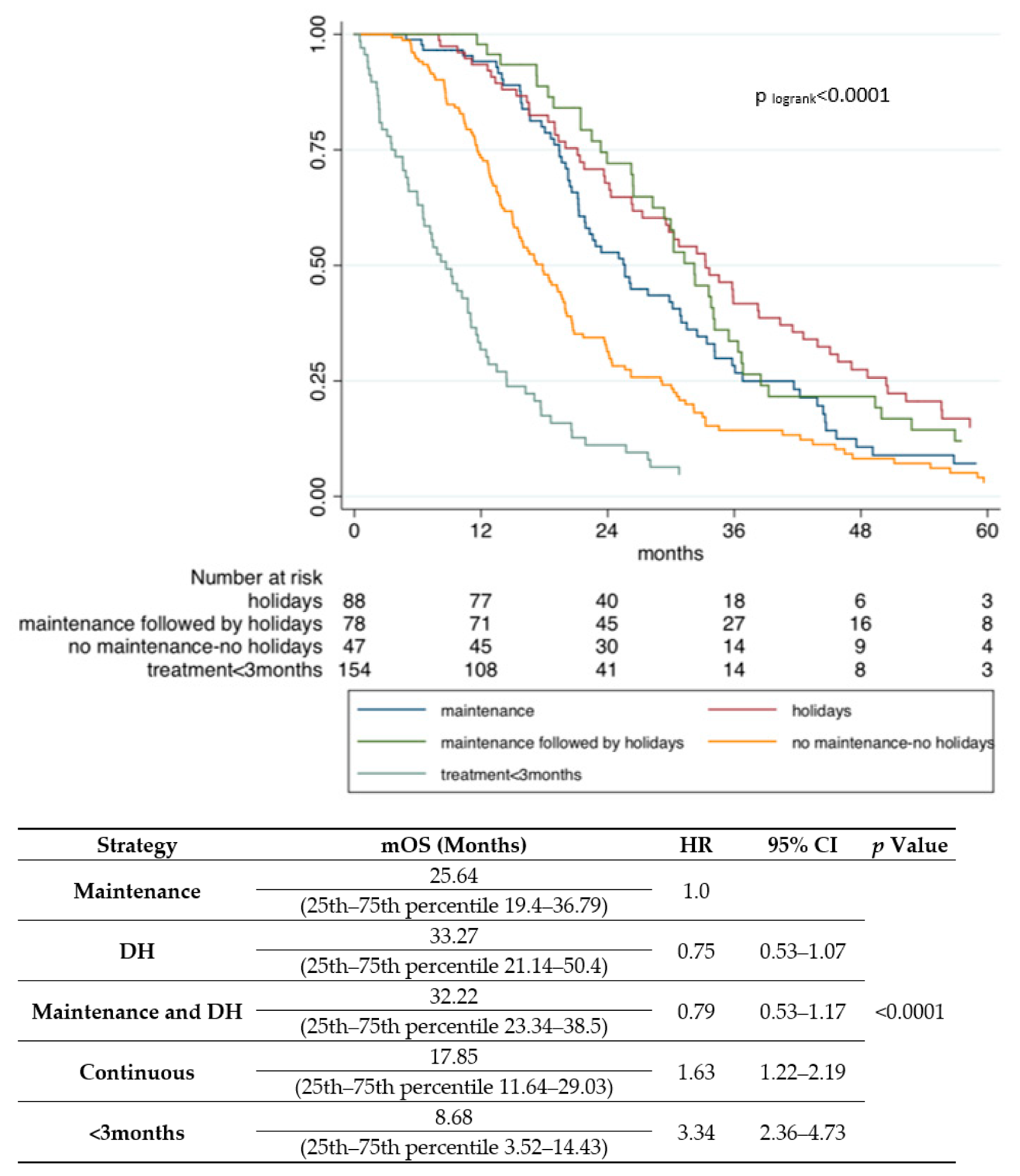
2.2. Survival Impact of De-Escalation Strategies
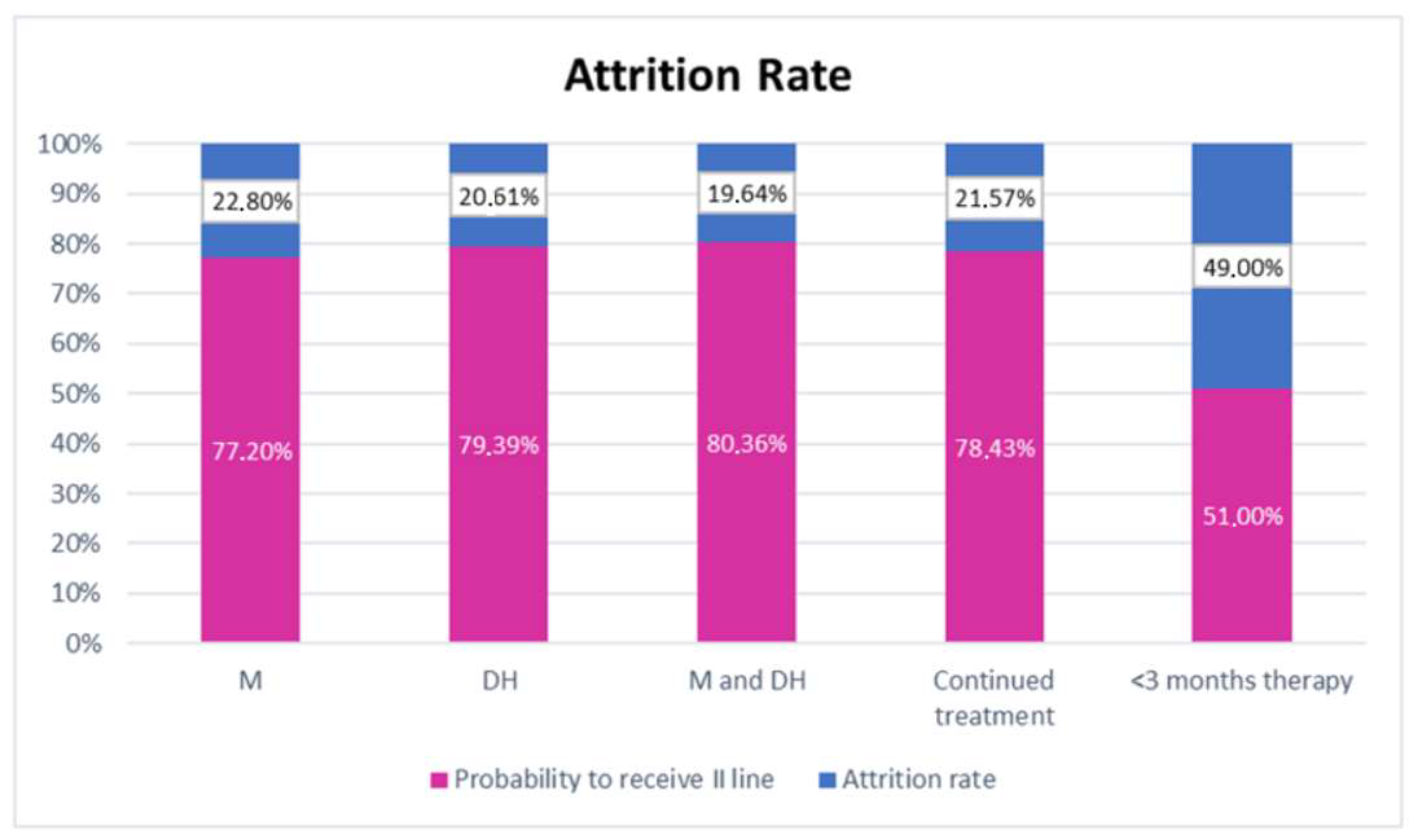
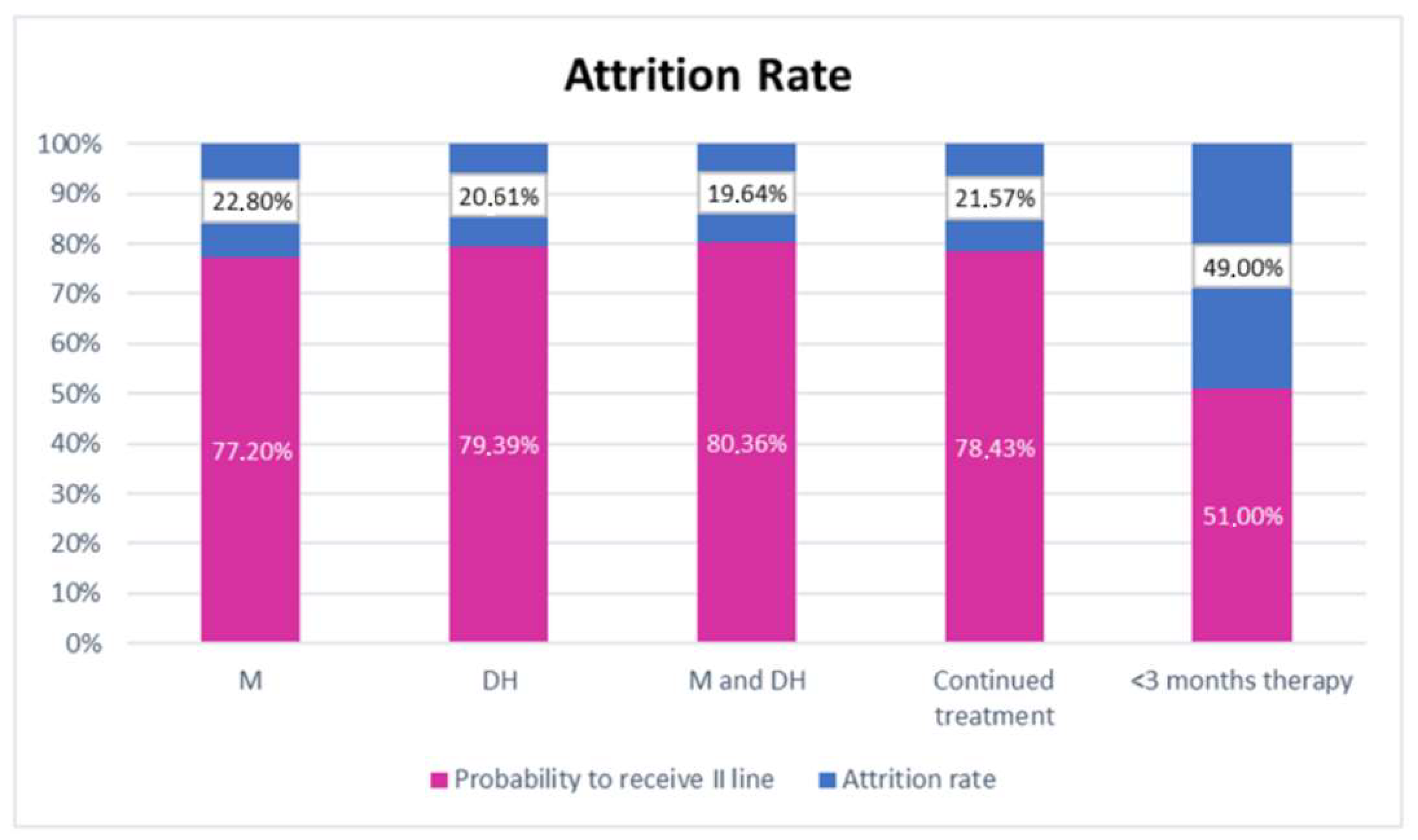
2.3. Attrition Rate across First-Line Treatment Strategies
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patient Population
4.3. Definition of Drug Holiday and Treatment Strategies
4.4. Sample Size Calculation
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Araghi, M.; Soerjomataram, I.; Jenkins, M.; Brierley, J.; Morris, E.; Bray, F.; Arnold, M. Global Trends in Colorectal Cancer Mortality: Projections to the Year 2035. Int. J. Cancer 2019, 144, 2992–3000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopetz, S.; Chang, G.J.; Overman, M.J.; Eng, C.; Sargent, D.J.; Larson, D.W.; Grothey, A.; Vauthey, J.-N.; Nagorney, D.M.; McWilliams, R.R. Improved Survival in Metastatic Colorectal Cancer Is Associated with Adoption of Hepatic Resection and Improved Chemotherapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 3677–3683. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus Bevacizumab versus FOLFIRI plus Bevacizumab as First-Line Treatment of Patients with Metastatic Colorectal Cancer: Updated Overall Survival and Molecular Subgroup Analyses of the Open-Label, Phase 3 TRIBE Study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Tabernero, J.; Van Cutsem, E.; Lakomý, R.; Prausová, J.; Ruff, P.; van Hazel, G.A.; Moiseyenko, V.M.; Ferry, D.R.; McKendrick, J.J.; Soussan-Lazard, K.; et al. Aflibercept versus Placebo in Combination with Fluorouracil, Leucovorin and Irinotecan in the Treatment of Previously Treated Metastatic Colorectal Cancer: Prespecified Subgroup Analyses from the VELOUR Trial. Eur. J. Cancer 2014, 50, 320–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartzberg, L.S.; Rivera, F.; Karthaus, M.; Fasola, G.; Canon, J.-L.; Hecht, J.R.; Yu, H.; Oliner, K.S.; Go, W.Y. PEAK: A Randomized, Multicenter Phase II Study of Panitumumab Plus Modified Fluorouracil, Leucovorin, and Oxaliplatin (MFOLFOX6) or Bevacizumab Plus MFOLFOX6 in Patients With Previously Untreated, Unresectable, Wild-Type KRAS Exon 2 Metastatic Colorectal. J. Clin. Oncol. 2014, 32, 2240–2247. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, V.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.-E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; Seipelt, G.; et al. FOLFIRI plus Cetuximab versus FOLFIRI plus Bevacizumab as First-Line Treatment for Patients with Metastatic Colorectal Cancer (FIRE-3): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2014, 15, 1065–1075. [Google Scholar] [CrossRef]
