Efficacy of Panitumumab and Cetuximab in Patients with Colorectal Cancer Previously Treated with Bevacizumab; a Combined Analysis of Individual Patient Data from ASPECCT and WJOG6510G

 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Participants
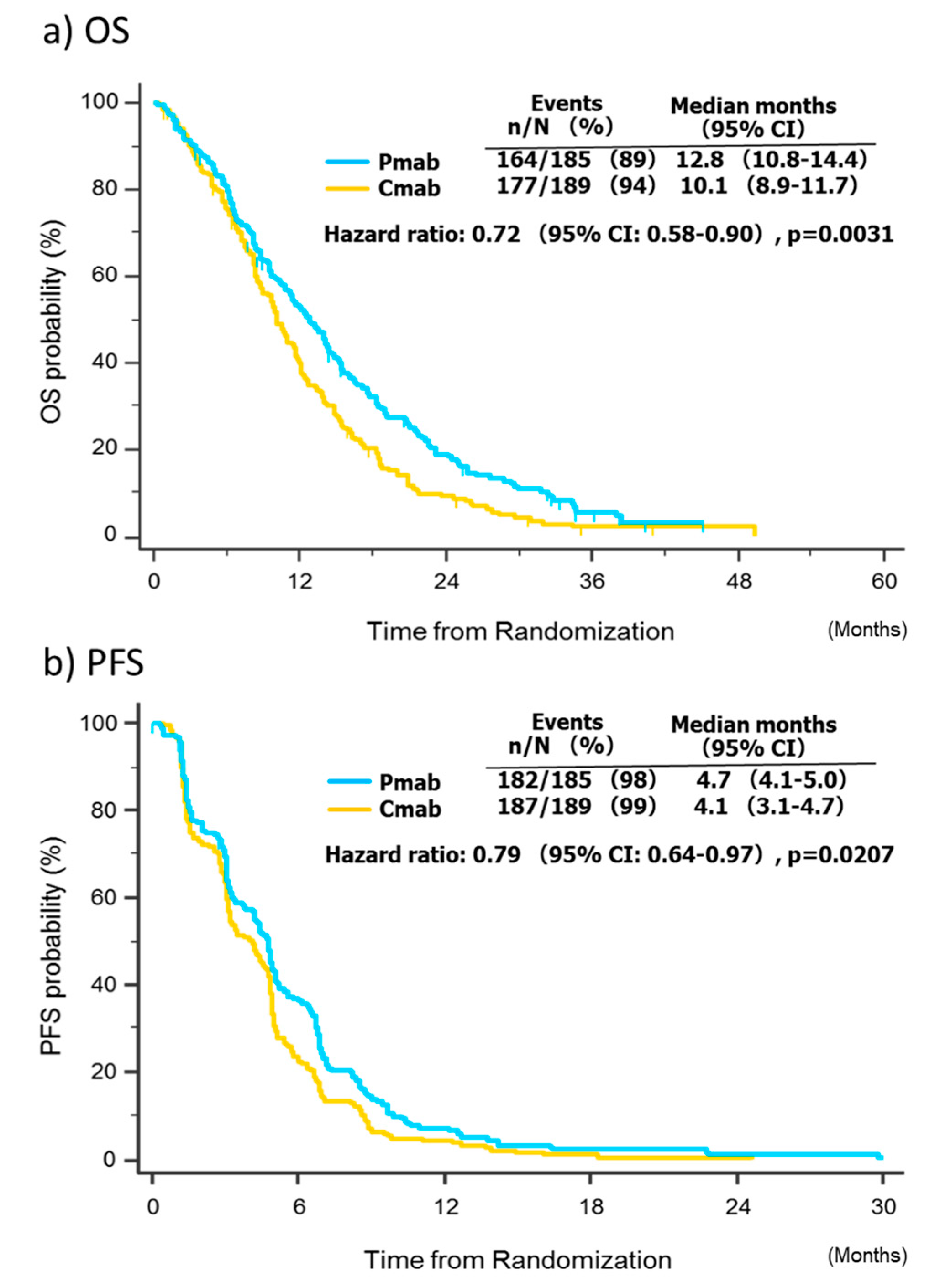
2.2. Pooled Overall Survival and Progression-Free Survival Analyses
2.3. Pooled Univariate and Multivariate Analyses of Factors Affecting Survival
2.4. Pooled Analysis of Treatment Response
2.5. Pooled Analysis of Treatment Safety
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Treatment
4.3. Efficacy and Safety Assessments
4.4. Outcomes and Definitions
4.5. Statistical Analysis of the Pooled Data
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Karapetis, C.S.; Khambata-Ford, S.; Jonker, D.J.; O’Callaghan, C.J.; Tu, D.; Tebbutt, N.C.; Simes, R.J.; Chalchal, H.; Shapiro, J.D.; Robitaille, S.M.; et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N. Engl. J. Med. 2008, 359, 1757–1765. [Google Scholar] [CrossRef]
- Amado, R.G.; Wolf, M.; Peeters, M.; Cutsem, E.V.; Siena, S.; Freeman, D.J.; Juan, T.; Sikorski, R.; Suggs, S.; Patterson, S.D.; et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 1626–1634. [Google Scholar] [CrossRef]
- Price, T.J.; Peeters, M.; Kim, T.W.; Li, J.; Cascinu, S.; Ruff, P.; Suresh, A.S.; Thomas, A.; Tjulandin, S.; Zhang, K.; et al. Panitumumab versus cetuximab in patients with chemotherapy-refractory wild-type KRAS exon 2 metastatic colorectal cancer (ASPECCT): A randomised, multicentre, open-label, non-inferiority phase 3 study. Lancet Oncol. 2014, 15, 569–579. [Google Scholar] [CrossRef]
- Price, T.; Kim, T.W.; Li, J.; Cascinu, S.; Ruff, P.; Suresh, A.S.; Thomas, A.; Tjulandin, S.; Guan, X.; Peeter, M. Final results and outcomes by prior bevacizumab exposure, skin toxicity, and hypomagnesaemia from ASPECCT: randomized phase 3 non-inferiority study of panitumumab versus cetuximab in chemorefractory wild-type KRAS exon 2 metastatic colorectal cancer. Eur. J. Cancer 2016, 68, 51–59. [Google Scholar] [CrossRef][Green Version]
- Cunningham, D.; Humblet, Y.; Siena, S.; Khayat, D.; Bleiberg, H.; Santoro, A.; Bets, D.; Mueser, M.; Harstrick, A.; Verslype, C.; et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N. Engl. J. Med. 2004, 351, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Sakai, D.; Taniguchi, H.; Sugimoto, N.; Tamura, T.; Nishina, T.; Hara, H.; Esaki, T.; Denda, T.; Sakamoto, T.; Okuda, H.; et al. Randomised phase II study of panitumumab plus irinotecan versus cetuximab plus irinotecan in patients with KRAS wild-type metastatic colorectal cancer refractory to fluoropyrimidine, irinotecan, and oxaliplatin (WJOG6510G). Eur. J. Cancer 2020, 135, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Cascinu, S.; Rosati, G.; Nasti, G.; Lonardi, S.; Zaniboni, A.; Marchetti, P.; Leone, F.; Bilancia, D.; Iaffaioli, R.V.; Zagonel, V.; et