Prognostic Significance of PET/CT in Patients with Chronic Lymphocytic Leukemia (CLL) Treated with Frontline Chemoimmunotherapy

 , ,
, ,  , , , ,
, , , ,  ,
, 

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. PET/CT and Biopsy
2.3. Distribution of Clinical and Biologic Characteristics According to the SUVmax Value
2.4. Outcomes of Patients According to the SUVmax Values
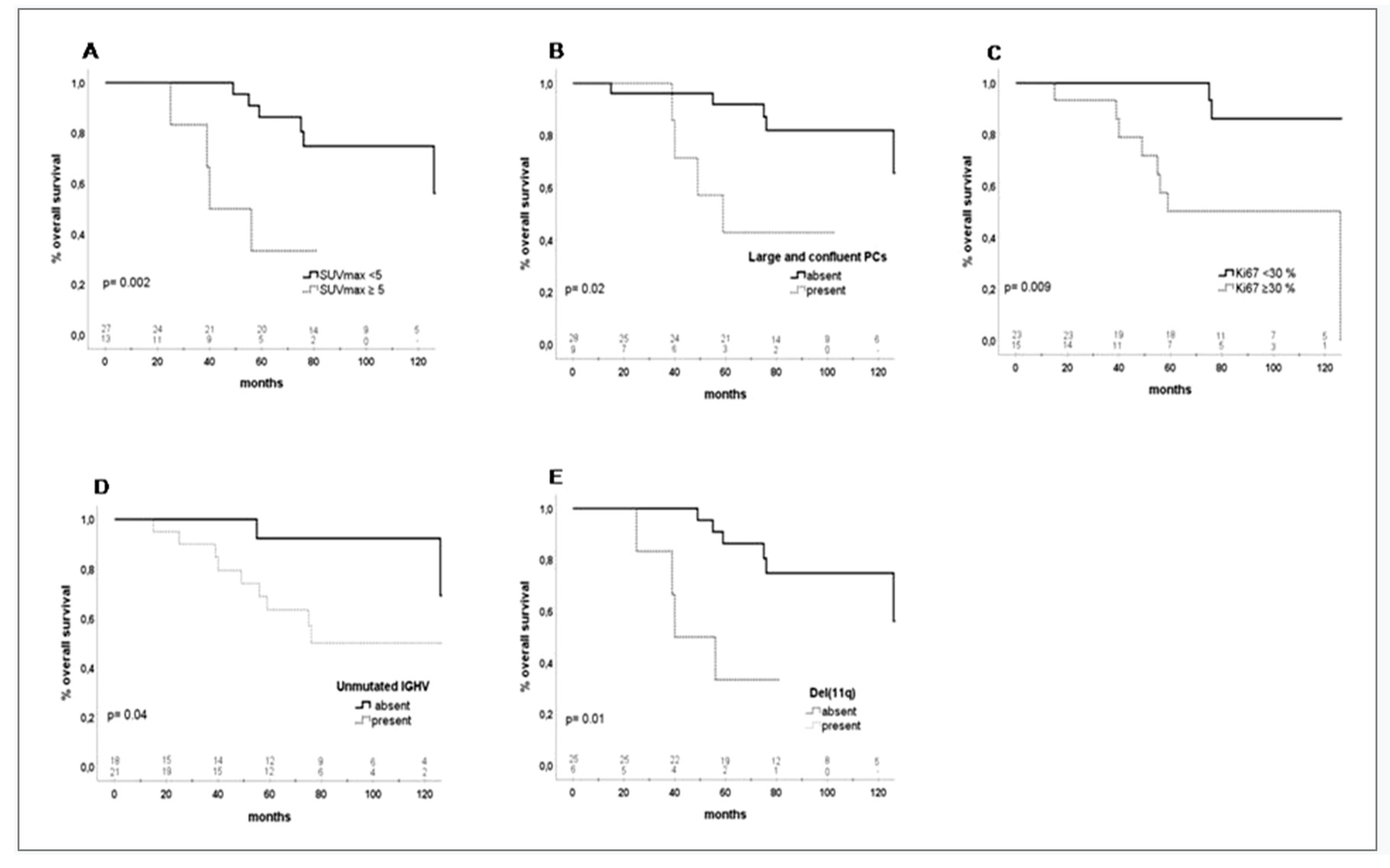
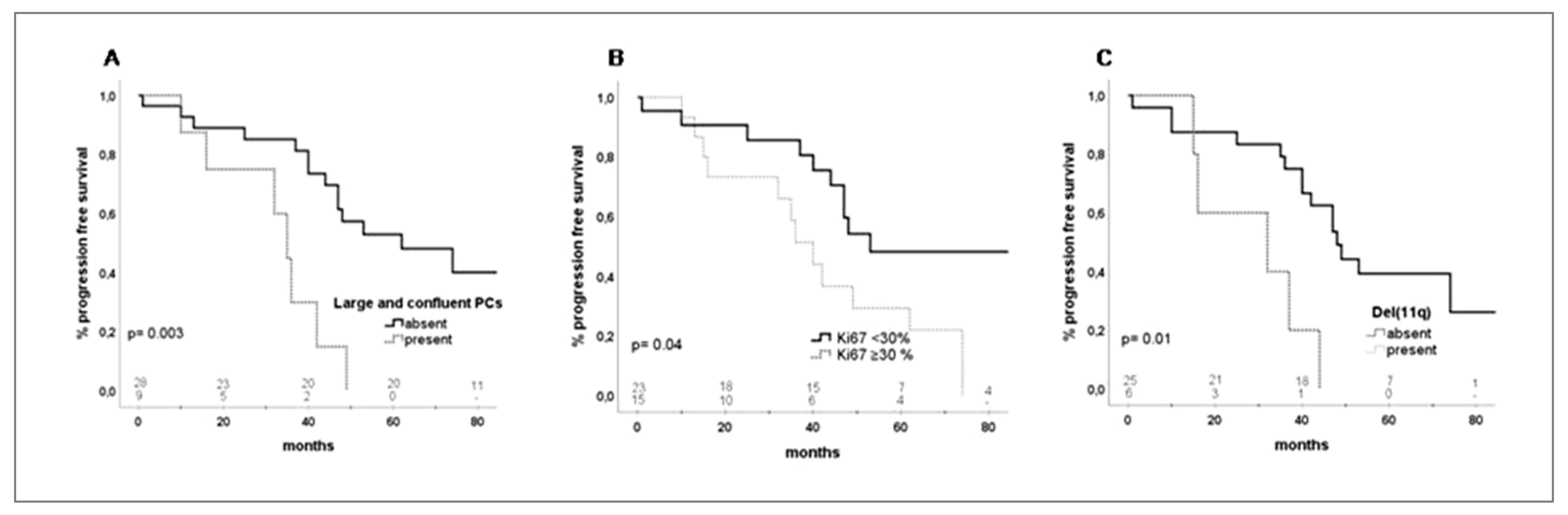
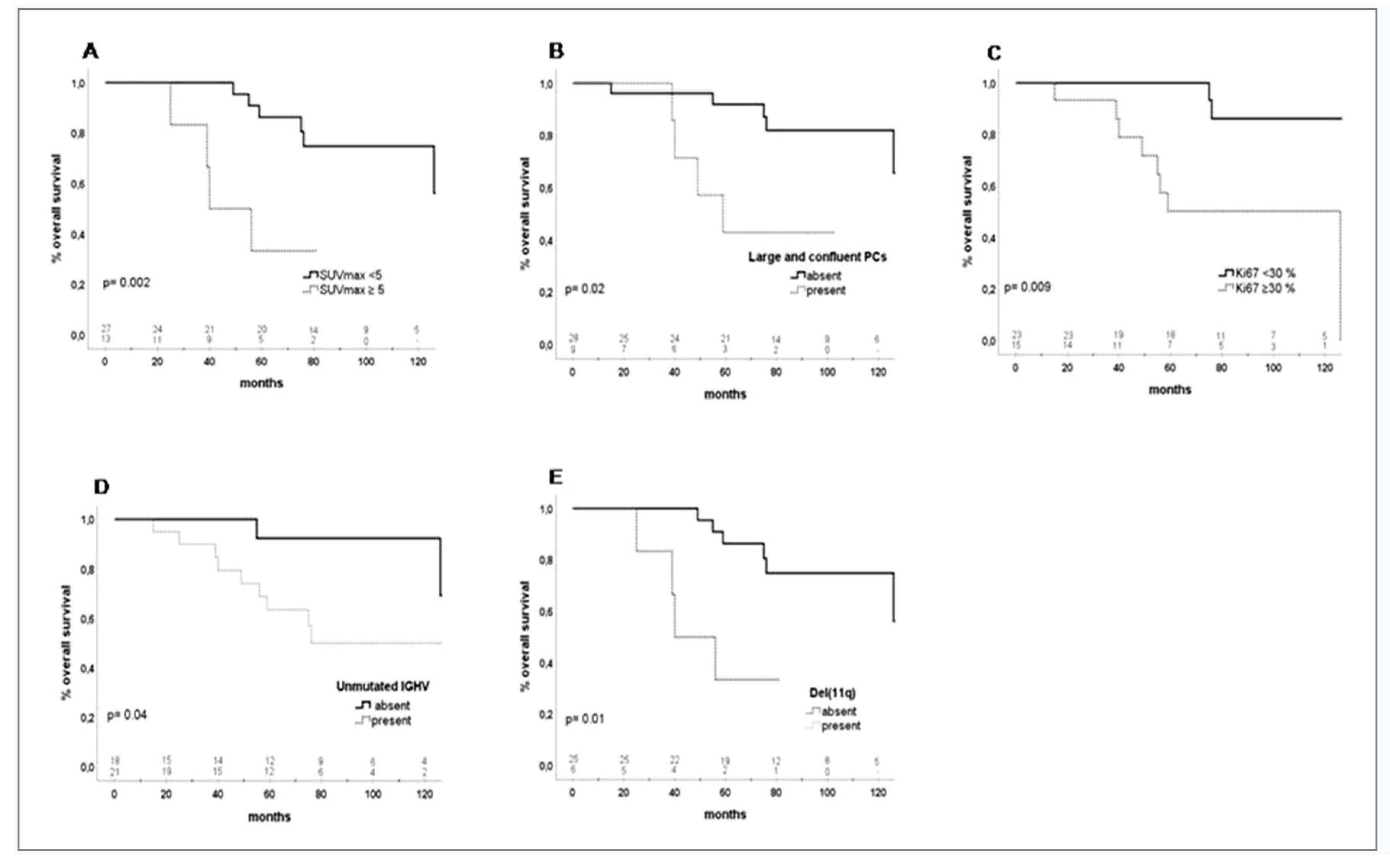
2.5. Survival
3. Discussion
4. Methods
4.1. Patients Population
4.2. PET/CT Imaging
4.3. Histologic Analysis
4.4. Statistical Analysis
4.5. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yee, K.W.; O’Brien, S.M. Chronic Lymphocytic Leukemia: Diagnosis and Treatment. Mayo Clin. Proc. 2006, 81, 1105–1129. [Google Scholar] [CrossRef] [Green Version]
- Rossi, D.; Spina, V.; Gaïdano, G. Biology and treatment of Richter syndrome. Blood 2018, 131, 2761–2772. [Google Scholar] [CrossRef] [Green Version]
- Rossi, D.; Gaïdano, G. Richter syndrome: Pathogenesis and management. Semin. Oncol. 2016, 43, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, G.; Khiabanian, H.; Holmes, A.B.; Wang, J.; Messina, M.; Mullighan, C.G.; Pasqualucci, L.; Rabadan, R.; Dalla-Favera, R. Genetic lesions associated with chronic lymphocytic leukemia transformation to Richter syndrome. J. Exp. Med. 2013, 210, 2273–2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruzzi, J.F.; Macapinlac, H.; Tsimberidou, A.M.; Truong, M.T.; Keating, M.J.; Marom, E.M.; Munden, R. Detection of Richter’s transformation of chronic lymphocytic leukemia by PET/CT. J. Nucl. Med. 2006, 47, 1267–1273. [Google Scholar] [PubMed]
