Long-Term Follow-Up Outcomes after Percutaneous US/CT-Guided Radiofrequency Ablation for cT1a-b Renal Masses: Experience from Single High-Volume Referral Center

 ,
,  ,
, 
Abstract
1. Introduction
2. Results
2.1. General Characteristics of the Study Populations
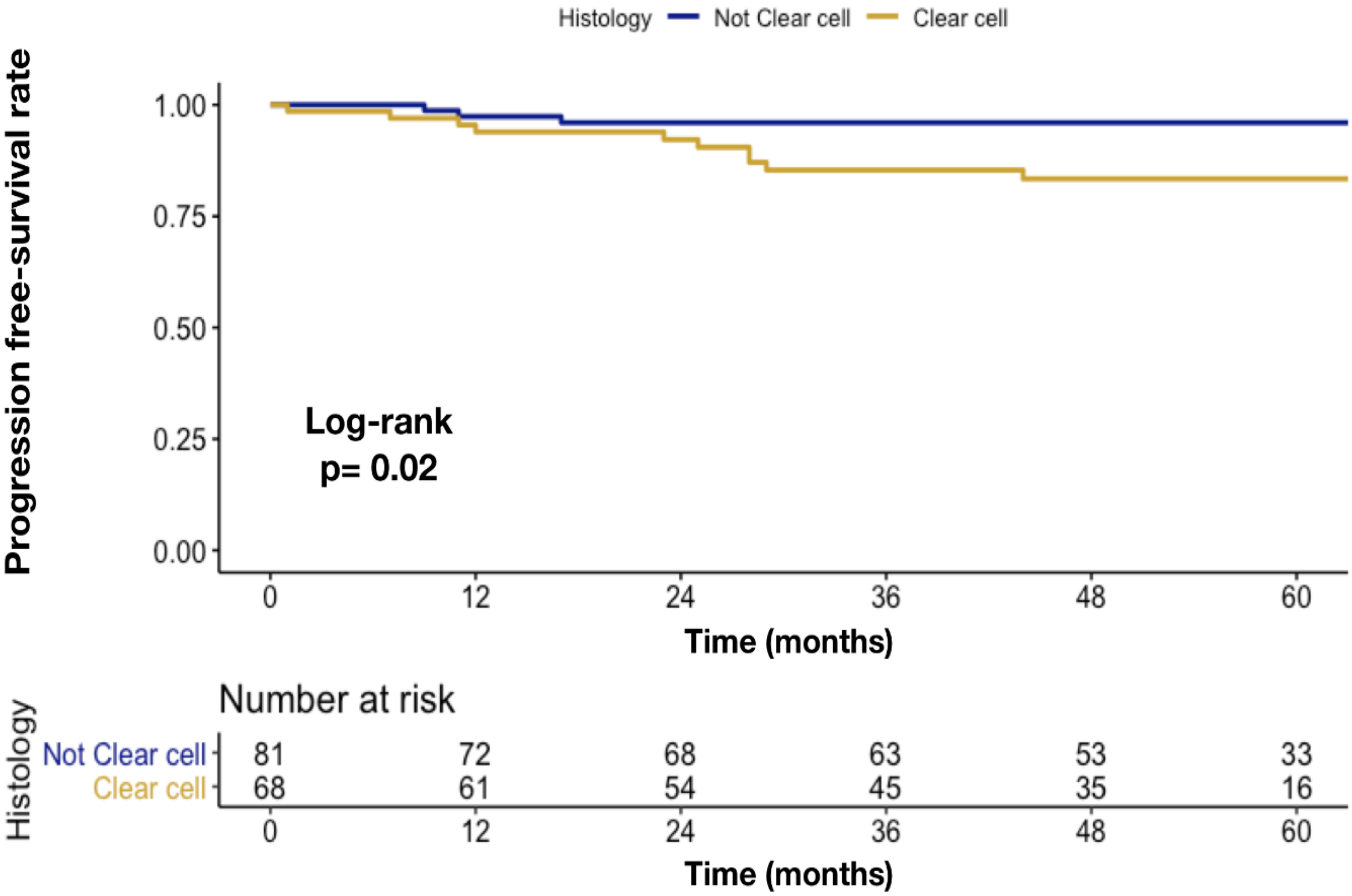
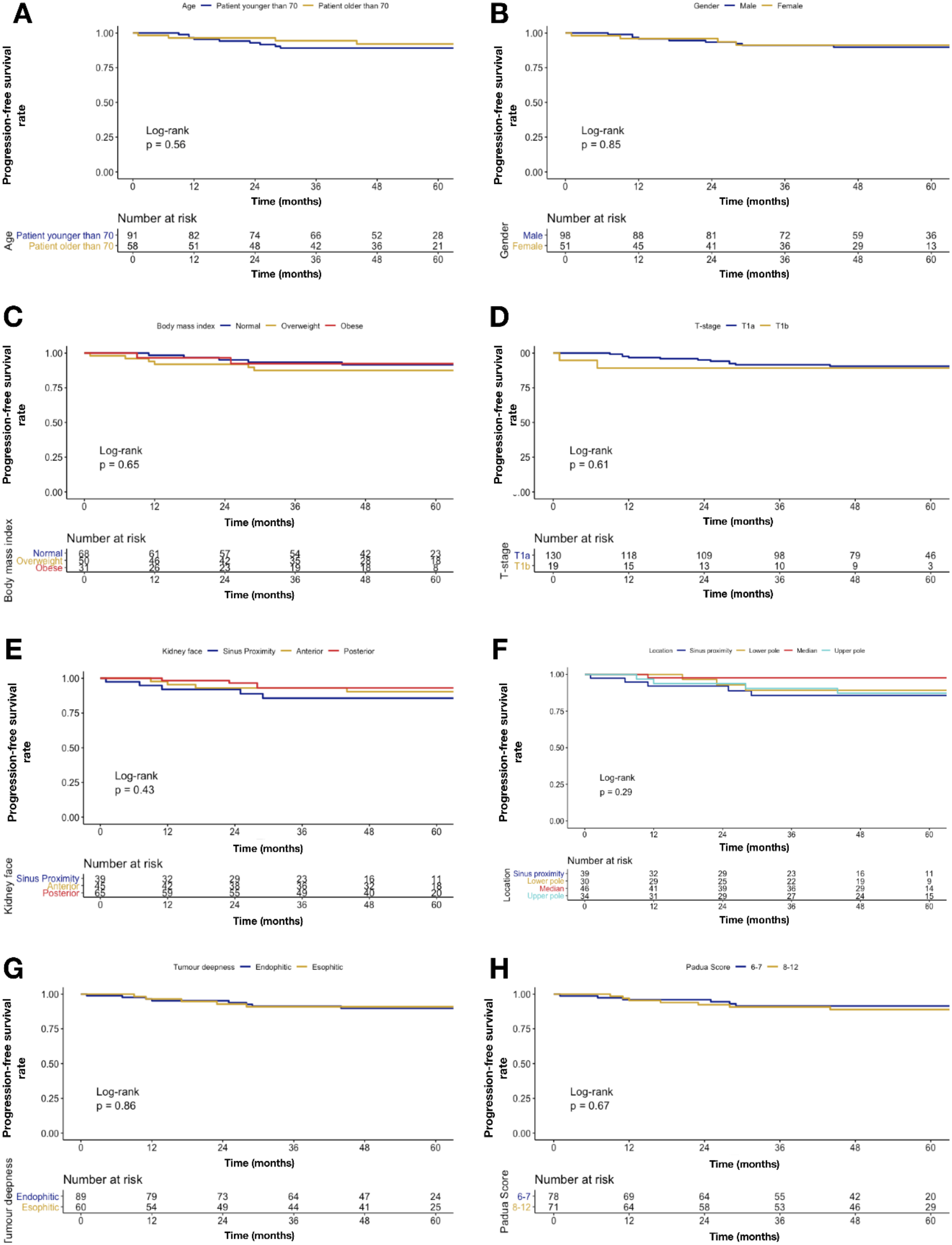
2.2. Primary Endpoints
2.3. Secondary Endpoints
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. RFA Procedure
4.3. Endpoints and Variables of Interest
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Znaor, A.; Lortet-Tieulent, J.; Laversanne, M.; Jemal, A.; Bray, F. International variations and trends in renal cell carcinoma incidence and mortality. Eur. Urol. 2015, 67, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Lightfoot, N.; Conlon, M.; Kreiger, N.; Bissett, R.; Desai, M.; Warde, P.; Prichard, H.M. Impact of noninvasive imaging on increased incidental detection of renal cell carcinoma. Eur. Urol. 2000, 37, 521–527. [Google Scholar] [CrossRef]
- Ljungberg, B.; Bensalah, K.; Canfield, S.; Dabestani, S.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur. Urol. 2015, 67, 913–924. [Google Scholar] [CrossRef]
- Katsanos, K.; Mailli, L.; Krokidis, M.; McGrath, A.; Sabharwal, T.; Adam, A. Systematic review and meta-analysis of thermal ablation versus surgical nephrectomy for small renal tumours. Cardiovasc. Interv. Radiol. 2014, 37, 427–437. [Google Scholar] [CrossRef]
- Mauri, G.; Nicosia, L.; Varano, G.M.; Bonomo, G.; Della Vigna, P.; Monfardini, L.; Orsi, F. Tips and tricks for a safe and effective image-guided percutaneous renal tumour ablation. Insights Imaging 2017, 8, 357–363. [Google Scholar] [CrossRef]
- Aarts, B.M.; Prevoo, W.; Meier, M.A.J.; Bex, A.; Beets-Tan, R.G.H.; Klompenhouwer, E.G.; Gomez, F.M. Percutaneous Microwave Ablation of Histologically Proven T1 Renal Cell Carcinoma. Cardiovasc. Interv. Radiol. 2020. [Google Scholar] [CrossRef]
- Filippiadis, D.; Mauri, G.; Marra, P.; Charalampopoulos, G.; Gennaro, N.; De Cobelli, F. Percutaneous ablation techniques for renal cell carcinoma: Current status and future trends. Int. J. Hyperth. 2019, 36, 21–30. [Google Scholar] [CrossRef]
