
The Clinical Relevance of Target Lymph Node Biopsy after Primary Systemic Therapy in Initially Node-Positive Breast Cancer Patients


Abstract
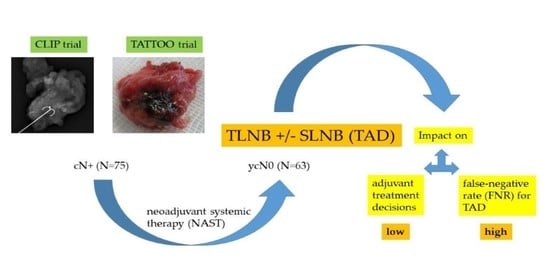
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Labeling of the TLN and Axillary Surgery
2.3. Pathologic Eevaluation
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinicopathologic Characteristics
3.2. DR and FNR of SLN and TLN
3.3. Impact of TLN on Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banys-Paluchowsky, M.; Gasparri, M.L.; de Boniface, J.; Gentilini, O.; Stickeler, E.; Hartmann, S.; Thill, M.; Rubio, I.T.; Di Micco, R.; Bonci, E.A.; et al. Surgical management of the axilla in clinically node-positive breast cancer patients converting to clinical node negativity through neoadjuvant chemotherapy: Current status, knowledge gaps and rational for the EUBREAST-03 AXSANA Study. Cancers 2021, 13, 1565. [Google Scholar] [CrossRef] [PubMed]
- Dominici, L.S.; Negron Gonzalez, V.M.; Buzdar, A.U.; Lucci, A.; Mittendorf, E.A.; Le-Petross, H.T.; Babiera, G.V.; Meric-Bernstam, F.; Hunt, K.K.; Kuerer, H.M. Cytologically proven axillary lymph node metastases are eradicated in patients receiving preoperative chemotherapy with concurrent trastuzumab for HER2-positive breast cancer. Cancer 2010, 15, 2884–2889. [Google Scholar] [CrossRef]
- Boughey, J.C.; McCall, L.M.; Ballman, K.V.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Flippo-Morton, T.; Hunt, K.K. Tumor biology correlates with rates of breast-conserving surgery and pathologic complete response after neoadjuvant chemotherapy for breast cancer: Findings from the ACOSOG Z1071 (Alliance) prospective multicenter clinical trial. Ann. Surg. 2014, 260, 608–614. [Google Scholar] [CrossRef]
- Diego, E.J.; McAuliffe, P.F.; Soran, A.; McGuire, K.P.; Johnson, R.R.; Bonaventura, M.; Ahrendt, G.M. Axillary staging after neoadjuvant chemotherapy for breast cancer: A pilot study combining sentinel lymph node biopsy with radioactive seed localization of pre-treatment positive axillary lymph nodes. Ann. Surg. Oncol. 2016, 23, 1549–1553. [Google Scholar] [CrossRef]
- Fleissig, A.; Fallowfield, L.J.; Langridge, C.I.; Johnson, L.; Newcombe, R.G.; Dixon, J.M.; Kissin, M.; Mansel, R.E. Post-operative arm morbidity and quality of life. Results of the ALMANAC randomised trial comparing sentinel node biopsy with standard axillary treatment in the management of patients with early breast cancer. Breast Cancer Res. Treat. 2006, 95, 279–293. [Google Scholar] [CrossRef]
- Lucci, A.; McCall, L.M.; Beitsch, P.D.; Whitworth, P.W.; Reintgen, D.S.; Blumencranz, P.W.; Leitch, A.M.; Saha, S.; Hunt, K.K.; Giuliano, A.E. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J. Clin. Oncol. 2007, 25, 3657–3663. [Google Scholar] [CrossRef] [PubMed]
- Simons, J.M.; van Nijnatten, T.J.A.; van der Pol, C.C.; Luiten, E.J.T.; Koppert, L.B.; Smidt, M.L. Diagnostic accuracy of different surgical procedures for axillary staging after neoadjuvant systemic therapy in node-positive breast cancer: A systematic review and meta-analysis. Ann. Surg. 2019, 269, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; von Mickwitz, G.; Nekljudova, V.; et al. Sentinel-lymph-node biopsy with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective multi-center cohort study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.; et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) clinical trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef]
- Boileau, J.F.; Basik, M.; Holloway, C.M.; Gaboury, L.; Sideris, L.; Meterissian, S.; Arnaout, A.; Brackstone, M.; McCready, D.R.; Karp, S.E.; et al. Sentinel node biopsy after neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: The SN FNAC study. J. Clin. Oncol. 2015, 33, 258–264. [Google Scholar] [CrossRef]
- Boughey, J.C.; Ballman, K.V.; Le-Petross, H.T.; McCall, L.M.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Feliberti, E.C.; Hunt, K.K. Identification and resection of clipped node decreases the false-negative rate of sentinel lymph node surgery in patients presenting with node-positive breast cancer (T0-T4, N1-N2) who receive neoadjuvant chemotherapy: Results from ACOSOG Z1071 (Alliance). Ann. Surg. 2016, 263, 802–807. [Google Scholar] [CrossRef]
