
Time-Sequencing of the Neutrophil-to-Lymphocyte Ratio to Predict Prognosis of Triple-Negative Breast Cancer

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Sequential NLR Measurements
2.4. Statistical Analysis
3. Results
3.1. Clinicopathologic Characteristics
3.2. Linear Mixed Model Analysis
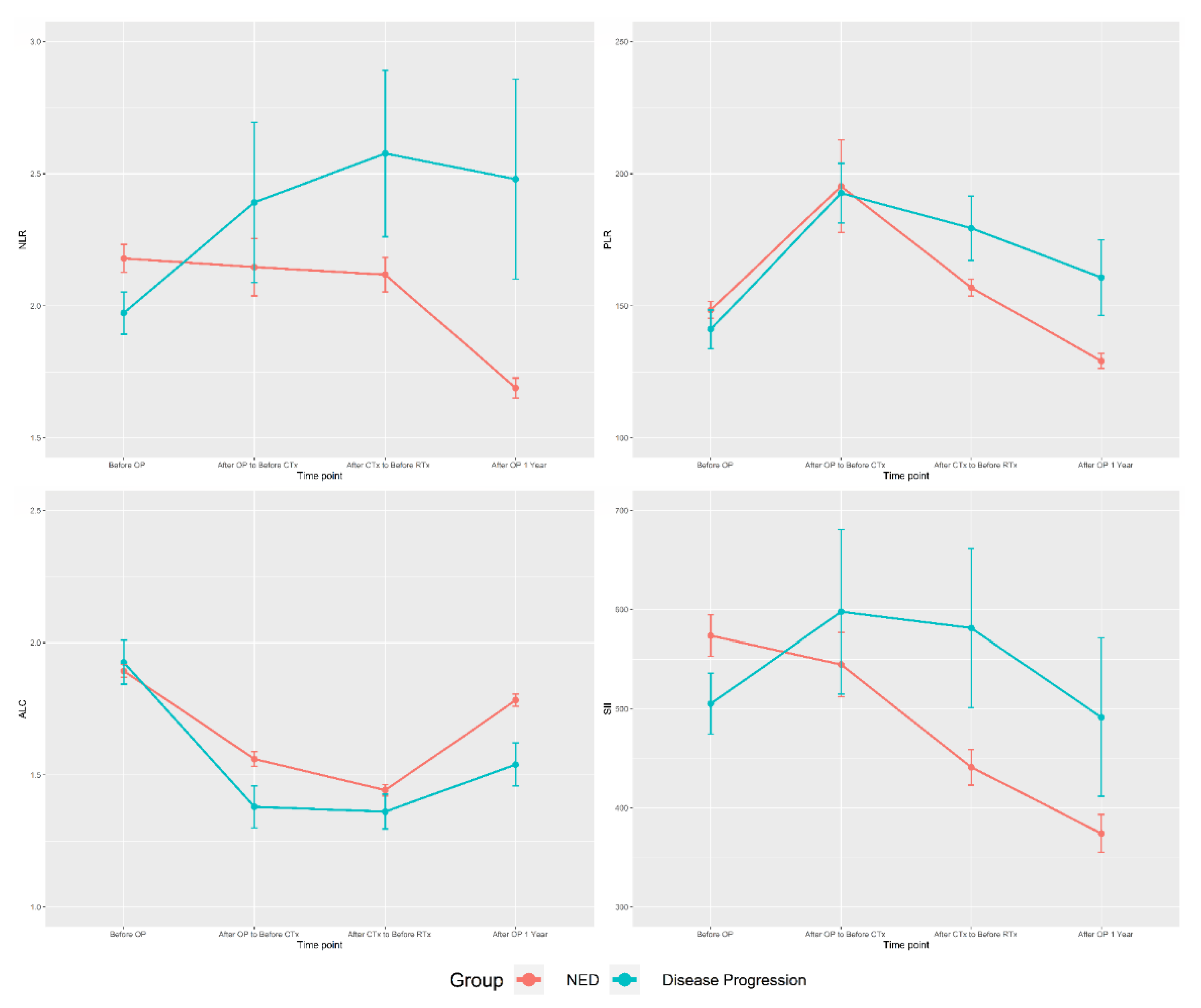
3.3. Time-Sequence Plot
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J. Clinic. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.Y.; Kim, Y.S.; Kim, Z.; Kim, H.Y.; Kim, H.J.; Park, S.; Bae, S.Y.; Yoon, K.H.; Lee, S.B.; Lee, S.K.; et al. Breast cancer statistics in korea in 2017: Data from a breast cancer registry. J. Breast Cancer 2020, 23, 115–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, A.; Eroles, P.; Zaragoza, R.; Viña, J.R.; Lluch, A. Triple-negative breast cancer: Molecular features, pathogenesis, treatment and current lines of research. Cancer Treat. Rev. 2010, 36, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Hancock, M.J. Appraisal of clinical practice guideline: Early and locally advanced breast cancer: Diagnosis and management. Nice guideline [ng101]. J. Physiother. 2019, 65, 57. [Google Scholar] [CrossRef]
- Pogoda, K.; Niwińska, A.; Murawska, M.; Pieńkowski, T. Analysis of pattern, time and risk factors influencing recurrence in triple-negative breast cancer patients. Med. Oncol. 2013, 30, 388. [Google Scholar] [CrossRef] [Green Version]
- Burstein, M.D.; Tsimelzon, A.; Poage, G.M.; Covington, K.R.; Contreras, A.; Fuqua, S.A.; Savage, M.I.; Osborne, C.K.; Hilsenbeck, S.G.; Chang, J.C.; et al. Comprehensive genomic analysis identifies novel subtypes and targets of triple-negative breast cancer. Clin. Cancer Res. 2015, 21, 1688–1698. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Invest. 2011, 121, 2750–2767. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Nat. Cancer Inst. 2014, 106, 124. [Google Scholar] [CrossRef] [Green Version]
- Wariss, B.R.; de Souza Abrahão, K.; de Aguiar, S.S.; Bergmann, A.; Thuler, L.C.S. Effectiveness of four inflammatory markers in predicting prognosis in 2374 women with breast cancer. Maturitas 2017, 101, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Chen, X.; Gao, W.; Zhu, S.; Wu, J.; Huang, O.; He, J.; Zhu, L.; Chen, W.; Li, Y.; et al. A high absolute lymphocyte count predicts a poor prognosis in her-2- positive breast cancer patients treated with trastuzumab. Cancer Manag. Res. 2019, 11, 3371–3379. [Google Scholar] [CrossRef] [Green Version]
- Huszno, J.; Kolosza, Z. Prognostic value of the neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratio in breast cancer patients. Oncol. Lett. 2019, 18, 6275–6283. [Google Scholar]
