Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial?

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Cancer Patients and COVID-19: What Are the Global Consequences for Oncology?
3. Cancer Care and COVID-19: Clinical Observations
4. COVID-19 and Anti-Cancer Therapy: Advantages and Disadvantages of ICI-Immunotherapy
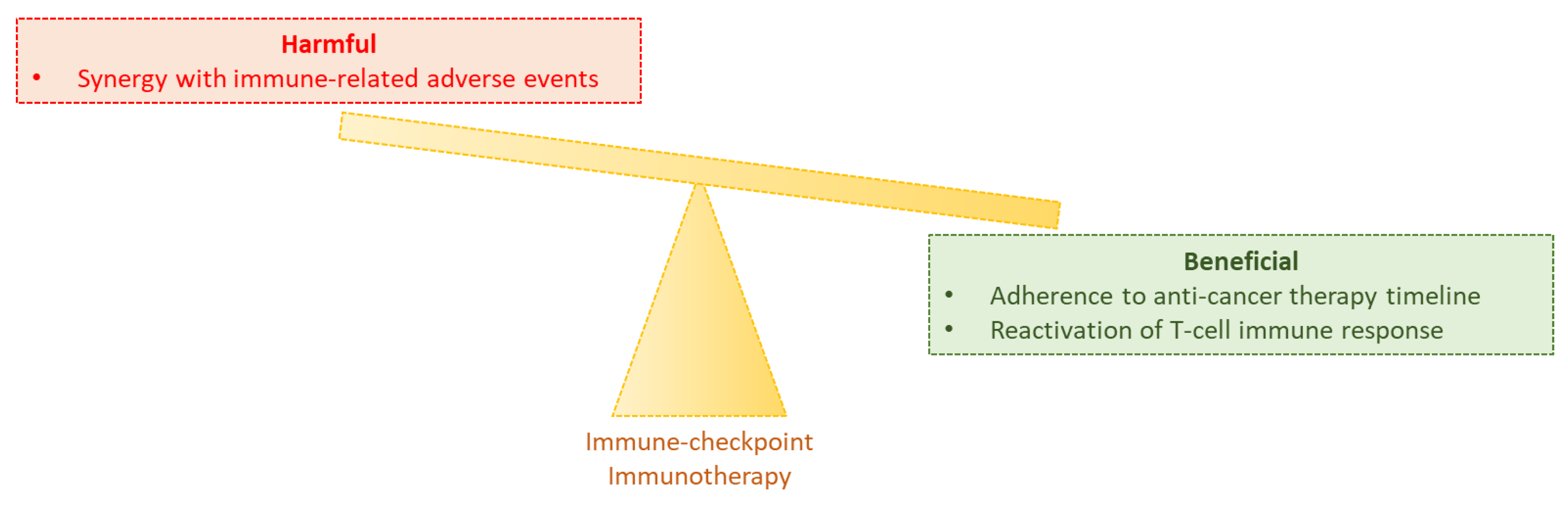
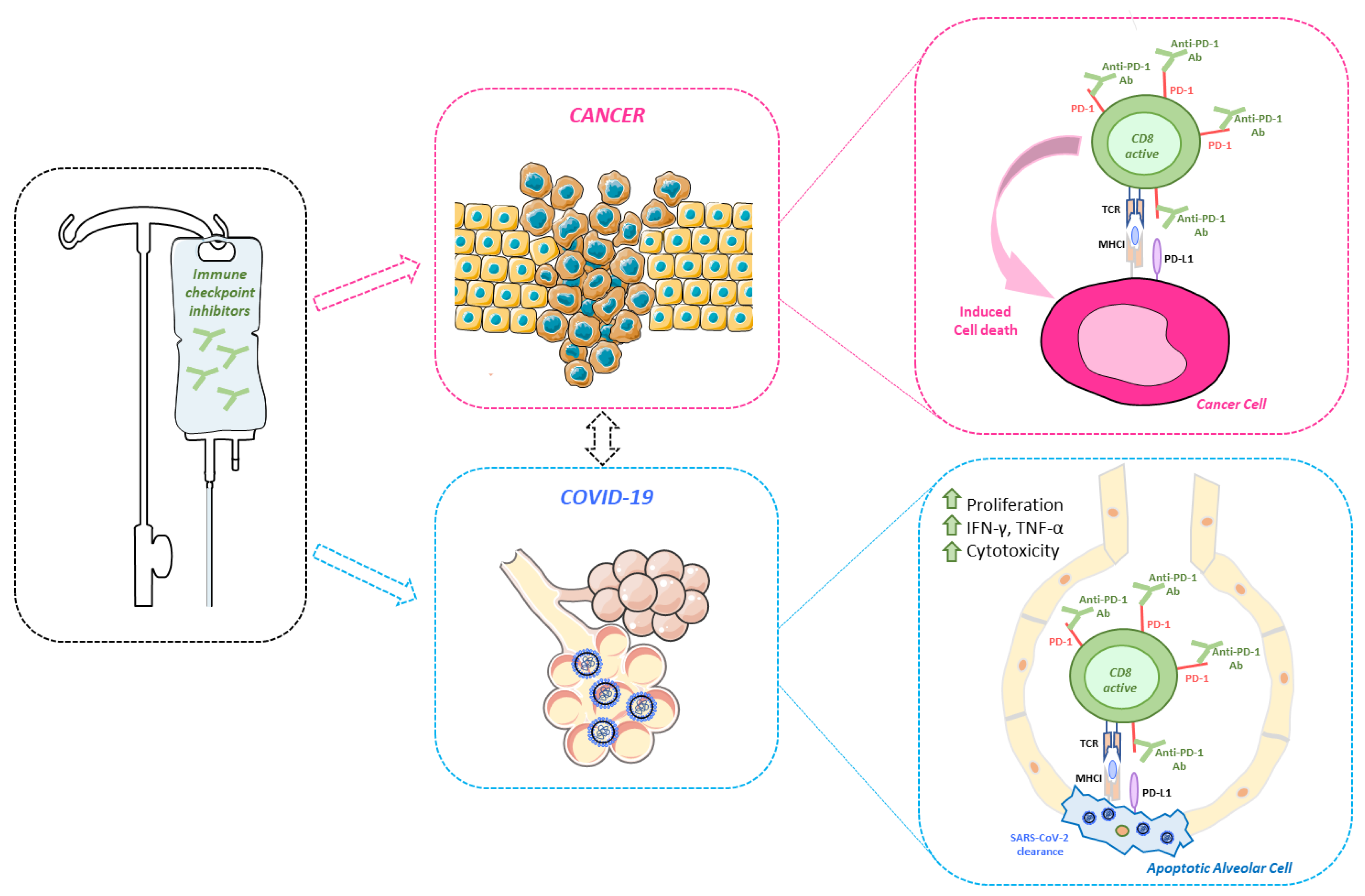
5. Our Hypothesis: Using ICI-Blockade in Cancer Patients during the Pandemic Does not Harm and Might Be a Game-Changer
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Cui, J.; Li, F.; Shi, Z.-L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef]
- Arab-Zozani, M.; Hassanipour, S. Features and Limitations of LitCovid Hub for Quick Access to Literature About COVID-19. Balk. Med. J. 2020, 37. [Google Scholar] [CrossRef]
- Bimonte, S.; Crispo, A.; Amore, A.; Celentano, E.; Cuomo, A.; Cascella, M. Potential Antiviral Drugs for SARS-Cov-2 Treatment: Preclinical Findings and Ongoing Clinical Research. In Vivo 2020, 34, 1597–1602. [Google Scholar] [CrossRef]
- Li, X.; Ma, X. Acute respiratory failure in COVID-19: Is it “typical” ARDS? Crit. Care 2020, 24, 198. [Google Scholar] [CrossRef]
- Renu, K.; Prasanna, P.L.; Valsala Gopalakrishnan, A. Coronaviruses pathogenesis, comorbidities and multi-organ damage–A review. Life Sci. 2020, 255, 117839. [Google Scholar] [CrossRef]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor Recognition by the Novel Coronavirus from Wuhan: An Analysis Based on Decade-Long Structural Studies of SARS Coronavirus. J. Virol. 2020, 94. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef]
