Multicenter Retrospective Analysis of Second-Line Therapy after Gemcitabine Plus Nab-Paclitaxel in Advanced Pancreatic Cancer Patients

 ,
,  , ,
, , 
 and
and
Abstract
1. Introduction
2. Materials and Methods
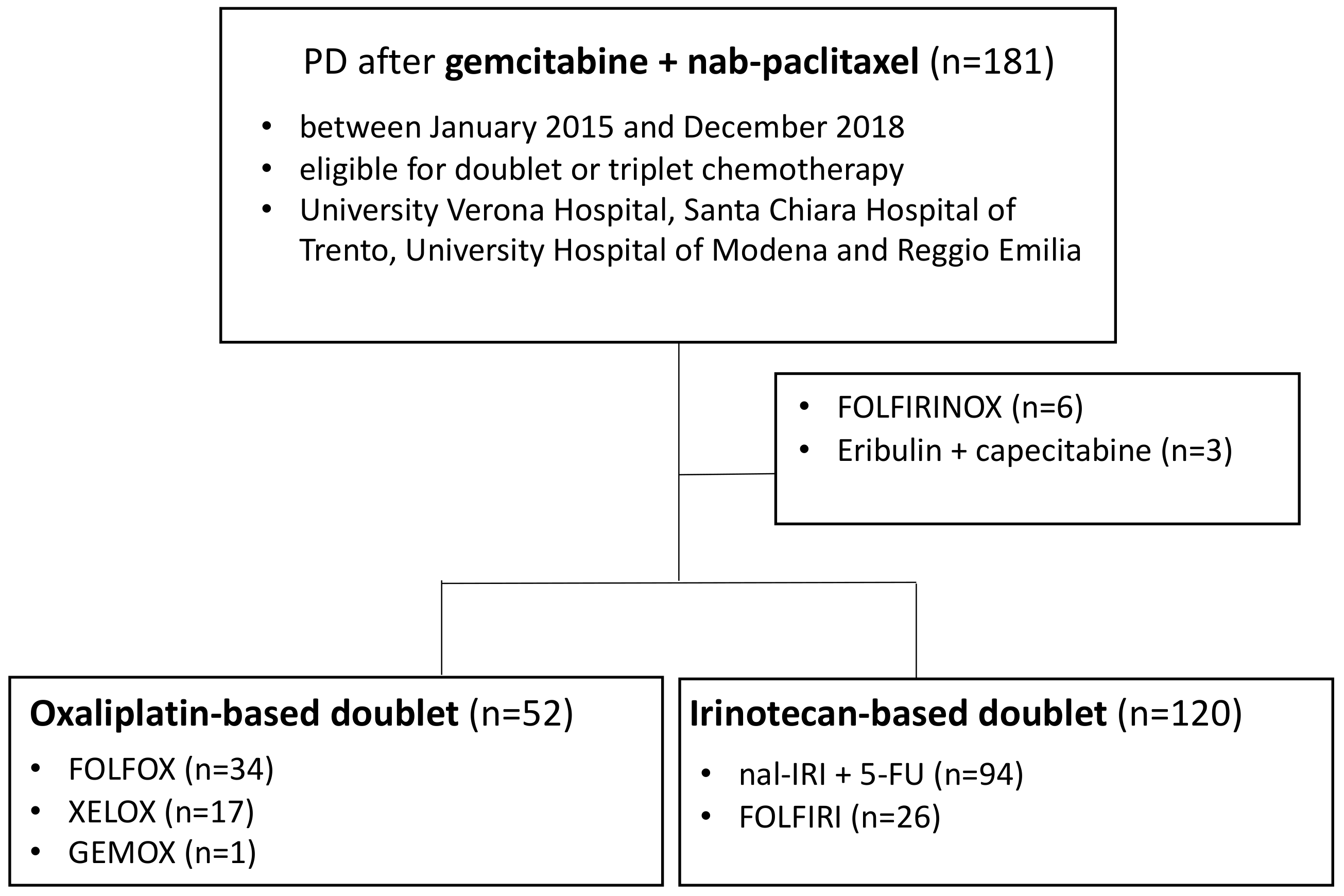
2.1. Population
2.2. Evaluation of Outcomes
2.3. Statistical Analysis
3. Results
3.1. Population
3.2. Survival Outcomes and Response Rates of Second-Line Therapies in the Overall Population
3.3. Second-Line Therapies in the Overall Population
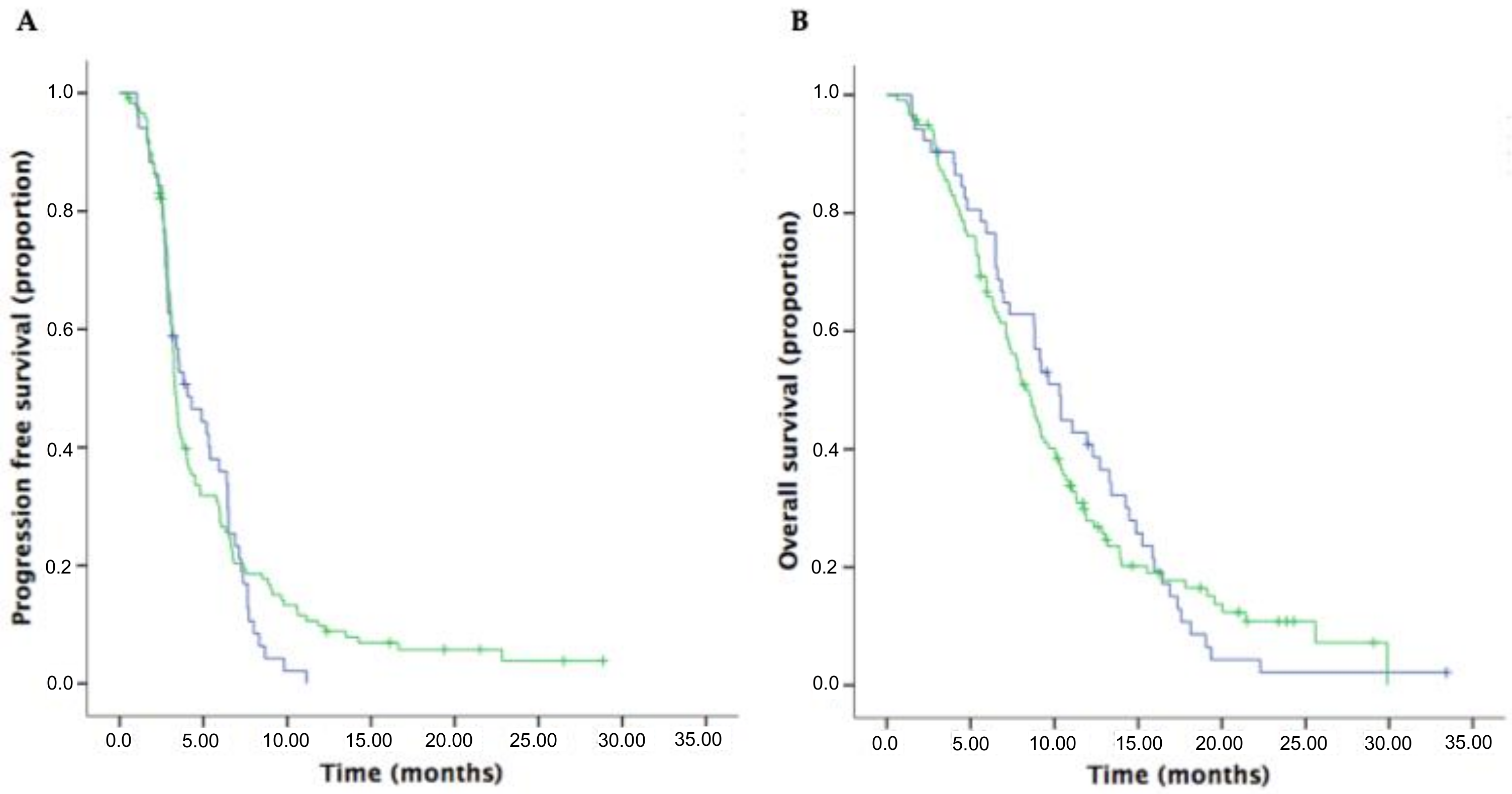
3.4. Survival Outcomes and Response Rates in Patients Receiving Oxaliplatin-Based and Irinotecan-Based Doublet Regimens in the Second-Line Setting
3.5. Survival Outcomes of First-Line Therapy in the Overall Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Melisi, D.; Calvetti, L.; Frizziero, M.; Tortora, G. Pancreatic cancer: Systemic combination therapies for a heterogeneous disease. Curr. Pharm. Des. 2014, 20, 6660–6669. [Google Scholar] [CrossRef]
- Melisi, D.; Budillon, A. Pancreatic cancer: Between bench and bedside. Curr. Drug Targets 2012, 13, 729–730. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Pourshams, A.; Sepanlou, S.G.; Ikuta, K.S.; Bisignano, C.; Safiri, S.; Roshandel, G.; Sharif, M.; Khatibian, M.; Fitzmaurice, C.; Nixon, M.R.; et al. The global, regional, and national burden of pancreatic cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2019, 4, 934–947. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; De La Fouchardiere, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; Prager, G.W.; Melisi, D.; Westphalen, C.B.; D’Esquermes, N.; Ferreras, A.; Carrato, A.; Macarulla, T. First-line and second-line treatment of patients with metastatic pancreatic adenocarcinoma in routine clinical practice across Europe: A retrospective, observational chart review study. ESMO Open 2020, 5, e000587. [Google Scholar] [CrossRef]
- Chiorean, E.G.; Von Hoff, D.D.; Tabernero, J.; El-Maraghi, R.; Ma, W.W.; Reni, M.; Manax, V. Second-line therapy after nab-paclitaxel plus gemcitabine or after gemcitabine for patients with metastatic pancreatic cancer. Br. J. Cancer 2016, 115, 188–194. [Google Scholar] [CrossRef]
