Abstract
Circulating tumor cells (CTCs) detected by CellSearch are prognostic in non-small-cell lung cancer (NSCLC), but rarely found. CTCs can be extracted from the blood together with mononuclear cell populations by diagnostic leukapheresis (DLA), therefore concentrating them. However, CellSearch can only process limited DLA volumes (≈2 mL). Therefore, we established a protocol to enumerate CTCs in DLA products with Isolation by SizE of Tumor cells (ISET), and compared CTC counts between CellSearch® and ISET. DLA was performed in NSCLC patients who started a new therapy. With an adapted protocol, ISET could process 10 mL of DLA. CellSearch detected CTCs in a volume equaling 2 × 108 leukocytes (mean 2 mL). CTC counts per mL were compared. Furthermore, the live cell protocol of ISET was tested in eight patients. ISET successfully processed all DLA products—16 with the fixed cell protocol and 8 with the live cell protocol. In total, 10–20 mL of DLA was processed. ISET detected CTCs in 88% (14/16), compared to 69% (11/16, p < 0.05) with CellSearch. ISET also detected higher number of CTCs (ISET median CTC/mL = 4, interquartile range [IQR] = 2–6, CellSearch median CTC/mL = 0.9, IQR = 0–1.8, p < 0.01). Cells positive for the epithelial cell adhesion molecule (EpCAM+) per mL were detected in similar counts by both methods. Eight patients were processed with the live cell protocol. All had EpCAM+, CD45−, CD235- cells isolated by fluorescence-activated cell sorting (FACS). Overall, ISET processed larger volumes and detected higher CTC counts compared to CellSearch. EpCAM+ CTCs were detected in comparable rates.
1. Introduction
Circulating tumor cells (CTCs) isolated from the peripheral blood of non-small-cell lung cancer (NSCLC) patients are associated with worse prognosis and worse tumor response to therapy [1,2,3,4]. When detected in sufficient numbers, they can be used for molecular analysis. Unfortunately, CTCs are only detected in 30% of NSCLC patients and usually in low numbers, hampering their clinical application [5,6]. It is likely that the majority of metastatic patients have CTCs in circulation, but that the volume of blood screened for CTCs (7.5 mL) is insufficient for a reliable detection [7]. For NSCLC, it was calculated that 10 CTCs could be detected in 78% of patients if 0.75 L of blood is screened [8].
Due to their similar densities, CTCs and mononuclear cells (lymphocytes and monocytes) can be extracted from the blood by diagnostic leukapheresis (DLA). In this way, larger blood volumes can be screened for the presence of CTCs, e.g., 5 L instead of 10 mL, with little burden for the patient [8]. In breast and prostate cancer, significantly higher CTC counts are detected in DLA products compared to peripheral blood by CellSearch [9,10,11]. CellSearch uses the expression of the epithelial cell adhesion molecule (EpCAM) to identify CTCs and is currently the only FDA-approved method. A drawback of CellSearch is that the number of white blood cells that can be processed is limited to 2 × 108 leukocytes. Consequently, the volume of DLA product that can be screened for CTCs is restricted to a few milliliters of DLA product [9,10,11].
We envisaged that a marker-independent CTC detection method could process larger volumes of DLA. Isolation by SizE of Tumor cells (ISET) (Rarecells Diagnostics, Paris, France) uses filtration to identify CTCs by their size. In this manner, ISET can identify both EpCAM+ and EpCAM− CTCs. Some studies have reported a loss of EpCAM+ CTCs but ISET has been shown to identify higher CTC counts in the peripheral blood than CellSearch and the identified CTCs are associated with survival [12,13,14,15]. In other words, ISET could be a useful method to process larger volumes of DLA product, identifying a higher number of CTCs. We thus aim to compare CTC counts of NSCLC patients using ISET with an optimized protocol for DLA products and CellSearch.
2. Results
2.1. NSCLC Patients and Filtration
First, we used 18 filtrations of DLA product to optimize the ISET protocol (Appendix A). Thereafter, with the adapted protocol, the DLA products of 16 patients were successfully processed (Table A1). The mean DLA procedure time was 95 minutes (standard deviation [sd] = 20 min). During this time, an average 86% of the patients’ blood volume was processed, resulting in 80 mL of DLA product (including 12 mL of acid citrate dextrose solution A [ACDA] for anticoagulation). The vast majority of cells in the DLA product were concentrated in leukocytes and platelets (Table S1). Using lymphocytes as a reference, the mean efficacy of the procedure reached 65% (IQR = 59–71). Blood cell values decreased during apheresis, partly due to the removal of the cells and in part due to dilution (Table S2). DLA procedures were well tolerated and without adverse events, except for minor paresthesia in two patients (classified as grade I, not requiring any intervention, or II, requiring medication), either resolved by administering oral calcium or decreasing the speed of the procedure. Paresthesia is a known side effect of ACDA. All patients signed informed consent before being included in the study.
2.2. Spiking Efficacy and Immunostaining Control
Two samples were spiked with 100 H292 cells. These were subsequently filtered according to the adjusted protocol. The filters were stained with EpCAM and CD45 in two spots. We identified 65% and 80% of expected H292 cells, respectively. Two other spots were stained with TTF1 and CD45, and (as expected) no cells were identified.
2.3. CTC Identification by ISET
All 16 DLA products processed with the adapted protocol were filtered successfully. CTC counts were identified in in 88% (14/16, Figure 1A) of the patients with ISET. EpCAM+ CTCs were detected in 75% (12/16) and TTF1+ CTCs were also detected in 75% (12/16, Figure 1B). The total median CTC count detected by ISET was 3.8 CTC/mL DLA product (IQR = 1.3–4.0, Figure 2A). The median EpCAM+ CTC count was 1.0 per mL DLA (IQR = 0.3–2.8), while the median TTF1+ CTC count was 2.5 per mL DLA (IQR = 1.3–3.0). The highest count on one spot was a cluster of 18 CTCs. In two patients, we observed only EpCAM+ CTCs (Figure 3A) and only TTF1+ CTCs in two other patients (Figure 3B). Immunohistochemical (IHC) staining for both TTF-1 and EpCAM showed TTF1+ CTCs that were negative for EpCAM and vice versa (Figure 3C).
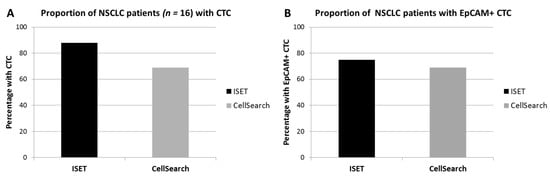
Figure 1.
Percentage of diagnostic apheresis products with circulating tumor cells (CTCs) detected by Isolation by SizE of Tumor cells (ISET) or CellSearch. The proportion of patients with CTCs (defined as either expressing TTF1/p40 or EpCAM, while lacking CD45) (A), and the proportion of patients with CTCs expressing the epithelial cell adhesion molecule (EpCAM) (B) have been shown.