- Li, X.; Geng, M.; Peng, Y.; Meng, L.; Lu, S. Molecular immune pathogenesis and diagnosis of COVID-19. J. Pharm. Anal. 2020, 10, 102–108. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Coperchini, F.; Chiovato, L.; Croce, L.; Magri, F.; Rotondi, M. The cytokine storm in COVID-19: An overview of the involvement of the chemokine/chemokine-receptor system. Cytokine Growth Factor Rev. 2020, 53, 25–32. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Ong, E.Z.; Chan, Y.F.Z.; Leong, W.Y.; Lee, N.M.Y.; Kalimuddin, S.; Haja Mohideen, S.M.; Chan, K.S.; Tan, A.T.; Bertoletti, A.; Ooi, E.E.; et al. A Dynamic Immune Response Shapes COVID-19 Progression. Cell Host Microbe 2020, 27, 879–882. [Google Scholar] [CrossRef]
- McKechnie, J.L.; Blish, C.A. The Innate Immune System: Fighting on the Front Lines or Fanning the Flames of COVID-19? Cell Host Microbe 2020, 27, 863–869. [Google Scholar] [CrossRef]
- Buonaguro, F.M.; Puzanov, I.; Ascierto, P.A. Anti-IL6R role in treatment of COVID-19-related ARDS. J. Transl. Med. 2020, 18, 165. [Google Scholar] [CrossRef]
- Arnaldez, F.I.; O’Day, S.J.; Drake, C.G.; Fox, B.A.; Fu, B.; Urba, W.J.; Montesarchio, V.; Weber, J.S.; Wei, H.; Wigginton, J.M.; et al. The Society for Immunotherapy of Cancer perspective on regulation of interleukin-6 signaling in COVID-19-related systemic inflammatory response. J. Immunother. Cancer 2020, 8, e000930. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef]
- Wang, B.; Wang, L.; Kong, X.; Geng, J.; Xiao, D.; Ma, C.; Jiang, X.; Wang, P. Long-term coexistence of SARS-CoV-2 with antibody response in COVID-19 patients. J. Med. Virol. 2020, 28. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 287. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Landscape of COVID-19 Candidate Vaccines. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 27 June 2020).