- Aprile, G.; Negri, F.; Giuliani, F.; De Carlo, E.; Melisi, D.; Simionato, F.; Silvestris, N.; Brunetti, O.; Leone, F.; Marino, D.; et al. Second-line chemotherapy for advanced pancreatic cancer: Which is the best option? Crit. Rev. Oncol. 2017, 115, 1–12. [Google Scholar] [CrossRef]
- Pelzer, U.; Schwaner, I.; Stieler, J.M.; Adler, M.; Seraphin, J.; Dörken, B.; Riess, H.; Oettle, H. Best supportive care (BSC) versus oxaliplatin, folinic acid and 5-fluorouracil (OFF) plus BSC in patients for second-line advanced pancreatic cancer: A phase III-study from the German CONKO-study group. Eur. J. Cancer 2011, 47, 1676–1681. [Google Scholar] [CrossRef]
- Oettle, H.; Riess, H.; Stieler, J.M.; Heil, G.; Schwaner, I.; Seraphin, J.; Görner, M.; Mölle, M.; Greten, T.F.; Lakner, V.; et al. Second-Line Oxaliplatin, Folinic Acid, and Fluorouracil Versus Folinic Acid and Fluorouracil Alone for Gemcitabine-Refractory Pancreatic Cancer: Outcomes From the CONKO-003 Trial. J. Clin. Oncol. 2014, 32, 2423–2429. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Ko, Y.-J.; Cripps, C.; Beaudoin, A.; Dhesy-Thind, S.; Zulfiqar, M.; Zalewski, P.; Do, T.; Cano, P.; Lam, W.Y.H.; et al. PANCREOX: A Randomized Phase III Study of Fluorouracil/Leucovorin With or Without Oxaliplatin for Second-Line Advanced Pancreatic Cancer in Patients Who Have Received Gemcitabine-Based Chemotherapy. J. Clin. Oncol. 2016, 34, 3914–3920. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.R.; Lonardi, S.; Bendell, J.C.; Sim, H.-W.; Macarulla, T.; Lopez, C.D.; Van Cutsem, E.; Martin, A.J.M.; Park, J.O.; Greil, R.; et al. Randomized Phase III Study of FOLFOX Alone and with Pegilodecakin as Second-line Therapy in Patients with Metastatic Pancreatic Cancer (SEQUOIA). J. Clin. Oncol. 2020, 38, 637. [Google Scholar] [CrossRef]
- Wang-Gillam, A.; Li, C.-P.; Bodoky, G.; Dean, A.; Shan, Y.-S.; Jameson, G.; Macarulla, T.; Lee, K.-H.; Cunningham, D.; Blanc, J.F.; et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): A global, randomised, open-label, phase 3 trial. Lancet 2016, 387, 545–557. [Google Scholar] [CrossRef]