- Mayer, R.J.; Van Cutsem, E.; Falcone, A.; Yoshino, T.; Garcia-Carbonero, R.; Mizunuma, N.; Yamazaki, K.; Shimada, Y.; Tabernero, J.; Komatsu, Y.; et al. Randomized Trial of TAS-102 for Refractory Metastatic Colorectal Cancer. N. Engl. J. Med. 2015, 372, 1909–1919. [Google Scholar] [CrossRef] [Green Version]
- Grothey, A.; Van Cutsem, E.; Sobrero, A.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Regorafenib Monotherapy for Previously Treated Metastatic Colorectal Cancer (CORRECT): An International, Multicentre, Randomised, Placebo-Controlled, Phase 3 Trial. Lancet 2013, 381, 303–312. [Google Scholar] [CrossRef]
- Tournigand, C.; Cervantes, A.; Figer, A.; Lledo, G.; Flesch, M.; Buyse, M.; Mineur, L.; Carola, E.; Etienne, P.-L.; Rivera, F.; et al. OPTIMOX1: A Randomized Study of FOLFOX4 or FOLFOX7 with Oxaliplatin in a Stop-and-Go Fashion in Advanced Colorectal Cancer—A GERCOR Study. J. Clin. Oncol. 2006, 24, 394–400. [Google Scholar] [CrossRef] [Green Version]
- de Gramont, A.; Buyse, M.; Abrahantes, J.C.; Burzykowski, T.; Quinaux, E.; Cervantes, A.; Figer, A.; Lledo, G.; Flesch, M.; Mineur, L.; et al. Reintroduction of Oxaliplatin Is Associated with Improved Survival in Advanced Colorectal Cancer. J. Clin. Oncol. 2007, 25, 3224–3229. [Google Scholar] [CrossRef]
- Wasan, H.; Meade, A.M.; Adams, R.; Wilson, R.; Pugh, C.; Fisher, D.; Sydes, B.; Madi, A.; Sizer, B.; Lowdell, C.; et al. Intermittent Chemotherapy plus Either Intermittent or Continuous Cetuximab for First-Line Treatment of Patients with KRAS Wild-Type Advanced Colorectal Cancer (COIN-B): A Randomised Phase 2 Trial. Lancet Oncol. 2014, 15, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Luo, H.Y.; Li, Y.H.; Wang, W.; Wang, Z.Q.; Yuan, X.; Ma, D.; Wang, F.H.; Zhang, D.S.; Lin, D.R.; Lin, Y.C.; et al. Single-Agent Capecitabine as Maintenance Therapy after Induction of XELOX (or FOLFOX) in First-Line Treatment of Metastatic Colorectal Cancer: Randomized Clinical Trial of Efficacy and Safety. Ann. Oncol. 2016, 27, 1074–1081. [Google Scholar] [CrossRef]