- Caudle, A.S.; Yang, W.T.; Krishnamurthy, S.; Mittendorf, E.A.; Black, D.M.; Gilcrease, M.Z.; Bedrosian, I.; Hobbs, B.P.; DeSnyder, S.M.; Hwang, R.F.; et al. Improved axillary evaluation following neoadjuvant chemotherapy for patients with node-positive breast cancer using selective evaluation of clipped nodes: Implementation of targeted axillary dissection. J. Clin. Oncol. 2016, 34, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Kuemmel, S.; Heil, J.; Rueland, A.; Seiberling, C.; Harrach, H.; Schindowski, D.; Lubitz, J.; Hellerhoff, K.; Ankel, C.; Graßhoff, S.T.; et al. A prospective, multicenter registry study to evaluate the clinical feasibility of targeted axillary dissection (TAD) in node-positive breast cancer patients. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Weiss, A.; King, C.; Grossmith, S.; Portnow, L.; Raza, S.; Nakhlis, F.; Dominici, L.; Mittendorf, E.A.; King, T.A. How often does retrieval of a clipped lymph node change adjuvant therapy recommendations? A prospective consecutive patient cohort study. In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 8–11 December 2020. Poster discussion 4-06. [Google Scholar]
- Hartmann, S.; Reimer, T.; Gerber, B.; Stubert, J.; Stengel, B.; Stachs, A. Wire localization of clip-marked axillary lymph nodes in breast cancer patients treated with primary systemic therapy. Eur. J. Surg. Oncol. 2018, 44, 1307–1311. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, S.; Kühn, T.; de Boniface, J.; Stachs, A.; Winckelmann, A.; Frisell, J.; Wiklander-Brakenhielm, I.; Stubert, J.; Gerber, B.; Reimer, T. The prospective multicenter TATTOO trial evaluating carbon tattooing for targeted lymph node biopsy after primary systemic therapy in breast cancer patients. Br. J. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ditsch, N.; Untch, M.; Kolberg-Liedtke, C.; Jackisch, C.; Krug, D.; Friedrich, M.; Janni, W.; Müller, V.; Albert, U.S.; Banys-Paluchowski, M.; et al. AGO recommendations for the diagnosis and treatment of patients with locally advanced and metastatic breast cancer: Update 2020. Breast Care 2020, 15, 294–309. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.; Lester, S.C. Pathology of breast carcinomas after neoadjuvant chemotherapy: An overview with recommendations on specimen processing and reporting. Arch. Pathol. Lab. Med. 2009, 133, 633–642. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Huang, C.S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Masuda, N.; Lee, S.J.; Ohtani, S.; Im, Y.H.; Lee, E.S.; Yokota, I.; Kuroi, K.; Im, S.A.; Park, B.W.; Kim, S.B.; et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Tadros, A.B.; Yang, W.T.; Krishnamurty, S.; Rauch, G.M.; Smith, B.D.; Valero, V.; Black, D.M.; Lucci Jr, A.; Caudle, A.S.; DeSnyder, S.M.; et al. Identification of patients with documented pathologic complete response in the breast after neoadjuvant chemotherapy for omission of axillary surgery. JAMA Surg. 2017, 152, 665–670. [Google Scholar] [CrossRef]
- Riba, L.A.; Russell, T.; Alapati, A.; Davis, R.B.; James, T.A. Characterizing response to neoadjuvant chemotherapy in invasive lobular breast carcinoma. J. Surg. Res. 2019, 233, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Moo, T.A.; Edelweiss, M.; Haijyeva, S.; Stempel, M.; Raiss, M.; Zabor, E.C.; Barrio, A.; Morrow, M. Is low-volume disease in the sentinel node after neoadjuvant chemotherapy an indication for axillary dissection? Ann. Surg. Oncol. 2018, 25, 1488–1494. [Google Scholar] [CrossRef]
- Clinical trials.gov. Comparison of Axillary Lymph Node Dissection with Axillary Radiation for Patients with Node-Positive Breast Cancer Treated with Chemotherapy. Available online: https://clinicaltrials.gov/ct2/show/study/NCT01901094 (accessed on 4 April 2021).
- Clinical trials.gov. Standard or Comprehensive Radiation Therapy in Treating Patients with Early-Stage Breast Cancer Previously Treated with Chemotherapy and Surgery. Available online: https://clinicaltrials.gov/ct2/show/NCT01872975 (accessed on 4 April 2021).
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology, Breast Cancer. Version 3. 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 3 April 2021).