- Falchi, L.; Keating, M.J.; Marom, E.M.; Truong, M.T.; Schlette, E.J.; Sargent, R.L.; Trinh, L.; Wang, X.; Smith, S.C.; Jain, N.; et al. Correlation between FDG/PET, histology, characteristics, and survival in 332 patients with chronic lymphoid leukemia. Blood 2014, 123, 2783–2790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conte, M.J.; Bowen, D.A.; Wiseman, G.A.; Rabe, K.G.; Slager, S.L.; Schwager, S.M.; Call, T.G.; Viswanatha, D.S.; Zent, C.S. Use of Positron Emission Tomography-Computerized Tomography (PET-CT) in the Management of Patients with Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL). Leuk. Lymphoma 2014, 55, 2079–2084. [Google Scholar] [CrossRef] [Green Version]
- Mauro, F.R.; Chauvie, S.; Paoloni, F.; Biggi, A.; Cimino, G.; Rago, A.; Gentile, M.; Morabito, F.; Coscia, M.; Bello, M.; et al. Diagnostic and prognostic role of PET/CT in patients with chronic lymphocytic leukemia and progressive disease. Leukemia 2015, 29, 1360–1365. [Google Scholar] [CrossRef]
- Michallet, A.-S.; Sesques, P.; Rabe, K.G.; Itti, E.; Tordot, J.; Tychyj-Pinel, C.; Baseggio, L.; Subtil, F.; Salles, G.; Dupuis, J.M.; et al. An 18F-FDG-PET maximum standardized uptake value > 10 represents a novel valid marker for discerning Richter’s Syndrome. Leuk. Lymphoma 2016, 57, 1474–1477. [Google Scholar] [CrossRef]
- Boellaard, R. Standards for PET Image Acquisition and Quantitative Data Analysis. J. Nucl. Med. 2009, 50, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Makris, N.E.; Huisman, M.C.; Kinahan, P.E.; Lammertsma, A.A.; Boellaard, R. Evaluation of strategies towards harmonization of FDGPET/CT studies in multicentretrials: Comparison of scanner validation phantoms and data analysis procedures. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1507–1515. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumor imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A.; Alliance, Australasian Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group; European Mantle Cell Lymphoma Consortium; et al. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3067. