
Comparison of Surgical Outcomes between Robotic Transaxillary and Conventional Open Thyroidectomy in Pediatric Thyroid Cancer

 ,
,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Operative Procedure
2.3. Postoperative Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Surgical Outcomes and Pathologic Findings
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chaukar, D.A.; Rangarajan, V.; Nair, N.; Dcruz, A.K.; Nadkarni, M.S.; Pai, P.S.; Mistry, R.C. Pediatric thyroid cancer. J. Surg. Oncol. 2005, 92, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Paulson, V.A.; Rudzinski, E.R.; Hawkins, D.S. Thyroid cancer in the pediatric population. Genes 2019, 10, 723. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.A.; Yun, H.R.; Lee, J.; Moon, H.; Shin, C.H.; Kim, S.G.; Park, Y.J. Trends in Pediatric Thyroid Cancer Incidence, Treatment, and Clinical Course in Korea during 2004–2016: A Nationwide Population-Based Study. Thyroid 2021, 31, 902–911. [Google Scholar] [CrossRef]
- Cho, Y.Y.; Jang, H.W.; Joung, J.Y.; Park, S.-M.; Jeong, D.J.; Kim, S.W.; Chung, J.H. Trends in thyroid cancer incidence in Korean children (1999–2012) based on palpation and nonpalpation detection methods. Eur. Thyroid. J. 2015, 4, 252–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, Z.J.; Jin, M.C.; Meister, K.D.; Megwalu, U.C. Pediatric thyroid cancer incidence and mortality trends in the United States, 1973–2013. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Dermody, S.; Walls, A.; Harley, E.H., Jr. Pediatric thyroid cancer: An update from the SEER database 2007–2012. Int. J. Pediatr. Otorhinolaryngol. 2016, 89, 121–126. [Google Scholar] [CrossRef]
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.; Hay, I.D.; Luster, M. Management guidelines for children with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on pediatric thyroid cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [Green Version]
- Welch Dinauer, C.A.; Tuttle, M.; Robie, D.K.; McClellan, D.R.; Svec, R.L.; Adair, C.; Francis, G.L. Clinical features associated with metastasis and recurrence of differentiated thyroid cancer in children, adolescents and young adults. Clin. Endocrinol. 1998, 49, 619–628. [Google Scholar] [CrossRef]
- Hunter, J.G. Minimally invasive surgery: The next frontier. World J. Surg. 1999, 23, 422. [Google Scholar] [CrossRef] [PubMed]
- Seybt, M.W.; Terris, D.J. Minimally Invasive Thyroid Surgery in Children. Ann. Otol. Rhinol. Laryngol. 2011, 120, 215–219. [Google Scholar] [CrossRef]
- Lee, J.; Chung, W.Y. Advanced developments in neck dissection technique: Perspectives in minimally invasive surgery. Neck Dissection Clinical Appl. Recent Adv. 2012, 176, 87–102. [Google Scholar]
