Venous Thromboembolism in Lymphoma: Risk Stratification and Antithrombotic Prophylaxis

 ,
, 
Abstract
1. Introduction
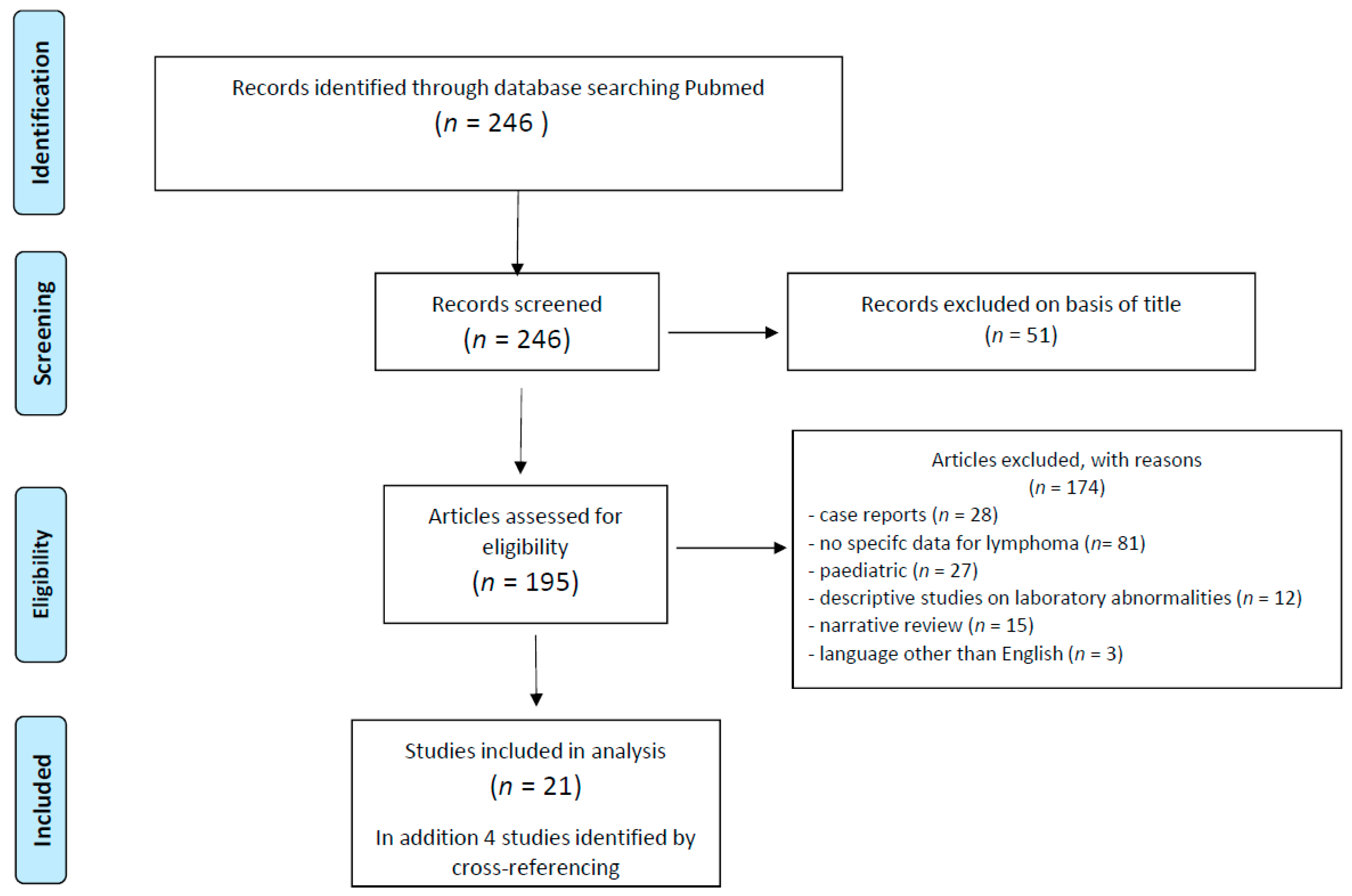
2. Methodology
3. Epidemiology
4. Risk-Modifying Factors
4.1. Individual Patient-Related Factors
4.1.1. Age
4.1.2. Gender
4.1.3. Obesity
4.1.4. Performance Status/Immobility
4.1.5. Comorbidity
4.1.6. Prior Thrombosis/Thrombophilia
4.2. Lymphoma-Related Factors
4.2.1. Histology
4.2.2. Site of Disease
4.2.3. Stage of the Disease
4.2.4. Laboratory Variables
4.2.5. International Prognostic Index (IPI)
4.2.6. Time after Diagnosis
4.2.7. Type of Therapeutic Regimen
4.2.8. Indwelling Central Venous Catheters
4.2.9. Supportive Care Agents
5. Risk Assessment Models
6. Treatment and Prophylaxis of VTE in Lymphomas
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Kuderer, N.M.; Lyman, G.H. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J. Thromb. Haemost. 2007, 5, 632–634. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Culakova, E.; Poniewierski, M.S.; Kuderer, N.M. Morbidity, mortality and costs associated with venous thromboembolism in hospitalized patients with cancer. Thromb. Res. 2018, 164, S112–S118. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef] [PubMed]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; Solymoss, S.; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients with Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef]
- Lim, S.H.; Woo, S.-Y.; Kim, S.; Ko, Y.H.; Kim, W.S.; Kim, S.J. Cross-sectional Study of Patients with Diffuse Large B-Cell Lymphoma: Assessing the Effect of Host Status, Tumor Burden, and Inflammatory Activity on Venous Thromboembolism. Cancer Res. Treat. 2016, 48, 312–321. [Google Scholar] [CrossRef]
- Antic, D.; Milic, N.; Nikolovski, S.; Todorovic, M.; Bila, J.; Djurdjevic, P.; Andjelic, B.; Djurasinovic, V.; Sretenovic, A.; Vukovic, V.; et al. Development and validation of multivariable predictive model for thromboembolic events in lymphoma patients. Am. J. Hematol. 2016, 91, 1014–1019. [Google Scholar] [CrossRef]
- Hohaus, S.; Tisi, M.C.; Bartolomei, F.; Cuccaro, A.; Maiolo, E.; Alma, E.; D’Alo, F.; Bellesi, S.; Rossi, E.; De Stefano, V. Risk factors for venous thromboembolism in patients with lymphoma requiring hospitalization. Blood Cancer J. 2018, 8, 54. [Google Scholar] [CrossRef]
- Borchmann, S.; Muller, H.; Hude, I.; Fuchs, M.; Borchmann, P.; Engert, A. Thrombosis as a treatment complication in Hodgkin lymphoma patients: A comprehensive analysis of three prospective randomized German Hodgkin Study Group (GHSG) trials. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 1329–1334. [Google Scholar] [CrossRef]