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Maillard, I.; Schuster, S.J.; Alavi, A. Utility of fluorodeoxyglucose-PET imaging in the management of patients with Hodgkin’s and non-Hodgkin’s lymphomas. Radiol. Clin. N. Am. 2004, 42, 1083–1100. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.; Ell, P.; Linch, D.C. The role of PET imaging in lymphoma. Br. J. Haematol. 2004, 126, 772–784. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.M.; Mato, A.R. PET/Computed Tomography in Chronic Lymphocytic Leukemia and Richter Transformation. PET Clin. 2019, 14, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.; Agostinelli, C.; Rigolin, G.M.; Piccaluga, P.P.; Cavazzini, F.; Righi, S.; Sista, M.T.; Sofritti, O.; Rizzotto, L.; Sabattini, E.; et al. Proliferation centers in chronic lymphocytic leukemia: Correlation with cytogenetic and clinicobiological features in consecutive patients analyzed on tissue microarrays. Leukemia 2011, 26, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Giné, E.; Martinez, A.; Villamor, N.; López-Guillermo, A.; Camos, M.; Martinez, D.; Esteve, J.; Calvo, X.; Muntañola, A.; Abrisqueta, P.; et al. Expanded and highly active proliferation centers identify a histologic subtype of chronic lymphocytic leukemia (“accelerated” chronic lymphocytic leukemia) with aggressive clinical behavior. Haematologica 2010, 95, 1526–1533. [Google Scholar] [CrossRef]
- Döhner, H.; Stilgenbauer, S.; James, M.R.; Benner, A.; Weilguni, T.; Bentz, M.; Fischer, K.; Hunstein, W.; Lichter, P. 11q Deletions Identify a New Subset of B-Cell Chronic Lymphocytic Leukemia Characterized by Extensive Nodal Involvement and Inferior Prognosis. Blood 1997, 89, 2516–2522. [Google Scholar] [CrossRef]
