Survival of Patients with Hepatocellular Carcinoma in Renal Insufficiency: Prognostic Role of Albumin-Bilirubin Grade

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Diagnosis and Definitions
2.3. Treatment
2.4. Statistics
3. Results
3.1. Patient Characteristics
3.2. Survival Prognostic Predictors
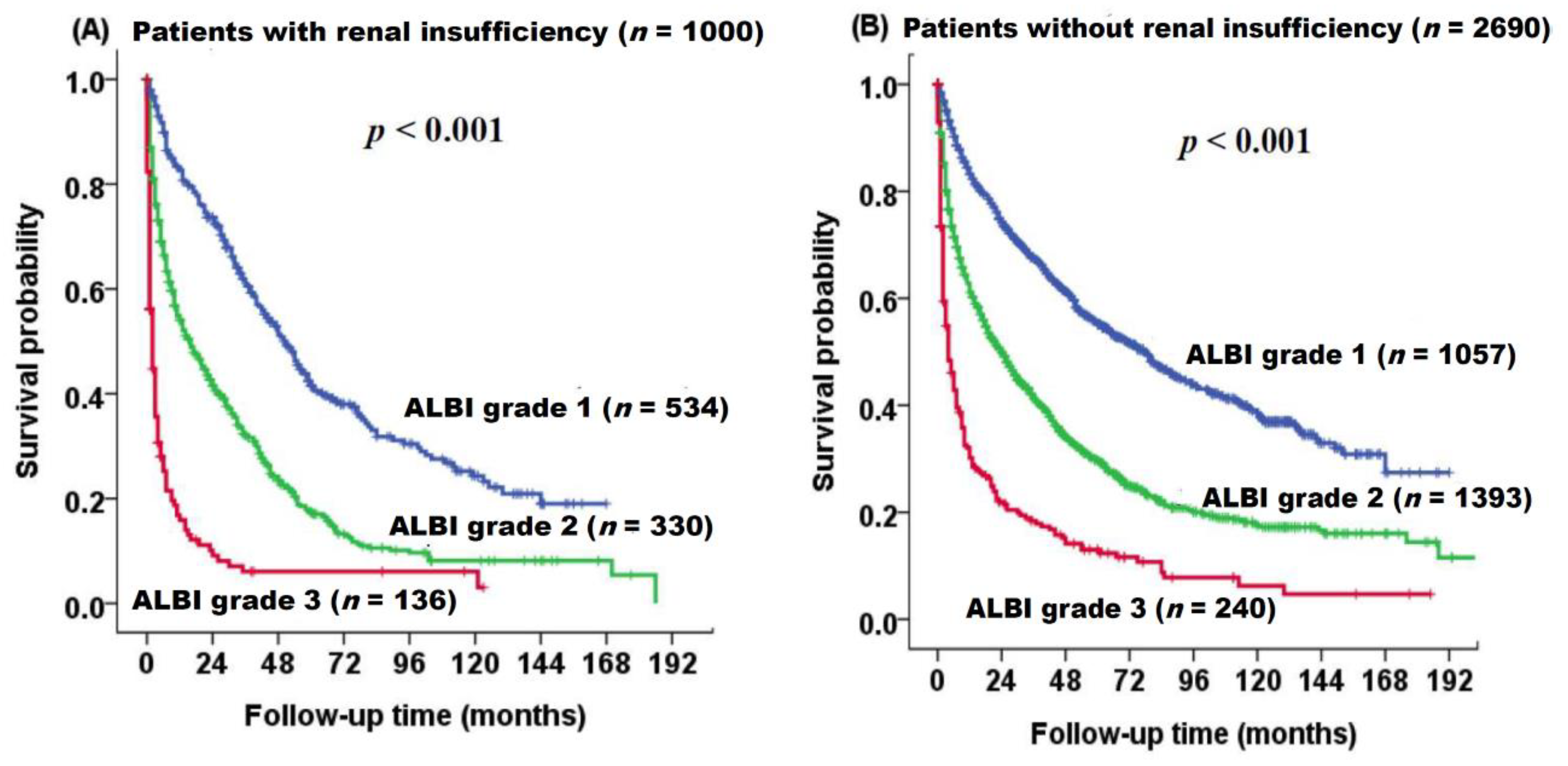
3.3. Survival of Patients with and without RI Based on ALBI Grade
3.4. Prognostic Predictors in Patients with RI
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ALBI | albumin-bilirubin |
| ALT | alanine aminotransferase |
| Anti-HCV | antibody for hepatitis C virus |
| AST | aspartate aminotransferase |
| AFP | α-fetoprotein |
| BCLC | Barcelona Clinic Liver Cancer |
| CTP | Child–Turcotte–Pugh |
| eGFR | estimated glomerular filtration rate |
| DM | diabetes mellitus |
| HBsAg | hepatitis B surface antigen |
| HBV | hepatitis B virus |
| HCV | hepatitis C virus |
| HR | hazard ratio |
| INR of PT | international normalized ratio of prothrombin time |
| MDRD | modification of diet in renal disease |
| MELD | model of end-stage liver disease |
| TACE | transarterial chemoembolization |
| RI | renal insufficiency |
| SD | standard deviation |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Surveillance group; Diagnosis group; Staging group; Surgery group; Local ablation group; group TTH; Target therapy/systemic therapy group; Radiotherapy group; Prevention group; Drafting group. Management consensus guideline for hepatocellular carcinoma: 2016 updated by the Taiwan Liver Cancer Association and the Gastroenterological Society of Taiwan. J. Formos Med. Assoc. 2018, 117, 381–403. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Li, D.; Sedano, S.; Allen, R.; Gong, J.; Cho, M.; Sharma, S. Current Treatment Landscape for Advanced Hepatocellular Carcinoma: Patient Outcomes and the Impact on Quality of Life. Cancers 2019, 11, 841. [Google Scholar] [CrossRef] [PubMed]
- Ginès, P.; Schrier, R.W. Renal failure in cirrhosis. N. Engl. J. Med. 2009, 361, 1279–1290. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E. Summary of KDIGO 2012 CKD Guideline: Behind the scenes, need for guidance, and a framework for moving forward. Kidney Int. 2014, 85, 49–61. [Google Scholar] [CrossRef]
- Hsu, C.-Y.; Hsia, C.-Y.; Huang, Y.-H.; Su, C.-W.; Lin, H.-C.; Chiou, Y.-Y.; Lee, R.-C.; Lee, F.-Y.; Huo, T.-I.; Lee, S.-D. Differential prognostic impact of renal insufficiency on patients with hepatocellular carcinoma: A propensity score analysis and staging strategy. J. Gastroenterol. Hepatol. 2012, 27, 690–699. [Google Scholar] [CrossRef]