- Lekovic, D.; Miljic, P.; Mihaljevic, B. Increased risk of venous thromboembolism in patients with primary mediastinal large B-cell lymphoma. Thromb. Res. 2010, 126, 477–480. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, J.-J.; Xia, Y.; Li, C.-F.; Wang, Y.; Liu, P.-P.; Bi, X.-W.; Sun, P.; Lin, T.-Y.; Jiang, W.-Q.; et al. High risk of deep vein thrombosis associated with peripherally inserted central catheters in lymphoma. Oncotarget 2016, 7, 35404–35411. [Google Scholar] [CrossRef] [PubMed]
- Rupa-Matysek, J.; Brzezniakiewicz-Janus, K.; Gil, L.; Krasinski, Z.; Komarnicki, M. Evaluation of the ThroLy score for the prediction of venous thromboembolism in newly diagnosed patients treated for lymphoid malignancies in clinical practice. Cancer Med. 2018, 35, 5. [Google Scholar] [CrossRef] [PubMed]
- Rupa-Matysek, J.; Gil, L.; Kazmierczak, M.; Baranska, M.; Komarnicki, M. Prediction of venous thromboembolism in newly diagnosed patients treated for lymphoid malignancies: Validation of the Khorana Risk Score. Med. Oncol. 2017, 35, 5. [Google Scholar] [CrossRef] [PubMed]
- Mohren, M.; Markmann, I.; Jentsch-Ullrich, K.; Koenigsmann, M.; Lutze, G.; Franke, A. Increased risk of venous thromboembolism in patients with acute leukaemia. Br. J. Cancer 2006, 94, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Teegala, S.; Huen, A.; Ji, Y.; Fayad, L.; Hagemeister, F.B.; Gladish, G.; Vadhan-Raj, S. Incidence and risk factors of venous thromboembolic events in lymphoma. Am. J. Med. 2010, 123, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Komrokji, R.S.; Uppal, N.P.; Khorana, A.A.; Lyman, G.H.; Kaplan, K.L.; Fisher, R.I.; Francis, C.W. Venous thromboembolism in patients with diffuse large B-cell lymphoma. Leuk. Lymphoma 2006, 47, 1029–1033. [Google Scholar] [CrossRef]
- Borg, I.H.; Bendtsen, M.D.; Bogsted, M.; Madsen, J.; Severinsen, M.T. Incidence of venous thromboembolism in patients with diffuse large B-cell lymphoma. Leuk. Lymphoma 2016, 57, 2771–2776. [Google Scholar] [CrossRef]
- Goldschmidt, N.; Linetsky, E.; Shalom, E.; Varon, D.; Siegal, T. High incidence of thromboembolism in patients with central nervous system lymphoma. Cancer 2003, 98, 1239–1242. [Google Scholar] [CrossRef]
- Yokoyama, K.; Murata, M.; Ikeda, Y.; Okamoto, S. Incidence and risk factors for developing venous thromboembolism in Japanese with diffuse large b-cell lymphoma. Thromb. Res. 2012, 130, 7–11. [Google Scholar] [CrossRef]
- Byun, J.M.; Hong, J.; Yoon, S.-S.; Koh, Y.; Ock, C.-Y.; Kim, T.M.; Lee, J.H.; Kim, S.-H.; Lee, J.-O.; Bang, S.-M.; et al. Incidence and characteristics of venous thromboembolism in Asian patients with primary central nervous system lymphoma undergoing chemotherapy. Thromb. Res. 2019, 183, 131–135. [Google Scholar] [CrossRef]
- Gebhart, J.; Lechner, K.; Skrabs, C.; Sliwa, T.; Muldur, E.; Ludwig, H.; Nosslinger, T.; Vanura, K.; Stamatopoulos, K.; Simonitsch-Klupp, I.; et al. Lupus anticoagulant and thrombosis in splenic marginal zone lymphoma. Thromb. Res. 2014, 134, 980–984. [Google Scholar] [CrossRef] [PubMed]