- Mato, A.R.; Wierda, W.G.; Davids, M.S.; Cheson, B.D.; Coutre, S.E.; Choi, M.; Furman, R.R.; Heffner, L.; Barr, P.M.; Eradat, H.; et al. Utility of positron emission tomography-computed tomography in patients with chronic lymphocytic leukemia following B-cell receptor pathway inhibitor therapy. Haematologica 2019, 104, 2258–2264. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Rabe, K.G.; Bold, M.S.; Shi, M.; Hanson, C.A.; Schwager, S.M.; Call, T.G.; Kenderian, S.S.; Muchtar, E.; Hayman, S.R.; et al. The role of 18F-FDG FDG PET in detecting Richter’s transformation of chronic lymphocytic leukemia in patients receiving therapy with a B-cell receptor inhibitor. Haematologica 2020. [Google Scholar] [CrossRef] [PubMed]
- Balogh, Z.; Reiniger, L.; Rajnai, H.; Csomor, J.; Szepesi, A.; Balogh, A.; Deák, L.; Gagyi, E.; Bödör, C.; Matolcsy, A. High rate of neoplastic cells with genetic abnormalities in proliferation centers of chronic lymphocytic leukemia. Leuk. Lymphoma 2011, 52, 1080–1084. [Google Scholar] [CrossRef] [PubMed]
- Herishanu, Y.; Pérez-Galán, P.; Liu, D.; Biancotto, A.; Pittaluga, S.; Vire, B.; Gibellini, F.; Njuguna, N.; Lee, E.; Stennett, L.; et al. The lymph node microenvironment promotes B-cellreceptor signaling, NF-kappaB activation, and tumor proliferation in chronic lymphocytic leukemia. Blood 2011, 117, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Hallek, M.; Cheson, B.D.; Catovsky, D.; Caligaris-Cappio, F.; Dighiero, G.; Döhner, H.; Hillmen, P.; Keating, M.J.; Montserrat, E.; Rai, K.R.; et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: A report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute—Working Group 1996 guidelines. Blood 2008, 111, 5446–5456. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Tested Variables | All Patients n (%) | SUVmax ≥ 5 n (%) | SUVmax < 5 n (%) | p Value |
|---|---|---|---|---|
| 40 (100) | 13 (33) | 27 (67) | - | |
| Age | ||||
| ≥65 years | 14 (35) | 6 (46) | 8 (30) | 0.30 |
| <65 years | 26 (65) | 7 (54) | 19 (70) | |
| Sex | ||||
| Male | 31 (78) | 12 (92) | 19 (70) | 0.12 |
| Female | 9 (22) | 1(8) | 8 (30) | |
| Binet stage | ||||