- Lobe, T.E.; Wright, S.K.; Irish, M.S. Novel uses of surgical robotics in head and neck surgery. J. Laparoendosc Adv. Surg. Tech. A 2005, 15, 647–652. [Google Scholar] [CrossRef]
- Wu, E.L.; Garstka, M.E.; Kang, S.-W.; Kandil, E. Robotic neck surgery in the pediatric population. JSLs 2018, 22, e2018.00012. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-W.; Lee, S.C.; Lee, S.H.; Lee, K.Y.; Jeong, J.J.; Lee, Y.S.; Nam, K.-H.; Chang, H.S.; Chung, W.Y.; Park, C.S. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: The operative outcomes of 338 consecutive patients. Surgery 2009, 146, 1048–1055. [Google Scholar] [CrossRef]
- Lee, J.; Nah, K.Y.; Kim, R.M.; Ahn, Y.H.; Soh, E.-Y.; Chung, W.Y. Differences in postoperative outcomes, function, and cosmesis: Open versus robotic thyroidectomy. Surg. Endosc. 2010, 24, 3186–3194. [Google Scholar] [CrossRef]
- Brunaud, L.; Germain, A.; Zarnegar, R.; Klein, M.; Ayav, A.; Bresler, L. Robotic thyroid surgery using a gasless transaxillary approach: Cosmetic improvement or improved quality of surgical dissection? J. Visc. Surg. 2010, 147, e399–e402. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-W.; Park, J.H.; Jeong, J.S.; Lee, C.R.; Park, S.; Lee, S.H.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y.; Park, C.S. Prospects of robotic thyroidectomy using a gasless, transaxillary approach for the management of thyroid carcinoma. Surg. Laparosc. Endosc Percutan. Tech. 2011, 21, 223–229. [Google Scholar] [CrossRef] [Green Version]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; Schlumberger, M. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, I.D.; Gonzalez-Losada, T.; Reinalda, M.S.; Honetschlager, J.A.; Richards, M.L.; Thompson, G.B. Long-term outcome in 215 children and adolescents with papillary thyroid cancer treated during 1940 through 2008. World J. Surg. 2010, 34, 1192–1202. [Google Scholar] [CrossRef]
- Ryu, H.R.; Kang, S.-W.; Lee, S.H.; Rhee, K.Y.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y.; Park, C.S. Feasibility and safety of a new robotic thyroidectomy through a gasless, transaxillary single-incision approach. J. Am. Coll. Surg. 2010, 211, e13–e19. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Chung, W.Y. Robotic thyroidectomy and neck dissection: Past, present, and future. Cancer J. 2013, 19, 151–161. [Google Scholar] [CrossRef]
- Xing, M.; Liu, R.; Liu, X.; Murugan, A.K.; Zhu, G.; Zeiger, M.A.; Pai, S.; Bishop, J. BRAF V600E and TERT promoter mutations cooperatively identify the most aggressive papillary thyroid cancer with highest recurrence. J. Clin. Oncol. 2014, 32, 2718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, X.C.; Yu, W.Q.; Shang, J.B.; Wang, K.J. Clinical characteristics and treatment of thyroid cancer in children and adolescents: A retrospective analysis of 83 patients. J. Zhejiang Univ. Sci. B 2017, 18, 430–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambale, C.; Elisei, R.; Matrone, A. Management and follow-up of differentiated thyroid cancer not submitted to radioiodine treatment: A systematic review. Minerva Endocrinol. 2020, 45, 306–317. [Google Scholar] [PubMed]