- Wang-Gillam, A.; Hubner, R.A.; Siveke, J.T.; Von Hoff, D.D.; Belanger, B.; de Jong, F.A.; Mirakhur, B.; Chen, L.T. NAPOLI-1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: Final overall survival analysis and characteristics of long-term survivors. Eur. J. Cancer 2019, 108, 78–87. [Google Scholar] [CrossRef]
- Hubner, R.A.; Cubillo, A.; Blanc, J.-F.; Melisi, D.; Von Hoff, D.D.; Wang-Gillam, A.; Chen, L.-T.; Becker, C.; Mamlouk, K.; Belanger, B.; et al. Quality of life in metastatic pancreatic cancer patients receiving liposomal irinotecan plus 5-fluorouracil and leucovorin. Eur. J. Cancer 2019, 106, 24–33. [Google Scholar] [CrossRef]
- Pelzer, U.; Blanc, J.-F.; Melisi, D.; Cubillo, A.; Von Hoff, D.D.; Wang-Gillam, A.; Chen, L.-T.; Siveke, J.T.; Wan, Y.; Solem, C.T.; et al. Quality-adjusted survival with combination nal-IRI+5-FU/LV vs 5-FU/LV alone in metastatic pancreatic cancer patients previously treated with gemcitabine-based therapy: A Q-TWiST analysis. Br. J. Cancer 2017, 116, 1247–1253. [Google Scholar] [CrossRef]
- Zaniboni, A.; Aitini, E.; Barni, S.; Ferrari, D.; Cascinu, S.; Catalano, V.; Valmadre, G.; Ferrara, D.; Veltri, E.; Codignola, C.; et al. FOLFIRI as second-line chemotherapy for advanced pancreatic cancer: A GISCAD multicenter phase II study. Cancer Chemother. Pharmacol. 2012, 69, 1641–1645. [Google Scholar] [CrossRef]
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 1491–1492. [Google Scholar] [CrossRef]
- O’Reilly, E.M.; Lee, J.W.; Zalupski, M.; Capanu, M.; Park, J.; Golan, T.; Tahover, E.; Lowery, M.A.; Chou, J.F.; Sahai, V.; et al. Randomized, Multicenter, Phase II Trial of Gemcitabine and Cisplatin With or Without Veliparib in Patients With Pancreas Adenocarcinoma and a Germline BRCA/PALB2 Mutation. J. Clin. Oncol. 2020, JCO1902931. [Google Scholar] [CrossRef]