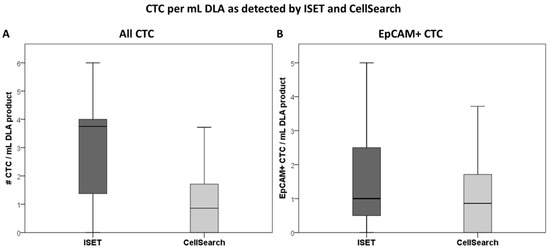
Figure 2.
Boxplot depicting the median number of CTC/mL diagnostic apheresis product as identified by ISET (CTCs defined as either expressing TTF1/p40 or EpCAM, while lacking CD45) and CellSearch. All CTCs (A) and only those expressing EpCAM (B) are considered.
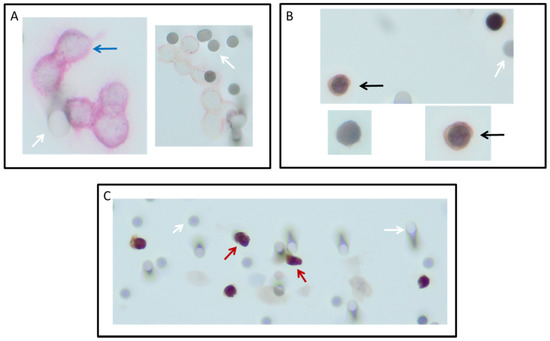
Figure 3.
Circulating tumor cells (CTCs) detected on ISET filters after filtration of diagnostic leukapheresis product of non-small-cell lung cancer (NSCLC) patients. CTCs were detected with immunocytochemistry in three different manners: Cells positive for the epithelial cell adhesion molecule (stained red) with CD45 (stained brown) as a negative marker (A); TTF1 or p40 (stained brown) as a positive marker, with CD45 as a negative marker (stained red); (B) and a combination of TTF1 with EpCAM (C). Images were taken with a focus of 200×. White arrow: 8 µm pores of the filter. Red arrow: two cells suspected to be EpCAM and TTF1 positive; black arrow: TTF1-positive, EpCAM-negative cell, blue arrow: EpCAM-positive cell.
2.4. Comparison to CellSearch
ISET processed significantly more cells and volume of DLA product compared to CellSearch, but in lower concentrations (Table 1). CTCs were detected in 69% (11/16) by CellSearch and in 88% (14/16) by ISET (p < 0.05 by matched comparison, Figure 1A). In one patient, no CTCs were detected by any method. CellSearch detected a median CTC count of 0.9 per mL (IQR = 0–1.8), while ISET detected a median count of 3.8 (IQR = 1.3–4.0, p < 0.01, Figure 1B).

Table 1.
Sample and dilution volumes with cell counts processed by CellSearch and ISET for CTC enumeration.
The EpCAM+ CTC detection rate of ISET (75%) and CellSearch (69%) was similar (p = 0.5, Figure 1B). Counts of EpCAM+ CTC/mL DLA product also did not differ between ISET (median 1.0, IQR = 0.3–2.8) and CellSearch (median = 0.9, IQR = 0–1.8) (p = 0.2, Figure 2B). Absolute detected counts by ISET remained significantly higher compared to CellSearch (median = 5.0, IQR = 1.3–13.8, median = 1, IQR = 0.2–2.8, respectively, p < 0.01).
2.5. Live Cell Protocol
In eight patients, the live cell protocol was used. FACS identified populations of EpCAM+ cells, which did not express an erythrocyte (CD235A) or leukocyte marker (CD45). From the eight patients, we isolated 474, 188, 126, 47, 32, 30, 5 and 2 EpCAM+ CD45−CD235A− cells from 5–10 mL of DLA product by FACS, respectively. However, these cells had too low reads in single-cell whole-genome sequencing (scWGS) to come to reliable conclusions.
3. Discussion
The ISET filtration system was capable of processing a volume of 10 mL of DLA product for fixated cells. With the live cell protocol, the DLA product volume processed was between 10 and 20 mL, using half of the ISET filter. The FDA-cleared CellSearch system is widely used for CTC detection and is the current gold standard, but the volume of DLA product that can be processed is restricted. CellSearch uses positive immunomagnetic selection to extract cells expressing EpCAM from the processed sample. Leukocytes are also extracted by non-specific interactions with the EpCAM immunomagnetic particles. Therefore, CellSearch can only process samples with a limited number of white blood cells, estimated to be 2 × 108 leukocytes [9,10,11]. While this poses no issue for peripheral blood samples, this limitation restricts the volume of DLA product (1–4 mL) that can be processed, since DLA products contain a high concentration of leukocytes. After using additional anticoagulant in the fixed cell protocol, ISET was capable of processing up to 10 mL of DLA product, which contained between 3- and 8-fold as many leukocytes as could be handled by CellSearch. The number of CTCs detected by ISET had a larger standard deviation, due to the larger volumes screened and higher counts identified.
With immunohistochemistry, we identified both EpCAM− and EpCAM+ CTCs, in agreement with previous findings when investigating CTCs in the peripheral blood [12,16,17]. EpCAM+ CTCs were still identified in the DLA product, despite a previous report that some of these cells might be lost by ISET when examined in prostate cancer patients [15]. Possibly the size of CTCs derived from prostate cancer is smaller than CTCs derived from NSCLC, causing them to be able to pass through the ISET filter. However, whether this is responsible for this difference has to be further investigated. Besides EpCAM, cytokeratin is a commonly used marker. We did not utilize this marker for several reasons. It has been reported that cytokeratin expression is sometimes downregulated in CTCs [18,19]; cytokeratin is used for cytoplasmic staining and EpCAM is used for membrane staining. Thyroid transcription factor-1 (TTF-1) is a well-known and routinely used marker by pathologists for the identification of adenocarcinoma of the lung and thyroid cancers [20]. TTF1 is a nuclear marker that stains very strongly, making it relatively easy to detect. In our patients, it was known that their primary tumors were positive for TTF1. Moreover, it is known that TTF1 is not expressed in blood cells, making it a very useful marker for the identification of CTCs in the blood [20,21].
The larger volume that was screened for CTCs with ISET resulted in a significantly increased CTC detection rate. CellSearch was very sensitive in detecting the presence of EpCAM+ CTCs, even in small volumes. EpCAM+ CTCs were detected in similar proportions of patients and in similar concentrations by CellSearch and ISET. As EpCAM+ CTCs are possibly more strongly associated with clinical outcome, both CellSearch and ISET function well for CTCs that have been proven to be both predictive and prognostic [5]. However, due to the larger volume processed by ISET, this procedure can isolate a larger number of CTCs for further functional or genomic analysis.
Cells obtained with the live cell protocol were analyzed by FACS, which was capable of identifying populations of EpCAM-positive cells. Unfortunately, the DNA quality of isolated cells turned out to be quite low or had too few reads to draw conclusions. A possible explanation is that the CTCs were unable to withstand the shearing stress of the sorter, resulting in their destruction [22]. However, it has been shown before that FISH can be used on ISET filters to identify rearrangements, proving the malignant origin of cells identified in this manner [23].