- Cremolini, C.; Antoniotti, C.; Lonardi, S.; Aprile, G.; Bergamo, F.; Masi, G.; Grande, R.; Tonini, G.; Mescoli, C.; Cardellino, G.G.; et al. Activity and Safety of Cetuximab Plus Modified FOLFOXIRI Followed by Maintenance With Cetuximab or Bevacizumab for RAS and BRAF Wild-Type Metastatic Colorectal Cancer: A Randomized Phase 2 Clinical Trial. JAMA Oncol. 2018, 4, 529–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, A.; Schwenke, C.; Folprecht, G.; Arnold, D. Effect of Application and Intensity of Bevacizumab-Based Maintenance after Induction Chemotherapy with Bevacizumab for Metastatic Colorectal Cancer: A Meta-Analysis. Clin. Colorectal Cancer 2016, 15, e29–e39. [Google Scholar] [CrossRef] [PubMed]
- Hegewisch-Becker, S.; Graeven, U.; Lerchenmüller, C.A.; Killing, B.; Depenbusch, R.; Steffens, C.C.; Al-Batran, S.E.; Lange, T.; Dietrich, G.; Stoehlmacher, J.; et al. Maintenance Strategies after First-Line Oxaliplatin plus Fluoropyrimidine plus Bevacizumab for Patients with Metastatic Colorectal Cancer (AIO 0207): A Randomised, Non-Inferiority, Open-Label, Phase 3 Trial. Lancet Oncol. 2015, 16, 1355–1369. [Google Scholar] [CrossRef]
- Díaz-Rubio, E.; Gómez-España, A.; Massutí, B.; Sastre, J.; Abad, A.; Valladares, M.; Rivera, F.; Safont, M.J.; Martínez de Prado, P.; Gallén, M.; et al. First-Line XELOX plus Bevacizumab Followed by XELOX plus Bevacizumab or Single-Agent Bevacizumab as Maintenance Therapy in Patients with Metastatic Colorectal Cancer: The Phase III MACRO TTD Study. Oncologist 2012, 17, 15–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietrantonio, F.; Morano, F.; Corallo, S.; Miceli, R.; Lonardi, S.; Raimondi, A.; Cremolini, C.; Rimassa, L.; Bergamo, F.; Sartore-Bianchi, A.; et al. Maintenance Therapy with Panitumumab Alone vs. Panitumumab Plus Fluorouracil-Leucovorin in Patients with RAS Wild-Type Metastatic Colorectal Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2019, 5, 1268–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aparicio, T.; Ghiringhelli, F.; Boige, V.; Le Malicot, K.; Taieb, J.; Bouche, O.; Phelip, J.M.; François, E.; Borel, C.; Faroux, R.; et al. Bevacizumab Maintenance versus No Maintenance during Chemotherapy-Free Intervals in Metastatic Colorectal Cancer: A Randomized Phase III Trial (PRODIGE 9). J. Clin. Oncol. 2018, 36, 674–681. [Google Scholar] [CrossRef] [Green Version]
