Benefits of Conversion Surgery after Multimodal Treatment for Unresectable Pancreatic Ductal Adenocarcinoma

 ,
, 
Abstract
1. Introduction
2. Patients and Methods
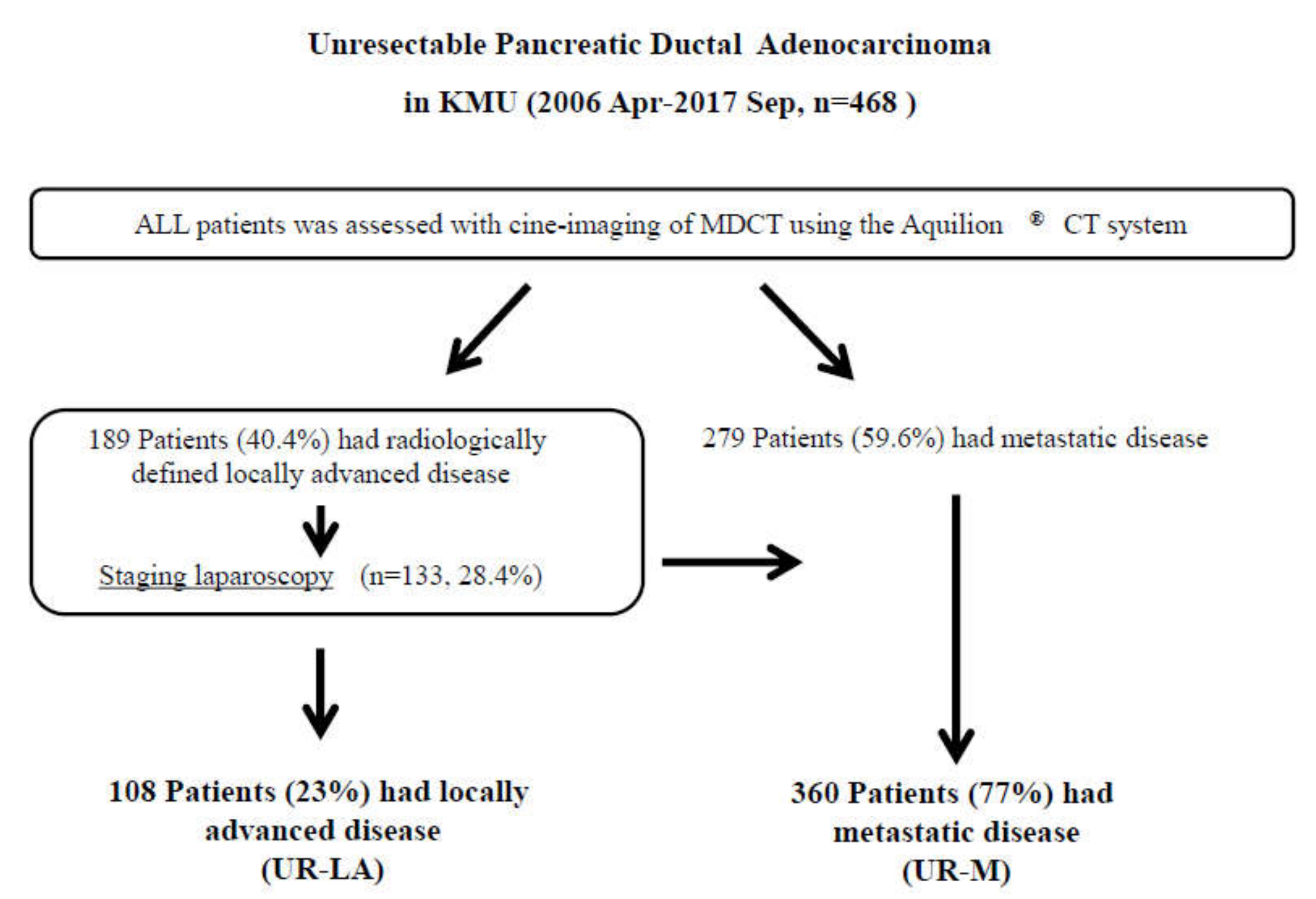
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Best Response After First-Line Treatment
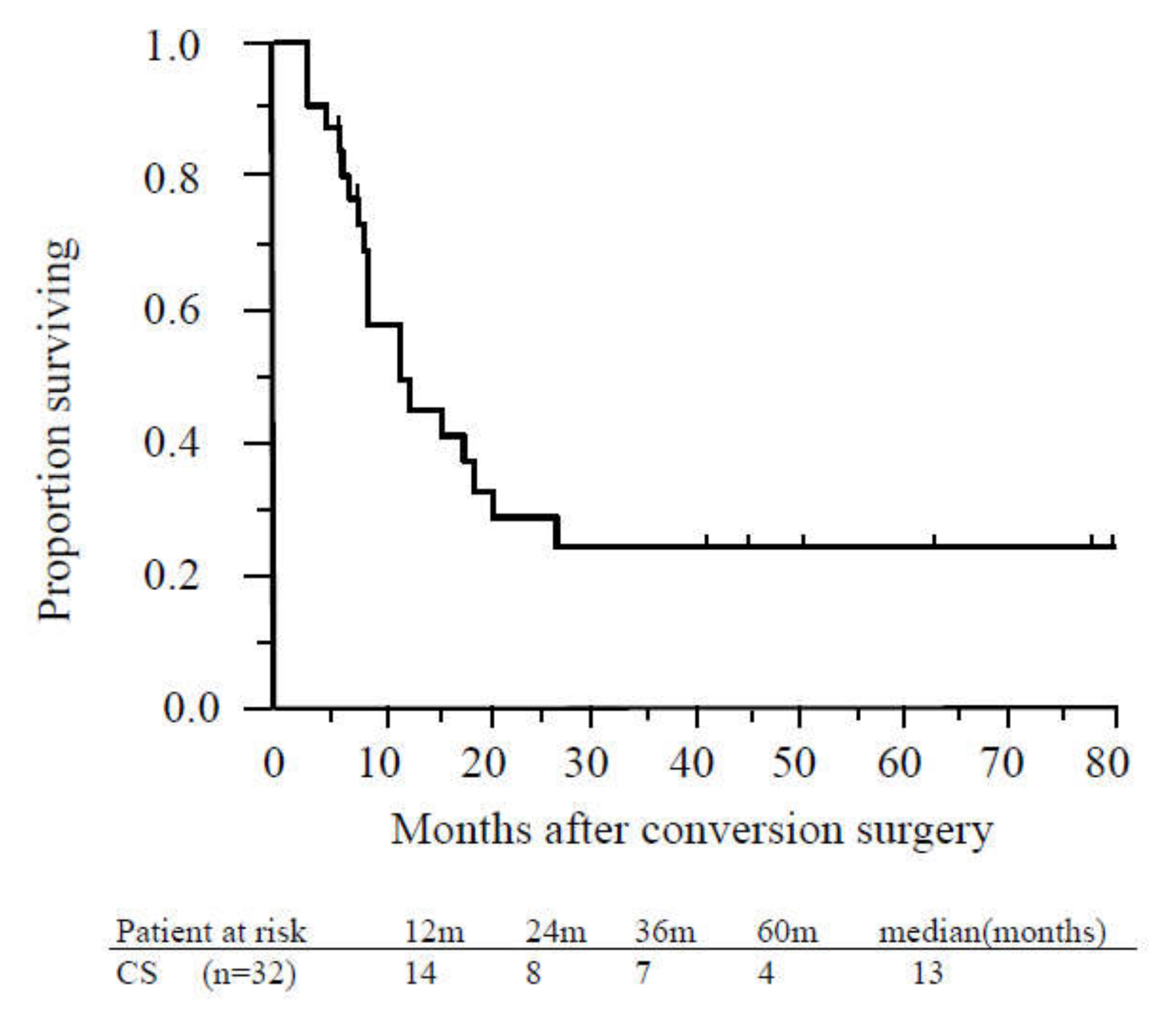
3.3. Conversion Surgery
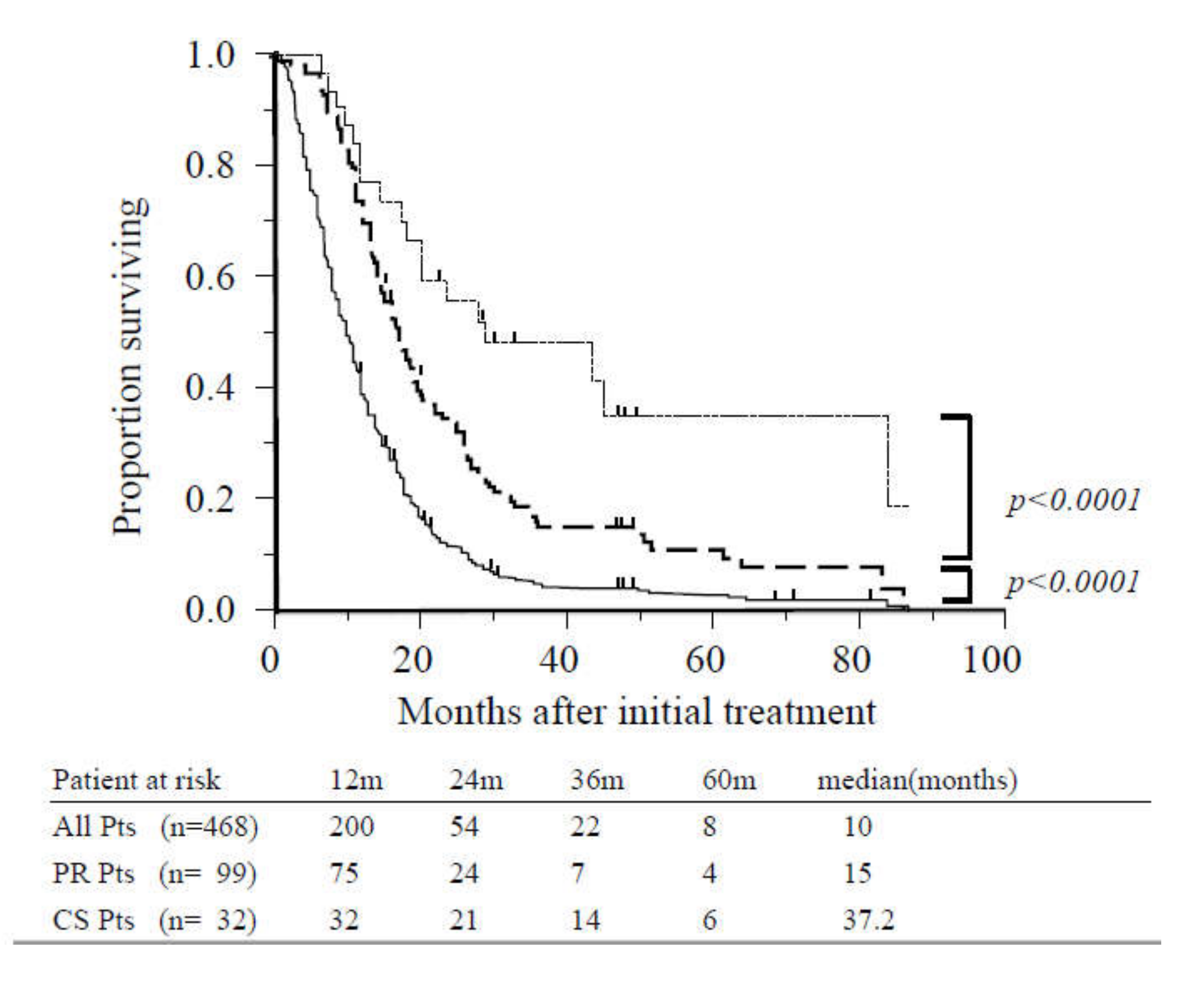
3.4. Survival Analysis
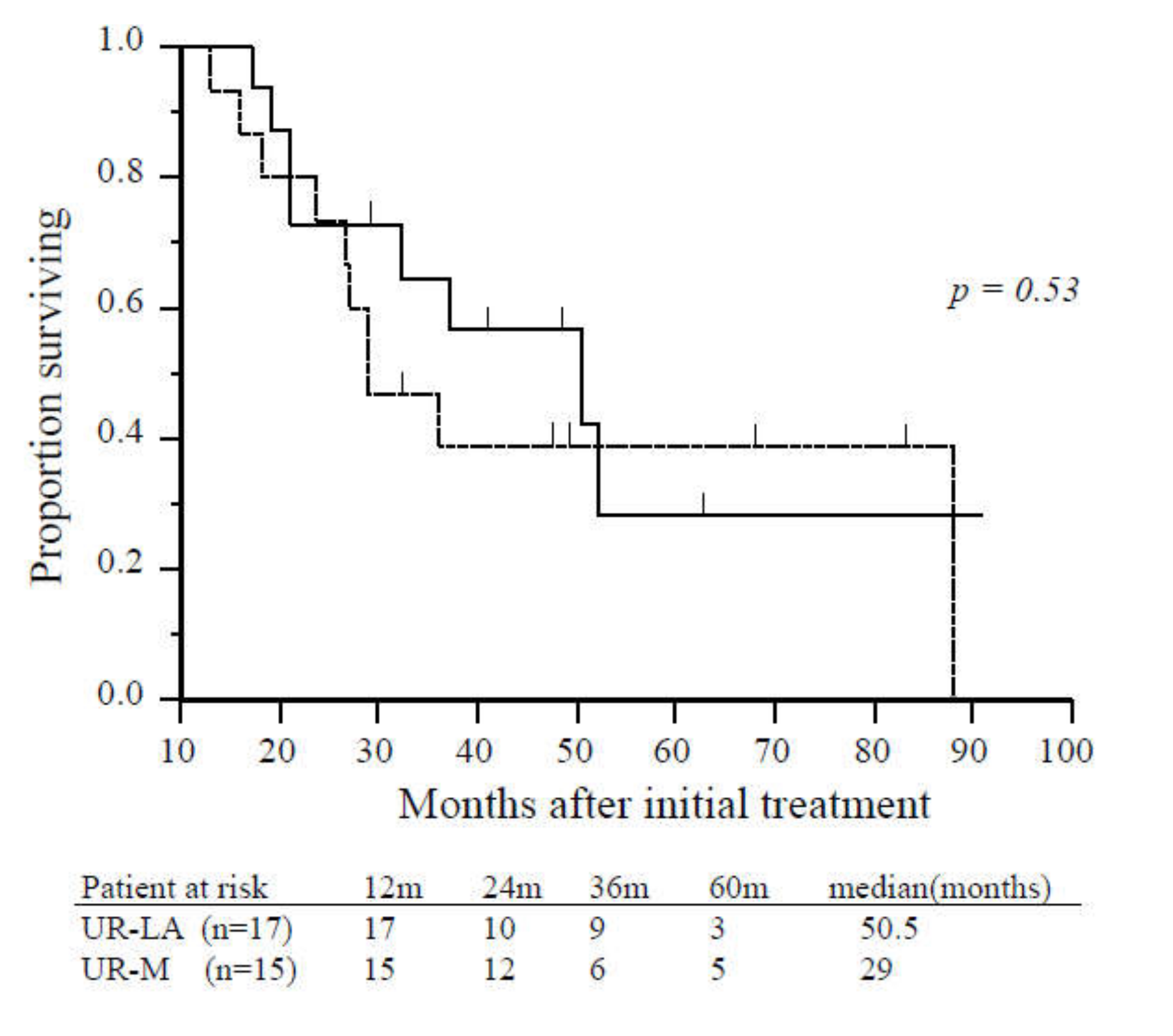
3.5. Comparison between Patients with Unresectable Locally Advanced and Metastatic Disease
3.6. Recurrence-Free Survival
3.7. Prognostic Factors for Overall Survival Among Patients Who Underwent Conversion Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hackert, T.; Büchler, M.W. Pancreatic Cancer: Advances in Treatment, Results and Limitations. Dig. Dis. 2013, 31, 51–56. [Google Scholar] [CrossRef]
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Nakao, A.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan Pancreatic Cancer Registry; 30th year anniversary: Japan Pancreas Society. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Network NCC. National Comprehensive Cancer Network NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). 2017. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on 11 September 2017).
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Asbun, H.; Bain, A.; Behrman, S.W.; Benson, A.B., 3rd; Binder, E.; Cardin, D.B.; Cha, C.; et al. Pancreatic adenocarcinoma, Version 2.2017, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 1028–1061. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Hurt, C.; Bridgewater, J.; Falk, S.; Cummins, S.; Wasan, H.; Crosby, T.; Jephcott, C.; Roy, R.; Radhakrishna, G.; et al. Gemcitabine-based or capecitabine-based chemoradiotherapy for locally advanced pancreatic cancer (SCALOP): A multicentre, randomised, phase 2 trial. Lancet Oncol. 2013, 14, 317–326. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; De La Fouchardiere, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef]
- Fukuchi, M.; Ishiguro, T.; Ogata, K.; Suzuki, O.; Kumagai, Y.; Ishibashi, K.; Ishida, H.; Kuwano, H.; Mochiki, E. Prognostic Role of Conversion Surgery for Unresectable Gastric Cancer. Ann. Surg. Oncol. 2015, 22, 3618–3624. [Google Scholar] [CrossRef]