It is also known that FACS is capable of identifying cell populations, but lacks sensitivity to capture rare cells efficiently [24,25,26]. This makes it a less than ideal method to capture CTCs—both in the blood and in the DLA product—even after concentrating CTCs by ISET. Alternatives to identifying CTCs with a high specificity would be by combining morphology, genomic and/or functional analyses. This would be an important development for clinical application of CTCs [27,28,29].
Due to the association of CTCs with shorter survival and their use to monitor disease status longitudinally, the detection of CTCs has been a topic of interest for years [2,12,16,30,31,32,33,34,35,36,37]. Just their presence at baseline is associated with lower tumor responses to immunotherapy, chemotherapy and targeted therapy [1]. However, if CTCs cannot be reliably detected, their clinic application remains limited.
CTC detection has been increased by DLA in prostate and breast cancer patients before, but only small volumes of DLA product were processed [9,10,11,38]. DLA is a well-tolerable procedure, even in our NSCLC population, and has few complications, while placing minimal burden (only two hours of time) on patients [39,40,41,42]. Also the calculated efficacy of our procedures in isolating mononuclear cells (MNCs) was shown to be comparable with that of isolating stem cells, and DLAs in breast cancer patients [8,9,10,11,43]. In the evolving area of immunotherapy, this method can also be used to study different T-cell populations. Here, we show that a larger volume of DLA product can be processed with ISET, allowing for more reliable CTC detection. At this time, apheresis is not used diagnostically but only therapeutically for hematological patients. Yet based on our results, apheresis could be used as a diagnostic tool in patients whose biopsies failed or where the tumor is inaccessible. With DLA, sufficient CTCs could be isolated to allow for diagnostic tests and tumor typing to be performed. As shown in our study and others, complications associated with DLA are mild and rare, making it an easily tolerable procedure even for NSCLC patients [39,40,41,42]
The number of included patients in our study was relatively small and heterogeneous in stage and treatment line. However, previous studies have shown that the number of CTCs is not influenced by these patient characteristics, and any influence of patient characteristics is accounted for since the comparisons were performed for each patient in a matched manner. Therefore, the power was increased sufficiently to observe significant outcomes. Furthermore, the automated identification of CTCs, e.g. as by the ACCEPT program which is being developed for CellSearch, would greatly improve the objective identification of CTCs [44,45,46]. The DLA, while very tolerable, remains a costly procedure that takes 2 hours per patient. ISET is very labor intensive. Using DLA and ISET to obtain CTCs for all NSCLC patients would be untenable. Still it could be used in patients with inaccessible tumors or in whom even repeated biopsies could not provide sufficient material for diagnostics.
4. Materials and Methods
4.1. Patient Inclusion and Clinical Data
Patients with proven NSCLC were prospectively included in an exploratory cohort. Eligibility criteria were an Eastern Cooperative Oncology Group performance status (PS) of 0–2, no use of anticoagulation and no clotting disorders. All patients started (a new line of) treatment at time of inclusion. Informed consent was obtained from all patients.
The study was approved by the Medical Ethical Committee (2015/602) and was registered in the Dutch trial register (NL55754.042.15/NL5423).
4.2. Diagnostic Leukapheresis Procedure
DLAs were carried out with the Spectra Optia® Apheresis System 11 (Terumo BCT Inc., Lakewood, CO, USA), as previously described [10]. We aimed to process the total body blood volume (TBV), as calculated by the formula of Nadler [47]. Before and after this procedure, an EDTA tube was taken for a full blood count. Procedure efficacy was calculated by dividing the number of lymphocytes in the total DLA product by the total number of lymphocytes that passed through the machine while the DLA product was collected.
4.3. The Adapted ISET Protocol for Fixated Cells
First, we processed different volumes of DLA product according to the protocol for fixed cells in blood (Appendix A). The protocol was adapted, as too many DLA products could not be filtered efficiently. Filtration failure was correlated with the volume of processed DLA product (ρ = 0.69, p < 0.01) and platelet count in the DLA product (ρ = 0.75, p < 0.01). Consequently, we used additional anticoagulation in the adapted protocol. DLA product was diluted 1:1 with ACDA and placed in blood collection tubes coated with EDTA (Becton Dickinson, Etten Leur, The Netherlands). No further filtration problems were encountered and we filtered 10 mL of DLA product, diluted with 10 mL ACDA in EDTA tubes, according to the standard ISET protocol [48]. In short, 20 mL of the DLA and ACDA mixture was further diluted with 90 mL of fixed ISET buffer and mixed for 10 min. Afterwards, the sample was transferred to the (prehydrated) ISET block and filtered with the pressure set between −10 and −25 kPA. After filtering the sample, CTCs were detected with immunocytochemistry (ICC) staining. As a positive marker, either the membrane staining of EpCAM (Ventana ReadyToUse 760–4383, Roche Diagnostics, Almere, The Netherlands) or a nuclear marker was used (either TTF1 [Ventana ReadyToUse 790–475, Roche Diagnostics, Almere, The Netherlands] recognizing the majority of adenocarcinomas or p40 [Venta ReadyToUse 790–4950, Roche Diagnostics, Almere, The Netherlands] detecting the majority of squamous cell carcinomas, depending on which one was positive in the primary tumor biopsy). As a negative marker, combined with either of the two positive markers, we used the membrane staining of CD45 (DAKO M0701, Stevens Creek, CA, USA). Between 3 and 6 spots of each ISET filter were evaluated for CTCs, following the procedure by Krebs et al. [12]. A certified pathologist (W.T. and M.T.) identified CTCs on the basis of immunocytochemistry. Two DLA products were spiked before filtration with 100 H292 cells. Afterwards, the capture efficacy was calculated.
4.4. CTCs Recognized by CellSearch
CellSearch identified CTCs in a DLA aliquot of 2 × 108 leukocytes, diluted with CellSearch Circulating Tumor Cell Kit Dilution Buffer (Menarini Silicon Biosystems, Huntingdon Valley, PA, USA) to 7.5 mL and placed in a Cellsave tube (Menarini). After the tube was stored at least overnight at room temperature, the sample was centrifuged at 800 g for 10 min before analysis. Sample processing occurred within 72 h using CellSearch according to the manufacturer’s instructions (Menarini Silicon Biosystems, Huntington Valley, PA, USA) [11]. CellSearch cartridges were scanned using the CellTracks Analyzer II (Menarini) and analyzed by a trained operator. Cells were classified as CTCs when they were EpCAM+ cytokeratin+ and CD45−, with a morphology consistent with a nucleated cell.