| A+B | 34 (85) | 11 (85) | 23 (85) | 0.96 |
| C | 6 (15) | 4 (15) | 2 (15) | |
| B symptoms | ||||
| Present | 11 (28) | 3 (23) | 8 (30) | 0.66 |
| Absent | 29 (72) | 10 (77) | 19 (70) | |
| LDH | ||||
| Normal | 13 (33) | 6 (50) | 20 (74) | 0.14 |
| Increased | 26 (67) | 6 (50) | 7 (26) | |
| Beta 2 microglobulin | ||||
| ≥3.5 mg/L | 21 (58) | 4 (40) | 11 (42) | 0.9 |
| <3.5 mg/L | 15 (42) | 6 (60) | 15 (58) | |
| Lymph nodes diameter | ||||
| ≥5 cm | 17 (46) | 8 (62) | 9 (38) | 0.16 |
| <5 cm | 20 (54) | 5 (38) | 15 (62) | |
| Large and confluent PCs | ||||
| Present | 9 (24) | 4 (36) | 5 (19) | 0.26 |
| Absent | 28 (76) | 7 (64) | 21 (81) | |
| Ki67% | ||||
| ≥30% | 15 (40) | 8 (67) | 7 (27) | 0.02 |
| <30% | 23 (60) | 4 (33) | 19 (73) | |
| CD38 positive | ||||
| Present | 18 (47) | 7 (58) | 11 (44) | 0.41 |
| Absent | 19 (51) | 5 (42) | 14 (56) | |
| Unmutated IGHV | ||||
| Present | 21 (54) | 9 (75) | 12 (44) | 0.07 |
| Absent | 18 (46) | 3 (25) | 15 (56) | |
| FISH b | ||||
| Del(11q) | ||||
| Present | 6 (19) | 5 (45) | 1 (5) | 0.006 |
| Absent | 25 (81) | 6 (55) | 19 (95) | |
| Trisomy 12 | ||||
| Present | 8 (26) | 4 (36) | 4 (20) | 0.32 |
| Absent | 23 (74) | 7 (64) | 16 (80) | |
| Del(13q) | ||||
| Present | 5 (16) | 1 (9) | 4 (20) | 0.43 |
| Absent | 26 (84) | 10 (91) | 16 (80) | |
| Del(17p) and/or mutated TP53 c | ||||
| Present | 7 (19) | 3 (27) | 4 (15) | 0.39 |
| Absent | 30 (81) | 8 (72) | 22 (85) | |
| Tested Variables | No. Patients n (%) | PFS | OS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 3 Year % | Median Months | p Value | HR (95% CI) | 3 Year % | Median Months | p Value | HR (95% CI) | ||
| 40 (100) | 75 | 48 | - | - | 94 | - | - | - | |
| SUVmax | |||||||||
| ≥5 | 13 (33) | 55 | 37 | 0.48 | 0.72 (0.2–1,7) | 83 | 56 | 0.002 | 0.12 (0.3–0.5) |
| <5 | 27 (67) | 79 | 49 | 100 | - | ||||
| Age | |||||||||
| ≥65 years | 14 (35) | 62 | 47 | 0.78 | 1.13 (0.4–2.7) | 84 | 126 | 0.33 | 1.81 (0.5–6) |