- Koeberle, D.; Betticher, D.C.; von Moos, R.; Dietrich, D.; Brauchli, P.; Baertschi, D.; Matter, K.; Winterhalder, R.; Borner, M.; Anchisi, S.; et al. Bevacizumab Continuation versus No Continuation after First-Line Chemotherapy plus Bevacizumab in Patients with Metastatic Colorectal Cancer: A Randomized Phase III Non-Inferiority Trial (SAKK 41/06). Ann. Oncol. 2015, 26, 709–714. [Google Scholar] [CrossRef]
- Chibaudel, B.; Maindrault-Goebel, F.; Lledo, G.; Mineur, L.; André, T.; Bennamoun, M.; Mabro, M.; Artru, P.; Carola, E.; Flesch, M.; et al. Can Chemotherapy Be Discontinued in Unresectable Metastatic Colorectal Cancer? The GERCOR OPTIMOX2 Study. J. Clin. Oncol. 2009, 27, 5727–5733. [Google Scholar] [CrossRef]
- Simkens, L.H.J.; Van Tinteren, H.; May, A.; Ten Tije, A.J.; Creemers, G.J.M.; Loosveld, O.J.L.; De Jongh, F.E.; Erdkamp, F.L.G.; Erjavec, Z.; Van Der Torren, A.M.E.; et al. Maintenance Treatment with Capecitabine and Bevacizumab in Metastatic Colorectal Cancer (CAIRO3): A Phase 3 Randomised Controlled Trial of the Dutch Colorectal Cancer Group. Lancet 2015, 385, 1843–1852. [Google Scholar] [CrossRef]
- Cremolini, C.; Casagrande, M.; Loupakis, F.; Aprile, G.; Bergamo, F.; Masi, G.; Moretto, R.R.; Pietrantonio, F.; Marmorino, F.; Zucchelli, G.; et al. Efficacy of FOLFOXIRI plus Bevacizumab in Liver-Limited Metastatic Colorectal Cancer: A Pooled Analysis of Clinical Studies by Gruppo Oncologico Del Nord Ovest. Eur. J. Cancer 2017, 73, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Modest, D.P.; Martens, U.M.; Riera-Knorrenschild, J.; Greeve, J.; Florschütz, A.; Wessendorf, S.; Ettrich, T.; Kanzler, S.; Nörenberg, D.; Ricke, J.; et al. FOLFOXIRI Plus Panitumumab As First-Line Treatment of RAS Wild-Type Metastatic Colorectal Cancer: The Randomized, Open-Label, Phase II VOLFI Study (AIO KRK0109). J. Clin. Oncol. 2019, 37, 3401–3411. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO Consensus Guidelines for the Management of Patients with Metastatic Colorectal Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Garattini, S.K.; Bonotto, M.; Porcu, L.; Ongaro, E.; Gerratana, L.; Basile, D.; Parnofiello, A.; Pelizzari, G.; Cortiula, F.; Corvaja, C.; et al. Determinants of Choice in Offering Drug Holidays during First-Line Therapy for Metastatic Colorectal Cancer. Future Oncol. Lond. Engl. 2020, 16, 2645–2660. [Google Scholar] [CrossRef]