- Wu, R.; Wang, L.; Kuo, H.-C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef]
- Magro, G. COVID-19: Review on latest available drugs and therapies against SARS-CoV-2. Coagulation and inflammation cross-talking. Virus Res. 2020, 286, 198070. [Google Scholar] [CrossRef]
- Rosa, S.G.V.; Santos, W.C. Clinical trials on drug repositioning for COVID-19 treatment. Rev. Panam. Salud Pública 2020, 44, 1. [Google Scholar] [CrossRef]
- Lythgoe, M.P.; Middleton, P. Ongoing Clinical Trials for the Management of the COVID-19 Pandemic. Trends Pharmacol. Sci. 2020, 41, 363–382. [Google Scholar] [CrossRef]
- Gonzalez, H.; Hagerling, C.; Werb, Z. Roles of the immune system in cancer: From tumor initiation to metastatic progression. Genes Dev. 2018, 32, 1267–1284. [Google Scholar] [CrossRef]
- Wargo, J.A.; Reuben, A.; Cooper, Z.A.; Oh, K.S.; Sullivan, R.J. Immune Effects of Chemotherapy, Radiation, and Targeted Therapy and Opportunities for Combination With Immunotherapy. Semin. Oncol. 2015, 42, 601–616. [Google Scholar] [CrossRef]
- Tan, J.; Yang, C. Prevention and control strategies for the diagnosis and treatment of cancer patients during the COVID-19 pandemic. Br. J. Cancer 2020, 123, 5–6. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.-C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, L. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020, 21, E181. [Google Scholar] [CrossRef]
- Kutikov, A.; Weinberg, D.S.; Edelman, M.J.; Horwitz, E.M.; Uzzo, R.G.; Fisher, R.I. A War on Two Fronts: Cancer Care in the Time of COVID-19. Ann. Intern. Med. 2020, 172, 756–758. [Google Scholar] [CrossRef] [PubMed]
- Mauri, D.; Kamposioras, K.; Tolia, M.; Alongi, F.; Tzachanis, D.; Petricevic, B.; Chilingirova, N.; Mihaylova, I.; Tsakiridis, T.; Salembier, C.; et al. Summary of international recommendations in 23 languages for patients with cancer during the COVID-19 pandemic. Lancet Oncol. 2020, 21, 759–760. [Google Scholar] [CrossRef]
- The Lancet Oncology. COVID-19: Global consequences for oncology. Lancet Oncol. 2020, 21, 467. [Google Scholar] [CrossRef]
- Burki, T.K. Cancer guidelines during the COVID-19 pandemic. Lancet Oncol. 2020, 21, 629–630. [Google Scholar] [CrossRef]
- Hanna, T.P.; Evans, G.A.; Booth, C.M. Cancer, COVID-19 and the precautionary principle: Prioritizing treatment during a global pandemic. Nat. Rev. Clin. Oncol. 2020, 17, 268–270. [Google Scholar] [CrossRef]
- van de Haar, J.; Hoes, L.R.; Coles, C.E.; Seamon, K.; Fröhling, S.; Jäger, D.; Valenza, F.; de Braud, F.; De Petris, L.; Bergh, J.; et al. Caring for patients with cancer in the COVID-19 era. Nat. Med. 2020, 26, 665–671. [Google Scholar] [CrossRef]
- Saini, K.S.; de las Heras, B.; de Castro, J.; Venkitaraman, R.; Poelman, M.; Srinivasan, G.; Saini, M.L.; Verma, S.; Leone, M.; Aftimos, P.; et al. Effect of the COVID-19 pandemic on cancer treatment and research. Lancet Haematol. 2020, 7, E432–E435. [Google Scholar] [CrossRef]
- Rubinstein, S.M.; Steinharter, J.A.; Warner, J.; Rini, B.I.; Peters, S.; Choueiri, T.K. The COVID-19 and Cancer Consortium: A Collaborative Effort to Understand the Effects of COVID-19 on Patients with Cancer. Cancer Cell 2020, 37, 738–741. [Google Scholar] [CrossRef]
- Anil, I.; Arnold, R.; Benkwitz-Beford, S.; Branford, S.; Campton, N.; Cazier, J.-B.; Cheng, V.; Curley, H.; D’Costa, J.; Edmondson, A.; et al. The UK Coronavirus Cancer Monitoring Project: Protecting patients with cancer in the era of COVID-19. Lancet Oncol. 2020, 21, 622–624. [Google Scholar] [CrossRef]
- Moujaess, E.; Kourie, H.R.; Ghosn, M. Cancer patients and research during COVID-19 pandemic: A systematic review of current evidence. Crit. Rev. Oncol. Hematol. 2020, 150, 102972. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Xia, Y.; Jin, R.; Zhao, J.; Li, W.; Shen, H. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020, 21, E180. [Google Scholar] [CrossRef]