- Foley, C.S.; Agcaoglu, O.; Siperstein, A.E.; Berber, E. Robotic transaxillary endocrine surgery: A comparison with conventional open technique. Surg. Endosc. 2012, 26, 2259–2266. [Google Scholar] [CrossRef] [PubMed]
- Jackson, N.R.; Yao, L.; Tufano, R.P.; Kandil, E.H. Safety of robotic thyroidectomy approaches: Meta-analysis and systematic review. Head Neck 2014, 36, 137–143. [Google Scholar] [CrossRef]
- Kandil, E.H.; Noureldine, S.I.; Yao, L.; Slakey, D.P. Robotic transaxillary thyroidectomy: An examination of the first one hundred cases. J. Am. Coll. Surg. 2012, 214, 558–564. [Google Scholar] [CrossRef]
- Cvasciuc, T.; Lansdown, M.; Fraser, S.M. Routine intraoperative neuromonitoring during thyroidectomy: A UK single-institution experience. Minerva Endocrinol. 2018, 44, 236–238. [Google Scholar] [CrossRef]
- Tuttle, R.; Haugen, B.; Perrier, N. The updated AJCC/TNM staging system for differentiated and anaplastic thyroid cancer: What changed and why. Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef]
- Tuggle, C.T.; Roman, S.A.; Wang, T.S.; Boudourakis, L.; Thomas, D.C.; Udelsman, R.; Sosa, J.A. Pediatric endocrine surgery: Who is operating on our children? Surgery 2008, 144, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Popadich, A.; Levin, O.; Lee, J.C.; Smooke-Praw, S.; Ro, K.; Fazel, M.; Arora, A.; Tolley, N.S.; Palazzo, F.; Learoyd, D.L. A multicenter cohort study of total thyroidectomy and routine central lymph node dissection for cN0 papillary thyroid cancer. Surgery 2011, 150, 1048–1057. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.A.; Jimeno, J.; Miquel, J.; Iglesias, M.; Munné, A.; Sancho, J.J.; Sitges-Serra, A. Nodal yield, morbidity, and recurrence after central neck dissection for papillary thyroid carcinoma. Surgery 2005, 138, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- Barczyński, M.; Konturek, A.; Stopa, M.; Nowak, W. Prophylactic central neck dissection for papillary thyroid cancer. Br. J. Surg. 2013, 100, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.-W.; Lee, S.H.; Park, J.H.; Jeong, J.S.; Park, S.; Lee, C.R.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y.; Park, C.S. A comparative study of the surgical outcomes of robotic and conventional open modified radical neck dissection for papillary thyroid carcinoma with lateral neck node metastasis. Surg. Endosc. 2012, 26, 3251–3257. [Google Scholar] [CrossRef]