- Maughan, T.S.; James, R.D.; Kerr, D.J.; Ledermann, J.A.; Seymour, M.T.; Topham, C.; McArdle, C.; Cain, D.; Stephens, R.J. Comparison of Intermittent and Continuous Palliative Chemotherapy for Advanced Colorectal Cancer: A Multicentre Randomised Trial. Lancet 2003, 361, 457–464. [Google Scholar] [CrossRef]
- Labianca, R.; Sobrero, A.; Isa, L.; Cortesi, E.; Barni, S.; Nicolella, D.; Aglietta, M.; Lonardi, S.; Corsi, D.; Turci, D.; et al. Intermittent versus Continuous Chemotherapy in Advanced Colorectal Cancer: A Randomised “GISCAD” Trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2011, 22, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.A.; Meade, A.M.; Seymour, M.T.; Wilson, R.H.; Madi, A.; Fisher, D.; Kenny, S.L.; Kay, E.; Hodgkinson, E.; Pope, M.; et al. Intermittent versus Continuous Oxaliplatin and Fluoropyrimidine Combination Chemotherapy for First-Line Treatment of Advanced Colorectal Cancer: Results of the Randomised Phase 3 MRC COIN Trial. Lancet Oncol. 2011, 12, 642–653. [Google Scholar] [CrossRef] [Green Version]
- Maindrault-Goebel, F.; Lledo, G.; Chibaudel, B.; Mineur, L.; Andre, T.; Bennamoun, M.; Mabro, M.; Artru, P.; Louvet, C.; De Gramont, A. OPTIMOX2, a Large Randomized Phase II Study of Maintenance Therapy or Chemotherapy-Free Intervals (CFI) after FOLFOX in Patients with Metastatic Colorectal Cancer (MRC). A GERCOR Study. J. Clin. Oncol. 2006, 24, 3504. [Google Scholar] [CrossRef]
- Berry, S.R.; Cosby, R.; Asmis, T.; Chan, K.; Hammad, N.; Krzyzanowska, M.K. Cancer Care Ontario’s Gastrointestinal Disease Site Group Continuous versus Intermittent Chemotherapy Strategies in Metastatic Colorectal Cancer: A Systematic Review and Meta-Analysis. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Loree, J.M.; Tan, S.K.; Lafond, L.M.; Speers, C.H.; Kennecke, H.F.; Cheung, W.Y. Real-World Effect of Maintenance and Intermittent Chemotherapy on Survival in Metastatic Colorectal Cancer. Clin. Colorectal Cancer 2018, 17, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahrabadi, A.; Ruan, J.; Gresham, G.; Cheung, W.Y. Predictors of Treatment Attrition in Patients with Metastatic Colorectal Cancer (mCRC). J. Clin. Oncol. 