| <65 years | 26 (65) | 75 | 48 | 100 | - | ||||
| Sex | |||||||||
| Male | 31 (78) | 68 | 47 | 0.44 | 0.65 (0.2–1.9) | 100 | - | 0.21 | 0.02 (0–8.6) |
| Female | 9 (22) | 85 | 53 | 93 | - | ||||
| B symptoms | |||||||||
| Present | 11 (28) | 72 | 47 | 0.57 | 1.28 (0.5–3) | 100 | 126 | 0.37 | 0.50 (0.1–2.3) |
| Absent | 29 (72) | 71 | 48 | 92 | - | ||||
| Binet stage | |||||||||
| A+B | 34 (85) | 71 | 47 | 0.45 | 0.57 (0.1–2.4) | 93 | - | 0.65 | 0.62 (0.8–4.9) |
| C | 6 (15) | 75 | 49 | 100 | - | ||||
| LDH | |||||||||
| Normal | 13 (33) | 70 | 62 | 0.31 | 1.56 (0.6–3.6) | 91 | - | 0.75 | 0.80 (0.2–3.1) |
| Increased | 26 (67) | 74 | 42 | 90 | - | ||||
| Beta 2 microglobulin | |||||||||
| ≥3.5 mg/L | 21(58) | 77 | 53 | 0.31 | 6.35 (0.2–1.5) | 92 | - | 0.94 | 0.95 (0.2–3.5) |
| <3.5 mg/L | 15 (42) | 64 | 42 | 95 | - | ||||
| Lymph nodes diameter | |||||||||
| ≥5 cm | 17 (46) | 67 | 44 | 0.78 | 1.1 (0.4–2.6) | 94 | - | 0.35 | 1.7 (0.5–5.8) |
| <5 cm | 20 (54) | 73 | 47 | 93 | - | ||||
| Large and confluent PCs | |||||||||
| Present | 9 (24) | 30 | 35 | 0.003 | 4.50 (1.6–12.1) | 85 | 59 | 0.02 | 5.17 (1.2–21.1) |
| Absent | 28 (76) | 85 | 62 | 96 | 0 | ||||
| Ki67% | |||||||||
| ≥30% | 15 (40) | 58 | 40 | 0.04 | 2.41 (1–5.6) | 93 | 126 | 0.009 | 8.1 (1.7–38.6) |
| <30% | 23 (60) | 85 | 53 | 100 | - | ||||
| CD38+ | |||||||||
| Present | 18 (47) | 65 | 49 | 0.93 | 0.96 (0.3–2.4) | 92 | 126 | 0.20 | 2.19 (0.6–7.2) |
| Absent | 19 (51) | 73 | 47 | 89 | - | ||||
| Unmutated IGHV | |||||||||
| Present | 21 (54) | 59 | 40 | 0.07 | 0.43 (0.2–1) | 95 | - | 0.04 | 0.20 (0.04–0.9) |
| Absent | 18 (46) | 86 | 53 | 100 | - | ||||
| Del(17p) and or mutated TP53 | |||||||||
| Present | 7 (19) | 57 | 47 | 0.70 | 1.21 (0.4–3.3) | 83 | 126 | 0.71 | 1.31 (0.3–5.6) |
| Absent | 30 (81) | 76 | 48 | 96 | - | ||||
| Del(11q) | |||||||||
