Prediction of High-Grade Clear Cell Renal Cell Carcinoma Based on Plasma mRNA Profiles in Patients with Localized Pathologic T1N0M0 Stage Disease

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics
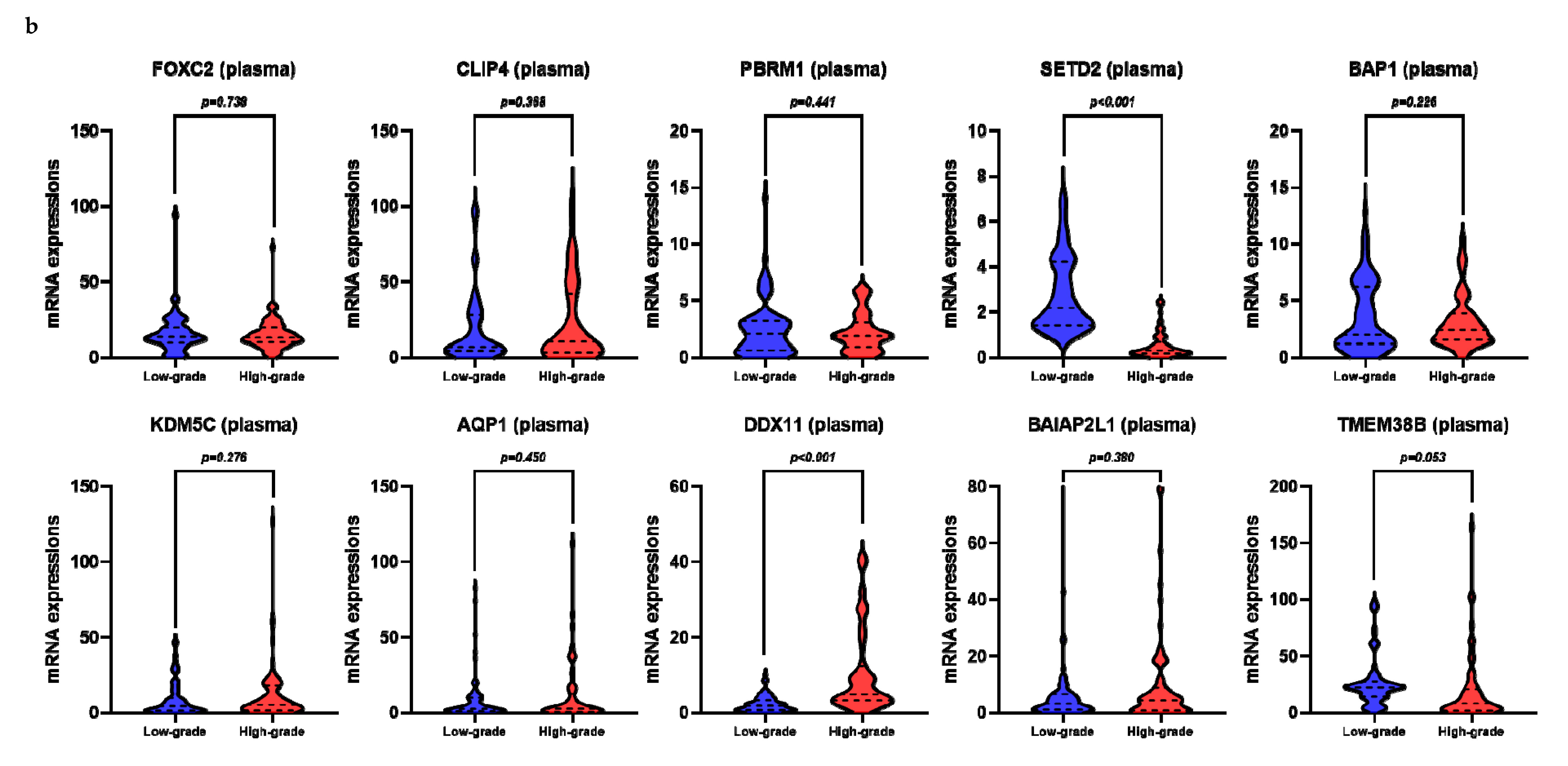
2.2. Expression of Target Genes in Frozen Tissue and Plasma
2.3. Correlation between mRNA Levels in the Frozen Tissue and Plasma
2.4. SETD2 and DDX11 Levels in Frozen Tissue and Plasma, in Accordance with the Fuhrman Grade
2.5. Prediction Model Comparison
3. Discussion
4. Materials and Methods
4.1. Patients and Tissues
4.2. Processing of Blood Samples
4.3. RNA Extraction and Reverse Transcription-Quantitative Polymerase Chain Reaction (RT-qPCR)
4.4. UALCAN Analysis
4.5. Statistical Analyses
4.6. Prediction Model Comparison
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of renal cell carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Capitanio, U.; Montorsi, F. Renal cancer. Lancet 2016, 387, 894–906. [Google Scholar] [CrossRef]
- Rini, B.I.; Campbell, S.C.; Escudier, B. Renal cell carcinoma. Lancet 2009, 373, 1119–1132. [Google Scholar] [CrossRef]
- Park, J.S.; Lee, H.J.; Cho, N.H.; Kim, J.; Jang, W.S.; Heo, J.E.; Ham, W.S. Risk prediction tool for aggressive tumors in clinical T1 stage clear cell renal cell carcinoma using molecular biomarkers. Comput. Struct. Biotechnol. J. 2019, 17, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Mizuno, R.; Mikami, S.; Tanaka, N.; Kanao, K.; Kikuchi, E.; Miyajima, A.; Nakagawa, K.; Oya, M. Prognostic significance of high nuclear grade in patients with pathologic T1a renal cell carcinoma. Jpn. J. Clin. Oncol. 2012, 42, 831–835. [Google Scholar] [CrossRef][Green Version]
- Mitchell, T.J.; Turajilic, S.; Rowan, A.; Nicol, D.; Farmery, J.H.; O’Brien, T.; Martincorena, I.; Tarpey, P.; Angelopoulos, N.; Yates, L.R.; et al. Timing the landmark events in the evolution of clear cell renal cell cancer: TRACERx Renal. Cell 2018, 173, 611. [Google Scholar] [CrossRef]
- Peña-Llopis, S.; Vega-Rubin-de-Celis, S.; Liao, A.; Leng, N.; Pavía-Jiménez, A.; Wang, S.; Yamasaki, T.; Zhrebker, L.; Sivanand, S.; Spence, P.; et al. BAP1 loss defines a new class of renal cell carcinoma. Nat. Genet. 2012, 44, 751. [Google Scholar] [CrossRef]
- Dalgliesh, G.L.; Furge, K.; Greenman, C.; Chen, L.; Bignell, G.; Butler, A.; Davies, H.; Edkins, S.; Hardy, C.; Latimer, C.; et al. Systematic sequencing of renal carcinoma reveals inactivation of histone modifying genes. Nature 2010, 463, 360. [Google Scholar] [CrossRef]