- Huo, T.I.; Huang, Y.H.; Wu, J.C.; Lee, P.C.; Chang, F.Y.; Lee, S.D. Percutaneous injection therapy for hepatocellular carcinoma in patients with chronic renal insufficiency. Eur. J. Gastroenterol. Hepatol. 2004, 16, 325–331. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Huang, Y.H.; Su, C.W.; Chiang, J.H.; Lin, H.C.; Lee, P.C.; Lee, F.Y.; Huo, T.I.; Lee, S.D. Transarterial chemoembolization in patients with hepatocellular carcinoma and renal insufficiency. J. Clin. Gastroenterol. 2010, 44, e171–e177. [Google Scholar] [CrossRef]
- Orii, T.; Takayama, T.; Haga, I.; Fukumori, T.; Amada, N. Efficacy of a liver resection for hepatocellular carcinoma in patients with chronic renal failure. Surg. Today 2008, 38, 329–334. [Google Scholar] [CrossRef]
- Antkowiak, M.; Gabr, A.; Das, A.; Ali, R.; Kulik, L.; Ganger, D.; Moore, C.; Abecassis, M.; Katariya, N.; Mouli, S.; et al. Prognostic role of albumin, bilirubin, and ALBI scores: Analysis of 1000 patients with hepatocellular carcinoma undergoing radioembolization. Cancers 2019, 11, 879. [Google Scholar] [CrossRef]
- Wiesner, R.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003, 124, 91–96. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Huo, T.I. ALBI grade as a new player in hepatocellular carcinoma. J. Chin. Med. Assoc. 2019, 82, 1. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Sharma, R.; Allara, E.; Yen, C.; Arizumi, T.; Kubota, K.; Bettinger, D.; Jang, J.W.; Smirne, C.; Kim, Y.W.; et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J. Hepatol. 2017, 66, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.Y.; Hsu, C.Y.; Liu, P.H.; Hsia, C.Y.; Lei, H.J.; Huang, Y.H.; Ko, C.C.; Su, C.W.; Lee, R.C.; Hou, M.C.; et al. Albumin-bilirubin grade-based nomogram of the BCLC system for personalized prognostic prediction in hepatocellular carcinoma. Liver Int. 2020, 40, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Yang, H.I.; Liu, J.; Batrla-Utermann, R.; Jen, C.L.; Iloeje, U.H.; Lu, S.N.; You, S.L.; Wang, L.Y.; Chen, C.J. Prediction models of long-term cirrhosis and hepatocellular carcinoma risk in chronic hepatitis B patients: Risk scores integrating host and virus profiles. Hepatology 2013, 58, 546–554. [Google Scholar] [CrossRef]
- Gholam, P.M.; Iyer, R.; Johnson, M.S. Multidisciplinary management of patients with unresectable hepatocellular carcinoma: A critical appraisal of current evidence. Cancers 2019, 11, 873. [Google Scholar] [CrossRef]