- Jasinski, M.; Siekiera, J.; Chlosta, P.; Mikolajczak, W.; Drewa, T. Radiofrequency ablation of small renal masses as an alternative to nephron-sparing surgery: Preliminary results. Wideochirurgia i inne Tech. małoinwazyjne = Videosurgery other miniinvasive Tech./Kwart. Pod patronatem Sekc. Wideochirurgii TChP oraz Sekc. Chir. Bariatrycznej TChP 2011, 6, 242–245. [Google Scholar]
- Wah, T.M.; Irving, H.C.; Gregory, W.; Cartledge, J.; Joyce, A.D.; Selby, P.J. Radiofrequency ablation (RFA) of renal cell carcinoma (RCC): Experience in 200 tumours. BJU Int. 2014, 113, 416–428. [Google Scholar] [CrossRef]
- Krokidis, M.; Spiliopoulos, S.; Jarzabek, M.; Fotiadis, N.; Sabharwal, T.; O’Brien, T.; Adam, A. Percutaneous radiofrequency ablation of small renal tumours in patients with a single functioning kidney: Long-term results. Eur. Radiol. 2013, 23, 1933–1939. [Google Scholar] [CrossRef] [PubMed]
- Lyrdal, D.; Andersson, M.; Hellstrm, M.; Sternal, J.; Lundstam, S. Ultrasound-guided percutaneous radiofrequency ablation of small renal tumors: Clinical results and radiological evolution during follow-up. Acta Radiol. 2010, 51, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Sartori, S.; Mauri, G.; Tombesi, P.; Di Vece, F.; Bianchi, L.; Pacella, C.M. Ultrasound-guided percutaneous laser ablation is safe and effective in the treatment of small renal tumors in patients at increased bleeding risk. Int. J. Hyperth. 2018, 35, 1–7. [Google Scholar] [CrossRef]
- Kim, H.J.; Park, B.K.; Park, J.J.; Kim, C.K. CT-guided radiofrequency ablation of T1a renal cell carcinoma in korea: Mid-term outcomes. Korean J. Radiol. 2016, 17, 763–770. [Google Scholar] [CrossRef][Green Version]
- Zagoria, R.J.; Traver, M.A.; Werle, D.M.; Perini, M.; Hayasaka, S.; Clark, P.E. Oncologic efficacy of CT-guided percutaneous radiofrequency ablation of renal cell carcinomas. Am. J. Roentgenol. 2007, 189, 429–436. [Google Scholar] [CrossRef]
- Andersson, M.; Hashimi, F.; Lyrdal, D.; Lundstam, S.; Hellström, M. Improved outcome with combined US/CT guidance as compared to US guidance in percutaneous radiofrequency ablation of small renal masses. Acta Radiol. 2015, 56, 1519–1526. [Google Scholar] [CrossRef]