- Ahn, J.; Han, K.S.; Heo, J.H.; Bang, D.; Kang, Y.H.; Jin, H.A.; Hong, S.J.; Lee, J.H.; Ham, W.S. FOXC2 and CLIP4: A potential biomarker for synchronous metastasis of ≤7-cm clear cell renal cell carcinomas. Oncotarget 2016, 7, 51423. [Google Scholar] [CrossRef]
- Park, J.S.; Pierorazio, P.M.; Lee, J.H.; Lee, H.J.; Lim, Y.S.; Jang, W.S.; Kim, J.; Lee, S.H.; Rha, K.H.; Cho, N.H.; et al. Gene expression analysis of aggressive clinical T1 stage clear cell renal cell carcinoma for identifying potential diagnostic and prognostic biomarkers. Cancers 2020, 12, 222. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.J.; Modak, J.; Kopetz, S.; Murthy, R.; Yao, J.C.; Hicks, M.E.; Abbruzzese, J.L.; Tam, A.L. Use of research biopsies in clinical trials: Are risks and benefits adequately discussed? J. Clin. Oncol. 2013, 31, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Caoili, E.M.; Davenport, M.S. Role of percutaneous needle biopsy for renal masses. Semin Interv. Radiol. 2014, 31, 20–26. [Google Scholar]
- Leveridge, M.J.; Finelli, A.; Kachura, J.R.; Evans, A.; Chung, H.; Shiff, D.A.; Fernandes, K.; Jewett, M.A. Outcomes of small renal mass needle core biopsy, nondiagnostic percutaneous biopsy, and the role of repeat biopsy. Eur. Urol. 2011, 60, 578–584. [Google Scholar] [CrossRef]
- Neuzillet, Y.; Lechevallier, E.; Andre, M.; Daniel, L.; Coulange, C. Accuracy and clinical role of fine needle percutaneous biopsy with computerized tomography guidance of small (less than 4.0 cm) renal masses. J. Urol. 2004, 171, 1802–1805. [Google Scholar] [CrossRef]
- Wan, J.C.; Massie, C.; Garcia-Corbacho, J.; Mouliere, F.; Brenton, J.D.; Caldas, C.; Pacey, S.; Baird, R.; Rosenfeld, N. Liquid biopsies come of age: Towards implementation of circulating tumour DNA. Nat. Rev. Cancer 2017, 17, 223–238. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Uemura, M.; Fujita, M.; Maejima, K.; Koh, Y.; Matsushita, M.; Nakano, K.; Hayashi, Y.; Wang, C.; Ishizuya, Y.; et al. Clinical significance of the mutational landscape and fragmentation of circulating tumor DNA in renal cell carcinoma. Cancer Sci. 2019, 110, 617–628. [Google Scholar] [CrossRef]