- EASL. Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Lee, Y.H.; Hsia, C.Y.; Huang, Y.H.; Su, C.W.; Lin, H.C.; Lee, R.C.; Chiou, Y.Y.; Lee, F.Y.; Huo, T.I. Performance status in patients with hepatocellular carcinoma: Determinants, prognostic impact, and ability to improve the Barcelona Clinic Liver Cancer system. Hepatology 2013, 57, 112–119. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Huang, Y.H.; Hsia, C.Y.; Su, C.W.; Lin, H.C.; Loong, C.C.; Chiou, Y.Y.; Chiang, J.H.; Lee, P.C.; Huo, T.I.; et al. A new prognostic model for hepatocellular carcinoma based on total tumor volume: The Taipei Integrated Scoring System. J. Hepatol. 2010, 53, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Hsia, C.Y.; Huang, Y.H.; Su, C.W.; Lin, H.C.; Pai, J.T.; Loong, C.C.; Chiou, Y.Y.; Lee, R.C.; Lee, F.Y.; et al. Comparison of surgical resection and transarterial chemoembolization for hepatocellular carcinoma beyond the Milan criteria: A propensity score analysis. Ann. Surg. Oncol. 2012, 19, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Peng, K.; Hu, D.; Shen, J.; Zhou, Z.; Xu, L.; Chen, J.; Pan, Y.; Wang, J.; Zhang, Y.; et al. Tumor location influences oncologic outcomes of hepatocellular carcinoma patients undergoing radiofrequency ablation. Cancers 2018, 10, 378. [Google Scholar] [CrossRef]
- Yoon, J.S.; Sinn, D.H.; Lee, J.H.; Kim, H.Y.; Lee, C.H.; Kim, S.W.; Lee, H.Y.; Nam, J.Y.; Chang, Y.; Lee, Y.B.; et al. Tumor marker-based definition of the transarterial chemoembolization-refractoriness in intermediate-stage hepatocellular carcinoma: A multi-cohort study. Cancers 2019, 11, 1721. [Google Scholar] [CrossRef]
- Hampel, H.; Bynum, G.D.; Zamora, E.; El-Serag, H.B. Risk factors for the development of renal dysfunction in hospitalized patients with cirrhosis. Am. J. Gastroenterol. 2001, 96, 2206–2210. [Google Scholar] [CrossRef]
- Huo, T.I.; Hsu, C.Y.; Huang, Y.H.; Hsia, C.Y.; Lin, H.C.; Lee, P.C.; Loong, C.C.; Chiang, J.H.; Chiou, Y.Y.; Lee, S.D. Diabetes mellitus as an independent prognostic predictor and its association with renal dysfunction in patients with hepatocellular carcinoma. Liver Int. 2010, 30, 198–207. [Google Scholar] [CrossRef]
- Lee, C.H.; Hsieh, S.Y.; Lin, J.L.; Liu, M.S.; Yen, T.H. Hepatocellular carcinoma in patients with chronic kidney disease. World J. Gastroenterol. 2013, 19, 2466–2472. [Google Scholar] [CrossRef]
- Botta, F.; Giannini, E.; Romagnoli, P.; Fasoli, A.; Malfatti, F.; Chiarbonello, B.; Testa, E.; Risso, D.; Colla, G.; Testa, R. MELD scoring system is useful for predicting prognosis in patients with liver cirrhosis and is correlated with residual liver function: A European study. Gut 2003, 52, 134–139. [Google Scholar] [CrossRef]
- Huo, T.I.; Lin, H.C.; Huang, Y.H.; Wu, J.C.; Chiang, J.H.; Lee, P.C.; Lee, S.D. The model for end-stage liver disease-based Japan Integrated Scoring system may have a better predictive ability for patients with hepatocellular carcinoma undergoing locoregional therapy. Cancer 2006, 107, 141–148. [Google Scholar] [CrossRef]