- Krokidis, M.E.; Orsi, F.; Katsanos, K.; Helmberger, T.; Adam, A. CIRSE Guidelines on Percutaneous Ablation of Small Renal Cell Carcinoma. Cardiovasc. Interv. Radiol. 2017, 40, 177–191. [Google Scholar] [CrossRef]
- Monfardini, L.; Gennaro, N.; Della Vigna, P.; Bonomo, G.; Varano, G.; Maiettini, D.; Bonello Solbiati, L.; Orsi, F.; Mauri, G. Cone-Beam CT-Assisted Ablation of Renal Tumors: Preliminary Results. Cardiovasc. Interv. Radiol. 2019, 42, 1718–1725. [Google Scholar] [CrossRef]
- Goldberg, S.N.; Gazelle, G.S.; Dawson, S.L.; Rittman, W.J.; Mueller, P.R.; Rosenthal, D.I. Tissue ablation with radiofrequency: Effect of probe size, gauge, duration, and temperature on lesion volume. Acad. Radiol. 1995, 2, 399–404. [Google Scholar] [CrossRef]
- Rossi, S.; Di Stasi, M.; Buscarini, E.; Cavanna, L.; Quaretti, P.; Squassante, E.; Garbagnati, F.; Buscarini, L. Percutaneous radiofrequency interstitial thermal ablation in the treatment of small hepatocellular carcinoma. Cancer J. Sci. Am. 1995, 1, 73–81. [Google Scholar]
- Kobayashi, M.; Sawada, S.; Morioka, N.; Kodani, K.; Iwamiya, T.; Senda, T.; Tanigawa, N.; Katoh, T.; Okuda, Y.; Hashimoto, M.; et al. Percutaneous radiofrequency coagulation therapy for liver tumor: Experimental study. Nihon Igaku Hoshasen Gakkai Zasshi 1994, 54, 530–532. [Google Scholar] [PubMed]
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- Zlotta, A.R.; Wildschutz, T.; Raviv, G.; Peny, M.-O.; van Gansbeke, D.; Noel, J.-C.; Schulman, C.C. Radiofrequency Interstitial Tumor Ablation (RITA) Is a Possible New Modality for Treatment of Renal Cancer: Ex Vivo and in Vivo Experience. J. Endourol. 1997, 11, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, T.; Obara, W. Committee for Establishment of the Clinical Practice Guideline for the Management of Renal Cell Carcinoma and the Japanese Urological Association. Evidence-based clinical practice guideline for renal cell carcinoma: The Japanese Urological Association 2011 update. Int. J. Urol. 2012, 19, 496–503. [Google Scholar]
- Campbell, S.C.; Novick, A.C.; Belldegrun, A.; Blute, M.L.; Chow, G.K.; Derweesh, I.H.; Faraday, M.M.; Kaouk, J.H.; Leveillee, R.J.; Matin, S.F.; et al. Guideline for Management of the Clinical T1 Renal Mass. J. Urol. 2009, 182, 1271–1279. [Google Scholar] [CrossRef]