- Kaufman, B.; Shapira-Frommer, R.; Schmutzler, R.K.; Audeh, M.W.; Friedlander, M.; Balmaña, J.; Rosengarten, O. Olaparib Monotherapy in Patients with Advanced Cancer and a Germline BRCA1/2 Mutation. J. Clin. Oncol. 2015, 33, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Shroff, R.T.; Hendifar, A.; McWilliams, R.R.; Geva, R.; Epelbaum, R.; Rolfe, L.; Goble, S.; Lin, K.K.; Biankin, A.V.; Giordano, H.; et al. Rucaparib Monotherapy in Patients With Pancreatic Cancer and a Known Deleterious BRCA Mutation. JCO Precis. Oncol. 2018, 2018, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v56–v68. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.A. NCCN Guidelines Updates: Pancreatic Cancer. J. Natl. Compr. Canc. Netw. 2019, 17, 603–605. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | n (%) |
|---|---|
| Sex | |
| female | 82 (45.4) |
| male | 99 (54.6) |
| Median age (years) | 64 (34-81) |
| ECOG PS | |
| 0 | 114 (62.9) |
| 1 | 49 (27.1) |
| 2 | 11 (6.0) |
| unknown | 7 (3.9) |
| Tumor location | |
| head | 92 (50.9) |
| body-tail | 87 (48.1) |
| unknown | 2 (1.2) |
| CA19.9 | |
| <40 U/mL | 24 (13.2) |
| ≥40 U/mL | 142 (78.5) |
| unknown | 15 (8.3) |
| BMI | |
| ≥25 | 42 (23.2) |
| 18.5–24.9 | 113 (62.5) |
| <18.5 | 13 (7.2) |
| unknown | 13 (7.2) |
| Metastatic sites | |
| liver | 130 (71.8) |
| peritoneum | 43 (23.8) |
| lung | 59 (32.6) |
| other | 16 (8.8) |
| Number of metastatic sites | |
| 0 | 3 (1.6) |
| 1 | 83 (45.9) |
| 2 | 59 (32.6) |
| ≥3 | 36 (19.9) |
| Previous procedures | |
| radiotherapy | 19 (10.4) |
| surgery | 42 (23.2) |
| Prior neoadjuvant therapy | 14 (7.7) |
| Prior adjuvant therapy | 16 (8.8) |
| Response | Overall Population n (%) | Oxaliplatin-Based Doublet n (%) | Irinotecan-Based Doublet n (%) |
|---|---|---|---|
| ORR | 18 (10.5) | 7 (13.7) | 11 (9.6) |
| PR | 16 (9.3) | 7 (13.7) | 9 (7.8) |
| CR | 2 (1.2) | 0 | 2 (1.7) |
| DCR | 56 (32.3) | 18 (35.2) | 35 (30.7) |
| SD | 38 (22.0) | 11 (21.5) | 24 (21.1) |
| PR | 16 (9.3) | 7 (13.7) | 9 (7.8) |
| CR | 2 (1.2) | 0 | 2 (1.7) |
| Variables | PFS | OS | ||
|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |
| p | p | p | p | |
| Sex | ||||
| Male vs. female | 0.935 | 0.274 | ||
| PS | ||||
| 0 vs. 1–2 | 0.062 | 0.077 | ||
| Pancreatic tumor site | ||||