- Hua, X.; Long, Z.Q.; Zhang, Y.L.; Wen, W.; Guo, L.; Xia, W.; Zhang, W.W.; Lin, H.X. Prognostic value of preoperative systemic immune-inflammation index in breast cancer: A propensity score-matching study. Front. Oncol. 2020, 10, 580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corbeau, I.; Jacot, W.; Guiu, S. Neutrophil to lymphocyte ratio as prognostic and predictive factor in breast cancer patients: A systematic review. Cancers 2020, 12, 958. [Google Scholar] [CrossRef]
- Ethier, J.L.; Desautels, D.; Templeton, A.; Shah, P.S.; Amir, E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: A systematic review and meta-analysis. Breast Cancer Res. 2017, 19, 2. [Google Scholar] [CrossRef] [Green Version]
- Zenan, H.; Zixiong, L.; Zhicheng, Y.; Mei, H.; Xiongbin, Y.; Tiantian, W.; Min, D.; Renbin, L.; Changchang, J. Clinical prognostic evaluation of immunocytes in different molecular subtypes of breast cancer. J. Cell. Physiol. 2019, 234, 20584–20602. [Google Scholar] [CrossRef] [PubMed]
- Pistelli, M.; De Lisa, M.; Ballatore, Z.; Caramanti, M.; Pagliacci, A.; Battelli, N.; Ridolfi, F.; Santoni, M.; Maccaroni, E.; Bracci, R.; et al. Pre-treatment neutrophil to lymphocyte ratio may be a useful tool in predicting survival in early triple negative breast cancer patients. BMC Cancer 2015, 15, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American society of clinical oncology/college of american pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American society of clinical oncology/college of american pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef] [PubMed]
- Abramson, V.G.; Lehmann, B.D.; Ballinger, T.J.; Pietenpol, J.A. Subtyping of triple-negative breast cancer: Implications for therapy. Cancer 2015, 121, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Kim, D.M.; Lee, A. Prognostic role and clinical association of tumor-infiltrating lymphocyte, programmed death ligand-1 expression with neutrophil-lymphocyte ratio in locally advanced triple-negative breast cancer. Cancer Res. Treat. 2019, 51, 649–663. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.A.; Xi, J.; Luo, J.; Hassan, B.; Thomas, S.; Ma, C.X.; Campian, J.L. Neutrophil-to-lymphocyte ratio as a predictor of survival in patients with triple-negative breast cancer. Breast Cancer Res. Treat. 2019, 174, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, S.; Asano, Y.; Goto, W.; Takada, K.; Morisaki, T.; Kouhashi, R.; Yabumoto, A.; Tanaka, S.; Takashima, T.; Ohsawa, M.; et al. Validation of systemic and local tumour immune response to eribulin chemotherapy in the treatment of breast cancer. Anticancer Res. 2020, 40, 3345–3354. [Google Scholar] [CrossRef]