- Santi, R.M.; Ceccarelli, M.; Bernocco, E.; Monagheddu, C.; Evangelista, A.; Valeri, F.; Monaco, F.; Vitolo, U.; Cortelazzo, S.; Cabras, M.G.; et al. Khorana score and histotype predicts incidence of early venous thromboembolism in non-Hodgkin lymphomas. A pooled-data analysis of 12 clinical trials of Fondazione Italiana Linfomi (FIL). Thromb. Haemost. 2017, 117, 1615–1621. [Google Scholar] [CrossRef]
- Caruso, V.; Di Castelnuovo, A.; Meschengieser, S.; Lazzari, M.A.; de Gaetano, G.; Storti, S.; Iacoviello, L.; Donati, M.B. Thrombotic complications in adult patients with lymphoma: A meta-analysis of 29 independent cohorts including 18,018 patients and 1149 events. Blood 2010, 115, 5322–5328. [Google Scholar] [CrossRef] [PubMed]
- Yamshon, S.; Christos, P.J.; Demetres, M.; Hammad, H.; Leonard, J.P.; Ruan, J. Venous thromboembolism in patients with B-cell non-Hodgkin lymphoma treated with lenalidomide: A systematic review and meta-analysis. Blood Adv. 2018, 2, 1429–1438. [Google Scholar] [CrossRef]
- Sanfilippo, K.M.; Wang, T.F.; Gage, B.F.; Luo, S.; Riedell, P.; Carson, K.R. Incidence of venous thromboembolism in patients with non-Hodgkin lymphoma. Thromb. Res. 2016, 143, 86–90. [Google Scholar] [CrossRef]
- Gangaraju, R.; Chen, Y.; Hageman, L.; Wu, J.; Francisco, L.; Kung, M.; Ness, E.; Parman, M.; Weisdorf, D.J.; Forman, S.J.; et al. Risk of venous thromboembolism in patients with non-Hodgkin lymphoma surviving blood or marrow transplantation. Cancer 2019, 125, 4498–4508. [Google Scholar] [CrossRef]
- Mahajan, A.; Wun, T.; Chew, H.; White, R.H. Lymphoma and venous thromboembolism: Influence on mortality. Thromb. Res. 2014, 133, S23–S28. [Google Scholar] [CrossRef]
- Lund, J.L.; Ostgard, L.S.; Prandoni, P.; Sorensen, H.T.; de Nully Brown, P. Incidence, determinants and the transient impact of cancer treatments on venous thromboembolism risk among lymphoma patients in Denmark. Thromb. Res. 2015, 136, 917–923. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Pfeiffer, R.M.; Bjorkholm, M.; Goldin, L.R.; Turesson, I.; Schulman, S.; Landgren, O.; Kristinsson, S.Y. Elevated risk of venous but not arterial thrombosis in Waldenstrom macroglobulinemia/lymphoplasmacytic lymphoma. J. Thromb. Haemost. 2014, 12, 1816–1821. [Google Scholar] [CrossRef]
- Park, L.C.; Woo, S.; Kim, S.; Jeon, H.; Ko, Y.H.; Kim, S.J.; Kim, W.S. Incidence, risk factors and clinical features of venous thromboembolism in newly diagnosed lymphoma patients: Results from a prospective cohort study with Asian population. Thromb. Res. 2012, 130, e6–e12. [Google Scholar] [CrossRef]
- Abdol Razak, N.B.; Jones, G.; Bhandari, M.; Berndt, M.C.; Metharom, P. Cancer-Associated Thrombosis: An Overview of Mechanisms, Risk Factors, and Treatment. Cancers 2018, 10, 380. [Google Scholar] [CrossRef] [PubMed]
- Falanga, A.; Russo, L.; Verzeroli, C. Mechanisms of thrombosis in cancer. Thromb. Res. 2013, 131 (Suppl. 1), S59–S62. [Google Scholar] [CrossRef]