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Huang, Y.H.; Su, C.W.; Lin, H.C.; Chiang, J.H.; Lee, P.C.; Lee, F.Y.; Huo, T.I.; Lee, S.D. Renal failure in patients with hepatocellular carcinoma and ascites undergoing transarterial chemoembolization. Liver Int. 2010, 30, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Hsu, C.Y.; Huang, Y.H.; Hsia, C.Y.; Chiou, Y.Y.; Su, C.W.; Lin, H.C.; Huo, T.I. Vascular invasion in hepatocellular carcinoma: Prevalence, determinants and prognostic impact. J. Clin. Gastroenterol. 2014, 48, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Lee, Y.H.; Huang, Y.H.; Hsia, C.Y.; Su, C.W.; Lin, H.C.; Lee, R.C.; Chiou, Y.Y.; Lee, F.Y.; Huo, T.I.; et al. Ascites in patients with hepatocellular carcinoma: Prevalence, associated factors, prognostic impact, and staging strategy. Hepatol. Int. 2013, 7, 188–198. [Google Scholar] [CrossRef] [PubMed]
- EASL. Clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J. Hepatol. 2010, 53, 397–417. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Hiraoka, A.; Tada, T.; Michitaka, K.; Takaguchi, K.; Tsuji, K.; Itobayashi, E.; Takizawa, D.; Hirooka, M.; Koizumi, Y.; et al. Characteristics and prognosis of hepatocellular carcinoma in japanese patients undergoing dialysis. Ther. Apher. Dial. 2017, 21, 465–472. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 3690) | Patients with RI (n = 1000) | Patients without RI (n = 2690) | p-Value | |
|---|---|---|---|---|---|
| Age (years, mean ± SD) | 65 ± 13 | 72 ± 11 | 62 ± 13 | <0.001 | |
| Male/Female, n (%) | 2815/875 (76/24) | 732/268 (73/27) | 2083/83 (77/23) | 0.008 | |
| Etiologies of liver disease | <0.001 | ||||
| HBV, n (%) | 1475 (40) | 308 (31) | 1165 (43) | ||
| HCV, n (%) | 809 (22) | 249 (25) | 560 (21) | ||
| HBV + HCV, (%) | 133 (4) | 35 (4) | 98 (4) | ||
| Others, (%) | 1275 (35) | 408 (40) | 867 (32) | ||
| Laboratory values (mean ± SD) | |||||
| Albumin (g/L) | 3.6 ± 0.6 | 3.5 ± 0.7 | 3.7 ± 0.6 | 0.001 | |
| Bilirubin (mg/dL) | 1.5 ± 2.9 | 1.7 ± 3.9 | 1.5 ± 2.4 | 0.003 | |
| ALT (IU/L) | 69 ± 88 | 63 ± 94 | 72 ± 85 | 0.043 | |
| AST (IU/L) | 98 ± 207 | 113 ± 345 | 94 ± 120 | 0.399 | |
| Creatinine (mg/dL) | 1.2 ± 1.1 | 2.0 ± 1.9 | 0.9 ± 0.2 | <0.001 | |
| Sodium (mmol/L) | 138 ± 5 | 137 ± 6 | 139 ± 4 | 0.001 | |
| INR of PT | 1.1 ± 0.2 | 1.1 ± 0.3 | 1.1 ± 0.1 | 0.615 | |
| Platelet (1000 uL/L) | 172 ± 110 | 170 ± 101 | 173 ± 113 | 0.371 | |
| AFP (ng/mL) median (IQR) | 44 (8–794) | 31 (6–886) | 51 (9–764) | 0.004 | |
| Tumor nodules (single/multiple), n (%) | 2354/1336 (64/36) | 653/347 (65/35) | 1701/989 (63/37) | 0.248 | |