- Yoon, C.I.; Park, S.; Cha, Y.J.; Lee, H.S.; Bae, S.J.; Cha, C.; Lee, D.Y.; Ahn, S.G.; Jeong, J. Associations between absolute neutrophil count and lymphocyte-predominant breast cancer. Breast 2020, 50, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, Y.; Ozawa, H.; Higuchi, T.; Miyagawa, Y.; Bun, A.; Imamura, M.; Miyoshi, Y. Improved prognosis of low baseline neutrophil-to-lymphocyte ratio is significantly exclusive in breast cancer patients with high absolute counts of lymphocytes. Mol. Clin. Oncol. 2019, 10, 275–284. [Google Scholar] [CrossRef]
- Ivars Rubio, A.; Yufera, J.C.; de la Morena, P.; Fernandez Sanchez, A.; Navarro Manzano, E.; Garcia Garre, E.; Garcia Martinez, E.; Marin Zafra, G.; Sanchez Canovas, M.; Garcia Torralba, E.; et al. Neutrophil-lymphocyte ratio in metastatic breast cancer is not an independent predictor of survival, but depends on other variables. Sci. Rep. 2019, 9, 16979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moldoveanu, D.; Pravongviengkham, V.; Best, G.; Martínez, C.; Hijal, T.; Meguerditchian, A.N.; Lajoie, M.; Dumitra, S.; Watson, I.; Meterissian, S. Dynamic neutrophil-to-lymphocyte ratio: A novel prognosis measure for triple-negative breast cancer. Ann. Surg. Oncol. 2020, 27, 4028–4034. [Google Scholar] [CrossRef]
- Schmidt, M.; Böhm, D.; von Törne, C.; Steiner, E.; Puhl, A.; Pilch, H.; Lehr, H.A.; Hengstler, J.G.; Kölbl, H.; Gehrmann, M. The humoral immune system has a key prognostic impact in node-negative breast cancer. Cancer Res. 2008, 68, 5405–5413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu-Trantien, C.; Loi, S.; Garaud, S.; Equeter, C.; Libin, M.; de Wind, A.; Ravoet, M.; Le Buanec, H.; Sibille, C.; Manfouo-Foutsop, G.; et al. Cd4⁺ follicular helper t cell infiltration predicts breast cancer survival. J. Clin. Invest. 2013, 123, 2873–2892. [Google Scholar] [CrossRef]
- Kuwabara, T.; Kobayashi, S.; Sugiyama, Y. Pharmacokinetics and pharmacodynamics of a recombinant human granulocyte colony-stimulating factor. Drug Metabol. Rev. 1996, 28, 625–658. [Google Scholar] [CrossRef] [PubMed]
- Pillay, J.; den Braber, I.; Vrisekoop, N.; Kwast, L.M.; de Boer, R.J.; Borghans, J.A.; Tesselaar, K.; Koenderman, L. In vivo labeling with 2h2o reveals a human neutrophil lifespan of 5.4 days. Blood 2010, 116, 625–627. [Google Scholar] [CrossRef]
- Yang, B.B.; Kido, A. Pharmacokinetics and pharmacodynamics of pegfilgrastim. Clin. Pharmacokin. 2011, 50, 295–306. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Total | NED Group | Disease Progression Group | p-Value |
|---|---|---|---|---|
| Number of patients | 600 (100.00%) | 545 (90.83%) | 55 (9.17%) | |
| Age (years) | 49.88 ± 10.71 | 50.06 ± 10.50 | 48.15 ± 12.56 | 0.2070 |