| Head vs. body-tail | 0.639 | 0.318 | ||
| Previous surgery | ||||
| No vs. yes | 0.304 | 0.126 | ||
| Previous radiotherapy | ||||
| No vs. yes | 0.213 | 0.901 | ||
| Site of metastasis | ||||
| Liver (no vs. yes) | 0.865 | 0.051 | ||
| Lung (no vs. yes) | 0.048 | 0.060 | 0.624 | |
| Peritoneum (no vs. yes) | 0.123 | 0.237 | ||
| Bone (no vs. yes) | 0.002 | 0.004 | 0.070 | |
| BMI | ||||
| ≤25 vs. >25 kg/m2 | 0.099 | 0.058 | ||
| CA19.9 | ||||
| <40 vs. ≥40 U/mL | 0.069 | 0.172 | ||
| N/L ratio | ||||
| ≤5 vs. >5 | 0.770 | 0.809 | ||
| PFS | OS | |||||
|---|---|---|---|---|---|---|
| Characteristic | Oxaliplatin-Based Doublet Months (95%CI) | Irinotecan-Based Doublet Months (95%CI) | p | Oxaliplatin-Based Doublet Months (95%CI) | Irinotecan-Based Doublet Months (95%CI) | p |
| Sex | ||||||
| Male | 4.0 (2.2–6.0) | 3.2 (3.1–3.5) | 0.446 | 8.8 (8.0–9.6) | 8.0 (5.3–10.7) | 0.972 |
| Female | 3.5 (0.6–6.5) | 3.3 (3.0–3.7) | 0.901 | 11.9 (7.8–16) | 8.5 (6.9–10.1) | 0.550 |
| PS | ||||||
| 0 | 4.0 (1.4–6.7) | 3.6 (2.8–4.5) | 0.323 | 11.0 (8.1–14.0) | 9.1 (7.3–10.9) | 0.843 |
| 1–2 | 2.8 (1.7–4.1) | 2.8 (2.5–3.2) | 0.871 | 6.8 (5.2–8.5) | 5.9 (3.6–8.3) | 0.905 |
| Pancreatic tumor site | ||||||
| Head | 5.3 (3.9–6.9) | 3.3 (2.9–3.6) | 0.532 | 10.3 (6.3–14.3) | 8.0 (6.3–9.7) | 0.211 |
| Body-tail | 3.1 (2.2–4.1) | 3.5 (3.0–4.0) | 0.085 | 9.1 (7.2–11.1) | 8.9 (1.2–6.7) | 0.355 |
| Previous surgery | ||||||
| Yes | 5.1 (1.1–9.2) | 3.7 (2.6–4.9) | 0.450 | 10.3 (7.7–13.1) | 10.0 (6.9–13.2) | 0.621 |
| No | 3.8 (2.6–4.9) | 3.2 (3.0–3.5) | 0.855 | 9.2 (7.4–11.1) | 7.7 (6.2–9.3) | 0.417 |
| Previous radiotherapy | ||||||
| Yes | 7.1 (3.2–11.1) | 4.5 (1.1–7.8) | 0.813 | 12.7 (4.2–21.2) | 9.1 (7.9–10.6) | 0.679 |
| No | 3.5 (2.6–4.4) | 3.2 (3.1–3.4) | 0.428 | 9.2 (6.4–11.9) | 8.0 (6.6–9.4) | 0.789 |
| Site of metastasis | ||||||
| Liver | 3.5 (2.5–4.4) | 3.3 (2.9–3.9) | 0.361 | 9.2 (7.5–10.9) | 7.7 (6.6–8.9) | 0.831 |
| Lung | 3.0 (2.5–3.6) | 3.0 (2.6–3.5) | 0.903 | 8.8 (4.8–12.9) | 9.3 (7.1–11.6) | 0.889 |
| Peritoneum | 2.8 (2.3–3.5) | 2.9 (2.6–3.4) | 0.554 | 6.6 (5.0–8.2) | 7.7 (4.7–10.9) | 0.676 |