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 Transmission in Patients With Cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Miyashita, H.; Mikami, T.; Chopra, N.; Yamada, T.; Chernyavsky, S.; Rizk, D.; Cruz, C. Do patients with cancer have a poorer prognosis of COVID-19? An experience in New York City. Ann. Oncol. 2020, 31, 1088–1089. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-COV-2: A multi-center study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [PubMed]
- Basse, C.; Diakite, S.; Servois, V.; Maxime, F.; Noret, A.; Bellesoeur, A.; Massiani, M.-A.; Bouyers, A.; Laurence, B.; Cottu, P. Characteristics and outcome of SARS-CoV-2 infection in cancer patients. Medrxiv Prepr. 2020. [Google Scholar] [CrossRef]
- Lee, L.Y.; Cazier, J.-B.; Starkey, T.; Turnbull, C.; UK Coronavirus Cancer Monitoring Project Team; Kerr, R.; Middleton, G. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Poortmans, P.M.; Guarneri, V.; Cardoso, M.-J. Cancer and COVID-19: What do we really know? Lancet 2020, 395, 1884–1885. [Google Scholar] [CrossRef]
- Robilotti, E.V.; Babady, N.E.; Mead, P.A.; Rolling, T.; Perez-Johnston, R.; Bernardes, M.; Bogler, Y.; Caldararo, M.; Figueroa, C.J.; Glickman, M.S.; et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zappasodi, R.; Merghoub, T.; Wolchok, J.D. Emerging Concepts for Immune Checkpoint Blockade-Based Combination Therapies. Cancer Cell 2018, 33, 581–598. [Google Scholar] [CrossRef] [PubMed]
- Christofi, T.; Baritaki, S.; Falzone, L.; Libra, M.; Zaravinos, A. Current Perspectives in Cancer Immunotherapy. Cancers 2019, 11, 1472. [Google Scholar] [CrossRef] [PubMed]
- Darvin, P.; Toor, S.M.; Sasidharan Nair, V.; Elkord, E. Immune checkpoint inhibitors: Recent progress and potential biomarkers. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Falzone, L.; Salomone, S.; Libra, M. Evolution of Cancer Pharmacological Treatments at the Turn of the Third Millennium. Front. Pharmacol. 2018, 9, 1300. [Google Scholar] [CrossRef]
- Leonardi, G.; Candido, S.; Falzone, L.; Spandidos, D.; Libra, M. Cutaneous melanoma and the immunotherapy revolution (Review). Int. J. Oncol. 2020, 57, 609–618. [Google Scholar]
- La-Beck, N.M.; Nguyen, D.T.; Le, A.D.; Alzghari, S.K.; Trinh, S.T. Optimizing Patient Outcomes with PD-1/PD-L1 Immune Checkpoint Inhibitors for the First-Line Treatment of Advanced Non–Small Cell Lung Cancer. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 239–255. [Google Scholar] [CrossRef]
- Souza, I.L.; Fernandes, Í.; Taranto, P.; Buzaid, A.C.; Schvartsman, G. Immune-related pneumonitis with nivolumab and ipilimumab during the coronavirus disease 2019 (COVID-19) pandemic. Eur. J. Cancer 2020, 135, 147–149. [Google Scholar] [CrossRef]
- Di Giacomo, A.M.; Gambale, E.; Monterisi, S.; Valente, M.; Maio, M. SARS-COV-2 infection in patients with cancer undergoing checkpoint blockade: Clinical course and outcome. Eur. J. Cancer 2020, 133, 1–3. [Google Scholar] [CrossRef]
- Kattan, J.; Kattan, C.; Assi, T. Do checkpoint inhibitors compromise the cancer patients’ immunity and increase the vulnerability to COVID-19 infection? Immunotherapy 2020. [Google Scholar] [CrossRef]
- Trinh, S.; Le, A.; Gowani, S.; La-Beck, N. Management of Immune-Related Adverse Events Associated with Immune Checkpoint Inhibitor Therapy: A Minireview of Current Clinical Guidelines. Asia Pac. J. Oncol. Nurs. 2019, 6, 154. [Google Scholar] [PubMed]
- Di Noia, V.; D’Aveni, A.; Squadroni, M.; Beretta, G.D.; Ceresoli, G.L. Immune checkpoint inhibitors in SARS-CoV-2 infected cancer patients: The spark that ignites the fire? Lung Cancer 2020, 145, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Wykes, M.N.; Lewin, S.R. Immune checkpoint blockade in infectious diseases. Nat. Rev. Immunol. 2018, 18, 91–104. [Google Scholar] [CrossRef] [PubMed]