| Tumor size, Mean ± SD | 6.03 ± 4.5 | 6.22 ± 4.5 | 5.97 ± 4.5 | 0.766 | |
| Tumor size >3 cm, n (%) | 2407 (65) | 681 (68) | 1726 (64) | 0.026 | |
| TTV median, (IQR) Mean ± SD | 47 (9–381) | 65 (10–609) 391 ± 844 | 47 (9–381) 372 ± 732 | 0.382 | |
| Vascular invasion, n (%) | 897 (24) | 227 (23) | 670 (25) | 0.167 | |
| Distant metastasis, n (%) | 355 (10) | 103 (10) | 252 (9) | 0.414 | |
| Ascites, n (%) | 837 (23) | 261 (26) | 576 (21) | 0.003 | |
| DM, n (%) | 936 (26) | 360 (36) | 576 (21) | <0.001 | |
| CTP class (A/B/C), n (%) | 2706/812/172 (73/22/5) | 718/226/56 (72/22/6) | 2169/451/70 (80/17/3) | <0.001 | |
| CTP score (mean ± SD) | 6.1 ± 1.5 | 6.4 ± 1.8 | 6.0 ± 1.4 | 0.254 | |
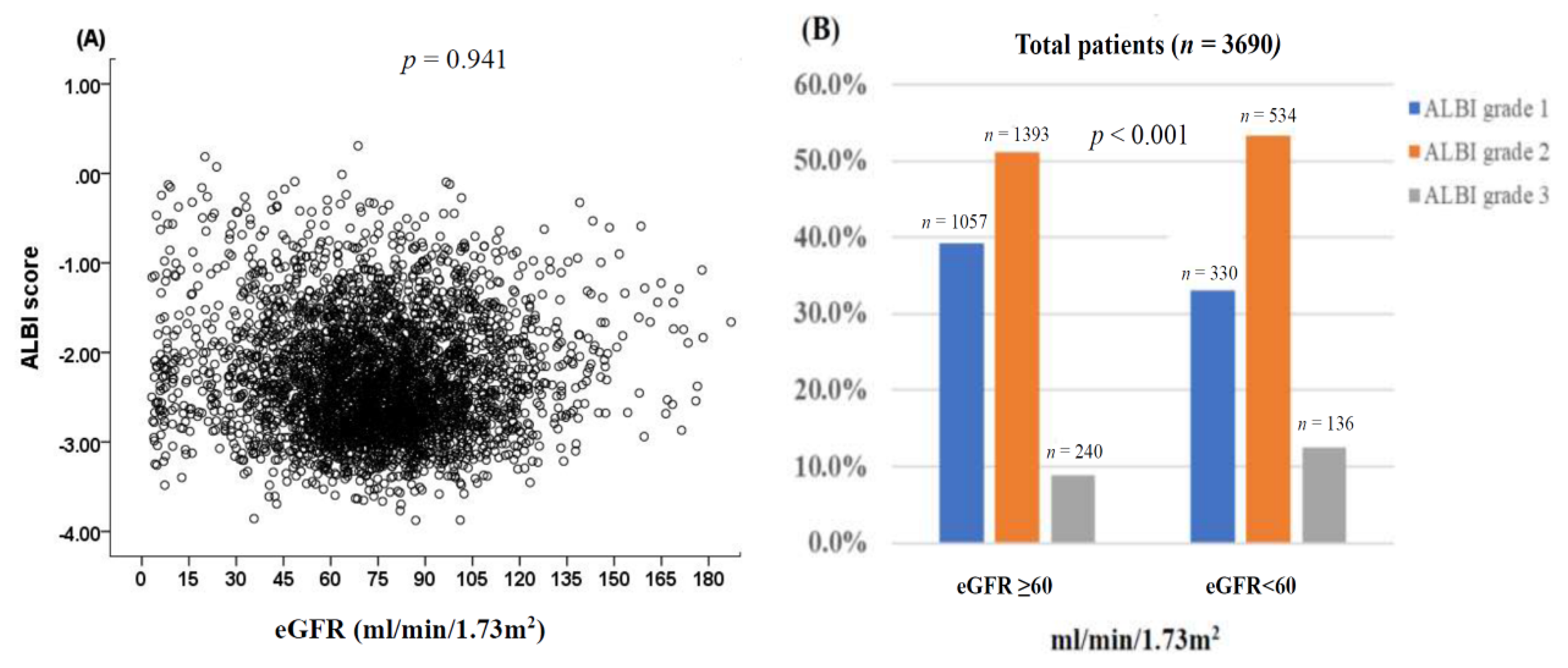
| ALBI grade | <0.001 | ||||
| 1 | 1387 (38) | 330 (33) | 664 (36) | ||
| 2 | 1927 (52) | 534 (53) | 996 (54) | ||
| 3 | 376 (10) | 136 (14) | 184 (10) | ||
| Performance status | <0.001 | ||||
| 0 | 2168 (60) | 514 (51) | 1654 (62) | ||
| 1 | 770 (21) | 167 (17) | 603 (32) | ||
| 2 | 399 (11) | 151 (15) | 248 (9) | ||
| 3–4 | 353 (10) | 168 (17) | 185 (7) | ||
| BCLC, n (%) | <0.001 | ||||
| 0 | 295 (8) | 65 (7) | 230 (9) | ||
| A | 908 (24) | 216 (22) | 692(26) | ||
| B | 610 (17) | 157 (15) | 453 (17) | ||
| C | 1459 (40) | 371 (37) | 1088 (40) | ||
| D | 418 (11) | 191 (19) | 227 (8) | ||
| Treatment | <0.001 | ||||
| Surgical resection | 1069 (29) | 231 (23) | 838 (31) | ||
| Liver transplantation | 18 (1) | 4 (1) | 14 (1) | ||
| Percutaneous ablation | 672(18) | 213 (21) | 459 (17) | ||
| TACE | 1047 (28) | 292 (29) | 755 (28) | ||
| Targeted therapy | 123 (3) | 26 (3) | 97 (4) | ||
| Chemotherapy | 174 (5) | 38 (4) | 136 (5) | ||
| Best supportive care | 587 (16) | 196 (19) | 391 (15) | ||
| Overall Survival | Number | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| HR | CI | p-Value | HR | CI | p-Value | |||
| Age (≤65/>65 years) | 1839/1851 | 1.200 | 1.107–1.300 | <0.001 | 1.160 | 1.064–1.264 | <0.001 | |
| Sex (male/female) | 2815/875 | 1.177 | 1.069–1.296 | 0.001 | 1.207 | 1.095–1.332 | <0.001 | |
| HBsAg (negative/positive) | 1703/1987 | 1.108 | 1.023–1.210 | 0.012 | ||||
| Anti-HCV (negative/positive) | 2579/1111 | 0.964 | 0.884–1.051 | 0.407 | ||||
| Albumin level (≥3.5/<3.5 g/dL) | 2403/1287 | 2.315 | 2.133–2.513 | <0.001 | 1.670 | 1.522–1.832 | <0.001 | |
| Bilirubin level (≤1.5/>1.5 mg/dL) | 2899/791 | 2.048 | 1.867–2.247 | <0.001 | 1.433 | 1.293–1.588 | <0.001 | |
| ALT (≤40/>40 IU/L) | 1555/2135 | 1.235 | 1.138–1.340 | <0.001 | ||||
| Platelet (≥150,000/<150,000 μL) | 1903/1787 | 1.195 | 1.104–1.295 | <0.001 | ||||