| Bone | 1.7 (-) | 2.1 (1.0–3.4) | 0.321 | 2.6 (-) | 7.7 (2.2–13.4) | 0.145 |
| BMI | ||||||
| ≤25 kg/m2 | 3.5 (1.9–5.1) | 3.2 (2.9–3.6) | 0.751 | 9.1 (5.8–12.5) | 8.0 (6.8–9.2) | 0.792 |
| >25 kg/m2 | 4.0 (1.8–6.3) | 3.7 (0.6–7.0) | 0.415 | 10.3 (4.1–16.7) | 10.0 (7.0–13.1) | 0.639 |
| CA19.9 | ||||||
| <40 U/mL | 6.5 (5.5–7.5) | 4.0 (2.8–5.2) | 0.857 | 14.8 (13.0–16.7) | 7.4 (4.9–9.9) | 0.959 |
| ≥40 U/mL | 3.5 (2.4–4.6) | 3.2 (3.0–3.5) | 0.482 | 9.6 (8.0–11.3) | 8.6 (7.4–9.9) | 0.827 |
| N/L ratio | ||||||
| ≤5 | 3.8 (2.6–5.1) | 3.3 (3.2–3.6) | 0.364 | 10.3 (7.8–12.9) | 8.0 (6.4–9.7) | 0.564 |
| >5 | 6.4 (6.3–6.6) | 2.8 (2.6–3.2) | 0.384 | 12.2 (7.0–17.5) | 7.7 (3.6–11.8) | 0.816 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merz, V.; Cavaliere, A.; Messina, C.; Salati, M.; Zecchetto, C.; Casalino, S.; Milella, M.; Caffo, O.; Melisi, D. Multicenter Retrospective Analysis of Second-Line Therapy after Gemcitabine Plus Nab-Paclitaxel in Advanced Pancreatic Cancer Patients. Cancers 2020, 12, 1131. https://doi.org/10.3390/cancers12051131
Merz V, Cavaliere A, Messina C, Salati M, Zecchetto C, Casalino S, Milella M, Caffo O, Melisi D. Multicenter Retrospective Analysis of Second-Line Therapy after Gemcitabine Plus Nab-Paclitaxel in Advanced Pancreatic Cancer Patients. Cancers. 2020; 12(5):1131. https://doi.org/10.3390/cancers12051131
Chicago/Turabian StyleMerz, Valeria, Alessandro Cavaliere, Carlo Messina, Massimiliano Salati, Camilla Zecchetto, Simona Casalino, Michele Milella, Orazio Caffo, and Davide Melisi. 2020. "Multicenter Retrospective Analysis of Second-Line Therapy after Gemcitabine Plus Nab-Paclitaxel in Advanced Pancreatic Cancer Patients" Cancers 12, no. 5: 1131. https://doi.org/10.3390/cancers12051131
APA StyleMerz, V., Cavaliere, A., Messina, C., Salati, M., Zecchetto, C., Casalino, S., Milella, M., Caffo, O., & Melisi, D. (2020). Multicenter Retrospective Analysis of Second-Line Therapy after Gemcitabine Plus Nab-Paclitaxel in Advanced Pancreatic Cancer Patients. Cancers, 12(5), 1131. https://doi.org/10.3390/cancers12051131