| Preoperative NLR | 2.16 ± 1.20 | 2.18 ± 1.24 | 1.97 ± 0.59 | 0.0349 |
| Preoperative PLR | 147.68 ± 73.12 | 148.33 ± 74.75 | 141.13 ± 54.26 | 0.4906 |
| Preoperative ALC (1000 cells/mm3) | 1.90 ± 0.57 | 1.90 ± 0.57 | 1.93 ± 0.61 | 0.7215 |
| Preoperative SII | 567.01 ± 467.66 | 573.15 ± 484.86 | 505.17 ± 225.19 | 0.5626 a |
| T stage | 0.0019 | |||
| T1 | 362 (60.33%) | 341 (62.57%) | 21 (38.18%) | |
| T2 | 226 (37.67%) | 194 (35.60%) | 32 (58.18%) | |
| T3 | 12 (2.00%) | 10 (1.83%) | 2 (3.64%) | |
| N stage | <0.0001 | |||
| N0 | 506 (84.33%) | 470 (86.24%) | 36 (65.45%) | |
| N1 | 76 (12.67%) | 64 (11.74%) | 12 (21.82%) | |
| N2 | 10 (1.67%) | 7 (1.28%) | 3 (5.45%) | |
| N3 | 8 (1.33%) | 4 (0.73%) | 4 (7.27%) | |
| Histologic grade | 0.6016 | |||
| Low (Grade 1) | 147 (24.58%) | 134 (24.68%) | 13 (23.64%) | |
| High (Grade 2–3) | 425 (71.07%) | 384 (70.72%) | 41 (74.55%) | |
| Unknown | 26 (4.35%) | 25 (4.60%) | 1 (1.82%) | |
| CTx regimen | 0.0139 | |||
| Non taxane-based | 497 (82.83%) | 458 (84.04%) | 39 (70.91%) | |
| Taxane-based | 103 (17.17%) | 87 (15.96%) | 16 (29.09%) | |
| G-CSF | 0.9412 | |||
| No | 341 (56.83%) | 310 (56.88%) | 31 (56.36%) | |
| Yes | 259 (43.17%) | 235 (43.12%) | 24 (43.64%) | |
| Ki-67, N (%) c | 216 (36.00%) | 206 (37.80%) | 10 (18.18%) | 0.4564 b |
| 20% | 47 (21.76%) | 44 (21.36%) | 3 (30.00%) | |
| >20% | 169 (78.24%) | 162 (78.64%) | 7 (70.00%) | |
| LVI, N (%) c | 425 (70.83%) | 389 (71.38%) | 20 (65.45%) | 0.0003 b |
| Not identified | 389 (91.53%) | 363 (93.32%) | 26 (72.22%) | |
| Present | 36 (8.47%) | 26 (6.68%) | 10 (27.78%) |
| Time Point | Entire Cohort | NED Group | Disease Progression Group | p-Value |
|---|---|---|---|---|
| NLR | ||||
| Preoperative | 2.16 ± 1.20 | 2.18 ± 1.24 | 1.97 ± 0.59 | 0.0349 |
| Postoperative-before CTx | 2.17 ± 2.48 | 2.14 ± 2.50 | 2.39 ± 2.25 | 0.4812 |
| After CTx-before RTx | 2.16 ± 1.60 | 2.12 ± 1.50 | 2.58 ± 2.34 | 0.1595 |
| One year after surgery | 1.76 ± 1.15 | 1.69 ± 0.86 | 2.48 ± 2.68 | 0.0430 |
| PLR | ||||
| Preoperative | 147.68 ± 73.12 | 148.33 ± 74.75 | 141.13 ± 54.26 | 0.3739 |
| Postoperative-before CTx | 194.87 ± 385.61 | 195.10 ± 404.00 | 192.67 ± 83.87 | 0.9071 |
| After CTx-before RTx | 158.96 ± 74.33 | 156.88 ± 72.26 | 179.39 ± 90.56 | 0.0791 |
| One year after surgery | 131.83 ± 69.89 | 129.12 ± 65.69 | 160.73 ± 101.18 | 0.0348 |
| ALC (1000 cells/mm3) | ||||
| Preoperative | 1.90 ± 0.57 | 1.90 ± 0.56 | 1.93 ± 0.61 | 0.7379 |
| Postoperative-before CTx | 1.54 ± 0.63 | 1.56 ± 0.63 | 1.38 ± 0.59 | 0.0405 |
| After CTx-before RTx | 1.44 ± 0.49 | 1.44 ± 0.48 | 1.36 ± 0.48 | 0.2335 |
| One year after surgery | 1.76 ± 0.54 | 1.78 ± 0.53 | 1.54 ± 0.58 | 0.0019 |
| SII | ||||