- Yokota, T.; Kato, K.; Hamamoto, Y.; Tsubosa, Y.; Ogawa, H.; Ito, Y.; Hara, H.; Ura, T.; Kojima, T.; Chin, K.; et al. Phase II study of chemoselection with docetaxel plus cisplatin and 5-fluorouracil induction chemotherapy and subsequent conversion surgery for locally advanced unresectable oesophageal cancer. Br. J. Cancer 2016, 115, 1328–1334. [Google Scholar] [CrossRef]
- Satoi, S.; Yanagimoto, H.; Toyokawa, H.; Inoue, K.; Wada, K.; Yamamoto, T.; Hirooka, S.; Yamaki, S.; Yui, R.; Mergental, H.; et al. Selective Use of Staging Laparoscopy Based on Carbohydrate Antigen 19-9 Level and Tumor Size in Patients With Radiographically Defined Potentially or Borderline Resectable Pancreatic Cancer. Pancreas 2011, 40, 426–432. [Google Scholar] [CrossRef]
- Satoi, S.; Yanagimoto, H.; Yamamoto, T.; Toyokawa, H.; Hirooka, S.; Yamaki, S.; Opendro, S.S.; Inoue, K.; Michiura, T.; Ryota, H.; et al. A clinical role of staging laparoscopy in patients with radiographically defined locally advanced pancreatic ductal adenocarcinoma. World J. Surg. Oncol. 2016, 14, 14. [Google Scholar] [CrossRef]
- Satoi, S.; Fujii, T.; Yanagimoto, H.; Motoi, F.; Kurata, M.; Takahara, N.; Yamada, S.; Yamamoto, T.; Mizuma, M.; Honda, G.; et al. Multicenter Phase II Study of Intravenous and Intraperitoneal Paclitaxel With S-1 for Pancreatic Ductal Adenocarcinoma Patients With Peritoneal Metastasis. Ann. Surg. 2017, 265, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Satoi, S.; Yamaue, H.; Kato, K.; Takahashi, S.; Hirono, S.; Takeda, S.; Eguchi, H.; Sho, M.; Wada, K.; Shinchi, H.; et al. Role of adjuvant surgery for patients with initially unresectable pancreatic cancer with a long-term favorable response to non-surgical anti-cancer treatments: Results of a project study for pancreatic surgery by the Japanese Society of Hepato-Biliary-Pan. J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Brennan, M.; Gonen, M.; Coit, D.G.; Fong, Y.; Chung, S.; Tang, L.; Klimstra, D.; Allen, P.J. Pancreatic Adenocarcinoma: The Actual 5-Year Survivors. J. Gastrointest. Surg. 2007, 12, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Gillen, S.; Schuster, T.; Büschenfelde, C.M.Z.; Friess, H.; Kleeff, J. Preoperative/Neoadjuvant