- Wood, B.J.; Kruecker, J.; Abi-Jaoudeh, N.; Locklin, J.K.; Levy, E.; Xu, S.; Solbiati, L.; Kapoor, A.; Amalou, H.; Venkatesan, A.M. Navigation systems for ablation. J. Vasc. Interv. Radiol. 2010, 21, S257–S263. [Google Scholar] [CrossRef]
- Amalou, H.; Wood, B.J. Multimodality Fusion with MRI, CT, and Ultrasound Contrast for Ablation of Renal Cell Carcinoma. Case Rep. Urol. 2012, 2012, 390912. [Google Scholar] [CrossRef]
- Mauri, G.; De Beni, S.; Forzoni, L.; D’Onofrio, S.; Kolev, V.; Lagana, M.M.; Solbiati, L. Virtual navigator automatic registration technology in abdominal application. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2014, 2014, 5570–5574. [Google Scholar]
- Mauri, G.; Gennaro, N.; De Beni, S.; Ierace, T.; Goldberg, S.N.; Rodari, M.; Solbiati, L.A. Real-Time US-18FDG-PET/CT Image Fusion for Guidance of Thermal Ablation of 18FDG-PET-Positive Liver Metastases: The Added Value of Contrast Enhancement. Cardiovasc. Interv. Radiol. 2018, 42, 60–68. [Google Scholar] [CrossRef]
- Hao, G.; Hao, Y.; Cheng, Z.; Zhang, X.; Cao, F.; Yu, X.; Han, Z.; Liu, F.; Mu, M.; Dou, J. Local tumor progression after ultrasound-guided percutaneous microwave ablation of stage T1a renal cell carcinoma: Risk factors analysis of 171 tumors. Int. J. Hyperth. 2018, 35, 62–70. [Google Scholar] [CrossRef]
- Gervais, D.A.; Arellano, R.S.; McGovern, F.J.; McDougal, W.S.; Mueller, P.R. Radiofrequency Ablation of Renal Cell Carcinoma: Part 2, Lessons Learned with Ablation of 100 Tumors. Am. J. Roentgenol. 2005, 185, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, J.D.; Gervais, D.A.; Singh, S.; Kalra, M.K.; Sabir, S.H.; Paul, A.B.; Pandharipande, P.V. Radiation Exposure from CT-Guided Ablation of Renal Masses: Effects on Life Expectancy. Am. J. Roentgenol. 2015, 204, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Ierardi, A.M.; Carnevale, A.; Rossi, U.G.; Renzulli, M.; Garanzini, E.; Golfieri, R.; Macchione, N.; Cittanti, C.; Giganti, M.; Carrafiello, G. Percutaneous microwave ablation therapy of renal cancer local relapse after radical nephrectomy: A feasibility and efficacy study. Med. Oncol. 