- Falanga, A.; Russo, L.; Milesi, V.; Vignoli, A. Mechanisms and risk factors of thrombosis in cancer. Crit. Rev. Oncol. Hematol. 2017, 118, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Kuderer, N.M.; Lyman, G.H. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer 2007, 110, 2339–2346. [Google Scholar] [CrossRef] [PubMed]
- A predictive model for aggressive non-Hodgkin’s lymphoma. New Engl. J. Med. 1993, 329, 987–994. [CrossRef] [PubMed]
- Khorana, A.A.; Francis, C.W.; Culakova, E.; Fisher, R.I.; Kuderer, N.M.; Lyman, G.H. Thromboembolism in hospitalized neutropenic cancer patients. J. Clin. Oncol. 2006, 24, 484–490. [Google Scholar] [CrossRef]
- White, R.H.; Chew, H.K.; Zhou, H.; Parikh-Patel, A.; Harris, D.; Harvey, D.; Wun, T. Incidence of venous thromboembolism in the year before the diagnosis of cancer in 528,693 adults. Arch. Intern. Med. 2005, 165, 1782–1787. [Google Scholar] [CrossRef]
- Blom, J.W.; Doggen, C.J.M.; Osanto, S.; Rosendaal, F.R. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA 2005, 293, 715–722. [Google Scholar] [CrossRef]
- Pabinger, I.; Ay, C.; Dunkler, D.; Thaler, J.; Reitter, E.-M.; Marosi, C.; Zielinski, C.; Mannhalter, C. Factor V Leiden mutation increases the risk for venous thromboembolism in cancer patients—Results from the Vienna Cancer and Thrombosis Study (CATS). J. Thromb. Haemost. 2015, 13, 17–22. [Google Scholar] [CrossRef]
- Yokoyama, K. Thrombosis in Lymphoma Patients and in Myeloma Patients. Keio J. Med. 2015, 64, 37–43. [Google Scholar] [CrossRef]
- Hohaus, S.; Massini, G.; Giachelia, M.; Vannata, B.; Bozzoli, V.; Cuccaro, A.; D’Alo’, F.; Larocca, L.M.; Raymakers, R.A.P.; Swinkels, D.W.; et al. Anemia in Hodgkin’s lymphoma: The role of interleukin-6 and hepcidin. J. Clin. Oncol. 2010, 28, 2538–2543. [Google Scholar] [CrossRef]
- Riedl, J.; Kaider, A.; Reitter, E.-M.; Marosi, C.; Jager, U.; Schwarzinger, I.; Zielinski, C.; Pabinger, I.; Ay, C. Association of mean platelet volume with risk of venous thromboembolism and mortality in patients with cancer. Results from the Vienna Cancer and Thrombosis Study (CATS). Thromb. Haemost. 2014, 111, 670–678. [Google Scholar] [PubMed]
- Ferroni, P.; Guadagni, F.; Riondino, S.; Portarena, I.; Mariotti, S.; La Farina, F.; Davi, G.; Roselli, M. Evaluation of mean platelet volume as a predictive marker for cancer-associated venous thromboembolism during chemotherapy. Haematologica 2014, 99, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Rupa-Matysek, J.; Gil, L.; Baranska, M.; Dytfeld, D.; Komarnicki, M. Mean platelet volume as a predictive marker for venous thromboembolism in patients treated for Hodgkin lymphoma. Oncotarget 2018, 9, 21190–21200. [Google Scholar] [CrossRef] [PubMed]