al. Treatment sequence with either irinotecan/cetuximab followed by FOLFOX-4 or the reverse strategy in metastatic colorectal cancer patients progressing after first-line FOLFIRI/bevacizumab: An Italian Group for the Study of Gastrointestinal Cancer phase III, randomised trial comparing two sequences of therapy in colorectal metastatic patients. Eur. J. Cancer 2017, 83, 106–115. [Google Scholar] [PubMed]
- Bennouna, J.; Hiret, S.; Bertaut, A.; Bouché, O.; Deplanque, G.; Borel, C.; François, E.; Conroy, T.; Ghiringhelli, F.; Guetz, G.; et al. Continuation of bevacizumab vs cetuximab plus chemotherapy after first progression in KRAS wild-type metastatic colorectal cancer: The UNICANCER PRODIGE18 Randomized Clinical Trial. JAMA Oncol. 2019, 5, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Yonesaka, K.; Denda, T.; Yamazaki, K.; Moriwaki, T.; Tsuda, M.; Takano, T.; Okuda, H.; Nishina, T.; Sakai, K.; et al. Randomized study of FOLFIRI plus either panitumumab or bevacizumab for wild-type KRAS colorectal cancer-WJOG 6210G. Cancer Sci. 2016, 107, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.D.; Jia, X.C.; Corvalan, J.R.; Wang, P.; Davis, C.G. Development of ABX-EGF, a fully human anti-EGF receptor monoclonal antibody, for cancer therapy. Crit. Rev. Oncol. Hematol. 2001, 38, 17–23. [Google Scholar] [CrossRef]
- Kearns, J.D.; Bukhalid, R.; Sevecka, M.; Tan, G.; Gerami-Moayed, N.; Werner, S.L.; Kohli, N.; Burenkova, O.; Sloss, C.M.; King, A.M.; et al. Enhanced targeting of the EGFR network with MM-151, an oligoclonal anti-EGFR antibody therapeutic. Mol. Cancer Ther. 2015, 14, 1625–1636. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Yoo, J.; Kim, M.-S.; Hur, M.; Lee, E.H.; Hur, H.-S.; Lee, J.-C.; Lee, S.-N.; Park, T.-W.; Lee, K.; et al. GC1118, an anti-EGFR antibody with a distinct binding epitope and superior inhibitory activity against high-affinity EGFR ligands. Mol. Cancer Ther. 2016, 15, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Groenestege, W.M.T.; Thébault, S.; van der Wijst, J.; van den Berg, D.; Janssen, R.; Tejpar, S.; van den Heuvel, L.P.; van Cutsem, E.; Hoenderop, J.G.; Knoers, N.V.; et al. Impaired basolateral sorting of pro-EGF causes isolated recessive renal hypomagnesemia. J. Clin. Invest. 2007, 117, 2260–2267. [Google Scholar] [CrossRef] [PubMed]
- Seligmann, J.F.; Elliott, F.; Richman, S.D.; Jacobs, B.; Hemmings, G.; Brown, S.; Barrett, J.H.; Tejpar, S.; Quirke, P.; Seymour, M.T. Combined epiregulin and amphiregulin expression levels as a predictive biomarker for panitumumab therapy benefit or lack of benefit in patients with RAS wild-type advanced colorectal cancer. JAMA Oncol. 2016, 2, 633–642. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Siena, S.; Cassidy, J.; Tabernero, J.; Burkes, R.; Barugel, M.; Humblet, Y.; Bodoky, G.; Cunningham, D.; Jassem, J.; et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: The PRIME study. J. Clin. Oncol. 