2017, 35, e18041. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Feinstein, A.R.; Holford, T.R. Importance of Events per Independent Variable in Proportional Hazards Regression Analysis. II. Accuracy and Precision of Regression Estimates. J. Clin. Epidemiol. 1995, 48, 1503–1510. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | N Total (608 Patients) | Frequency (%) |
|---|---|---|
| Sex: | ||
| Male | 383 | 63.0% |
| Female | 225 | 37.0% |
| Age: | ||
| <70 | 390 | 64.14% |
| >70 | 218 | 35.86% |
| ECOG performance status: | ||
| 0 | 51 | 8.39% |
| 1 | 463 | 76.15% |
| 2 | 48 | 7.89% |
| Missing | 46 | 7.57% |
| Location of primary tumor: | ||
| Right | 176 | 28.95% |
| Left | 245 | 40.30% |
| Rectum | 181 | 29.77% |
| Missing | 6 | 0.99% |
| Pathological T stage (TNM): | ||
| pT1 | 7 | 1.15% |
| pT2 | 31 | 5.10% |
| pT3 | 281 | 46.22% |
| PT4 | 117 | 19.24% |
| Missing | 172 | 28.30% |
| Pathological N stage (TNM): | ||
| N0 | 107 | 17.60% |
| N1 | 142 | 23.36% |
| N2 | 172 | 28.95% |
| N3 | 55 | 9.05% |
| Missing | 132 | 21.71% |
| Tumor Grading: | ||
| G1–2 | 244 | 40.13% |
| G3–4 | 156 | 26.66% |
| Missing | 208 | 34.21% |
| Resection of primary tumor: | ||
| Yes | 443 | 72.86% |
| No | 161 | 26.48% |
| Missing | 4 | 0.66% |
| Adjuvant chemotherapy: | ||
| Yes | 87 | 14.31% |
| No | 362 | 26.48% |
| N.A. | 159 | 26.15% |
| Neoadjuvant chemotherapy and RT: | ||
| Yes | 76 | 12.50% |
| No | 509 | 83.72% |
| Missing | 23 | 3.78% |
| Metastasectomy before first-line chemotherapy: | ||
| Yes | 128 | 21.05% |
| No | 478 | 78.62% |
| Missing | 2 | 0.33% |
| Number of metastatic sites: | ||
| 1 | 352 | 57.89% |
| >1 | 240 | 39.47% |
| Missing | 16 | 2.63% |
| Metastatic sites: | ||
| Liver | 204 | 33.55% |
| Lung | 128 | 21.05% |
| Lymph nodes | 102 | 16.78% |
| Peritoneum | 123 | 20.23% |
| Bone | 12 | 1.97% |
| CNS | 6 | 0.99% |
| Missing | 33 | 5.43% |
| Histotype: | ||
| Mucinous | 72 | 11.84% |
| Not mucinous | 324 | 53.29% |
| Missing | 212 | 34.87% |
| First-line chemotherapy: | ||
| Single agent | 72 | 11.84% |
| Doublet | 191 | 31.41% |
| Doublet + biologic agent | 270 | 44.41% |