4.5. Live Cell Protocol
In addition to fixed cells, we wanted to explore the protocol for live cell isolation by ISET, as these live cells can be cultured and later analyzed by different molecular methods. Live cells were isolated from 10–20 mL of DLA product, diluted 1:1 with ACDA and placed in EDTA tubes after ISET live buffer was added (4:1). Subsequently, the standard live cell protocol of ISET was followed [48]. In short, 10–20 mL of DLA with ISET buffer was filtered with the pressure set to between −4 and −10 kPa. During this process, the filter was washed and always remained submerged in DPBS until the liquid was clear. A 1 mL pipette was used to wash cells of the filter and aspirate 1 mL fluid, which was placed in a 15 mL tube. This was repeated 5 times. Afterwards, the tube was centrifuged at 120 g for 10 min. Live cells were stored for further experiments such as single-cell whole-genome sequencing (scWGS). Filtered cells were fixated with formaldehyde 1% (end concentration 0.1%). Fluorescence-activated cell sorting ([FACS] BD FACSJazz, BD biosciences, Allschwil, Switzerland) was used to sort the cells and identify cell populations. For DLA products processed with the live cell protocol, CTCs were defined as cells containing a nucleus and expressing EpCAM, while lacking CD45 (leukocyte marker) and CD235A (erythrocyte marker). These single cells were isolated and placed into a 96-well plate and used for scWGS.
4.6. Single-Cell Whole-Genome Sequencing
Single isolated CTCs were stored in freeze buffer after isolation. We performed scWGS as described previously with some minor modifications [49]. In short, upon MNase treatment, de-crosslinking was performed by incubation at 65 °C for 1 h in the presence of Proteinase K (0.025U) and NaCl (200 mM), followed by AMPure XP bead purification and subsequent end repair and A-tailing. During PCR, indexes were introduced to each DNA fragment allowing multiplexing of the libraries for sequencing. All libraries were sequenced with the Illumina NextSeq 500. Data analysis was performed using the AneuFinder package [49,50].
4.7. Statistical Analysis
From the DLA product, the number of CTCs identified with ISET was compared with those from CellSearch. Comparisons were performed using non-parametric matched analyses. Differences in the proportion of patients with CTCs were evaluated with McNemars test. CTC counts per mL DLA product were compared with Wilcoxon’s matched analysis.
We estimated that CellSearch would detect CTCs in 50% of patients, while the filtration methods would detect CTCs in 90% of patients. Assuming a good association between both measurement types (ρ = 0.66) with β = 0.2 and α = 0.05, 15 matched comparisons were required.
5. Conclusions
ISET was capable of processing 10 mL volumes of DLA product with an adjusted fixated cell protocol. CTCs were detected in the majority of patients (88%). The adjusted live cell protocol could be used to process up to 20 mL of DLA product on half an ISET block, allowing the capture of a sufficient number of CTCs for tumor typing not only by IHC but also for single-cell genomics.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6694/12/4/896/s1, Table S1: Blood cell counts in peripheral blood and DLA product; Table S2: Mean cell counts (pre and post apheresis) in blood and in diagnostic leukapheresis product.
Author Contributions
Conceptualization, M.T., K.C.A., T.J.N.H., W.T. and H.J.M.G.; methodology, M.T., T.J.N.H., M.J. and W.T.; formal analysis, M.T., K.C.A., H.v.d.B. and W.T.; resources, H.J.M.G., M.J. and L.W.M.M.T.; data curation, M.T., K.C.A. and H.v.d.B.; writing—original draft preparation, M.T.; writing—review and editing, K.C.A., T.J.N.H., E.S., H.v.d.B., M.J., D.C.J.S., P.M.L., W.T., L.W.M.M.T. and H.J.M.G.; supervision, T.J.N.H., W.T., D.C.J.S., P.M.L., L.W.M.M.T. and H.J.M.G.; funding acquisition, L.W.M.M.T. and H.J.M.G. All authors have read and agreed to the published version of the manuscript.
Funding
The authors are part of the CANCER-ID consortium, which has received support from the Innovative Medicines Initiative (IMI) Joint Undertaking under grant agreement No 115749. Rarecells Diagnostics provided the ISET system for CTC enumeration. The UMCG Cancer research fund provided further financial support. Funding sources had no influence on the gathering of data, interpretation of results or publication.
Acknowledgments
During the study, R. Smith, J. Wheeler and J. Ladtkow (Terumo BCT, Lakewood, CO, USA) provided advice and key insights into the apheresis procedure and technology. Procedures were run with the assistance of the personnel from Sanquin (Sanquin, Sanquin Bloedvoorziening, Groningen, The Netherlands). We are very grateful for all of their expertise and efforts.
Conflicts of Interest
Author M. Jayat is an employee of Rarecells Diagnostics and has provided advice regarding the filtration and staining of samples but was not involved in CTC enumeration, statistical analysis or writing the original manuscript. The authors have no other disclosures.
Appendix A
Appendix A.1. The Standard ISET Protocol for Fixed Cells
The ISET instruction manual for processing CTCs obtained from venous blood was followed. ISET filters the samples through a disposable block, which consists of six compartments. One compartment leads to five filtration spots (locations where cells pass through the filter) and can contain a volume of up to 50 mL (intended 5 mL sample and 45 mL ISET buffer). The other five compartments each lead to one spot and can contain a volume of up to 10 mL (1 mL sample and 9 mL ISET buffer) (Appendix Figure A1).
We used the five small compartments to filter different volumes of DLA product (0.1, 0.25, 0.5, 0.75 and 1 mL), diluted to 1 mL with Dulbecco’s Phosphate-Buffered Saline (DPBS, ThermoFisher, Waltham, MA, USA) (Appendix Figure A1). The filter procedure was carried out according to the protocol provided by Rarecells diagnostics and was previously described [17]. In short, after prehydration of all compartments, a 10 mL (sample with ISET buffer) sample was deposited into each small compartment. The pump was set at −10 kPA and the valve was opened, allowing for filtration of the sample. If the sample did not filter, the pressure was adjusted up to a maximum of −25 kPA. The largest volume of DLA product which filtered successfully within 5 minutes at −20 kPa was used further on for the large compartment (volume ×5). The same procedure would be followed then.

Figure A1.
Top view of an (schematic) ISET filter (A), with the dilutions of the different tested protocols. First, the standard protocol was followed as closely as possible with different dilutions (B). By using additional anticoagulant, the adjusted protocol (C) was able to process up to 10 mL of DLA product without fail. With additional anticoagulant, the live cell protocol was capable of filtering up to 20 mL of DLA product with just half a filter (D). The other half (the large compartment) was used to filter an additional 5 mL of DLA product with the adjusted protocol. No significant differences between DLA products processed with the different protocols were observed (Appendix Table A1 and Table A2).
Table A1.
Characteristics of filtered diagnostic leukapheresis samples by ISET®, according to original protocol (cohort 1), adjusted protocol (cohort 2) and the live cell protocol by half the filter.
Table A1.