| Preoperative | 567.01 ± 467.66 | 573.15 ± 484.86 | 505.17 ± 225.19 | 0.5626 a |
| Postoperative-before CTx | 549.14 ± 736.87 | 544.17 ± 748.62 | 597.75 ± 613.90 | 0.6812 a |
| After CTx-before RTx | 453.91 ± 438.29 | 440.98 ± 417.80 | 581.37 ± 594.30 | 0.0577 a |
| One year after surgery | 384.11 ± 450.85 | 374.04 ± 437.98 | 491.46 ± 564.53 | 0.0067 a |
| Unadjusted Model | Adjusted Model | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| NLR time point | ||||
| Preoperative | 1 | − | 1 | − |
| Postoperative-before CTx | 1.056 (0.981, 1.137) | 0.1472 | 1.228 (1.158, 1.301) | <0.0001 |
| After CTx-before RTx | 1.115 (1.011, 1.229) | 0.0292 | 1.269 (1.195, 1.349) | <0.0001 |
| One year after surgery | 1.196 (1.057, 1.354) | 0.0047 | 1.321 (1.237, 1.410) | <0.0001 |
| CTx regimen | ||||
| Non taxane-based | 1 | − | 1 | − |
| Taxane-based | 2.160 (1.847, 2.526) | <0.0001 | 0.956 (0.758, 1.206) | 0.7022 |
| T stage | ||||
| T1 | 1 | − | 1 | − |
| T2 | 2.678 (2.005, 3.579) | <0.0001 | 2.136 (1.818, 2.508) | <0.0001 |
| T3 | 3.248 (1.470, 7.174) | 0.0036 | 1.874 (1.125, 3.122) | 0.0159 |
| N stage | ||||
| N0 | 1 | − | 1 | − |
| N1 | 2.448 (1.720, 3.483) | <0.0001 | 2.201 (1.726, 2.806) | <0.0001 |
| N2 | 5.595 (2.781, 11.258) | <0.0001 | 5.651 (3.764, 8.485) | <0.0001 |
| N3 | 13.056 (6.384, 26.699) | <0.0001 | 9.175 (6.281, 13.402) | <0.0001 |
| Histologic grade | ||||
| Low (Grade 1) | 1 | − | 1 | − |
| High (Grade 2–3) | 1.101 (0.793, 1.528) | 0.5663 | 0.875 (0.733, 1.046) | 0.1425 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Son, N.-H.; Lee, J.-S.; Mun, J.-E.; Kim, J.-Y.; Park, H.-S.; Park, S.; Kim, S.-I.; Park, B.-W. Time-Sequencing of the Neutrophil-to-Lymphocyte Ratio to Predict Prognosis of Triple-Negative Breast Cancer. Cancers 2021, 13, 3472. https://doi.org/10.3390/cancers13143472
Kim J-H, Son N-H, Lee J-S, Mun J-E, Kim J-Y, Park H-S, Park S, Kim S-I, Park B-W. Time-Sequencing of the Neutrophil-to-Lymphocyte Ratio to Predict Prognosis of Triple-Negative Breast Cancer. Cancers. 2021; 13(14):3472. https://doi.org/10.3390/cancers13143472
Chicago/Turabian StyleKim, Joo-Heung, Nak-Hoon Son, Jun-Sang Lee, Ji-Eun Mun, Jee-Ye Kim, Hyung-Seok Park, Seho Park, Seung-Il Kim, and Byeong-Woo Park. 2021. "Time-Sequencing of the Neutrophil-to-Lymphocyte Ratio to Predict Prognosis of Triple-Negative Breast Cancer" Cancers 13, no. 14: 3472. https://doi.org/10.3390/cancers13143472
APA StyleKim, J.-H., Son, N.-H., Lee, J.-S., Mun, J.-E., Kim, J.-Y., Park, H.-S., Park, S., Kim, S.-I., & Park, B.-W. (2021). Time-Sequencing of the Neutrophil-to-Lymphocyte Ratio to Predict Prognosis of Triple-Negative Breast Cancer. Cancers, 13(14), 3472. https://doi.org/10.3390/cancers13143472