- Rupa-Matysek, J.; Gil, L.; Kroll-Balcerzak, R.; Baranska, M.; Komarnicki, M. Mean platelet volume as a predictive marker for venous thromboembolism and mortality in patients treated for diffuse large B-cell lymphoma. Hematol. Oncol. 2017, 35, 456–464. [Google Scholar] [CrossRef] [PubMed]
- van Es, N.; Franke, V.F.; Middeldorp, S.; Wilmink, J.W.; Buller, H.R. The Khorana score for the prediction of venous thromboembolism in patients with pancreatic cancer. Thromb. Res. 2017, 150, 30–32. [Google Scholar] [CrossRef]
- Mansfield, A.S.; Tafur, A.J.; Wang, C.E.; Kourelis, T.V.; Wysokinska, E.M.; Yang, P. Predictors of active cancer thromboembolic outcomes: Validation of the Khorana score among patients with lung cancer. J. Thromb. Haemost. 2016, 14, 1773–1778. [Google Scholar] [CrossRef]
- van Es, N.; Ventresca, M.; Di Nisio, M.; Zhou, Q.; Noble, S.; Crowther, M.; Briel, M.; Garcia, D.; Lyman, G.H.; Macbeth, F.; et al. The Khorana score for prediction of venous thromboembolism in cancer patients: An individual patient data meta-analysis. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef]
- Mulder, F.I.; Candeloro, M.; Kamphuisen, P.W.; Di Nisio, M.; Bossuyt, P.M.; Guman, N.; Smit, K.; Buller, H.R.; van Es, N. The Khorana score for prediction of venous thromboembolism in cancer patients: A systematic review and meta-analysis. Haematologica 2019, 104, 1277–1287. [Google Scholar] [CrossRef]
- Cella, C.A.; Di Minno, G.; Carlomagno, C.; Arcopinto, M.; Cerbone, A.M.; Matano, E.; Tufano, A.; Lordick, F.; De Simone, B.; Muehlberg, K.S.; et al. Preventing Venous Thromboembolism in Ambulatory Cancer Patients: The ONKOTEV Study. Oncologist 2017, 22, 601–608. [Google Scholar] [CrossRef]
- Munoz Martin, A.J.; Ortega, I.; Font, C.; Pachon, V.; Castellon, V.; Martinez-Marin, V.; Salgado, M.; Martinez, E.; Calzas, J.; Ruperez, A.; et al. Multivariable clinical-genetic risk model for predicting venous thromboembolic events in patients with cancer. Br. J. Cancer 2018, 118, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Pabinger, I.; van Es, N.; Heinze, G.; Posch, F.; Riedl, J.; Reitter, E.-M.; Di Nisio, M.; Cesarman-Maus, G.; Kraaijpoel, N.; Zielinski, C.C.; et al. A clinical prediction model for cancer-associated venous thromboembolism: A development and validation study in two independent prospective cohorts. Lancet Haematol. 2018, 5, e289–e298. [Google Scholar] [CrossRef]
- Napolitano, M.; Saccullo, G.; Marietta, M.; Carpenedo, M.; Castaman, G.; Cerchiara, E.; Chistolini, A.; Contino, L.; De Stefano, V.; Falanga, A.; et al. Platelet cut-off for anticoagulant therapy in thrombocytopenic patients with blood cancer and venous thromboembolism: An expert consensus. Blood Transfus. 2019, 17, 171–180. [Google Scholar] [PubMed]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. New Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an Oral Factor Xa Inhibitor With Low Molecular Weight Heparin in Patients With Cancer With Venous Thromboembolism: Results of a Randomized Trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- McBane, R.D., 2nd; Wysokinski, W.E.; Le-Rademacher, J.G.; Zemla, T.; Ashrani, A.; Tafur, A.; Perepu, U.; Anderson, D.; Gundabolu, K.; Kuzma, C.; et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: The ADAM VTE trial. J. Thromb. Haemost. 2020, 18, 411–421. [Google Scholar] [CrossRef]