| Present | 6 (19) | 75 | 32 | 0.01 | 4.21 (1.3–13) | 83 | 40 | 0.01 | 5.49 (1.4–20.8) |
| Absent | 25 (81) | 40 | 48 | 100 | - | ||||
| Trisomy 12 | |||||||||
| Present | 8 (26) | 85 | 49 | 0.43 | 0.64 (0–1.9) | 100 | - | 0.93 | 0.40 (0.05–3.2) |
| Absent | 23 (74) | 64 | 47 | 95 | 126 | ||||
| Del(13q) | |||||||||
| Present | 4(14) | 50 | 35 | 0.20 | 2.04 (0.6–6.1) | 100 | - | 0.60 | 0.57 (0.07–4.5) |
| Absent | 27 (86) | 72 | 47 | 95 | 126 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porrazzo, M.; Nicolai, E.; Riminucci, M.; Vitale, C.; Coscia, M.; De Paoli, L.; Rago, A.; Buscicchio, G.; Maestrini, G.; Ligia, S.; et al. Prognostic Significance of PET/CT in Patients with Chronic Lymphocytic Leukemia (CLL) Treated with Frontline Chemoimmunotherapy. Cancers 2020, 12, 1773. https://doi.org/10.3390/cancers12071773
Porrazzo M, Nicolai E, Riminucci M, Vitale C, Coscia M, De Paoli L, Rago A, Buscicchio G, Maestrini G, Ligia S, et al. Prognostic Significance of PET/CT in Patients with Chronic Lymphocytic Leukemia (CLL) Treated with Frontline Chemoimmunotherapy. Cancers. 2020; 12(7):1773. https://doi.org/10.3390/cancers12071773
Chicago/Turabian StylePorrazzo, Marika, Emanuele Nicolai, Mara Riminucci, Candida Vitale, Marta Coscia, Lorenzo De Paoli, Angela Rago, Giulia Buscicchio, Giacomo Maestrini, Silvio Ligia, and et al. 2020. "Prognostic Significance of PET/CT in Patients with Chronic Lymphocytic Leukemia (CLL) Treated with Frontline Chemoimmunotherapy" Cancers 12, no. 7: 1773. https://doi.org/10.3390/cancers12071773
APA StylePorrazzo, M., Nicolai, E., Riminucci, M., Vitale, C., Coscia, M., De Paoli, L., Rago, A., Buscicchio, G., Maestrini, G., Ligia, S., Di Prima, A., Corsi, A., Caronna, R., Gaidano, G., & Mauro, F. R. (2020). Prognostic Significance of PET/CT in Patients with Chronic Lymphocytic Leukemia (CLL) Treated with Frontline Chemoimmunotherapy. Cancers, 12(7), 1773. https://doi.org/10.3390/cancers12071773