| INR of PT (<1.1/≥1.1) | 2422/1267 | 1.653 | 1.521–1.796 | <0.001 | ||||
| eGFR (≥60/<60 mL/min/1.73 m2) | 2690/1000 | 1.414 | 1.296–1.549 | <0.001 | 1.234 | 1.123–1.355 | <0.001 | |
| AFP (<20/≥20 ng/mL) | 1494/2196 | 2.020 | 1.855–2.199 | <0.001 | 1.856 | 1.702–2.025 | <0.001 | |
| Multiple tumors (no/yes) | 2354/1336 | 1.318 | 1.215–1.430 | <0.001 | 1.136 | 1.045–1.234 | 0.003 | |
| Tumor size (≤3/>3 cm) | 1283/2407 | 2.234 | 2.043–2.442 | <0.001 | 1.793 | 1.632–1.970 | <0.001 | |
| Vascular invasion (no/yes) | 2793/897 | 4.296 | 3.925–4.703 | <0.001 | 2.486 | 2.240–2.759 | <0.001 | |
| Distant metastasis (no/yes) | 3335/355 | 3.534 | 3.124–3.998 | <0.001 | 1.494 | 1.309–1.705 | <0.001 | |
| Ascites (no/yes) | 2853/837 | 1.653 | 1.507–1.813 | <0.001 | ||||
| Performance status | ||||||||
| 0 | 2168 | 1 | 1 | |||||
| 1–2 | 1169 | 2.139 | 1.957–2.337 | <0.001 | 1.515 | 1.380–1.663 | <0.001 | |
| 3–4 | 353 | 5.365 | 4.728–6.087 | <0.001 | 2.511 | 2.172–2.904 | <0.001 | |
| ALBI grade | ||||||||
| Grade 1 | 1387 | 1 | 1 | |||||
| Grade 2 | 1927 | 2.074 | 1.894–2.272 | <0.001 | 1.855 | 1.689–2.036 | <0.001 | |
| Grade 3 | 376 | 4.675 | 4.086–5.348 | <0.001 | 2.916 | 2.513–3.383 | <0.001 | |
| Overall Survival | Number | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| HR | CI | p-Value | HR | CI | p-Value | |||
| Age (≤65/>65 years) | 256/744 | 1.120 | 0.945–1.326 | 0.192 | ||||
| Sex (male/female) | 732/268 | 0.933 | 0.789–1.103 | 0.418 | ||||
| HBsAg (negative/positive) | 589/411 | 1.197 | 1.031–1.390 | 0.018 | ||||
| Anti-HCV (negative/positive) | 669/331 | 0.957 | 0.820–1.117 | 0.576 | ||||
| Albumin level (≥3.5/<3.5 g/dL) | 581/419 | 2.286 | 1.970–2.652 | <0.001 | 1.579 | 1.338–1.864 | <0.001 | |
| Bilirubin level (≤1.5/>1.5 mg/dL) | 796/204 | 2.455 | 2.063–2.9222 | <0.001 | 1.536 | 1.266–1.863 | <0.001 | |
| ALT (≤40/>40 IU/L) | 485/515 | 1.297 | 1.121–1.502 | <0.001 | ||||
| Platelet (≥150,000/<150,000 μL) | 503/497 | 1.187 | 1.026–1.373 | 0.021 | ||||
| INR of PT (<1.1/≥1.1) | 663/337 | 1.700 | 1.459–1.980 | <0.001 | ||||
| AFP (<20/≥20 ng/mL) | 443/557 | 1.971 | 1.695–2.292 | <0.001 | 1.727 | 1.481–2.013 | <0.001 | |
| Multiple tumors (no/yes) | 653/347 | 1.410 | 1.214–1.637 | <0.001 | ||||
| Tumor size (≤3/>3 cm) | 319/681 | 2.293 | 1.942–2.707 | <0.001 | 1.850 | 1.551–2.207 | <0.001 | |
| Vascular invasion (no/yes) | 773/227 | 3.622 | 3.053–4.297 | <0.001 | 1.809 | 1.491–2.195 | <0.001 | |
| Distant metastasis (no/yes) | 897/103 | 3.343 | 2.671–4.185 | <0.001 | 1.494 | 1.175–1.900 | 0.001 | |
| Ascites (no/yes) | 739/261 | 1.924 | 1.638–2.261 | <0.001 | 1.228 | 1.036–1.456 | 0.043 | |
| Performance status | ||||||||