2020, 37, 27. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Zhang, X.; Liu, H.; Zhang, R.; Yu, X.; Cheng, Z.; Han, Z.; Liu, F.; Hao, G.; Mu, M.J.; et al. Percutaneous Microwave Ablation versus Laparoscopic Partial Nephrectomy for cT1a Renal Cell Carcinoma: A Propensity-matched Cohort Study of 1955 Patients. Radiology 2020, 294, 698–706. [Google Scholar] [CrossRef]
- Monfardini, L.; Varano, G.M.; Foà, R.; Della Vigna, P.; Bonomo, G.; Orsi, F. Local Recurrence of Renal Cancer After Surgery: Prime Time for Percutaneous Thermal Ablation? Cardiovasc. Interv. Radiol. 2015, 38, 1542–1547. [Google Scholar] [CrossRef]
- Ferrari, F.; Mauri, G.; Nicosia, L.; Varano, G.M.; Bonomo, G.; Orsi, F. Image-guided laser ablation in the treatment of recurrence of renal tumours: Technique and preliminary results. Eur. Radiol. Exp. 2020, 4, 1. [Google Scholar] [CrossRef]
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; Chen, M.H.; Choi, B.I.; de Baère, T.; Dodd, G.D.; et al. Image-guided Tumor Ablation: Standardization of Terminology and Reporting Criteria—A 10-Year Update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Overall (n 149) | |
|---|---|---|
| Age | Median | 67 |
| Interquartile Range | 60–75 | |
| Gender (n; (%)) | Male | 98 (65.8) |
| Female | 51 (34.2) | |
| Body mass index categories (n; (%)) | Normal | 68 (45.6) |
| Overweight | 50 (33.6) | |
| Obese | 31 (20.8) | |
| Tumor diameter (mm) | Median | 25 |
| Interquartile Range | 17–32 | |
| T-stage (n; (%)) | T1a | 130 (87.2) |
| T1b | 19 (12.8) | |
| Histovariant (n; (%)) | Clear cell | 68 (45.6) |
| Papillary | 12 (8.1) | |
| Benign | 13 (8.7) | |
| Chromophobe | 3 (2.0) | |
| Not diagnostic | 53 (35.6) | |
| Tumor laterality (n; (%)) | Right | 80 (53.7) |
| Left | 66 (44.3) | |
| Bilateral | 3 (2.0) | |
| Tumor location (n; (%)) | Anterior lower pole | 9 (6) |
| Anterior median | 17 (11.4) | |
| Anterior upper pole | 19 (12.8) | |
| Posterior lower pole | 21 (14.1) | |
| Posterior median | 29 (19.5) | |
| Posterior upper pole | 15 (10.1) | |
| Sinus proximity | 39 (26.2) | |
| Tumor deepness (n; (%)) | ≥50% intraparenchymal | 89 (59.7) |
| <50% intraparenchymal | 60 (40.3) | |
