Effectiveness and Costs Associated to Adding Cetuximab or Bevacizumab to Chemotherapy as Initial Treatment in Metastatic Colorectal Cancer: Results from the Observational FABIO Project

 ,
, 
 , ,
, ,
Abstract
1. Introduction
2. Results
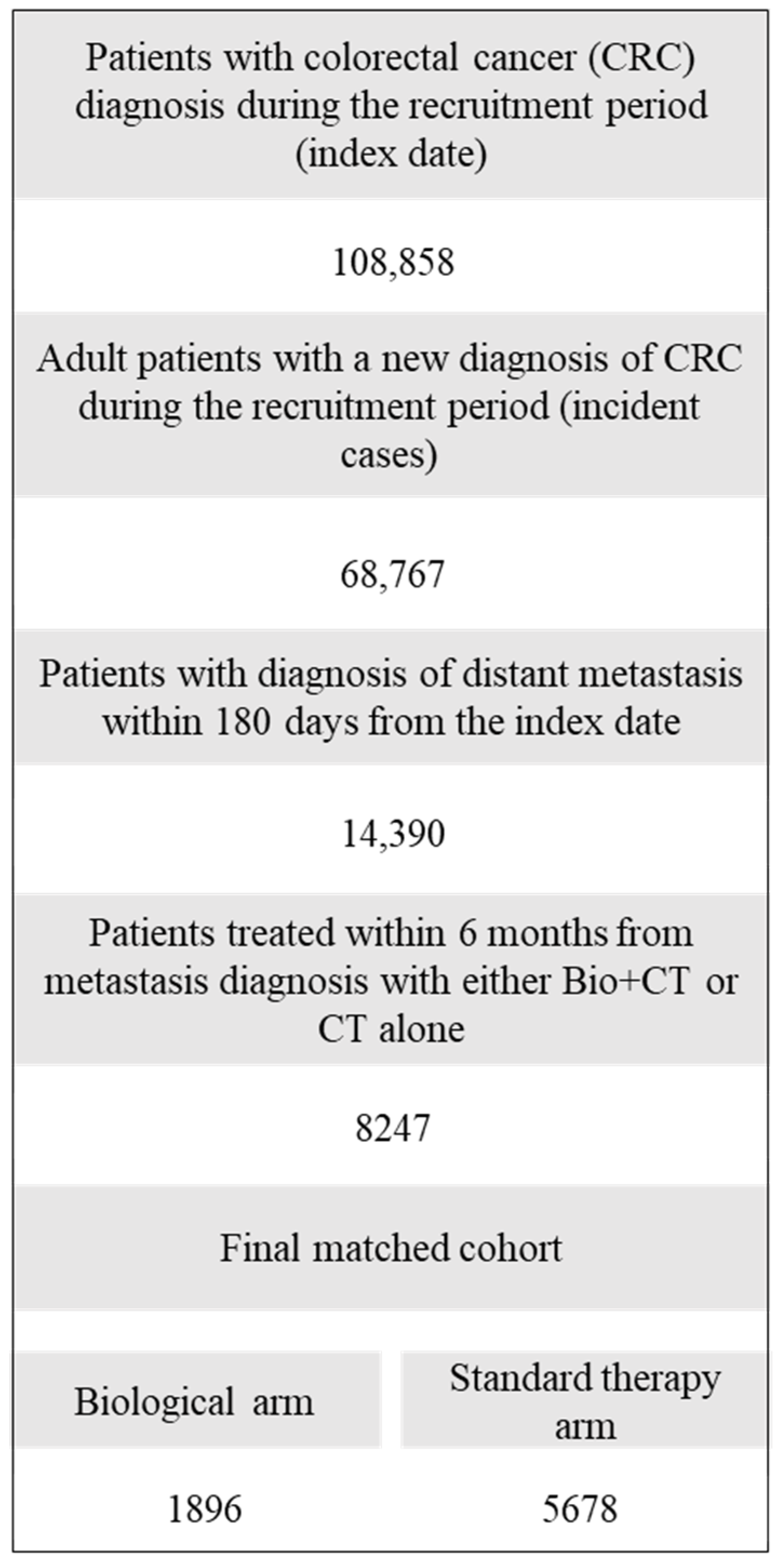