| Triplet + biologic agent | 57 | 9.38% |
| Other | 18 | 2.96% |
| Maintenance therapy or drug holiday within first-line: | ||
| Maintenance | 117 | 19.24% |
| Holiday | 98 | 16.12% |
| Maintenance and holiday | 60 | 9.87% |
| Continuous treatment | 195 | 32.07% |
| <3 months of chemotherapy | 102 | 16.78% |
| Missing | 36 | 5.92% |
| Molecular biology status: | ||
| BRAF mut. | 45 | 7.40% |
| BRAF unknown | 131 | 21.55% |
| KRAS mut. | 237 | 38.98% |
| KRAS unknown | 93 | 15.30% |
| NRAS mut. | 16 | 2.63% |
| NRAS unknown | 192 | 31.58% |
| All-RAS mut. | 295 | 48.5% |
| All-RAS unknown | 62 | 10.2% |
| Second-line chemotherapy: | ||
| Yes | 422 | 69.41% |
| No | 161 | 26.48% |
| Missing | 25 | 4.11% |
| Drug Holiday: | ||
| Yes | 156 | 26.7% |
| No | 421 | 69.2% |
| Missing | 31 | 5.1% |
| Motivation for DH: | ||
| Patient’s request | 17 | 10.9% |
| Physician-patient shared choice | 103 | 66.0% |
| Unacceptable toxicity | 29 | 18.6% |
| Missing | 7 | 4.5% |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | HR | p | 95% CI | HR | p | 95% CI |
| Location of primary tumor: | ||||||
| Right | 1.00 | |||||
| Left | 0.66 | <0.001 | 0.54–0.82 | 0.59 | <0.001 | 0.45–0.79 |
| Rectum | 0.64 | <0.001 | 0.51–0.81 | 0.56 | <0.001 | 0.41–0.77 |
| Resection of primary tumor: | ||||||
| No | 1.00 | |||||
| Yes | 0.47 | <0.001 | 0.39–0.58 | 1.37 | 0.17 | 0.87–2.17 |
| Grading: | ||||||
| G1–2 | 1.00 | |||||
| G3–4 | 1.07 | 0.552 | 0.86–1.33 | |||
| Nodes: | ||||||
| 0 | 1.00 | |||||
| 1 | 1.16 | 0.304 | 0.87–1.55 | 1.04 | 0.784 | 0.75–1.46 |
| 2 | 1.56 | 0.001 | 1.19–2.05 | 1.57 | 0.005 | 1.14–2.17 |
| 3 | 2.31 | <0.001 | 1.61–3.30 | 1.52 | 0.129 | 0.88–2.63 |
| Adjuvant chemotherapy: | ||||||
| No | 1.00 | |||||
| Yes | 1.02 | 0.888 | 0.78–1.34 | |||
| All-RAS: | ||||||
| wt | 1.00 | |||||
| mut | 1.38 | 0.001 | 1.14–1.66 | 1.07 | 0.572 | 0.84–1.36 |
| ECOG performance status: | ||||||
| 0 | 1.00 | |||||
| 1 | 1.99 | <0.001 | 1.39–2.85 | 2.48 | <0.001 | 1.67–3.76 |
| 2 | 3.44 | <0.001 | 2.18–5.44 | 1.67 | 0.083 | 0.93–3.00 |
| Number of metastatic sites: | ||||||
| <1 | 1.00 | |||||
| >1 | 1.40 | <0.001 | 1.16–1.67 | 1.19 | 0.155 | 0.93–1.52 |
| Metastasectomy before first-line: | ||||||
| No | 1.00 | |||||
| Yes | 0.73 | 0.005 | 0.59–0.91 | 0.86 | 0.291 | 0.66–1.13 |