- Wong, S.M.; Almana, N.; Choi, J.; Hu, J.; Gagnon, H.; Natsuhara, K.; Shen, A.H.; DeSantis, S.; Dominici, L.; Golshan, M.; et al. Prognostic significance of residual axillary nodal micrometastases and isolated tumor cells after neoadjuvant chemotherapy for breast cancer. Ann. Surg. Oncol. 2019, 26, 3502–3509. [Google Scholar] [CrossRef] [PubMed]
- Kahler-Ribeiro-Fontana, S.; Pagan, E.; Magnoni, F.; Vicini, E.; Morigi, C.; Corso, G.; Intra, M.; Canegallo, F.; Ratini, S.; Leonardi, M.C.; et al. Long-term standard sentinel node biopsy after neoadjuvant treatment in breast cancer: A single institution ten-year follow-up. Eur. J. Surg. Oncol. 2021, 47, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Damin, A.P.; Zancan, M.; Melo, M.P.; Biazus, J.V. Sentinel lymph node biopsy after neoadjuvant chemotherapy in patients with node-positive breast cancer: Guiding a more selective axillary approach. Breast Cancer Res. Treat. 2021, 186, 527–534. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Minimal Invasive Axillary Staging and Treatment after Neoadjuvant Systemic Therapy in Node Positive Breast Cancer (MINIMAX). Available online: https://www.clinicaltrials.gov/ct2/show/NCT04486495 (accessed on 5 April 2021).


{kind=link}
{kind=link}
| Characteristics | No. of Patients | % |
|---|---|---|
| Initial clinical tumor stage | ||
| cT1 | 19 | 25.3 |
| cT2 | 53 | 70.7 |
| cT3/4 | 3 | 4.0 |
| No. of initially suspicious LN on US | ||
| 1–3 | 62 | 82.7 |
| ˃3 | 13 | 17.3 |
| Tumor type | ||
| invasive ductal | 66 | 88.0 |
| invasive lobular | 5 | 6.7 |
| other | 4 | 5.3 |
| Grading | ||
| 2 | 16 | 21.3 |
| 3 | 59 | 78.7 |
| Receptor-based subtype | ||
| HR+/HER2− | 16 | 21.3 |
| HR+/HER2+ | 11 | 14.7 |
| HR−/HER2+ | 14 | 18.7 |
| HR−/HER2− | 34 | 45.3 |
| Suspicious LN on US after PST | ||
| no | 63 | 84.0 |
| yes | 12 | 16.0 |
| Pathologic complete remission | ||
| no | 44 | 58.7 |
| yes | 31 | 41.3 |
| Type of surgery | ||
| breast conservation | 56 | 74.7 |
| mastectomy | 19 | 25.3 |
| Removed LN | ycN0/n = 20 (%) | No. of SLN ˂3/n = 14 (%) | SLN ≠ TLN/n = 5 (%) |
|---|---|---|---|
| SLNB | 4 (20.0) | 4 (28.6) | 3 (60.0) |
| TLNB | 3 (15.0) | 2 (14.3) | 3 (60.0) |
| TAD | 1 (5.0) | 1 (7.1) | 1 (20.0) |
| Patient | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Age (years) | 53 | 45 | 66 | 73 | 63 |
| Initial tumor size (mm) | 47 | 23 | 57 | 17 | 17 |
| No. of initially suspicious LN | 1 | 2 | 3 | 2 | 1 |
| Receptor-based subtype | HR+/ HER2− | HR+/ HER2− | HR−/HER2+ | HR−/HER2− | HR+/ HER2− |
| Type of breast surgery | ME | BCS | ME | BCS | BCS |
| Invasive breast tumor after PST (mm) | 8 | 12 | 5 | 0 | 11 |
| metastatic TLN | 1/1 | 1/2 | 1/1 | 1/2 | 2/3 |
| SLN | 0/1 | 0/1 | ND | ND | ND |
| metastatic LN (TLN + ALND) | 2/13 | 1/8 | 2/6 | 3/7 | 5/8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartmann, S.; Stachs, A.; Schultek, G.; Gerber, B.; Reimer, T. The Clinical Relevance of Target Lymph Node Biopsy after Primary Systemic Therapy in Initially Node-Positive Breast Cancer Patients. Cancers 2021, 13, 2620. https://doi.org/10.3390/cancers13112620
Hartmann S, Stachs A, Schultek G, Gerber B, Reimer T. The Clinical Relevance of Target Lymph Node Biopsy after Primary Systemic Therapy in Initially Node-Positive Breast Cancer Patients. Cancers. 2021; 13(11):2620. https://doi.org/10.3390/cancers13112620
Chicago/Turabian StyleHartmann, Steffi, Angrit Stachs, Gesche Schultek, Bernd Gerber, and Toralf Reimer. 2021. "The Clinical Relevance of Target Lymph Node Biopsy after Primary Systemic Therapy in Initially Node-Positive Breast Cancer Patients" Cancers 13, no. 11: 2620. https://doi.org/10.3390/cancers13112620
APA StyleHartmann, S., Stachs, A., Schultek, G., Gerber, B., & Reimer, T. (2021). The Clinical Relevance of Target Lymph Node Biopsy after Primary Systemic Therapy in Initially Node-Positive Breast Cancer Patients. Cancers, 13(11), 2620. https://doi.org/10.3390/cancers13112620