| 0 | 514 | 1 | 1 | |||||
| 1–2 | 318 | 2.059 | 1.739–2.437 | <0.001 | 1.413 | 1.180–1.693 | <0.001 | |
| 3–4 | 168 | 4.574 | 3.755–5.571 | <0.001 | 1.985 | 1.553–2.536 | <0.001 | |
| ALBI grade | ||||||||
| Grade 1 | 330 | 1 | 1 | |||||
| Grade 2 | 534 | 2.107 | 1.776–2.499 | <0.001 | 1.695 | 1.418–2.026 | <0.001 | |
| Grade 3 | 136 | 5.662 | 4.468–7.175 | <0.001 | 2.878 | 1.972–3.444 | <0.001 | |
| Overall Survival | Number | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| HR | CI | p-Value | HR | CI | p-Value | |||
| Age (≤65/>65 years) | 114/334 | 1.338 | 1.018–1.757 | 0.037 | 1.385 | 1.041–1.844 | 0.026 | |
| Sex (male/female) | 335/113 | 0.908 | 0.695–1.186 | 0.479 | ||||
| HBsAg (negative/positive) | 262/186 | 1.316 | 1.037–1.671 | 0.024 | ||||
| Anti-HCV (negative/positive) | 295/153 | 0.946 | 0.744–1.203 | 0.650 | ||||
| Albumin level (≥3.5/<3.5 g/dL) | 294/154 | 2.453 | 1.931–3.115 | <0.001 | 1.748 | 1.340–2.281 | <0.001 | |
| Bilirubin level (≤1.5/>1.5 mg/dL) | 380/68 | 2.522 | 1.876–3.391 | <0.001 | 1.950 | 1.389–2.736 | <0.001 | |
| ALT (≤40/>40 IU/L) | 227/221 | 1.311 | 1.040–1.653 | 0.014 | ||||
| Platelet (≥150,000/<150,000 μL) | 207/241 | 0.992 | 0.786–1.250 | 0.943 | ||||
| INR of PT (<1.1/≥1.1) | 311/137 | 1.935 | 1.519–2.466 | <0.001 | ||||
| AFP (<20/≥20 ng/mL) | 239/209 | 1.733 | 1.375–2.184 | <0.001 | 1.697 | 1.333–2.082 | <0.001 | |
| Multiple tumors (no/yes) | 342/106 | 0.965 | 0.739–1.260 | 0.795 | ||||
| Tumor size (≤3/>3 cm) | 191/257 | 1.838 | 1.450–2.331 | <0.001 | 1.553 | 1.208–1.996 | <0.001 | |
| Vascular invasion (no/yes) | 390/58 | 3.948 | 2.896–5.383 | <0.001 | 2.321 | 1.639–3.287 | <0.001 | |
| Distant metastasis (no/yes) | 421/27 | 4.340 | 2.819–6.683 | <0.001 | 2.335 | 1.476–1.695 | <0.001 | |
| Ascites (no/yes) | 395/53 | 0.716 | 0.509–1.008 | 0.056 | ||||
| Performance status | ||||||||
| 0 | 281 | 1 | 1 | |||||
| 1–2 | 122 | 1.832 | 1.405–2.389 | <0.001 | 1.488 | 1.128–1.962 | 0.005 | |
| 3–4 | 45 | 4.808 | 3.380–6.840 | <0.001 | 1.958 | 1.259–3.045 | <0.001 | |
| ALBI grade | ||||||||
| Grade 1 | 185 | 1 | 1 | |||||
| Grade 2 | 220 | 2.036 | 1.577–2.629 | <0.001 | 1.682 | 1.293–2.189 | <0.001 | |
| Grade 3 | 43 | 10.676 | 7.203–15.825 | <0.001 | 7.115 | 4.395–11.520 | <0.001 | |
| Overall Survival | Number | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| HR | CI | p | HR | CI | p | |||
| Age (≤65/>65 years) | 142/410 | 0.956 | 0.770–1.187 | 0.683 | ||||
| Sex (male/female) | 397/155 | 1.282 | 1.033–1.590 | 0.024 | ||||
| HBsAg (negative/positive) | 327/255 | 0.889 | 0.734–1.077 | 0.231 | ||||
| Anti–HCV (negative/positive) | 374/178 | 0.903 | 0.738–1.105 | 0.320 | ||||