- Agnelli, G.; Becattini, C.; Meyer, G.; Munoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. New Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Mulder, F.I.; van Es, N.; Kraaijpoel, N.; Di Nisio, M.; Carrier, M.; Duggal, A.; Gaddh, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; et al. Edoxaban for treatment of venous thromboembolism in patient groups with different types of cancer: Results from the Hokusai VTE Cancer study. Thromb. Res. 2020, 185, 13–19. [Google Scholar] [CrossRef]
- Carrier, M.; Abou-Nassar, K.; Mallick, R.; Tagalakis, V.; Shivakumar, S.; Schattner, A.; Kuruvilla, P.; Hill, D.; Spadafora, S.; Marquis, K.; et al. Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. New Engl. J. Med. 2019, 380, 711–719. [Google Scholar] [CrossRef]
- Khorana, A.A.; Soff, G.A.; Kakkar, A.K.; Vadhan-Raj, S.; Riess, H.; Wun, T.; Streiff, M.B.; Garcia, D.A.; Liebman, H.A.; Belani, C.P.; et al. Rivaroxaban for Thromboprophylaxis in High-Risk Ambulatory Patients with Cancer. New Engl. J. Med. 2019, 380, 720–728. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Year | Country | Ref. No. | Type of Study | No. Pts | Histologies | Median Age | Identification of Events | Median Time | No. VTE | Cumulative Incidence |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sanfilippo | 2016 | USA | 25 | registry | 2730 | DLBCL FL | 64 | ICD codes | 28.4 mo. | 246 | DLBCL 10% at 6 mo. |
| Santi | 2017 | Italy | 22 | clinical trials | 1717 | NHL | 57 | pharmacovigilance | 6 mo. | 53 | 2.9% at 6 mo. |
| Antic | 2016 | Serbia | 7 | retrospective single center | 1820 | NHL, HL, CLL | 53 | records review | 9 mo, | 73 | 5.3% during therapy |
| Rupa-Matysek | 2018 | Polonia | 12 | retrospective single center | 428 | DLBCL, HL | 50 | records review | 37 mo. | 64 | 15% |
| Rupa-Matysek | 2018 | Polonia | 13 | retrospective single center | 428 | DLBCL, HL | 50 | records review | 37 mo. | 64 | 15% |
| Hohaus | 2018 | Italy | 8 | retrospective single center | 857 | NHL, HL | 51 | records review | 15 mo. | 95 | 11.1% at 9 mo. |
| Park | 2012 | Korea | 30 | prospective single center | 686 | NHL, HL, CLL | 51 | records review | 21.8 mo. | 54 | 7.9% at 1 yr |
| Mohren | 2005 | Germany | 14 | retrospective single center | 1038 | NHL, HL, | 59 | records review | n.a. | 80 | 7.7% |
| Zhou | 2010 | USA | 15 | retrospective single center | 422 | NHL, HL | 57 | records review | 2 yrs | 80 | 17.1% at 2 yrs |
| Mahajan | 2014 | USA | 27 | population-based databases | 16755 | NHL | n.a. | ICD codes | 2 yrs | 670 | 4% at 2 yrs |