- Kang, S.-W.; Jeong, J.J.; Yun, J.-S.; Sung, T.Y.; Lee, S.C.; Lee, Y.S.; Nam, K.-H.; Chang, H.S.; Chung, W.Y.; Park, C.S. Robot-assisted endoscopic surgery for thyroid cancer: Experience with the first 100 patients. Surg. Endosc. 2009, 23, 2399–2406. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Robotic (n = 99) | Open (n = 62) | p-Value | |
|---|---|---|---|---|
| Sex, male:female | 6:93 | 16:46 | <0.001 | |
| Age (years) | 16.9 ± 2.3 (8–19) | 16.8 ± 3.0 (7–19) | 0.559 | |
| BMI (kg/m2) | 22.2 ± 3.9 (14.1–39.7) | 22.0 ± 4.8 (13.2–35.9) | 0.425 | |
| Diagnostic Sx | ||||
| Incidentaloma | 90 (90.9) | 59 (95.2) | 0.317 | |
| Hypo- or Hyperthyroidism | 3 (3.0) | 1 (1.6) | 0.551 | |
| Others | 6 (6.1) | 2 (3.2) | 0.551 | |
| Radiation exposure | 0 (0.0) | 0 (0.0) | ||
| Family hx | 20 (20.2) | 11 (17.7) | 0.700 | |
| Thyroid cancer of first degree | 12 (12.1) | 2 (3.2) | ||
| Thyroid cancer of second degree | 6 (6.1) | 7 (11.3) | ||
| Others (Lung cancer, hypothyroidism) | 2 (2.0) | 2 (3.2) | ||
| Operation | Robotic (n = 99) | Open (n = 62) | p-Value | |
|---|---|---|---|---|
| Operation type | ||||
| Lobectomy | 3 (3.0) | 2 (3.2) | 0.432 | |
| Lobectomy with CCND | 29 (29.3) | 9 (14.5) | ||
| Ipsilateral TT and contralateral partial or subtotal thyroidectomy with CCND | 14 (14.1) | 3 (4.8) | ||
| BTT with CCND | 30 (30.3) | 15 (24.2) | 0.010 | |
| BTT with MRND | 23 (23.2) | 33 (53.2) | ||
| Operation time (min) | 171.2 ± 101.7 (69–635) | 182.6 ± 98.2 (43–456) | 0.496 | |
| Combined procedure during operation | 3 (3.0) | 7 (11.3) | 0.035 | |
| RLN shaving | 3 (3.0) | 1 (1.6) | ||
| Tracheal wall shaving | 0 (0.0) | 2 (3.2) | ||
| RLN and tracheal wall shaving | 0 (0.0) | 3 (4.8) | ||
| RLN shaving and tracheal re-anastomosis | 0 (0.0) | 1 (1.6) | ||
| Pathology | Robotic (n = 99) | Open (n = 62) | p-Value | |
|---|---|---|---|---|
| Pathology of cancer | 0.639 | |||
| PTC | 94 (94.9) | 58 (93.5) | ||
| FTC | 4 (4.1) | 4 (6.5) | ||
| PDTC | 1 (1.0) | 0 (0.0) | ||
| Tumor size (cm) | 1.8 ± 1.2 (0.2–5.3) | 2.5 ± 1.8 (0.3–8.5) | 0.010 | |
| Tumor number | 0.134 | |||
| Single | 70 (71.4) | 34 (54.8) | ||
| Multiple | 8 (8.2) | 10 (16.1) | ||
| Bilateral | 20 (20.4) | 18 (29.0) | ||
| Gross ETE positivity | 48 (48.5) | 39 (62.9) | 0.165 | |
| No. of harvested LNs | ||||
| Positive nodes of CCND | 2.8 ± 3.2 | 6.0 ± 5.2 | <0.001 | |
| Total node of CCND | 7.3 ± 5.1 | 11.3 ± 7.0 | <0.001 | |
| Positive node of MRND | 6.2 ± 4.1 | 12.5 ± 11.2 | 0.012 | |
| Total node of MRND | 43.0 ± 31.2 | 59.3 ± 40.9 | 0.107 | |
| Stage | Robotic (n = 99) | Open (n = 62) | p-Value | |
|---|---|---|---|---|
| T stage | 0.010 | |||
| T 0 | 1 (1.0) | 0 (0.0) | 0.401 | |