Therapy in Pancreatic Cancer: A Systematic Review and Meta-analysis of Response and Resection Percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Ahuja, N.; Makary, M.A.; Cameron, J.L.; Eckhauser, F.E.; Choti, M.A.; Hruban, R.H.; Pawlik, T.M.; Wolfgang, C.L. 2564 resected periampullary adenocarcinomas at a single institution: Trends over three decades. HPB 2013, 16, 83–90. [Google Scholar] [CrossRef]
- Kato, K.; Kondo, S.; Hirano, S.; Tanaka, E.; Shichinohe, T.; Tsuchikawa, T.; Matsumoto, J. Adjuvant surgical therapy for patients with initially-unresectable pancreatic cancer with long-term favorable responses to chemotherapy. J. Hepato-Biliary-Pancreat. Sci. 2011, 18, 712–716. [Google Scholar] [CrossRef]
- Wright, G.P.; Poruk, K.E.; Zenati, M.; Steve, J.; Bahary, N.; Hogg, M.E.; Zuriekat, A.H.; Wolfgang, C.L.; Zeh, H.J.; Weiss, M. Primary Tumor Resection Following Favorable Response to Systemic Chemotherapy in Stage IV Pancreatic Adenocarcinoma with Synchronous Metastases: A Bi-institutional Analysis. J. Gastrointest. Surg. 2016, 20, 1830–1835. [Google Scholar] [CrossRef]
- Nitsche, U.; Wenzel, P.; Siveke, J.T.; Braren, R.; Holzapfel, K.; Schlitter, A.M.; Stöß, C.; Kong, B.; Esposito, I.; Erkan, M.; et al. Resectability After First-Line FOLFIRINOX in Initially Unresectable Locally Advanced Pancreatic Cancer: A Single-Center Experience. Ann. Surg. Oncol. 2015, 22, 1212–1220. [Google Scholar] [CrossRef]
- Hackert, T.; Sachsenmaier, M.; Hinz, U.; Schneider, L.; Michalski, C.W.; Springfeld, C.; Strobel, O.; Jäger, D.; Ulrich, A.; Büchler, M.W. Locally advanced pancreatic cancer: Neoadjuvant therapy with FOLFIRINOX results in resectability in 60% of the patients. Ann. Surg. 2016, 264, 457–463. [Google Scholar] [CrossRef]
- Kenta, S.; Okabayashi, T.; Shima, Y.; Morita, S.; Iwata, J.; Sumiyoshi, T.; Saisaka, Y.; Yasuhiro, H.; Yoshihiro, N.; Matsumoto, M.; et al. Clinical effects of chemoradiotherapy in pursuit of optimal treatment of locally advanced unresectable pancreatic cancer. Br. J. Radiol. 2017, 90, 20170165. [Google Scholar]