| Lund | 2015 | Denmark | 28 | population-based databases | 10375 | NHL, HL | n.a. | ICD codes | 2 yrs | 355 | 3.9%at 2 yrs |
| Caruso | 2010 | International | 23 | meta-analysis | 18018 | NHL, HL | n.a. | published studies | n.a. | 1149 | 6.4% during therapy |
| Lim | 2016 | Korea | 6 | prospective single center | 322 | DLBCL | 56 | not specified | 41.9 mo. | 34 | 10.6% at 1 yr |
| Komrokji | 2006 | USA | 16 | retrospective single center | 211 | DLBCL | 57 | records review | n.a. | 27 | 12.7% during therapy |
| Borg | 2016 | Denmark | 6 | retrospective single center | 289 | DLBCL | 67 | ICD codes | 16 mo. | 32 | 11.1% at 2 yrs |
| Yokoyama | 2012 | Japan | 19 | retrospective single center | 142 | DLBCL | 63 | records review | n.a. | 15 | 11% during therapy |
| Goldschmidt | 2003 | Israel | 18 | retrospective single center | 42 | PCNSL | 61 | records review | n.a. | 25 | 59.5% at 3 mo. |
| Byun | 2019 | Korea | 20 | retrospective multicenter | 235 | PCNSL | 63 | records review | 21 mo. | 33 | 11.7% at 1 yr |
| Lekovic | 2010 | Serbia | 10 | retrospective single center | 42 | PMBCL | 34 | records review | 47 mo. | 15 | 35.7% at 6 mo. |
| Borchmann | 2019 | Germany | 9 | clinical trials | 573 | HL | 36 | trial data | 12 mo. | 173 | 3.3% |
| Gebhart | 2014 | Austria | 21 | retrospective multicenter | 70 | SMZL | n.a. | records review | n.a. | 9 | 13% |
| Hultcrantz | 2014 | Sweden | 29 | population-based databases | 2190 | WM/LPL | 74 | ICD codes | 10 yrs | 92 | 2.1% at 1 y |
| Gangaraju | 2019 | USA | 26 | registry | 734 | NHL | 49 | patient questionaire | 8.1 yrs | 58 | 8.1% at 10 yrs |
| Yamshon | 2018 | International | 24 | meta-analysis | 1433 | NHL | 66 | published studies | n.a. | 77 | 4.5% at 6 mo. |
| Zhang | 2016 | China | 11 | retrospective single center | 565 | lymphoma | n.a. | not specified | n.a. | 40 | 7.1% PICC-related |
| First Author | Ref. No. | Histology | Age | Gender | BMI | PriorVTE | Cmorb. | Stage | ECOG | LDH | Hb | WBC | Plt | KS | Other |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sanfilippo | 25 | DLBCL | No | n.d. | Yes | Yes | No | stage | n.d. | No | Yes | n.d | n.d. | No | |
| Santi | 22 | DLBCL | Yes | Female | n.d. | No | n.d. | n.d. | n.d. | n.d. | n.d. | Yes | |||
| Antic | 7 | aggressive | No | No | Yes | Yes | n.d. | E, Med | Yes | n.d. | Yes | Yes * | No | n.d. | |
| Rupa-Matysek | 12 | DLBCL | No | No | n.d. | Yes | n.d. | Med | Yes | n.d. | Yes | Yes | No | n.d. | |
| Rupa-Matysek | 13 | DLBCL | No | No | n.d. | n.d. | n.d. | Bulk | n.d. | n.d. | Yes | Yes | No | No | IPI score |
| Hohaus | 8 | aggressive | Yes | No | n.d. | n.d. | n.d. | bulk, CNS | Yes | Yes | No | No | No | No | albumin < 4 |
| Park | 30 | aggressive | Yes | No | n.d. | No | Yes | stage, E, Med, CNS | Yes | Yes | n.d. | n.d. | n.d. | n.d. | |
| Mohren | 14 | aggressive | No | No | n.d. | n.d. | n.d. | No | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | |
| Zhou | 15 | n.d. | No | Female | No | n.d. | No | No | n.d. | No | Yes | No | No | n.d. | creatinine |
| Mahajan | 27 | aggressive | Yes | No | n.d. | n.d. | Yes | stage | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | Asian |
| Lund | 28 | aggressive | No | No | n.d. | n.d. | No | CNS | Yes | Yes | No | No | No | n.d. | |
| Caruso | 23 | aggressive | n.d. | n.d. | n.d. | n.d. | n.d. | No | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | |
| Lim | 6 | n.a. | Yes | No | No | n.d | n.d. | stage, E | Yes | No | No | Yes | No | No | IPI score |
| Komrokji | 16 | n.a. | No | No | n.d. | n.d | n.d. | stage | No | No | n.d. | n.d. | n.d. | n.d. | IPI score |
| Borg | 17 | n.a. | n.d. | No | No | Yes | n.d. | stage | Yes | No | No | No | No | n.d. | IPI score |
| Yokoyama | 19 | n.a. | Yes | No | No | n.a. | n.d. | No | Yes | Yes | No | No | No | n.d. | IPI score |
| Goldschmidt | 18 | n.a. | No | n.d. | n.d. | n.a | n.d. | n.d. | n.d. | n.d. | n.d. | No | n.d. | n.d. | |
| Byun | 20 | n.a. | Yes | Female | No | n.a. | n.d. | n.d. | Yes | No | Yes | No | No | n.d. | albumin <4 |
| Lekovic | 10 | n.a. | No | No | n.d. | n.a | n.d. | n.d. | n.d. | n.d. | n.d. | No | No | n.d. | fibrinogen |
| Borchmann | 9 | n.a. | n.d. | No | No | n.d | n.d. | Yes | n.d. | n.d. | No | No | No | No | |
| Gebhart | 21 | n.a. | n.d. | n.d. | n.d. | n.d | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | LAC |
| Hultcrantz | 29 | n.a. | n.d. | n.d. | n.d. | n.d | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | |
| Gangaraju | 26 | n.d. | n.d. | n.d. | Yes | n.d | Yes | n.d. | n.d. | n.d. | n.d. | n.d | n.d. | n.d. | GVHD |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hohaus, S.; Bartolomei, F.; Cuccaro, A.; Maiolo, E.; Alma, E.; D’Alò, F.; Bellesi, S.; Rossi, E.; Stefano, V.D. Venous Thromboembolism in Lymphoma: Risk Stratification and Antithrombotic Prophylaxis. Cancers 2020, 12, 1291. https://doi.org/10.3390/cancers12051291
Hohaus S, Bartolomei F, Cuccaro A, Maiolo E, Alma E, D’Alò F, Bellesi S, Rossi E, Stefano VD. Venous Thromboembolism in Lymphoma: Risk Stratification and Antithrombotic Prophylaxis. Cancers. 2020; 12(5):1291. https://doi.org/10.3390/cancers12051291
Chicago/Turabian StyleHohaus, Stefan, Francesca Bartolomei, Annarosa Cuccaro, Elena Maiolo, Eleonora Alma, Francesco D’Alò, Silvia Bellesi, Elena Rossi, and Valerio De Stefano. 2020. "Venous Thromboembolism in Lymphoma: Risk Stratification and Antithrombotic Prophylaxis" Cancers 12, no. 5: 1291. https://doi.org/10.3390/cancers12051291
APA StyleHohaus, S., Bartolomei, F., Cuccaro, A., Maiolo, E., Alma, E., D’Alò, F., Bellesi, S., Rossi, E., & Stefano, V. D. (2020). Venous Thromboembolism in Lymphoma: Risk Stratification and Antithrombotic Prophylaxis. Cancers, 12(5), 1291. https://doi.org/10.3390/cancers12051291