- Pal, S.K.; Sonpavde, G.; Agarwal, N.; Vogelzang, N.J.; Srinivas, S.; Haas, N.B.; Signoretti, S.; McGregor, B.A.; Jones, J.; Lanman, R.B.; et al. Evolution of circulating tumor DNA profile from first-line to subsequent therapy in metastatic renal cell carcinoma. Eur. Urol. 2017, 72, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Ball, M.W.; Bezerra, S.M.; Gorin, M.A.; Cowan, M.; Pavlovich, C.P.; Pierorazio, P.M.; Netto, G.J.; Allaf, M.E. Grade heterogeneity in small renal masses: Potential implications for renal mass biopsy. J. Urol. 2015, 193, 36–40. [Google Scholar] [CrossRef]
- Bhattacharya, C.; Wang, X.; Becker, D. The DEAD/DEAH box helicase; DDX11; is essential for the survival of advanced melanomas. Mol. Cancer 2012, 11, 82. [Google Scholar] [CrossRef]
- Li, J.; Liu, L.; Liu, X.; Xu, P.; Hu, Q.; Yu, Y. The role of upregulated DDX11 as a potential prognostic and diagnostic biomarker in lung adenocarcinoma. J. Cancer 2019, 10, 4208–4216. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of clear cell renal cell carcinoma. Nature 2013, 499, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Hakimi, A.A.; Ostrovnaya, I.; Reva, B.; Schultz, N.; Chen, Y.B.; Gonen, M.; Liu, H.; Takeda, S.; Voss, M.H.; Tickoo, S.K.; et al. Adverse outcomes in clear cell renal cell carcinoma with mutations of 3p21 epigenetic regulators BAP1 and SETD2: A report by MSKCC and the KIRC TCGA research network. Clin. Cancer Res. 2013, 19, 3259–3267. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Guo, R.; Zhang, X.; Liang, Y.; Kong, F.; Wang, J.; Xu, Z. Loss of SETD2; but not H3K36me3; correlates with aggressive clinicopathological features of clear cell renal cell carcinoma patients. Biosci. Trends 2017, 11, 214–220. [Google Scholar] [CrossRef][Green Version]
- Al Sarakbi, W.; Sasi, W.; Jiang, W.G.; Roberts, T.; Newbold, R.F.; Mokbel, K. The mRNA expression of SETD2 in human breast cancer: Correlation with clinico-pathological parameters. BMC Cancer 2009, 9, 290. [Google Scholar] [CrossRef]
- Huang, Y.; Murakami, T.; Sano, F.; Kondo, K.; Nakaigawa, N.; Kishida, T.; Kubota, Y.; Nagashima, Y.; Yao, M. Expression of aquaporin 1 in primary renal tumors: A prognostic indicator for clear-cell renal cell carcinoma. Eur. Urol. 2009, 56, 690–698. [Google Scholar] [CrossRef]
- Dagher, J.; Delahunt, B.; Rioux-Leclercq, N.; Egevad, L.; Srigley, J.R.; Coughlin, G.; Dunglinson, N.; Gianduzzo, T.; Kua, B.; Malone, G.; et al. Clear cell renal cell carcinoma: Validation of World Health Organization/International Society of Urological Pathology grading. Histopathology 2017, 71, 918–925. [Google Scholar] [CrossRef]