2010, 28, 4697–4705. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Köhne, C.H.; Láng, I.; Folprecht, G.; Nowacki, M.P.; Cascinu, S.; Shchepotin, I.; Maurel, J.; Cunningham, D.; Tejpar, S.; et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: Updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J. Clin. Oncol. 2011, 29, 2011–2019. [Google Scholar] [CrossRef]
- Jain, R.K.; Duda, D.G.; Clark, J.W.; Loeffler, J.S. Lessons from phase III clinical trials on anti-VEGF therapy for cancer. Nat. Clin. Pract. Oncol. 2006, 3, 24–40. [Google Scholar] [CrossRef]
- Kerbel, R.; Folkman, J. Clinical translation of angiogenesis inhibitors. Nat. Rev. Cancer 2002, 2, 727–739. [Google Scholar] [CrossRef]
- Lee, C.M.; Tannock, I.F. The distribution of the therapeutic monoclonal antibodies cetuximab and trastuzumab within solid tumors. BMC Cancer 2010, 10, 255. [Google Scholar]
- Arnold, D.; Lueza, B.; Douillard., J.Y.; Peeters, M.; Lenz, H.J.; Venook, A.; Heinemann, V.; Cutsem, E.V.; Pignon, J.-P.; Tabernero, J.; et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef]
- Cremolini, C.; Rossini, D.; Dell’Aquila, E.; Lonardi, S.; Conca, E.; Del Re, M.; Busico, A.; Pietrantonio, F.; Danesi, R.; Aprile, G.; et al. Rechallenge for patients with RAS and BRAF wild-type metastatic colorectal cancer with acquired resistance to first-line cetuximab and irinotecan: A phase 2 single-arm clinical trial. JAMA Oncol. 2019, 5, 343–350. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics, n (%). | Panitumumab | Cetuximab | ||||
|---|---|---|---|---|---|---|
| N = 185 | N = 189 | p-Value | ||||
| Age | Median (Range) | 61 | (32–80) | 62 | (26–82) | 0.84 |
| <65 years | 119 | (64.3%) | 117 | (61.9%) | 0.63 | |
| ≥65 years | 66 | (35.7%) | 72 | (38.1%) | ||
| Sex | Male | 127 | (68.6%) | 112 | (59.3%) | 0.059 |
| Female | 58 | (31.4%) | 77 | (40.7%) | ||
| ECOG PS | 0 | 81 | (43.9%) | 83 | (43.8%) | |
| 1 | 92 | (48.7%) | 92 | (49.7%) | 0.93 | |
| 2 | 12 | (6.5%) | 14 | (7.4%) | ||
| Tumour location | Colon | 114 | (61.6%) | 120 | (63.5%) | 0.71 |
| Rectum | 71 | (38.4%) | 69 | (36.5%) | ||
| Prior surgery | Yes | 168 | (90.8%) | 172 | (91.0%) | 1.0 |
| No | 17 | (9.2%) | 17 | (9.0%) | ||
| Number of metastatic sites | 1–2 | 113 | (61.1%) | 130 | (68.8%) | 0.13 |
| ≥3 | 72 | (38.9%) | 59 | (31.2%) | ||
| Liver metastasis only | Yes | 24 | (13.0%) | 30 | (15.9%) | 0.46 |
| No | 161 | (87.0%) | 159 | (84.1%) | ||
| CEA | Median (ng/mL) | 90.50 | 55.70 | 0.028 | ||
| <50 | 71 | (39.9%) | 90 | (48.9%) | 0.091 | |
| ≥50 | 107 | (60.1%) | 94 | (51.1%) | ||
| Univariate analysis for OS | ||||
| Factor | Category | N | Median OS (m) | p-Value |
| Age | <65/≥65 | 236/138 | 10.09/13.44 | 0.077 |
| Sex | F/M | 135/239 | 10.87/11.63 | 0.72 |