| Padua score | 6-7 | 71 (47.7) |
| 8-12 | 78 (52.3) | |
| Incomplete ablation (n; (%)) | Occurred | 10 (6.7) |
| Local tumor progression (n; (%)) | Occurred | 8 (5.4) |
| Distant tumor progression (n; (%)) | Occurred | 4 (2.7) |
| Retreatment rate (n; (%)) | Retreated | 27 (18.1) |
| Complication | A | 6 (4.0) |
| B | 0 (0) | |
| C | 5 (3.4) | |
| D | 2 (1.3) | |
| No complications | 136 (91.3) | |
| Overall mortality rate (n; (%)) | Occurred | 24 (16.1) |
| Characteristics | Overall (n 149) | ≤ 70 Years (n 91; 61.1%) | > 70 Years (n 58; 38.9%) | p Value | |
|---|---|---|---|---|---|
| Tumor diameter | Median | 25 | 23 | 30 | <0.01 |
| Interquartile Range | 17–32 | 15–28 | 20–38 | ||
| T-stage (n; (%)) | T1a | 130 (87.2) | 85 (93.4) | 45 (77.6) | 0.01 |
| T1b | 19 (12.8) | 6 (6.6) | 13 (22.4) | ||
| Characteristics | Overall (n 149) | Female (n 51; 34.2%) | Male (n 98; 65.8%) | p Value | |
| Tumor deepness (n; (%)) | ≥50% intraparenchymal | 89 (59.7) | 37 (72.5) | 52 (53.1) | 0.03 |
| <50% intraparenchymal | 60 (40.3) | 14 (27.5) | 46 (46.9) | ||
| Characteristics | Overall (n 149) | Normal (n 69; 45.6%) | Overweight/obese (n 81; 54.4%) | p Value | |
| Tumor diameter | Median | 25 | 23 | 26 | 0.02 |
| Interquartile Range | 17–32 | 16–30 | 17–38 | ||
| T-stage (n; (%)) | T1a | 130 (87.2) | 66 (97.1) | 64 (79.0) | <0.01 |
| T1b | 19 (12.8) | 2 (2.9) | 17 (21.0) | ||
| Padua score | 6–7 | 71 (47.7) | 40 (58.8) | 31 (38.3) | 0.02 |
| 8–12 | 78 (52.3) | 28 (41.2) | 50 (61.7) | ||
| Characteristics | Characteristics | Univariable Odds Ratio | 2.5% | 97.5% | p-Value |
|---|---|---|---|---|---|
| Tumor diameter | Continuously coded | 1.04 | 1.00 | 1.08 | 0.04 |
| T-stage | T1a | Ref. | Ref. | Ref. | Ref. |
| T1b | 1.75 | 0.52 | 5.13 | 0.3 | |
| Renal face location | Sinus proximity | Ref. | Ref. | Ref. | Ref. |
| Anterior | 0.37 | 0.12 | 1.02 | 0.1 | |
| Posterior | 0.24 | 0.08 | 0.66 | 0.01 | |
| Renal polar location | Sinus proximity | Ref. | Ref. | Ref. | Ref. |
| Lower | 0.40 | 0.11 | 1.23 | 0.1 | |
| Median | 0.19 | 0.05 | 0.60 | 0.01 | |
| Upper | 0.34 | 0.10 | 1.05 | 0.1 | |
| Tumor laterality | Right | Ref. | Ref. | Ref. | Ref. |
| Left | 1.39 | 0.58 | 3.33 | 0.5 | |