- May, J.E.; Donaldson, C.; Gynn, L.; Morse, H.R. Chemotherapy-induced genotoxic damage to bone marrow cells: Long-term implications. Mutagenesis 2018, 33, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.J.; Al-Shbool, G.; Blackburn, M.; Cook, M.; Belouali, A.; Liu, S.V.; Madhavan, S.; He, A.R.; Atkins, M.B.; Gibney, G.T.; et al. Safety and efficacy of immune checkpoint inhibitors (ICIs) in cancer patients with HIV, hepatitis B, or hepatitis C viral infection. J. Immunother. Cancer 2019, 7, 353. [Google Scholar] [CrossRef]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef]
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501. [Google Scholar] [CrossRef]
- Zheng, H.-Y.; Zhang, M.; Yang, C.-X.; Zhang, N.; Wang, X.-C.; Yang, X.-P.; Dong, X.-Q.; Zheng, Y.-T. Elevated exhaustion levels and reduced functional diversity of T cells in peripheral blood may predict severe progression in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 541–543. [Google Scholar] [CrossRef]
- Li, H.; Liu, L.; Zhang, D.; Xu, J.; Dai, H.; Tang, N.; Su, X.; Cao, B. SARS-CoV-2 and viral sepsis: Observations and hypotheses. Lancet 2020, 395, 1517–1520. [Google Scholar] [CrossRef]
- Barber, D.L.; Wherry, E.J.; Masopust, D.; Zhu, B.; Allison, J.P.; Sharpe, A.H.; Freeman, G.J.; Ahmed, R. Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 2006, 439, 682–687. [Google Scholar] [CrossRef]
- Day, C.L.; Kaufmann, D.E.; Kiepiela, P.; Brown, J.A.; Moodley, E.S.; Reddy, S.; Mackey, E.W.; Miller, J.D.; Leslie, A.J.; DePierres, C.; et al. PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression. Nature 2006, 443, 350–354. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Colston, E.; Yende, S.; Crouser, E.D.; Martin, G.S.; Albertson, T.; Bartz, R.R.; Brakenridge, S.C.; Delano, M.J.; Park, P.K.; et al. Immune checkpoint inhibition in sepsis: A Phase 1b randomized study to evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of nivolumab. Intensive Care Med. 2019, 45, 1360–1371. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Colston, E.; Yende, S.; Angus, D.C.; Moldawer, L.L.; Crouser, E.D.; Martin, G.S.; Coopersmith, C.M.; Brakenridge, S.; Mayr, F.B.; et al. Immune Checkpoint Inhibition in Sepsis. Crit. Care Med. 2019, 47, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Chong, C.R.; Park, V.J.; Cohen, B.; Postow, M.A.; Wolchok, J.D.; Kamboj, M. Safety of Inactivated Influenza Vaccine in Cancer Patients Receiving Immune Checkpoint Inhibitors. Clin. Infect. Dis. 2020, 70, 193–199. [Google Scholar] [CrossRef]
- Bayle, A.; Khettab, M.; Lucibello, F.; Chamseddine, A.N.; Goldschmidt, V.; Perret, A.; Ropert, S.; Scotté, F.; Loulergue, P.; Mir, O. Immunogenicity and safety of influenza vaccination in cancer patients receiving checkpoint inhibitors targeting PD-1 or PD-L1. Ann. Oncol. 2020, 31, 959–961. [Google Scholar] [CrossRef]
- Caruana, G.; Croxatto, A.; Coste, A.T.; Opota, O.; Lamoth, F.; Jaton, K.; Greub, G. Diagnostic strategies for SARS-CoV-2 infection and interpretation of microbiological results. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Falzone, L.; Musso, N.; Gattuso, G.; Bongiorno, D.; Palermo, C.; Scalia, G.; Libra, M.; Stefani, S. Sensitivity assessment of droplet digital PCR for SARS-CoV-2 detection. Int. J. Mol. Med. 2020, 46, 957–964. [Google Scholar] [CrossRef]
- Yu, F.; Yan, L.; Wang, N.; Yang, S.; Wang, L.; Tang, Y.; Gao, G.; Wang, S.; Ma, C.; Xie, R.; et al. Quantitative Detection and Viral Load Analysis of SARS-CoV-2 in Infected Patients. Clin. Infect. Dis. 2020, 71, 793–798. [Google Scholar] [CrossRef]
- World Health Organization (WHO). COVID-2019 Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 23 June 2020).