| ECOG PS | 0–1/2 | 348/26 | 11.92/4.62 | <0.0001 |
| Tumour location | Colon/Rectum | 234/140 | 11.27/11.93 | 0.42 |
| Prior surgery | No/Yes | 34/340 | 8.71/11.63 | 0.29 |
| No. of mets | 1–2/≥3 | 243/131 | 12.81/8.71 | 0.00014 |
| Liver met only | No/Yes | 320/54 | 11.01/12.35 | 0.67 |
| CEA | <50/≥50 (ng/mL) | 161/201 | 13.27/10.51 | 0.0036 |
| Study | ASPECCT/WJOG | 258/116 | 10.35/12.81 | 0.29 |
| Regimen | Cmab/Pmab | 189/185 | 10.09 / 13.27 | 0.0077 |
| Multivariate analysis for OS | ||||
| Factor | Category | HR | 95%CI | p-Value |
| ECOG PS | 0–1 vs. 2 | 2.50 | 1.62–3.84 | <0.0001 |
| No. of mets | 1–2 vs. ≥3 | 1.57 | 1.22–2.00 | 0.00030 |
| CEA | <50 vs. ≥50 (ng/mL) | 1.32 | 1.03–1.67 | 0.023 |
| Regimen | Cmab vs. Pmab | 0.69 | 0.54–0.87 | 0.0013 |
| CTCAE v 4.0 | Panitumumab | Cetuximab | p-Value a | |||
|---|---|---|---|---|---|---|
| N = 184 | N = 188 | |||||
| Skin toxicity b | Any grade | 165 | (89.7%) | 165 | (87.8%) | 0.625 |
| Grade ≥ 3 | 25 | (13.6%) | 18 | (9.6%) | 0.258 | |
| Infusion reaction c | Any grade | 2 | (1.1%) | 16 | (8.5%) | 0.0054 |
| Grade ≥ 3 | 0 | (0%) | 4 | (2.1%) | 0.2440 | |
| Hypomagnesemia | Any grade | 86 | (47.0%) d | 60 | (32.0%) | 0.0040 |
| Grade ≥ 3 | 22 | (12.0%) d | 7 | (3.7%) | 0.0033 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taniguchi, H.; Yamanaka, T.; Sakai, D.; Muro, K.; Yamazaki, K.; Nakata, S.; Kimura, H.; Ruff, P.; Kim, T.W.; Peeters, M.; et al. Efficacy of Panitumumab and Cetuximab in Patients with Colorectal Cancer Previously Treated with Bevacizumab; a Combined Analysis of Individual Patient Data from ASPECCT and WJOG6510G. Cancers 2020, 12, 1715. https://doi.org/10.3390/cancers12071715
Taniguchi H, Yamanaka T, Sakai D, Muro K, Yamazaki K, Nakata S, Kimura H, Ruff P, Kim TW, Peeters M, et al. Efficacy of Panitumumab and Cetuximab in Patients with Colorectal Cancer Previously Treated with Bevacizumab; a Combined Analysis of Individual Patient Data from ASPECCT and WJOG6510G. Cancers. 2020; 12(7):1715. https://doi.org/10.3390/cancers12071715
Chicago/Turabian StyleTaniguchi, Hiroya, Takeharu Yamanaka, Daisuke Sakai, Kei Muro, Kentaro Yamazaki, Susumu Nakata, Hiroyuki Kimura, Paul Ruff, Tae Won Kim, Marc Peeters, and et al. 2020. "Efficacy of Panitumumab and Cetuximab in Patients with Colorectal Cancer Previously Treated with Bevacizumab; a Combined Analysis of Individual Patient Data from ASPECCT and WJOG6510G" Cancers 12, no. 7: 1715. https://doi.org/10.3390/cancers12071715
APA StyleTaniguchi, H., Yamanaka, T., Sakai, D., Muro, K., Yamazaki, K., Nakata, S., Kimura, H., Ruff, P., Kim, T. W., Peeters, M., & Price, T. (2020). Efficacy of Panitumumab and Cetuximab in Patients with Colorectal Cancer Previously Treated with Bevacizumab; a Combined Analysis of Individual Patient Data from ASPECCT and WJOG6510G. Cancers, 12(7), 1715. https://doi.org/10.3390/cancers12071715