| Albumin level (≥3.5/<3.5 g/dL) | 287/265 | 1.931 | 1.596–2.335 | <0.001 | 1.459 | 1.102–1.932 | 0.008 | |
| Bilirubin level (≤1.5/>1.5 mg/dL) | 416/136 | 2.158 | 1.739–2.679 | <0.001 | 1.401 | 1.134–1.730 | 0.002 | |
| ALT (≤40/>40 IU/L) | 258/294 | 1.266 | 1.048–1.529 | 0.014 | ||||
| Platelet (≥150,000/<150,000 μL) | 296/256 | 1.246 | 1.032–1.505 | 0.022 | ||||
| INR of PT (<1.1/≥1.1) | 352/200 | 1.488 | 1.223–1.811 | <0.001 | ||||
| AFP (<20/≥20 ng/mL) | 204/348 | 1.905 | 1.556–2.333 | <0.001 | 1.648 | 1.342–2.025 | <0.001 | |
| Multiple tumors (no/yes) | 311/241 | 1.371 | 1.136–1.655 | <0.001 | ||||
| Tumor size (≤3/>3 cm) | 128/424 | 2.639 | 1.858–3.021 | <0.001 | 1.914 | 1.470–2.491 | <0.001 | |
| Vascular invasion (no/yes) | 383/169 | 2.896 | 2.353–3.563 | <0.001 | 1.662 | 1.317–2.097 | <0.001 | |
| Distant metastasis (no/yes) | 476/76 | 2.621 | 2.013–3.413 | <0.001 | 1.395 | 1.052–1.849 | <0.021 | |
| Ascites (no/yes) | 344/208 | 1.679 | 1.385–2.037 | <0.001 | ||||
| Performance status | ||||||||
| 0 | 233 | |||||||
| 1–2 | 196 | 1.965 | 1.572–2.457 | <0.001 | 1.314 | 1.035–1.699 | 0.025 | |
| 3–4 | 123 | 3.665 | 2.866–4.688 | <0.001 | 1.876 | 1.395–2.521 | <0.001 | |
| ALBI grade | ||||||||
| Grade 1 | 145 | |||||||
| Grade 2 | 314 | 1.933 | 1.532–2.437 | <0.001 | 1.659 | 1.297–2.122 | <0.001 | |
| Grade 3 | 93 | 3.531 | 2.610–4.778 | <0.001 | 2.081 | 1.466–2.952 | <0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, S.-Y.; Hsu, C.-Y.; Liu, P.-H.; Ko, C.-C.; Huang, Y.-H.; Su, C.-W.; Lee, R.-C.; Hou, M.-C.; Huo, T.-I. Survival of Patients with Hepatocellular Carcinoma in Renal Insufficiency: Prognostic Role of Albumin-Bilirubin Grade. Cancers 2020, 12, 1130. https://doi.org/10.3390/cancers12051130
Ho S-Y, Hsu C-Y, Liu P-H, Ko C-C, Huang Y-H, Su C-W, Lee R-C, Hou M-C, Huo T-I. Survival of Patients with Hepatocellular Carcinoma in Renal Insufficiency: Prognostic Role of Albumin-Bilirubin Grade. Cancers. 2020; 12(5):1130. https://doi.org/10.3390/cancers12051130
Chicago/Turabian StyleHo, Shu-Yein, Chia-Yang Hsu, Po-Hong Liu, Chih-Chieh Ko, Yi-Hsiang Huang, Chien-Wei Su, Rheun-Chuan Lee, Ming-Chih Hou, and Teh-Ia Huo. 2020. "Survival of Patients with Hepatocellular Carcinoma in Renal Insufficiency: Prognostic Role of Albumin-Bilirubin Grade" Cancers 12, no. 5: 1130. https://doi.org/10.3390/cancers12051130
APA StyleHo, S.-Y., Hsu, C.-Y., Liu, P.-H., Ko, C.-C., Huang, Y.-H., Su, C.-W., Lee, R.-C., Hou, M.-C., & Huo, T.-I. (2020). Survival of Patients with Hepatocellular Carcinoma in Renal Insufficiency: Prognostic Role of Albumin-Bilirubin Grade. Cancers, 12(5), 1130. https://doi.org/10.3390/cancers12051130