- Manley, B.J.; Reznik, E.; Ghanaat, M.; Kashan, M.; Becerra, M.F.; Casuscelli, J.; Tennenbaum, D.; Redzematovic, A.; Carlo, M.I.; Sato, Y.; et al. Characterizing recurrent and lethal small renal masses in clear cell renal cell carcinoma using recurrent somatic mutations. Urol. Oncol. 2017, 17, 30549–30555. [Google Scholar] [CrossRef]
- Moch, H.; Humphrey, P.A.; Ulbright, T.M.; Reuter, V. WHO Classification of Tumours of the Urinary System and Male Genital Organs; International Agency for Research on Cancer (IARC) Press: Lyon, France, 2016. [Google Scholar]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Fuhrman, S.A.; Lasky, L.C.; Limas, C. Prognostic significance of morphologic parameters in renal cell carcinoma. Am. J. Surg. Pathol. 1982, 6, 655–663. [Google Scholar] [CrossRef]
- Delahunt, B.; Cheville, J.C.; Martignoni, G.; Humphrey, P.A.; Magi-Galluzzi, C.; McKenney, J.; Egevad, L.; Algaba, F.; Moch, H.; Grignon, D.J.; et al. The International Society of Urological Pathology (ISUP) grading system for renal cell carcinoma and other prognostic parameters. Am. J. Surg. Pathol. 2013, 37, 1490–1504. [Google Scholar] [CrossRef] [PubMed]
- UALCAN. Available online: http://ualcan.path.uab.edu (accessed on 21 April 2020).
- Lanczky, A.; Nagy, A.; Bottai, G.; Munkácsy, G.; Szabó, A.; Santarpia, L.; Győrffy, B. miRpower: A web-tool to validate survival-associated miRNAs utilizing expression data from 2178 breast cancer patients. Breast Cancer Res Treat. 2016, 160, 439–446. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Clinicopathological Data (n = 140) |
|---|---|
| Sex male/female | 97/43 (69.3/30.7%) |
| Age (years) | 56.0 ± 12.3 |
| Mean tumor diameter (cm) | 3.0 ± 1.5 |
| Median tumor diameter (cm) | 2.8 (1.7–4.0) |
| Fuhrman grade | |
| 1 | 7 (5.0%) |
| 2 | 63 (45.0%) |
| 3 | 58 (41.4%) |
| 4 | 12 (8.6%) |
| High-Grade ccRCC | Univariate β (95% CI) | pa | Multivariate β (95% CI) | pb |
|---|---|---|---|---|
| FOXC2 | 0.998 (0.982–1.014) | 0.792 | ||
| CLIP4 | 0.997 (0.988–1.007) | 0.548 | ||
| PBRM1 | 0.987 (0.961–1.013) | 0.321 | ||
| SETD2 | 0.303 (0.177–0.520) | <0.001 | 0.021 (0.001–0.466) | 0.014 |
| BAP1 | 1.620 (0.488–5.383) | 0.431 | ||
| KDM5C | 0.984 (0.876–1.107) | 0.794 | ||
| AQP1 | 0.012 (0.002–0.077) | <0.001 | ||
| DDX11 | 2.625 (1.811–3.805) | <0.001 | 6.116 (1.729–21.631) | 0.005 |
| BAIAP2L1 | 1.039 (0.942–1.146) | 0.446 | ||
| TMEM38B | 0.993 (0.959–1.029) | 0.700 | ||
| FOXC2 | 0.995 (0.967–1.024) | 0.736 | ||
| CLIP4 | 1.006 (0.993–1.019) | 0.367 | ||