| T 1 | 38 (38.4) | 11 (17.7) | ||
| T 2 | 12 (12.1) | 7 (11.3) | ||
| T 3a | 0 (0.0) | 5 (8.1) | 0.013 | |
| T 3b | 45 (45.5) | 32 (51.6) | ||
| T 4a | 3 (3.0) | 7 (11.3) | ||
| T 4b | 0 (0.0) | 0 (0.0) | ||
| N stage | 0.001 | |||
| N 0 | 33 (33.3) | 10 (16.1) | ||
| N 1a | 43 (43.4) | 19 (30.6) | ||
| N 1b | 23 (23.2) | 33 (53.2) | ||
| M stage | 0.009 | |||
| M 0 | 98 (99.0) | 56 (90.3) | ||
| M 1 | 1 (1.0) | 6 (9.7) | ||
| BRAF mutation positivity | 21 (50%) (n = 42) | 18 (62.1%) (n = 29) | 0.315 | |
| Characteristics | Robotic (n = 99) | Open (n = 62) | p-Value | |
|---|---|---|---|---|
| Postoperative complication | 21 (21.2) | 25 (40.3) | 0.009 | |
| Transient hypocalcemia | 15 (15.2) | 18 (29.0) | 0.076 | |
| Permanent hypocalcemia | 2 (2.0) | 2 (3.2) | 0.632 | |
| Chyle leakage | 2 (2.0) | 3 (4.8) | 0.316 | |
| Infection | 1 (1.0) | 0 (0.0) | 0.427 | |
| Transient hoarseness | 1 (1.0) | 0 (0.0) | 0.427 | |
| RLN injury | 0 (0.0) | 1 (1.6) | 0.205 | |
| Horner’s syndrome | 0 (0.0) | 1 (1.6) | 0.205 | |
| Length of hospital stay (days) | 3.6 ± 1.1 | 4.8 ± 2.0 | <0.001 | |
| Recurrence | Robotic (n = 99) | Open (n = 62) | p-Value | |
|---|---|---|---|---|
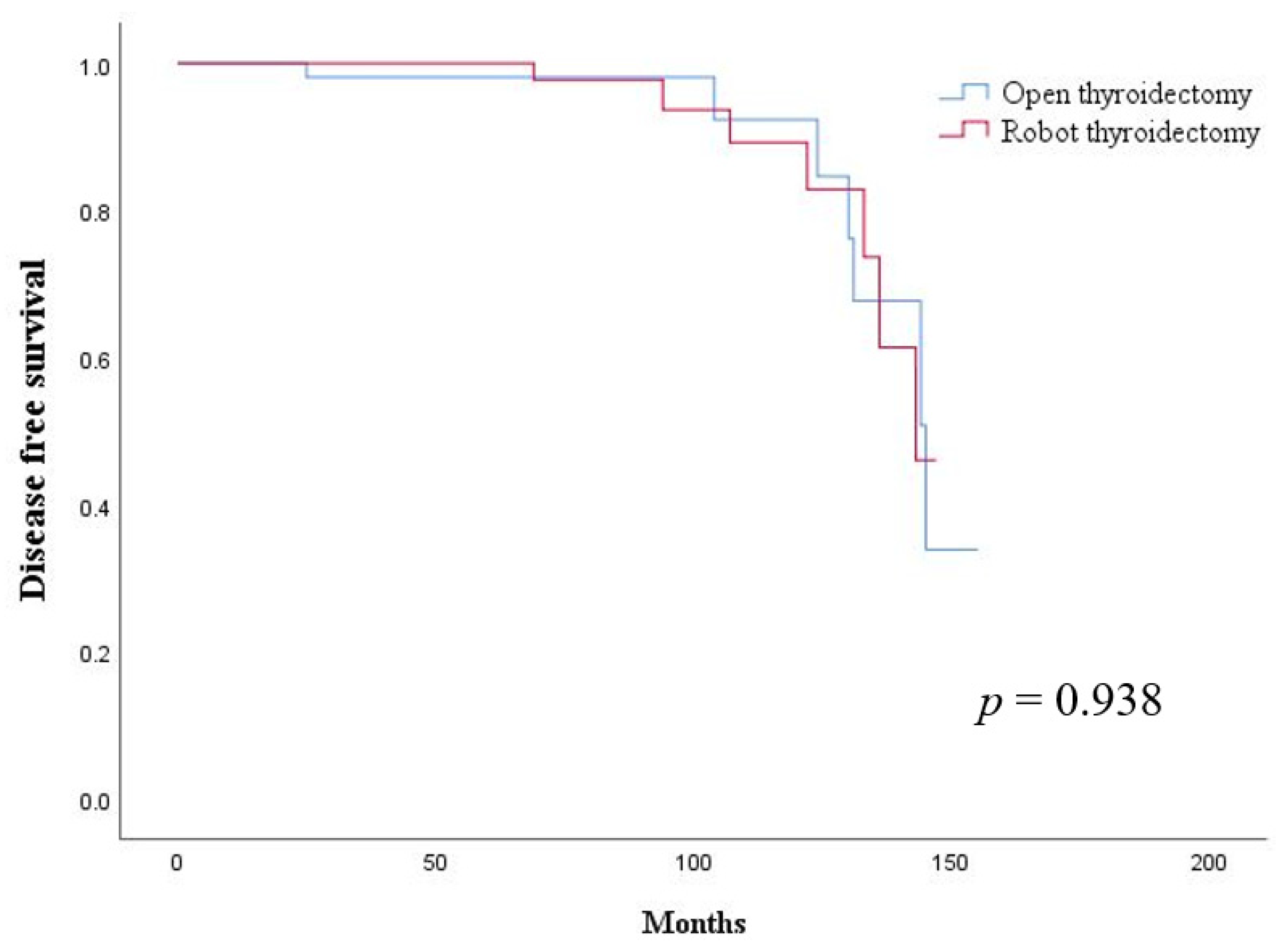
| Follow-up time (months) | 67.0 ± 38.5 (6–147) | 72.1 ± 42.7 (8–155) | 0.569 | |
| Recurrence rate | 7 (7.1) | 7 (11.3) | 0.355 | |
| Recurrence site | 0.472 | |||
| Local | 3 (3.0) | 5 (8.1) | ||
| Distant | 3 (3.0) | 1 (1.6) | ||
| Local and distant | 1 (1.0) | 1 (1.6) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.A.; Kim, K.; Kim, J.K.; Kang, S.-W.; Lee, J.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y. Comparison of Surgical Outcomes between Robotic Transaxillary and Conventional Open Thyroidectomy in Pediatric Thyroid Cancer. Cancers 2021, 13, 3293. https://doi.org/10.3390/cancers13133293
Lee IA, Kim K, Kim JK, Kang S-W, Lee J, Jeong JJ, Nam K-H, Chung WY. Comparison of Surgical Outcomes between Robotic Transaxillary and Conventional Open Thyroidectomy in Pediatric Thyroid Cancer. Cancers. 2021; 13(13):3293. https://doi.org/10.3390/cancers13133293
Chicago/Turabian StyleLee, In A, Kwangsoon Kim, Jin Kyong Kim, Sang-Wook Kang, Jandee Lee, Jong Ju Jeong, Kee-Hyun Nam, and Woong Youn Chung. 2021. "Comparison of Surgical Outcomes between Robotic Transaxillary and Conventional Open Thyroidectomy in Pediatric Thyroid Cancer" Cancers 13, no. 13: 3293. https://doi.org/10.3390/cancers13133293
APA StyleLee, I. A., Kim, K., Kim, J. K., Kang, S.-W., Lee, J., Jeong, J. J., Nam, K.-H., & Chung, W. Y. (2021). Comparison of Surgical Outcomes between Robotic Transaxillary and Conventional Open Thyroidectomy in Pediatric Thyroid Cancer. Cancers, 13(13), 3293. https://doi.org/10.3390/cancers13133293