{kind=link}
{kind=link}
| NCT Number | Title | Interventions | Gender | Phases | Enrollment |
|---|---|---|---|---|---|
| NCT04392128 | Study Evaluating the Efficacy of Hydroxychloroquine and Azithromycine in Patients With COVID-19 and Hematological Malignancies | Hydroxychloroquine; Azithromycin; Placebo | All | Phase 2 | 114 |
| NCT04341207 | Epidemiology of SARS-CoV-2 and Mortality to COVID-19 Disease in French Cancer Patients | Hydroxychloroquine; Azithromycin | All | Phase 2 | 1000 |
| NCT04447235 | Early Treatment With Ivermectin and Losartan for Cancer Patients With COVID-19 Infection | Ivermectin; Losartan; Placebo | All | Phase 2 | 176 |
| NCT04442048 | Immunization With IMM-101 vs. Observation for Prevention of Respiratory and Severe COVID-19 Related Infections in Cancer Patients at Increased Risk of Exposure | IMM-101 | All | Phase 3 | 1500 |
| NCT04333914 | Prospective Study in Patients With Advanced or Metastatic Cancer and SARS-CoV-2 Infection | Chloroquine analog (GNS651); Nivolumab; Tocilizumab; Avdoralimab; Monalizumab | All | Phase 2 | 384 |
| NCT04419623 | A Study of TL-895 With Standard Available Treatment Versus Standard Available Treatment for the Treatment of COVID-19 in Patients With Cancer | TL-895; Placebo | All | Phase 1|Phase 2 | 146 |
| NCT04379518 | Rintatolimod and IFN Alpha-2b for the Treatment of Mild or Moderate COVID-19 Infection in Cancer Patients | Recombinant Interferon Alfa-2b; Rintatolimod | All | Phase 1|Phase 2 | 80 |
| NCT03648372 | Evaluation of TAK-981 in Patients With Advanced or Metastatic Solid Tumors or Relapsed/Refractory Hematologic Malignancies and in a Subset With COVID-19 | TAK-981 | All | Phase 1 | 80 |
| NCT04370834 | Tocilizumab for Patients With Cancer and COVID-19 Disease | Tocilizumab | All | Phase 2 | 217 |
| NCT04369365 | Prophylactic Treatment With Oral Azithromycin Versus Placebo in Cancer Patients Undergoing Antineoplastic Treatment During the COVID-19 Pandemic | Azithromycin; Placebo | All | Phase 2 | 200 |
| NCT04404361 | PRE-VENT Study in Hospitalized Patients With Severe COVID-19 With or Without Cancer | Pacritinib; Placebo | All | Phase 3 | 358 |
| NCT04381988 | A Study of Hydroxychloroquine vs. Placebo to Prevent COVID-19 Infection in Patients Receiving Radiotherapy | Hydroxychloroquine; Placebo; Radiation | All | Phase 2 | 132 |
| NCT04384588 | COVID19-Convalescent Plasma for Treating Patients With Active Symptomatic COVID 19 Infection | Convalescent Plasma from COVID-19 donors | All | Phase 2|Phase 3 | 100 |
| NCT04426201 | InterLeukin-7 to Improve Clinical Outcomes in Lymphopenic Patients With COVID-19 | CYT107; Placebo | All | Phase 2 | 48 |
| NCT04394182 | Ultra Low Doses of Therapy With Radiation Applicated to COVID-19 | Low-dose radiotherapy; Lopinavir/ritonavir; Hydroxychloroquine; Azithromycin; Piperacillin/tazobactam; Low molecular weight heparin; Corticosteroid injection; Tocilizumab | All | na | 15 |
| NCT04439006 | Ibrutinib for the Treatment of COVID-19 in Patients Requiring Hospitalization | Ibrutinib | All | Phase 2 | 72 |
| NCT04446429 | Anti-Androgen Treatment for COVID-19 | Dutasteride; Ivermectin; Azithromycin | Male | na | 254 |
| NCT04445337 | Stellate Ganglion Blockade in COVID-19 Positive Patients | Stellate Ganglion Block | All | na | 10 |
| NCT04377659 | Tocilizumab for Prevention of Respiratory Failure in Patients With Severe COVID-19 Infection | Tocilizumab | All | Phase 2 | 40 |
| NCT04379492 | A Study of Hydroxycholoroquine Compared to Placebo as Treatment for People With COVID-19 | Hydroxychloroquine; Placebo | All | Phase 2 | 120 |