| PBRM1 | 0.939 (0.800–1.102) | 0.440 | ||
| SETD2 | 0.045 (0.015–0.132) | <0.001 | 0.028 (0.007–0.119) | <0.001 |
| BAP1 | 0.926 (0.818–1.048) | 0.225 | ||
| KDM5C | 1.013 (0.989–1.037) | 0.289 | ||
| AQP1 | 1.008 (0.988–1.028) | 0.451 | ||
| DDX11 | 1.504 (1.255–1.803) | <0.001 | 1.496 (1.187–1.885) | 0.001 |
| BAIAP2L1 | 1.010 (0.988–1.033) | 0.384 | ||
| TMEM38B | 0.986 (0.972–1.001) | 0.062 |
| Included Variables in Models | Sensitivity | Specificity | PPV | NPV | Accuracy (%) | AUC (95% CI) |
|---|---|---|---|---|---|---|
| SETD2 (frozen tissue) | 0.84 | 0.59 | 0.84 | 0.59 | 71.43% | 0.779 (0.704–0.853) |
| DDX11 (frozen tissue) | 1.00 | 0.93 | 1.00 | 0.93 | 96.43% | 0.964 (0.931–0.997) |
| SETD2 + DDX11 (frozen tissue) | 0.97 | 0.99 | 0.97 | 0.99 | 97.86% | 0.997 (0.992–1.000) |
| SETD2 (plasma) | 0.86 | 1.00 | 1.00 | 0.86 | 92.86% | 0.952 (0.918–0.987) |
| DDX11 (plasma) | 0.84 | 0.70 | 0.84 | 0.70 | 77.14% | 0.836 (0.771–0.900) |
| SETD2 + DDX11 (plasma) | 0.93 | 0.93 | 0.93 | 0.93 | 92.86% | 0.971 (0.947–0.994) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.S.; Lee, H.J.; Almujalhem, A.; Althubiany, H.H.; A, A.A.; Jang, W.S.; Kim, J.; Lee, S.H.; Rha, K.H.; Ham, W.S. Prediction of High-Grade Clear Cell Renal Cell Carcinoma Based on Plasma mRNA Profiles in Patients with Localized Pathologic T1N0M0 Stage Disease. Cancers 2020, 12, 1182. https://doi.org/10.3390/cancers12051182
Park JS, Lee HJ, Almujalhem A, Althubiany HH, A AA, Jang WS, Kim J, Lee SH, Rha KH, Ham WS. Prediction of High-Grade Clear Cell Renal Cell Carcinoma Based on Plasma mRNA Profiles in Patients with Localized Pathologic T1N0M0 Stage Disease. Cancers. 2020; 12(5):1182. https://doi.org/10.3390/cancers12051182
Chicago/Turabian StylePark, Jee Soo, Hyo Jung Lee, Ahmad Almujalhem, Hatem Hamed Althubiany, Alqahatani Ali A, Won Sik Jang, Jongchan Kim, Seung Hwan Lee, Koon Ho Rha, and Won Sik Ham. 2020. "Prediction of High-Grade Clear Cell Renal Cell Carcinoma Based on Plasma mRNA Profiles in Patients with Localized Pathologic T1N0M0 Stage Disease" Cancers 12, no. 5: 1182. https://doi.org/10.3390/cancers12051182
APA StylePark, J. S., Lee, H. J., Almujalhem, A., Althubiany, H. H., A, A. A., Jang, W. S., Kim, J., Lee, S. H., Rha, K. H., & Ham, W. S. (2020). Prediction of High-Grade Clear Cell Renal Cell Carcinoma Based on Plasma mRNA Profiles in Patients with Localized Pathologic T1N0M0 Stage Disease. Cancers, 12(5), 1182. https://doi.org/10.3390/cancers12051182