Characteristics of filtered diagnostic leukapheresis samples by ISET®, according to original protocol (cohort 1), adjusted protocol (cohort 2) and the live cell protocol by half the filter.
| Processed | Blood Cells | ISET Cohort 1 (n = 18) * | ISET Cohort 2 (n = 16) ** | ISET Live Cell (n = 8) *** |
|---|---|---|---|---|
| Sample volume (mL) | DLA product | 0.5–5 | 5 | 10–20 |
| Absolute blood cell counts processed (×108) | Leukocytes | 4.6 (3.7–7.3) | 5 (3.6–8.0) | 18.6 (9.6–33.9) |
| Lymphocytes | 1.9 (1.5–2.7) | 2.2 (1.9–3.5) | 7.7 (4.8–12.0) | |
| Monocytes | 0.8 (0.6–1.2) | 1.1 (0.7–1.8)) | 2.4 (1.6–4.7) | |
| Granulocytes | 1.9 (0.9–3.5) | 2.6 (1.1–3.8) | 8 (3.3–17.5) | |
| Platelets | 78.7 (69.5–94.8) | 76.3 (45.7–63.9) | 319.4 (199.1–500.8) | |
| Erythrocytes | 19.8 (15.7–32.1) | 32.5 (22.8–45.9) | 76.5 (50.5–219.0) | |
| Dilution and total processed sample (mL) | Dilution material | DPBS and fixed ISET buffer | ACDA and fixed ISET buffer | ACDA and live ISET buffer |
| Dilution volume | 0–4.5 and 45 | 5 and 45 | 10–20 and 80–160 | |
| Total sample | 50 | 55 | 100–200 | |
| Concentrations per mL sample (×106/mL) | Leukocytes | 9.2 (7.4–14.6) | 9.0 (6.4–14.5) | 9.3 (7.6–26.2) |
| Lymphocytes | 3.8 (2.9–5.5) | 4.0 (3.4–6.2) | 4.1 (3.9–7.8) | |
| Monocytes | 1.6 (1.3–2.4) | 1.9 (1.2–3.4) | 1.4 (1.2–3.5) | |
| Granulocytes | 3.8 (1.9–7.0) | 4.8 (1.9–6.9) | 4.0 (2.5–15.0) | |
| Platelets | 157.3 (139.1–189.6) | 138.7 (83.1–157.0) | 268.9 (142.7–314.5) | |
| Erythrocytes | 0.04 (0.03–0.06) | 0.1 (0.1–0.1) | 0.1 (0.1–0.1) | |
| Limiting factor | Platelets | None | None |
* Description of material filtrated by the large compartment of the ISET® filtration block is shown. ** Total filtered volume has been divided by two, for comparison with the other two protocols. *** Description of the material filtrated by the small compartment of the ISET® filtration block is shown.
Table A2.
Characteristics of non-small-cell lung cancer patients undergoing apheresis and ISET® filtering.
Table A2.
Characteristics of non-small-cell lung cancer patients undergoing apheresis and ISET® filtering.
| Characteristic | Specified | Original Protocol (n = 18) | Adjusted Protocol * (n = 16) | Live Cell Protocol * (n = 8) |
|---|---|---|---|---|
| Age | Mean (sd) | 64 (7) | 68 (11) | 67 (7) |
| Gender | Male | 12 (67) | 10 (62) | 4 (80) |
| Female | 6 (33) | 6 (38) | 1 (20) | |
| ECOG PS | 0 | 8 (44) | 9 (56) | 5 (63) |
| 1 | 7 (39) | 4 (25) | 2 (24) | |
| 2 | 3 (17) | 2 (13) | 0 (0) | |
| 3 | 0 (0) | 1 (6) | 1 (13) | |
| Smoking status | Smokers | 14 (78) | 7 (44) | 3 (38) |
| Previous | 1 (6) | 5 (31) | 3 (38) | |
| Non-smokers | 3 (17) | 4 (25) | 2 (24) | |
| Stage | I | 1 (6) | 2 (13) | 0 (0) |
| II | 1 (6) | 1 (6) | 0 (0) | |
| III | 0 (0) | 3 (19) | 0 (0) | |
| IV | 16 (89) | 10 (62) | 8 (100) | |
| Histology | Adenocarcinoma | 14 (78) | 9 (56) | 6 (75) |
| Squamous cell | 4 (22) | 4 (25) | 2 (25) | |
| other | 0 (0) | 3 (19) | 0 (0) | |
| Mutations | None identified | 7 (39) | 6 (38) | 4 (50) |
| KRAS | 7 (39) | 5 (31) | 2 (25) | |
| ALK | 3 (16) | 0 (0) | 0 (0) | |
| Other | 1 (6) | 5 (31) | 2 (25) | |
| Therapy line | 0 | 2 (11) | 5 (31) | 3 (37) |
| 1 | 6 (33) | 7 (44) | 2 (25) | |
| 2 | 7 (39) | 4 (25) | 3 (37) | |
| ≥3 | 3 (17) | 0 (0) | 0 (0) | |
| Treatment | Surgery | 2 (11) | 3 (19) | 0 (0) |
| Chemo(radio)therapy | 1 (6) | 2 (13) | 0 (0) | |
| Immunotherapy | 11 (61) | 9 (56) | 7 (87) | |
| Targeted therapy | 4 (22) | 2 (12) | 1 (13) | |
| Blood | Total blood volume (L) | 5.2 (0.8) | 5,1 (0.9) | 5.3 (0.8) |
| Processed volume (L) | 4.8 (1.1) | 4.2 (1.0) | 5.0 (0.6) | |
| Percentage processed (sd) | 89 (21) | 84 (16) | 96 (5) | |
| DLA product | mL (sd) | 83 (21) | 75 (17) | 85 (7) |
| ACDA (sd) | 12 (3) | 12 (4) | 11 (1) |
* Patients undergoing the live cell protocol are also included in the adjusted protocol population (half the ISET block was used for the adjusted protocol, and half for the live cell protocol).
Appendix A.2. CTC Detection Standard Protocol
The filters were stained with a Giemsa staining (hemacolor, Merck, Darmstadt, Germany) according to the manufacturer’s instructions [38].
Appendix A.3. Adjustment of the ISET Protocol for Fixed Cells
The protocol was adjusted after filtering 18 DLA samples when twelve samples failed; they could not be evaluated (six due to coagulation and clogging of the filter, as shown in Appendix Figure A2, six due too much cellular material on the filter for evaluation). In four out of six DLA products that were successfully filtered, we identified CTCs (66%, Appendix Figure A2). Failure to filter and filtration time were associated with the volume of processed DLA product (ρ = 0.69, p < 0.01) and platelet count in the DLA product (ρ = 0.75, p < 0.01). Thus, additional anticoagulation was used, and the DLA product was diluted in a 1:1 ratio with ACDA and placed in blood collection tubes coated with EDTA (Becton Dickinson, Etten Leur, The Netherlands). Two DLA products were filtered with different volumes as before in the five small compartments (0.1, 0.25, 0.5, 0.75 and 1 mL pure DLA product per respective spot). No filtration problems were encountered anymore, and both samples filtered the largest volume of DLA (1 mL per spot, and 5 mL for the large compartment). From then on, we filtered 10 mL of DLA product, diluted with 10 mL ACDA and placed in EDTA tubes according to the standard ISET protocol [17].