| Treatment strategy after induction: | ||||||
| Maintenance | 1.00 | - | - | 1.00 | - | - |
| Holiday | 0.76 | 0.12 | 0.59–1.07 | 0.94 | 0.758 | 0.66–1.35 |
| Maintenance and holiday | 0.78 | 0.137 | 0.55–1.10 | 0.70 | 0.108 | 0.46–1.08 |
| Continuous treatment | 1.57 | 0.001 | 1.22–2.02 | 1.68 | 0.002 | 1.22–2.32 |
| <3 months of chemotherapy | 3.75 | <0.001 | 2.81–5.01 | 4.89 | <0.001 | 3.33–7.19 |
| Multivariate Analysis | Score (Points) | |||
|---|---|---|---|---|
| Variables | HR | p | 95% CI | |
| Right location of primary tumor | 1.57 | <0.001 | 1.25–1.97 | 1 |
| All-RAS mutated | 1.26 | 0.189 | 0.89–1.78 | |
| ECOG performance status: | ||||
| 1 | 1.81 | 0.010 | 1.15–2.84 | 1 |
| 2 | 2.58 | 0.001 | 1.48–4.51 | 2 |
| Metastatic sites > 1 | 1.17 | 0.179 | 0.93–1.46 | |
| Metastasectomy | 0.95 | 0.703 | 0.73–1.24 | |
| Primary tumor unresected | 1.72 | <0.001 | 1.33–2.22 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garattini, S.K.; Basile, D.; Bonotto, M.; Ongaro, E.; Porcu, L.; Corvaja, C.; Cattaneo, M.; Andreotti, V.J.; Lisanti, C.; Bertoli, E.; et al. Drug Holidays and Overall Survival of Patients with Metastatic Colorectal Cancer. Cancers 2021, 13, 3504. https://doi.org/10.3390/cancers13143504
Garattini SK, Basile D, Bonotto M, Ongaro E, Porcu L, Corvaja C, Cattaneo M, Andreotti VJ, Lisanti C, Bertoli E, et al. Drug Holidays and Overall Survival of Patients with Metastatic Colorectal Cancer. Cancers. 2021; 13(14):3504. https://doi.org/10.3390/cancers13143504
Chicago/Turabian StyleGarattini, Silvio Ken, Debora Basile, Marta Bonotto, Elena Ongaro, Luca Porcu, Carla Corvaja, Monica Cattaneo, Victoria Josephine Andreotti, Camilla Lisanti, Elisa Bertoli, and et al. 2021. "Drug Holidays and Overall Survival of Patients with Metastatic Colorectal Cancer" Cancers 13, no. 14: 3504. https://doi.org/10.3390/cancers13143504
APA StyleGarattini, S. K., Basile, D., Bonotto, M., Ongaro, E., Porcu, L., Corvaja, C., Cattaneo, M., Andreotti, V. J., Lisanti, C., Bertoli, E., Pelizzari, G., Iacono, D., Miolo, G., Cardellino, G. G., Buonadonna, A., Aprile, G., Fasola, G., Puglisi, F., & Pella, N. (2021). Drug Holidays and Overall Survival of Patients with Metastatic Colorectal Cancer. Cancers, 13(14), 3504. https://doi.org/10.3390/cancers13143504