| Bilateral | 11.33 | 1.01 | 255.53 | 0.054 | |
| Tumor deepness | ≥50% intraparenchymal | Ref. | Ref. | Ref. | Ref. |
| <50% intraparenchymal | 0.46 | 0.17 | 1.11 | 0.1 | |
| Padua Score | 8–12 | Ref. | Ref. | Ref. | Ref. |
| 6–7 | 0.59 | 0.24 | 1.38 | 0.2 | |
| Histovariant | Not clear cell | Ref. | Ref. | Ref. | Ref. |
| Clear cell | 1.96 | 0.85 | 4.68 | 0.1 | |
| Gender | Male | Ref. | Ref. | Ref. | Ref. |
| Female | 0.77 | 0.30 | 1.86 | 0.6 | |
| Age | Continuously coded | 1.02 | 0.98 | 1.06 | 0.4 |
| Body mass index | Continuously coded | 1.02 | 0.94 | 1.09 | 0.6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauri, G.; Mistretta, F.A.; Bonomo, G.; Camisassi, N.; Conti, A.; Della Vigna, P.; Ferro, M.; Luzzago, S.; Maiettini, D.; Musi, G.; et al. Long-Term Follow-Up Outcomes after Percutaneous US/CT-Guided Radiofrequency Ablation for cT1a-b Renal Masses: Experience from Single High-Volume Referral Center. Cancers 2020, 12, 1183. https://doi.org/10.3390/cancers12051183
Mauri G, Mistretta FA, Bonomo G, Camisassi N, Conti A, Della Vigna P, Ferro M, Luzzago S, Maiettini D, Musi G, et al. Long-Term Follow-Up Outcomes after Percutaneous US/CT-Guided Radiofrequency Ablation for cT1a-b Renal Masses: Experience from Single High-Volume Referral Center. Cancers. 2020; 12(5):1183. https://doi.org/10.3390/cancers12051183
Chicago/Turabian StyleMauri, Giovanni, Francesco Alessandro Mistretta, Guido Bonomo, Nicola Camisassi, Andrea Conti, Paolo Della Vigna, Matteo Ferro, Stefano Luzzago, Daniele Maiettini, Gennaro Musi, and et al. 2020. "Long-Term Follow-Up Outcomes after Percutaneous US/CT-Guided Radiofrequency Ablation for cT1a-b Renal Masses: Experience from Single High-Volume Referral Center" Cancers 12, no. 5: 1183. https://doi.org/10.3390/cancers12051183
APA StyleMauri, G., Mistretta, F. A., Bonomo, G., Camisassi, N., Conti, A., Della Vigna, P., Ferro, M., Luzzago, S., Maiettini, D., Musi, G., Piacentini, N., Varano, G. M., de Cobelli, O., & Orsi, F. (2020). Long-Term Follow-Up Outcomes after Percutaneous US/CT-Guided Radiofrequency Ablation for cT1a-b Renal Masses: Experience from Single High-Volume Referral Center. Cancers, 12(5), 1183. https://doi.org/10.3390/cancers12051183