Figure A2.
Aggregates (A) and identified circulating tumor cells (B) observed on ISET filters after the filtration of diagnostic leukapheresis product obtained from non-small-cell lung cancer patients. Staining was performed with Giemsa, and CTCs were identified by their large size, relatively large nucleus and other morphological characteristics by a certified pathologist.
Appendix A.4. Adjustment for CTC Detection
While Giemsa staining was originally used for CTC detection on ISET filters, the three-dimensional plane of the cells on the ISET filters hampered identification by our pathologist (WT). In order to provide more evidence that cells were CTCs, we used additional immunohistochemical (IHC) staining. Three different combinations of antibodies were used. EpCAM (Ventana ReadyToUse 760–4383, Roche Diagnostics, Almere, The Netherlands) or a nuclear marker was used as a positive marker (either TTF1 [Ventana ReadyToUse 790–475, Roche Diagnostics, Almere, The Netherlands], recognizing the majority of pulmonary adenocarcinomas or p40 [Ventana ReadyToUse 790–4950, Roche Diagnostics, Almere, The Netherlands], recognizing squamous cell carcinomas, depending on which one was positive in the primary tumor biopsy). This staining was combined with EpCAM (Ventana ReadyToUse 760–4383, Roche Diagnostics, Almere, The Netherlands) and CD45 (DAKO M0701, Stevens Creek, CA, USA), with the latter as a negative marker for CTCs. In total, 3–6 spots in each filter were evaluated for CTCs, following the procedure by Krebs et al. [12]. Several slides were also stained for cytokeratin (Ventana ReadyToUse 760–2595, Roche Diagnostics, Almere, The Netherlands) when enough spots were available. However, it proved to be more reliably to use TTF1 than cytokeratin and EpCAM staining. Therefore, we dropped cytokeratin for the majority of filters and favored TTF1. In these filters, clusters of cells still did occur, but were no longer obstructing assessment for CTCs.
References
- Tamminga, M.; De Wit, S.; Hiltermann, T.J.; Timens, W.; Schuuring, E.; Terstappen, L.W.; Groen, H.J. Circulating tumor cells in advanced non-small cell lung cancer patients are associated with worse tumor response to checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 173. [Google Scholar] [CrossRef]
- Punnoose, E.A.; Atwal, S.; Liu, W.; Raja, R.; Fine, B.M.; Hughes, B.G.M.; Hicks, R.J.; Hampton, G.M.; Amler, L.C.; Pirzkall, A.; et al. Evaluation of circulating tumor cells and circulating tumor DNA in non-small cell lung cancer: Association with clinical endpoints in a phase II clinical trial of pertuzumab and erlotinib. Clin. Cancer Res. 2012, 18, 2391–2401. [Google Scholar] [CrossRef] [PubMed]
- Muinelo-Romay, L.; Vieito, M.; Abalo, A.; Nocelo, M.A.; Barón, F.; Anido, U.; Brozos, E.; Vázquez, F.; Aguín, S.; Abal, M.; et al. Evaluation of circulating tumor cells and related events as prognostic factors and surrogate biomarkers in advanced NSCLC patients receiving first-line systemic treatment. Cancers 2014, 6, 153–165. [Google Scholar] [CrossRef]
- Nieva, J.; Wendel, M.; Luttgen, M. High-definition imaging of circulating tumor cells and associated cellular events in non-small cell lung cancer patients: A longitudinal analysis. Phys. Biol. 2012, 9, 016004. [Google Scholar] [CrossRef][Green Version]
- de Wit, S.; Rossi, E.; Weber, S.; Tamminga, M.; Manicone, M.; Swennenhuis, J.F.; Groothuis-Oudshoorn, C.G.; Vidotto, R.; Facchinetti, A.; Zeune, L.L.; et al. Single tube liquid biopsy for advanced non-small cell lung cancer Single tube liquid biopsy for advanced non-small cell lung cancer. Int. J. Cancer 2019, 144, 3127–3137. [Google Scholar] [CrossRef] [PubMed]
- De Wit, S.; Van Dalum, G.; Lenferink, A.T.; Tibbe, A.G.; Hiltermann, T.J.; Groen, H.J.; Van Rijn, C.J.; Terstappen, L.W. The detection of EpCAM+ and EpCAM− circulating tumor cells. Sci. Rep. 2015, 5, 12270–12279. [Google Scholar] [CrossRef]
- Coumans, F.A.; Ligthart, S.T.; Uhr, J.W.; Terstappen, L.W. Challenges in the enumeration and phenotyping of CTC. Clin. Cancer Res. 2012, 18, 5711–5718. [Google Scholar] [CrossRef] [PubMed]
- Stoecklein, N.H.; Fischer, J.C.; Niederacher, D.; Terstappen, L.W.M.M. Challenges for CTC-based liquid biopsies: Low CTC frequency and diagnostic leukapheresis as a potential solution. Expert Rev. Mol. Diagn. 2015, 16, 147–164. [Google Scholar] [CrossRef]
- Fischer, J.C.; Niederacher, D.; Topp, S.A.; Honisch, E.; Schumacher, S.; Schmitz, N.; Zacarias Föhrding, L.; Vay, C.; Hoffmann, I.; Kasprowicz, N.S.; et al. Diagnostic leukapheresis enables reliable detection of circulating tumor cells of nonmetastatic cancer patients. Proc. Natl. Acad. Sci. USA 2013, 110, 16580–16585. [Google Scholar] [CrossRef]
- Fehm, T.N.; Meier-Stiegen, F.; Driemel, C.; Jäger, B.; Reinhardt, F.; Naskou, J.; Franken, A.; Neubauer, H.; Neves, R.P.L.; Dalum, G.; et al. Diagnostic leukapheresis for CTC analysis in breast cancer patients: CTC frequency, clinical experiences and recommendations for standardized reporting. Cytom. Part A 2018, 93, 1213–1219. [Google Scholar] [CrossRef]
- Andree, K.C.; Mentink, A.; Zeune, L.L.; Terstappen, L.W.M.M.; Stoecklein, N.H.; Neves, R.P.; Driemel, C.; Lampignano, R.; Yang, L.; Neubauer, H.; et al. Toward a real liquid biopsy in metastatic breast and prostate cancer: Diagnostic LeukApheresis increases CTC yields in a European prospective multicenter study (CTCTrap). Int. J. Cancer 2018, 143, 2584–2591. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.G.; Hou, J.M.; Sloane, R.; Lancashire, L.; Priest, L.; Nonaka, D.; Ward, T.H.; Backen, A.; Clack, G.; Hughes, A.; et al. Analysis of circulating tumor cells in patients with non-small cell lung cancer using epithelial marker-dependent and -independent approaches. J. Thorac. Oncol. 2012, 7, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Lecharpentier, A.; Vielh, P.; Perez-Moreno, P.; Planchard, D.; Soria, J.C.; Farace, F. Detection of circulating tumour cells with a hybrid (epithelial/mesenchymal) phenotype in patients with metastatic non-small cell lung cancer. Br. J. Cancer 2011, 105, 1338–1341. [Google Scholar] [CrossRef] [PubMed]