- Saito, T.; Ishido, K.; Kudo, D.; Kimura, N.; Wakiya, T.; Nakayama, Y.; Hakamada, K. Combination therapy with gemcitabine and nab-paclitaxel for locally advanced unresectable pancreatic cancer. Mol. Clin. Oncol. 2017, 6, 963–967. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.; Hirano, S.; Nakamura, T.; Okamura, K.; Tsuchikawa, T.; Noji, T.; Nakanishi, Y.; Tanaka, K.; Shichinohe, T. Survival benefit of conversion surgery for patients with initially unresectable pancreatic cancer who responded favorably to nonsurgical treatment. J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Natsume, S.; Shimizu, Y.; Senda, Y.; Hijioka, S.; Matsuo, K.; Ito, S.; Komori, K.; Abe, T.; Hara, K. Conversion surgery only for highly selected patients with unresectable pancreatic cancer: A satisfactory outcome in exchange for a lower resection rate. Surg. Today 2019, 49, 670–677. [Google Scholar] [CrossRef]
- Opendro, S.S.; Satoi, S.; Yanagimoto, H.; Yamamoto, T.; Toyokawa, H.; Hirooka, S.; Yamaki, S.; Inoue, K.; Matsui, Y.; Kwon, A.-H. Role of adjuvant surgery in initially unresectable pancreatic cancer after long-term chemotherapy or chemoradiation therapy: Survival benefit? J. Hepato-Biliary-Pancreat. Sci. 2014, 21, 695–702. [Google Scholar] [CrossRef]
- Yoo, C.; Shin, S.H.; Kim, K.P.; Jeong, J.H.; Chang, H.M.; Kang, J.H.; Lee, S.S.; Park, D.H.; Song, T.J.; Seo, D.W.; et al. Clinical outcomes of conversion surgery after neoadjuvant chemotherapy in patients with borderline resectable and locally advanced unresectable pancreatic cancer: A single-center, retrospective analysis. Cancers 2019, 11, 278. [Google Scholar] [CrossRef]
- Michelakos, T.; Pergolini, I.; Castillo, C.F.-D.; Honselmann, K.C.; Cai, L.; Deshpande, V.; Wo, J.Y.; Ryan, D.P.; Allen, J.N.; Blaszkowsky, L.S.; et al. Predictors of Resectability and Survival in Patients With Borderline and Locally Advanced Pancreatic Cancer who Underwent Neoadjuvant Treatment With FOLFIRINOX. Ann. Surg. 2019, 269, 733–740. [Google Scholar] [CrossRef]
- Klaiber, U.; Schnaidt, E.S.; Hinz, U.; Gaida, M.M.; Heger, U.; Hank, T.; Strobel, O.; Neoptolemos, J.P.; Mihaljevic, A.L.; Büchler, M.W. Prognostic Factors of Survival After Neoadjuvant Treatment and Resection for Initially Unresectable Pancreatic Cancer. Ann. Surg. 2019, in press. [Google Scholar] [CrossRef]