| NCT04402840 | Stellate Ganglion Block (SGB) for COVID-19 Acute Respiratory Distress Syndrome (ARDS) | Stellate Ganglion Block | All | na | 5 |
| NCT04341480 | The Safety of Chemotherapy for Patients With Gynecological Malignancy in High-risk Region of COVID-19 | Chemotherapy | Female | na | 207 |
| NCT04344002 | Lung Cancer Patients and COVID-19 | Observational | All | na | 200 |
| NCT04382495 | The Impact of COVID-19 Pandemic on Cancer Care | Observational | All | na | 200 |
| NCT04389996 | COVID-19 Pandemic Impact on Patients With Cancer—A Danish Survey | Observational | All | na | 5000 |
| NCT04367870 | COVID-19 Detection Test in Oncology | Observational | All | na | 2500 |
| NCT04354701 | COVID-19 and Cancer Consortium Registry (CCC19) | Observational | All | na | 1000 |
| NCT04330521 | Impact of the Coronavirus (COVID-19) on Patients With Cancer | Observational | All | na | 50 |
| NCT04407143 | Study of the Immunity of Patients With Lung Cancer and COVID-19 Infection | Observational | All | na | 1000 |
| NCT04393974 | COVID-19 and Cancer Patients | Observational | All | na | 1000 |
| NCT04406844 | An Observational Study to Identify the Issues and Challenges in Cancer Patients on Active Treatment During the COVID-19 Pandemic and the Resulting Lockdown | Observational | All | na | 150 |
| NCT04384926 | Outcomes of Elective Cancer Surgery During the COVID-19 Pandemic Crisis | Observational | All | na | 1000 |
| NCT04427280 | Cancer: Rapid Diagnostics and Immune Assessment for SARS-CoV-2 (COVID-19) | Observational | All | na | 60 |
| NCT04340219 | Oncology-patient-reported Anxiety, Mood, and QoL During the COVID-19 Pandemic | Observational | All | na | 394 |
| NCT04352556 | COVID19-hematological Malignancies: The Italian Hematology Alliance | Observational | All | na | 250 |
| NCT04408339 | COVID-19 in Cancer Patients: Evaluation of Clinical Course and Impact on Oncological Care Including Biobanking | Observational | All | na | 500 |
| NCT04387656 | NCI COVID-19 in Cancer Patients, NCCAPS Study | Observational | All | na | 2000 |
| NCT04380766 | Covid-19 Pandemic and Pancreatic Surgery in Italy | Observational | All | na | 700 |
| NCT04432870 | Patients’ Preferences About Rescheduling Colonoscopies Delayed Due to COVID-19: Cross Sectional Study | Observational | All | na | 200 |
| NCT04447222 | Impact of the COVID-19 Pandemic and HRQOL in Cancer Patients and Survivors | Observational | All | na | 1242 |
| NCT04385160 | Myeloproliferative Neoplasms (MPN) and COVID-19 | Observational | All | na | 80 |
| NCT04433871 | COVID-19 in Pediatric Oncology and Hematology Centers in France | Observational | All | na | 300 |
| NCT04351139 | Impact of the COVID-19 Pandemic in Gynecological Oncology | Observational | Female | na | 400 |
| NCT04445870 | Dramatic Changes in Oncology Care Pathway During COVID-19 Pandemic: The French ONCOCARE-COV Study | Observational | All | na | 100 |
| NCT04366154 | Impact of the COVID-19 on the Management of Oncology and Onco-hematology Patients and on the Psychological Consequences for Patients and Caregivers | Observational | All | na | 385 |
| NCT04444401 | Registry on NEN Patients and COVID-19 | Observational | All | na | 50 |
| NCT04374838 | Effect of COVID-19 Pandemic on Pediatric Cancer Care | Observational | All | na | 20 |
| NCT04363632 | Prospective Analysis of Morbi-mortality of Patients With Cancers in Active Phase of Treatment Suspected or Diagnosed of a SARS-CoV-2 Infection | Observational | All | na | 150 |
| NCT04416438 | COVID-19 Epidemic and Patients With Myeloproliferative Neoplasias | Observational | All | na | 50 |
| NCT04366219 | Impact of Confinement and Preventive Measures in Period of SARS-COV2 Infection on Patients With Lung Cancer | Observational | All | na | 2000 |