- Hofman, V.; Long, E.; Ilie, M.; Bonnetaud, C.; Vignaud, J.M.; Flejou, J.F.; Lantuejoul, S.; Piaton, E.; Mourad, N.; Butori, C.; et al. Morphological analysis of circulating tumour cells in patients undergoing surgery for non-small cell lung carcinoma using the isolation by size of epithelial tumour cell (ISET) method. Cytopathology 2010, 23, 30–38. [Google Scholar] [CrossRef]
- Massard, C.; Oulhen, M.; Le Moulec, S.; Auger, N.; Foulon, S.; Abou-Lovergne, A.; Billiot, F.; Valent, A.; Marty, V.; Loriot, Y.; et al. Phenotypic and genetic heterogeneity of tumor tissue and circulating tumor cells in patients with metastatic castration-resistant prostate cancer: A report from the PETRUS prospective study. Oncotarget 2016, 7, 55069. [Google Scholar] [CrossRef][Green Version]
- Hofman, V.; Ilie, M.I.; Long, E.; Selva, E.; Bonnetaud, C.; Molina, T.; Vénissac, N.; Mouroux, J.; Vielh, P.; Hofman, P. Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: Comparison of the efficacy of the CellSearch AssayTM and the isolation by size of epithelial tumor cell method. Int. J. Cancer 2010, 129, 1651–1660. [Google Scholar] [CrossRef]
- Pailler, E.; Oulhen, M.; Billiot, F.; Galland, A.; Auger, N.; Faugeroux, V.; Laplace-Builhé, C.; Besse, B.; Loriot, Y.; Ngo-Camus, M.; et al. Method for semi-automated microscopy of filtration-enriched circulating tumor cells. BMC Cancer 2016, 16, 477. [Google Scholar] [CrossRef]
- Polioudaki, H.; Agelaki, S.; Chiotaki, R.; Politaki, E.; Mavroudis, D.; Matikas, A.; Georgoulias, V.; Theodoropoulos, P.A. Variable expression levels of keratin and vimentin reveal differential EMT status of circulating tumor cells and correlation with clinical characteristics and outcome of patients with metastatic breast cancer. BMC Cancer 2015, 15, 399. [Google Scholar] [CrossRef]
- Lindsay, C.R.; Le Moulec, S.; Billiot, F.; Loriot, Y.; Ngo-Camus, M.; Vielh, P.; Fizazi, K.; Massard, C.; Farace, F. Vimentin and Ki67 expression in circulating tumour cells derived from castrate-resistant prostate cancer. BMC Cancer 2016, 16, 168. [Google Scholar] [CrossRef]
- Inamura, K. Update on Immunohistochemistry for the Diagnosis of Lung Cancer. Cancers 2018, 10, 72. [Google Scholar] [CrossRef]
- The Human Protein Atlas: TTF1. Available online: https://www.proteinatlas.org/ENSG00000125482-TTF1/tissue (accessed on 3 March 2020).
- Vidigal, J.; Dias, M.M.; Fernandes, F.; Patrone, M.; Bispo, C.; Andrade, C.; Gardner, R.; Carrondo, M.J.T.; Alves, P.M.; Teixeira, A.P. A cell sorting protocol for selecting high-producing sub-populations of Sf9 and High FiveTM cells. J. Biotechnol. 2013, 168, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Pailler, E.; Adam, J.; Barthélémy, A.; Oulhen, M.; Auger, N.; Valent, A.; Borget, I.; Planchard, D.; Taylor, M.; André, F.; et al. Detection of circulating tumor cells harboring a unique ALK rearrangement in ALK-positive non–small-cell lung cancer. J. Clin. Oncol. 2013, 31, 2273–2281. [Google Scholar] [CrossRef] [PubMed]
- Geens, M.; Van De Velde, H.; De Block, G.; Goossens, E.; Van Steirteghem, A.; Tournaye, H. The efficiency of magnetic-activated cell sorting and fluorescence-activated cell sorting in the decontamination of testicular cell suspensions in cancer patients. Hum. Reprod. 2007, 22, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Cummins, I.; Steel, P.G.; Edwards, R. Identification of a carboxylesterase expressed in protoplasts using fluorescence-activated cell sorting. Plant Biotechnol. J. 2007, 5, 354–359. [Google Scholar] [CrossRef]
- Lang, J.E.; Scott, J.H.; Wolf, D.M.; Novak, P.; Punj, V.; Magbanua, M.J.M.; Zhu, W.; Mineyev, N.; Haqq, C.M.; Crothers, J.R.; et al. Expression profiling of circulating tumor cells in metastatic breast cancer. Breast Cancer Res. Treat. 2015, 149, 121–131. [Google Scholar] [CrossRef]
- Carter, L.; Rothwell, D.G.; Mesquita, B.; Smowton, C.; Leong, H.S.; Fernandez-Gutierrez, F.; Li, Y.; Burt, D.J.; Antonello, J.; Morrow, C.J.; et al. Molecular analysis of circulating tumor cells identifies distinct copy-number profiles in patients with chemosensitive and chemorefractory small-cell lung cancer. Nat. Med. 2017, 23, 114. [Google Scholar] [CrossRef]
- Stevens, M.; Oomens, L.; Broekmaat, J.; Weersink, J.; Abali, F.; Swennenhuis, J.; Tibbe, A. VyCAP’s puncher technology for single cell identification, isolation, and analysis. Cytom. Part A 2018, 93, 1255–1259. [Google Scholar] [CrossRef]
- Tamminga, M.; de Wit, S.; van de Wauwer, C.; van den Bos, H.; Swennenhuis, J.F.; Klinkenberg, T.J.; Hiltermann, T.J.N.; Andree, K.C.; Spierings, D.C.J.; Lansdorp, P.M.; et al. Release of Circulating Tumor Cells during Surgery for Non-Small Cell Lung Cancer: Are They What They Appear to Be? Clin. Cancer Res. 2019. [Google Scholar] [CrossRef]
- Aieta, M.; Facchinetti, A.; De Faveri, S.; Manicone, M.; Tartarone, A.; Possidente, L.; Lerose, R.; Mambella, G.; Calderone, G.; Zamarchi, R.; et al. Monitoring and characterization of Circulating Tumor Cells (CTCs) in a patient with EML4-ALK positive Non Small Cell Lung Cancer (NSCLC). Clin. Lung Cancer 2016, 17, e173–e177. [Google Scholar] [CrossRef]