- Satoi, S.; Yamamoto, T.; Yamaki, S.; Sakaguchi, T.; Sekimoto, M. Surgical indication for and desirable outcomes of conversion surgery in patients with initially unresectable pancreatic ductal adenocarcinoma. Ann. Gastroenterol. Surg. 2019, 4, 6–13. [Google Scholar] [CrossRef]
- Van Veldhuisen, E.; Vogel, J.A.; Klompmaker, S.; Busch, O.R.; Van Laarhoven, H.W.M.; Van Lienden, K.P.; Wilmink, J.W.; Marsman, H.A.; Besselink, M.G. Added value of CA19-9 response in predicting resectability of locally advanced pancreatic cancer following induction chemotherapy. HPB 2018, 20, 605–611. [Google Scholar] [CrossRef]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Clark, J.W.; Jiang, W.; Yeap, B.Y.; Drapek, L.C.; Ly, L.; Baglini, C.V.; Blaszkowsky, L.S.; et al. Total Neoadjuvant Therapy With FOLFIRINOX in Combination With Losartan Followed by Chemoradiotherapy for Locally Advanced Pancreatic Cancer: A Phase 2 Clinical Trial. JAMA Oncol. 2019, 5, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Rangelova, E.; Wefer, A.; Persson, S.; Valente, R.; Tanaka, K.; Orsini, N.; Segersvärd, R.; Arnelo, U.; Del Chiaro, M. Surgery improves survival after neoadjuvant therapy for borderline and locally advanced pancreatic cancer: A single institution experience. Ann. Surg. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Heger, U.; Sun, H.; Hinz, U.; Klaiber, U.; Tanaka, M.; Liu, B.; Sachsenmaier, M.; Springfeld, C.; Michalski, C.W.; Büchler, M.W.; et al. Induction chemotherapy in pancreatic cancer: CA 19-9 may predict resectability and survival. HPB 2020, 22, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Heckler, M.; Mihaljevic, A.; Sun, H.; Klaiber, U.; Heger, U.; Büchler, M.W.; Hackert, T. CT response of primary tumor and CA19-9 predict resectability of metastasized pancreatic cancer after FOLFIRINOX. Eur. J. Surg. Oncol. 2019, 45, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, D.; Katz, M.H.; Rashid, A.; Varadhachary, G.R.; Wolff, R.A.; Wang, H.; Lee, J.E.; Pisters, P.W.; Vauthey, J.N.; Crane, C.; et al. Histologic grading the extent of residual carcinoma following neoadjuvant chemoradiation in pancreatic ductal adenocarcinoma: A predictor for patient outcome. Cancer 2012, 118, 3182–3190. [Google Scholar] [CrossRef]