| NCT04397575 | The GCO-002 CACOVID-19 Cohort: A French Nationwide Multicenter Study of COVID-19 Infected Cancer Patients | Observational | All | na | 1000 |
| NCT04345315 | Correlative Study on Cancer Patients and Healthcare Professionals Exposed to Infection by SARS-Cov-2 | Observational | All | na | 500 |
| NCT04406571 | Reorganization of the Healthcare System During COVID-19 Pandemic: Impact on Management of Patients With Exocrine Pancreatic Cancer | Observational | All | na | 700 |
| NCT04379232 | Surgical Activity During the Covid-19 Pandemic: Results for 112 Patients in a French Tertiary Care Center | Observational | All | na | 112 |
| NCT04397614 | Mobile Health Study and Enhanced Symptom Monitoring in COVID-19 Cancer Patients | Observational | All | na | 500 |
| NCT04434261 | Oncological Surgery in Times of COVID-19: Effectiveness of Preoperative Screening for Sars-Cov-2 | Observational | All | na | 1500 |
| NCT04357574 | Assessing the System for High-Intensity Evaluation During Radiotherapy During Changes in Response to COVID-19 | Observational | All | na | 1000 |
| NCT04445402 | Pediatrics HOT COVID-19 Database in NY Tristate | Observational | All | na | 1500 |
| NCT04401124 | Status of Management of Surgery in Beijing During COVID-19 | Observational | All | na | 500 |
| NCT04389684 | Clinical and Psycho-social Impact of COVID-19 Related Confinement on Patients With Digestive Tumors | Observational | All | na | 120 |
| NCT04371315 | Risk Factors, Clinical Characteristics and Outcomes of Acute Infection With COVID-19 In Children | Observational | All | na | 400 |
| NCT04341012 | Breath Analysis Based Disease Biomarkers of COVID-19 and Other Diseases | Observational | All | na | 120 |
| NCT04385147 | Advanced Endoscopy During COVID-19 | Observational | All | na | 250 |
| NCT04352699 | Outcomes of Urological Surgery During Periods of Social COVID-19 Containment: Is it Reasonable to Limit Access to Surgical Care for All? | Observational | All | na | 120 |
| NCT04354818 | COVID-19 Outcomes Registries in Immunocompromised Individuals Australia (CORIA) | Observational | All | na | 1000 |
| NCT04434417 | Validation of an Immunochromatographic Assay for IgG/IgM Antibodies to 2019-nCoV | Observational | All | na | 1000 |
| NCT04367805 | COVID-19 Infection in Patients With Hepatocellular Carcinoma | Observational | All | na | 50 |
| NCT04391946 | Observatory of Patients With Chronic Lymphocytic Leukemia/Lymphocytic Lymphoma or Waldenstrom Disease Infected With COVID-19 | Observational | All | na | 50 |
| NCT04386512 | Clinical Epidemiology and Characteristics Of COVID-19 Cases Occurred In A Lymphoma Setting In The First Epidemic Phase | Observational | All | na | 50 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vivarelli, S.; Falzone, L.; Grillo, C.M.; Scandurra, G.; Torino, F.; Libra, M. Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers 2020, 12, 2237. https://doi.org/10.3390/cancers12082237
Vivarelli S, Falzone L, Grillo CM, Scandurra G, Torino F, Libra M. Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers. 2020; 12(8):2237. https://doi.org/10.3390/cancers12082237
Chicago/Turabian StyleVivarelli, Silvia, Luca Falzone, Caterina Maria Grillo, Giuseppa Scandurra, Francesco Torino, and Massimo Libra. 2020. "Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial?" Cancers 12, no. 8: 2237. https://doi.org/10.3390/cancers12082237
APA StyleVivarelli, S., Falzone, L., Grillo, C. M., Scandurra, G., Torino, F., & Libra, M. (2020). Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers, 12(8), 2237. https://doi.org/10.3390/cancers12082237