- Hirose, T.; Murata, Y.; Oki, Y.; Sugiyama, T.; Kusumoto, S.; Ishida, H.; Shirai, T.; Nakashima, M.; Yamaoka, T.; Okuda, K.; et al. Relationship of Circulating Tumor Cells to the Effectiveness of Cytotoxic Chemotherapy in Patients With Metastatic Non-Small-Cell Lung Cancer. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2012, 20, 131–137. [Google Scholar] [CrossRef]
- Li, Y.; Cheng, X.; Chen, Z.; Liu, Y.; Liu, Z.; Xu, S. Circulating tumor cells in peripheral and pulmonary venous blood predict poor long-term survival in resected non-small cell lung cancer patients. Sci. Rep. 2017, 7, 4971. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.G.; Sloane, R.; Priest, L.; Lancashire, L.; Hou, J.-M.J.M.; Greystoke, A.; Ward, T.H.; Ferraldeschi, R.; Hughes, A.; Clack, G.; et al. Evaluation and prognostic significance of circulating tumor cells in patients with non-small-cell lung cancer. J. Clin. Oncol. 2011, 29, 1556–1563. [Google Scholar] [CrossRef] [PubMed]
- Bayarri-Lara, C.; Ortega, F.G.; de Guevara, A.C.; Puche, J.L.; Zafra, J.R.; de Miguel-Pérez, D.; Ramos, A.S.; Giraldo-Ospina, C.F.; Gómez, J.A.; Delgado-Rodriguez, M.; et al. Circulating tumor cells identify early recurrence in patients with non-small cell lung cancer undergoing radical resection. PLoS ONE 2016, 11, e0148659. [Google Scholar] [CrossRef]
- Dorsey, J.F.; Kao, G.D.; Macarthur, K.M.; Ju, M.; Steinmetz, D.; Paul, E.; Ii, C.B.S.; Hahn, S.M. Tracking Viable Circulating Tumor Cells (CTCs) in the Peripheral Blood of Non-Small Cell Lung Cancer Patients Undergoing Definitive Radiation Therapy: Pilot Study Results. Cancer 2015, 121, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Nel, I.; Jehn, U.; Gauler, T.; Hoffmann, A.-C. Individual profiling of circulating tumor cell composition in patients with non-small cell lung cancer receiving platinum based treatment. Transl. Lung Cancer Res. 2014, 3, 100–106. [Google Scholar]
- Maheswaran, S.; Sequist, L.V.; Nagrath, S.; Ulkus, L.; Brannigan, B.; Collura, C.V.; Inserra, E.; Diederichs, S.; Iafrate, A.J.; Bell, D.W.; et al. Detection of Mutations in EGFR in Circulating Lung-Cancer Cells. N. Engl. J. Med. 2008, 359, 366–377. [Google Scholar] [CrossRef]
- Lambros, M.B.; Seed, G.; Sumanasuriya, S.; Gil, V.; Crespo, M.; Fontes, M.; Chandler, R.; Mehra, N.; Fowler, G.; Ebbs, B.; et al. Single-Cell Analyses of Prostate Cancer Liquid Biopsies Acquired by Apheresis. Clin. Cancer Res. 2018, 24, 5635–5644. [Google Scholar] [CrossRef]
- McLeod, B.C.; Sniecinski, I.; Ciavarella, D.; Owen, H.; Price, T.H.; Randels, M.J.; Smith, J.W. Frequency of immediate adverse effects associated with therapeutic apheresis. Transfusion 1999, 39, 282–288. [Google Scholar] [CrossRef]
- Crocco, I.; Franchini, M.; Garozzo, G.; Gandini, A.R.; Gandini, G.; Bonomo, P.; Aprili, G. Adverse reactions in blood and apheresis donors: Experience from two Italian transfusion centres. Blood Transfus. 2009, 7, 35. [Google Scholar]
- Kraal, K.C.J.M.; Timmerman, I.; Kansen, H.M.; van den Bos, C.; Zsiros, J.; van den Berg, H.; Somers, S.; Braakman, E.; Peek, A.M.L.; van Noesel, M.M.; et al. Peripheral Stem Cell Apheresis is Feasible Post 131Iodine-Metaiodobenzylguanidine-Therapy in High-Risk Neuroblastoma, but Results in Delayed Platelet Reconstitution. Clin. Cancer Res. 2019, 25, 1012–1021. [Google Scholar] [CrossRef]
- Kiss, F.; Toth, E.; Miszti-Blasius, K.; Nemeth, N. The effect of centrifugation at various g force levels on rheological properties of rat, dog, pig and human red blood cells. Clin. Hemorheol. Microcirc. 2016, 62, 215–227. [Google Scholar] [CrossRef]
- Punzel, M.; Kozlova, A.; Quade, A.; Schmidt, A.H.; Smith, R. Evolution of MNC and lymphocyte collection settings employing different Spectra Optia ® Leukapheresis systems. Vox Sang. 2017, 112, 586–594. [Google Scholar] [CrossRef] [PubMed]
- de Wit, S.; Zeune, L.; Hiltermann, T.; Groen, H.; Dalum, G.; Terstappen, L.; de Wit, S.; Zeune, L.L.; Hiltermann, T.J.N.; Groen, H.J.M.; et al. Classification of Cells in CTC-Enriched Samples by Advanced Image Analysis. Cancers 2018, 10, 377. [Google Scholar] [CrossRef] [PubMed]
- Zeune, L. Toolbox ACCEPT. Available online: https://github.com/LeonieZ/ACCEPT (accessed on 4 March 2020).
- Zeune, L.L.; de Wit, S.; Berghuis, A.M.S.; IJzerman, M.J.; Terstappen, L.W.M.M.; Brune, C. How to Agree on a CTC: Evaluating the Consensus in Circulating Tumor Cell Scoring. Cytom. Part A 2018, 93, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Nadler, S.B.; Hidalgo, J.U.; Bloch, T. Prediction of blood volume in normal human adults. Surgery 1962, 51, 224–232. [Google Scholar] [PubMed]
- Laget, S.; Broncy, L.; Hormigos, K.; Dhingra, D.M.; BenMohamed, F.; Capiod, T.; Osteras, M.; Farinelli, L.; Jackson, S.; Paterlini-Bré chot, P. Technical Insights into Highly Sensitive Isolation and Molecular Characterization of Fixed and Live Circulating Tumor Cells for Early Detection of Tumor Invasion. PLoS ONE 2017, 12, e0169427. [Google Scholar] [CrossRef]
- van den Bos, H.; Bakker, B.; Taudt, A.; Guryev, V.; Colomé-Tatché, M.; Lansdorp, P.M.; Foijer, F.; Spierings, D.C.J. Quantification of Aneuploidy in Mammalian Systems; Humana Press: New York, NY, USA, 2019; pp. 159–190. [Google Scholar]
- Bakker, B.; Taudt, A.; Belderbos, M.E.; Porubsky, D.; Spierings, D.C.; de Jong, T.V.; Halsema, N.; Kazemier, H.G.; Hoekstra-Wakker, K.; Bradley, A.; et al. Single-cell sequencing reveals karyotype heterogeneity in murine and human malignancies. Genome Biol. 2016, 17, 115. [Google Scholar] [CrossRef]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).