- White, R.R.; Xie, H.B.; Gottfried, M.R.; Czito, B.G.; Hurwitz, H.I.; Morse, M.A.; Blobe, G.C.; Paulson, E.K.; Baillie, J.; Branch, M.S.; et al. Significance of Histological Response to Preoperative Chemoradiotherapy for Pancreatic Cancer. Ann. Surg. Oncol. 2005, 12, 214–221. [Google Scholar] [CrossRef]
- Moutardier, V.; Magnin, V.; Turrini, O.; Viret, F.; Hennekinne-Mucci, S.; Gonçalves, A.; Pésenti, C.; Guiramand, J.; Lelong, B.; Giovannini, M.; et al. Assessment of pathologic response after preoperative chemoradiotherapy and surgery in pancreatic adenocarcinoma. Int. J. Radiat. Oncol. 2004, 60, 437–443. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | UR-LA (n = 108) | UR-M (n = 360) | p-Value |
|---|---|---|---|
| Age (years), median (range) | 69(38–84) | 67(33–86) | 0.15 |
| Male/female, n (%) | 54(50)/54(50) | 210(58.3)/150(41.7) | 0.12 |
| ECOG PS, n (%): 0/1/2 | 86(79.6)/18(16.6)/4(3.8) | 218(60.5)/127(35.2)/15(4.2) | 0.0004 |
| Tumor location, n (%) | |||
| Head/Body-tail | 73(67.6)/35(32.4) | 148(41.1)/212(58.9) | <0.0001 |
| Tumor size (mm) | 38(20-76) | 40(15-83) | 0.062 |
| CA19-9 (U/L) | 237(1.1-8949) | 580(1-12219) | <0.0001 |
| Extent of disease, n (%) | |||
| Localized | |||
| Metastatic site | 108(100) | ||
| Liver | 193(53.6) | ||
| Peritoneum | 123(34.2) | ||
| Lung/LN/Other | 15(4.2)/23(6.4)/6(1.6) | ||
| Treatment, n (%) | |||
| GEM | 17(15.7) | 125(34.7) | |
| GEM + Erlotinib | 2(1.9) | 14(3.9) | |
| S-1 | 5(4.6) | 38(10.6) | |
| GS | 31(28.7) | 42(11.6) | |
| GnP | 13(12.0) | 63(17.5) | |
| FOLFIRINOX | 12(11.1) | 21(5.8) | |
| S-1or GnP or GS plus PTX (i.p. + i.v.) | 0(0) | 43(11.9) | |
| Chemoradiotherapy | 27(25) | 10(2.8) | |
| Other | 1(0.9) | 4(1.1) |
| Variables | n = 32 | UR-LA (n = 17) | UR-M (n = 15) | p-Value |
|---|---|---|---|---|
| Age(years), median (range) | 66 (36–84) | 65 (38–75) | 69 (50–83) | 0.135 |
| Male: Female, n (%) | 14 (44): 18 (56) | 7(41):10(59) | 7(47):8(53) | 0.754 |
| Ph: Pbt, n (%) | 14 (44): 18 (56) | 9 (53): 8 (47) | 5 (33): 10 (67) | 0.264 |
| Tumor Size(mm), median (range) | 36 (25–74) | 35 (25–55) | 40 (27–74) | 0.747 |
| Mets site: None:L:P, n (%) | 17 (53): 4 (13):11 (34) | 17 (100): 0 (0):0 (0) | 0(0): 4 (27):11 (73) | <0.0001 |
| CA19-9; U/mL, median (range) | 278 (1.2–3400) | 126 (8.4–2200) | 984 (6.6–1953) | 0.209 |
| Preoperative CA19-9 | 29.1(1.0–181.9) | 39.7(1.0–181.9) | 19(1.0–73.9) | 0.42 |
| Primary Treatment | ||||
| GEM or GS | 7 | 4 | 3 | |
| GEM + nab-PTX (GnP) | 7 | 4 | 3 | |
| S1 or GEM based + ip PTX | 8 | 0 | 8 | |
| FOLFIRINOX | 3 | 3 | 0 | |
| GEM or S-1 or GS + RT (50.4 Gy) | 7 | 6 | 1 | |
| Radiation, n (%) | 13(41) | 11(65) | 2(13) | 0.002 |
| Pretreatment period to op; (median, range) | 9.5(4–28) | 10 (4–28) | 9 (6–16) | 0.6207 |
| RECIST (CR: PR), n (%) | 1 (3.1%): 31(96.9%) | 0(0):17(100) | 1(7):14(63) | 0.153 |
| Operative time(min) | 454(223–866) | 441(223–655) | 467(227–866) | 0.36 |
| Intraoperative blood loss(mL) | 1229(207–6301) | 1087(237–2931) | 1255(207–6301) | 0.58 |
| Blood transfusion (U) | 0(0–12) | 0(0–7) | 0(0–12) | 0.42 |
| PD: DP: DP-CAR: TP, n (%) | 13 (40): 11(34): 4(13): 4(13) | 9(52):4(24):2(12):2(12) | 5(33):7(47):2(13):1(7) | 0.257 |
| -CHA/CA/PV resection- | -3(9)/4(13)/15(47)- | -3(18)/2(12)/9(52)- | -0(0)/2(13)/6(40)- | |
| Residual tumor (R0: R1), n (%) | 29(91): 3(9) | 16(94):1(6) | 13(87):2(13) | 0.471 |
| Postop comp/Mortality (%) | 8(25)/0(0) | 2(12)/0(0) | 6(40)/0(0) | 0.066/0 |
| Hospital stay (median, range) | 14 (7–114) | 11 (7–41) | 14 (7–114) | 0.271 |
| Evans (I/IIa/IIb/III/IV, (%)) | 1(3)/12(38)/10(31)/8(25)/1 (3) | 1(6)/7(41)/5(29)/4(24)/0 (0) | 0(0)/5(33)/5(33)/4 (27)/1(7) | 0.695 |
| Variables | Univariate Analysis | p-Value | Multivariate Analysis | p-Value | ||
|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | |||
| UR-M vs. UR-LA | 1.16 | 0.19–7.37 | 0.87 | 0.07 | ||
| Pbt vs. Ph | 4.99 | 0.68–102 | 0.12 | 0.07 | ||
| Tumor Size (>35 mm vs. <35 mm) | 5.83 | 0–0.40 | 0.007 | 2.16 | 0–2.31 | 0.003 |
| Pretreatment period (<8 m vs. >8 m) | 2.22 | 0.29–46.22 | 0.47 | 0.38 | ||
| Reduction of CA19-9 or DUPAN-2 (<70% vs. >70%) | 5.99 | 0.80–50.84 | 0.08 | 0.38 | ||
| LN mets (+) vs. (−) | 4.29 | 0.58–88.2 | 0.16 | 4.5 | 0.40–11.10 | 0.01 |
| R0 vs. R1 | 3.11 | 0–4.00 | 0.25 | 0.99 | ||
| CY (+) vs. (−) | 2.74 | 0.31–20.3 | 0.34 | 1.11 | 0.56–1.70 | <0.0001 |
| Evans I-IIa vs. IIb-IV | 1.47 | 0.24–11.9 | 0.68 | 0.46 | ||
| Adjuvant Tx (−) vs. (+) | 1.36 | 0.16–8.74 | 0.76 | 2.96 | 0.32–3.06 | 0.0029 |
| Variables | Univariate Analysis | p-Value | Multivariate Analysis | p-Value | ||
|---|---|---|---|---|---|---|
| HR | 95% CI | HR | 95% CI | |||
| UR-M vs. UR-LA | 1.34 | 0.53–3.54 | 0.53 | 0.44 | ||
| Pbt vs. Ph | 1.24 | 0.49–3.40 | 0.65 | 14.14 | 1.86–182 | 0.0092 |
| Tumor Size (>35 mm vs. <35 mm) | 2.47 | 0.89–7.53 | 0.08 | 0.61 | ||
| Pretreatment period (<8 m vs. >8 m) | 0.79 | 0.22–2.25 | 0.68 | 0.27 | ||
| Reduction of CA19-9 or DUPAN-2 (<70% vs. >70%) | 1.08 | 0.38–3.89 | 0.89 | 0.086 | ||
| LN mets (+) vs. (−) | 1.07 | 0.38–2.86 | 0.89 | 0.5 | ||
| R1 vs. R0 | 1.76 | 0.27–6.41 | 0.49 | 0.19 | ||
| CY (+) vs. (−) | 2.91 | 0.98–7.71 | 0.05 | 0.08 | ||
| Evans I-IIa vs. IIb-IV | 1.77 | 0.65–4.71 | 0.26 | 0.05 | ||
| Adjuvant Tx (−) vs. (+) | 4.63 | 1.76–12.13 | 0.0024 | 367.22 | 20.16–15093 | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanagimoto, H.; Satoi, S.; Yamamoto, T.; Yamaki, S.; Hirooka, S.; Kotsuka, M.; Ryota, H.; Ishida, M.; Matsui, Y.; Sekimoto, M. Benefits of Conversion Surgery after Multimodal Treatment for Unresectable Pancreatic Ductal Adenocarcinoma. Cancers 2020, 12, 1428. https://doi.org/10.3390/cancers12061428
Yanagimoto H, Satoi S, Yamamoto T, Yamaki S, Hirooka S, Kotsuka M, Ryota H, Ishida M, Matsui Y, Sekimoto M. Benefits of Conversion Surgery after Multimodal Treatment for Unresectable Pancreatic Ductal Adenocarcinoma. Cancers. 2020; 12(6):1428. https://doi.org/10.3390/cancers12061428
Chicago/Turabian StyleYanagimoto, Hiroaki, Sohei Satoi, Tomohisa Yamamoto, So Yamaki, Satoshi Hirooka, Masaya Kotsuka, Hironori Ryota, Mitsuaki Ishida, Yoichi Matsui, and Mitsugu Sekimoto. 2020. "Benefits of Conversion Surgery after Multimodal Treatment for Unresectable Pancreatic Ductal Adenocarcinoma" Cancers 12, no. 6: 1428. https://doi.org/10.3390/cancers12061428
APA StyleYanagimoto, H., Satoi, S., Yamamoto, T., Yamaki, S., Hirooka, S., Kotsuka, M., Ryota, H., Ishida, M., Matsui, Y., & Sekimoto, M. (2020). Benefits of Conversion Surgery after Multimodal Treatment for Unresectable Pancreatic Ductal Adenocarcinoma. Cancers, 12(6), 1428. https://doi.org/10.3390/cancers12061428