2.1. Patients
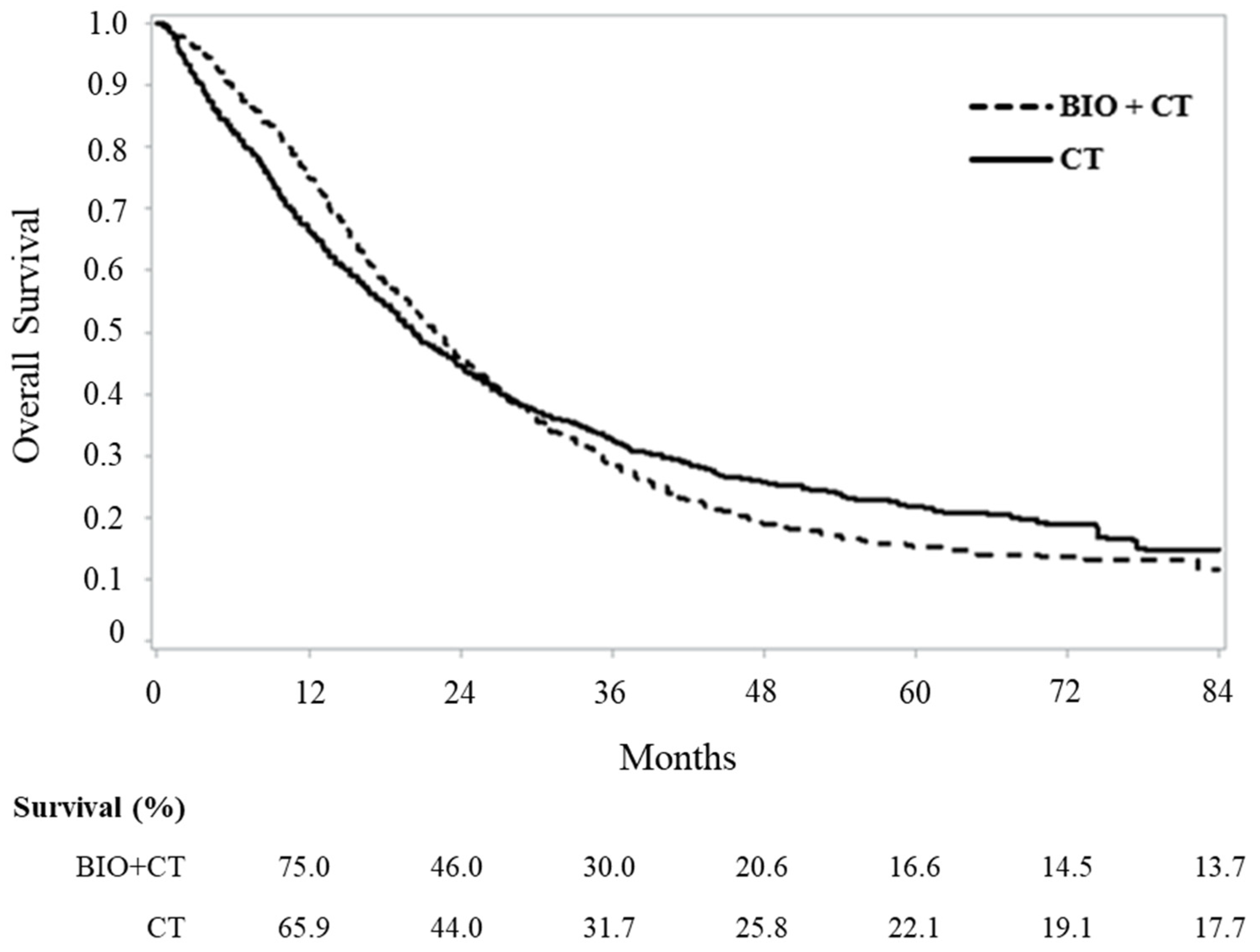
2.2. Effectiveness Profile
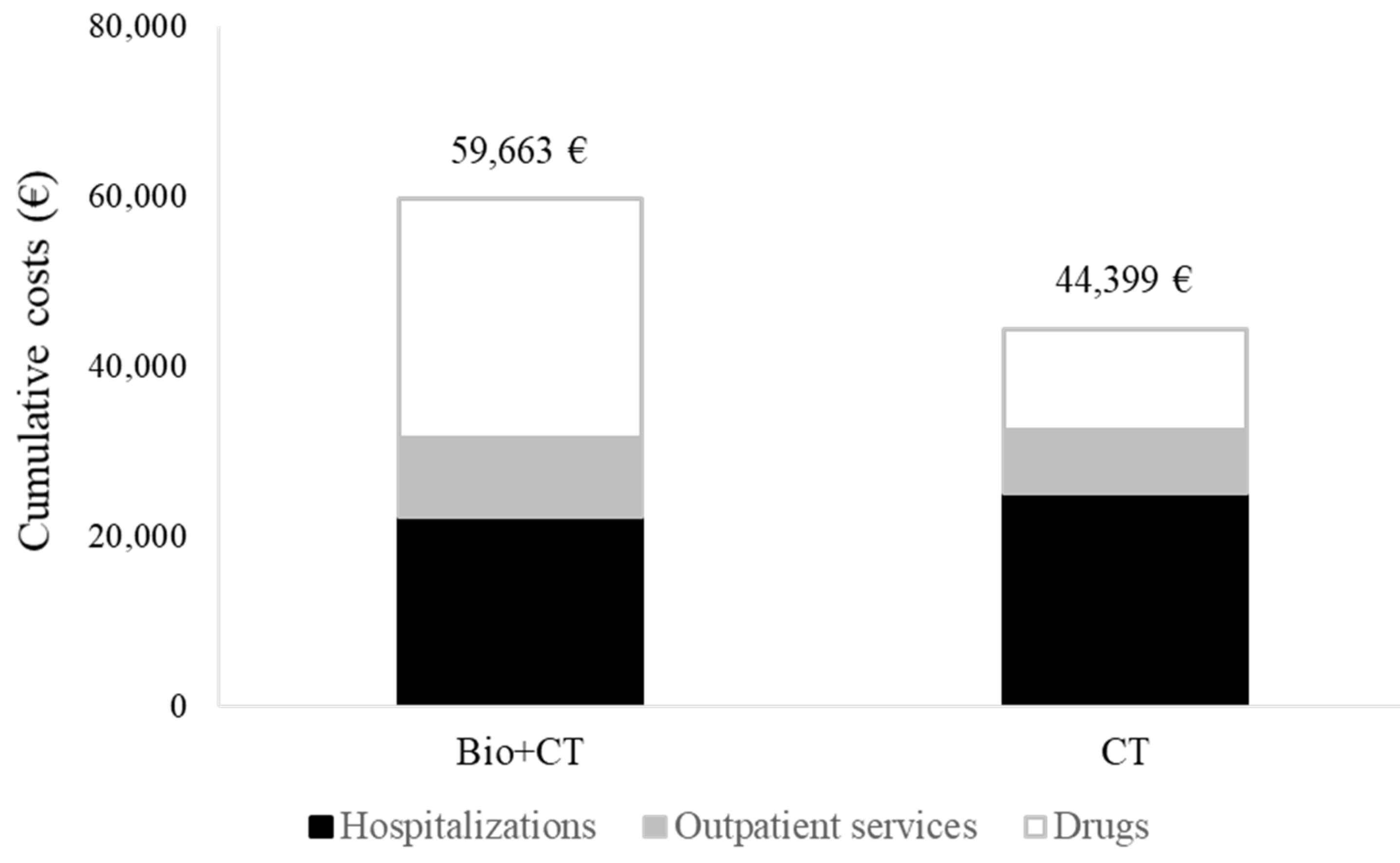
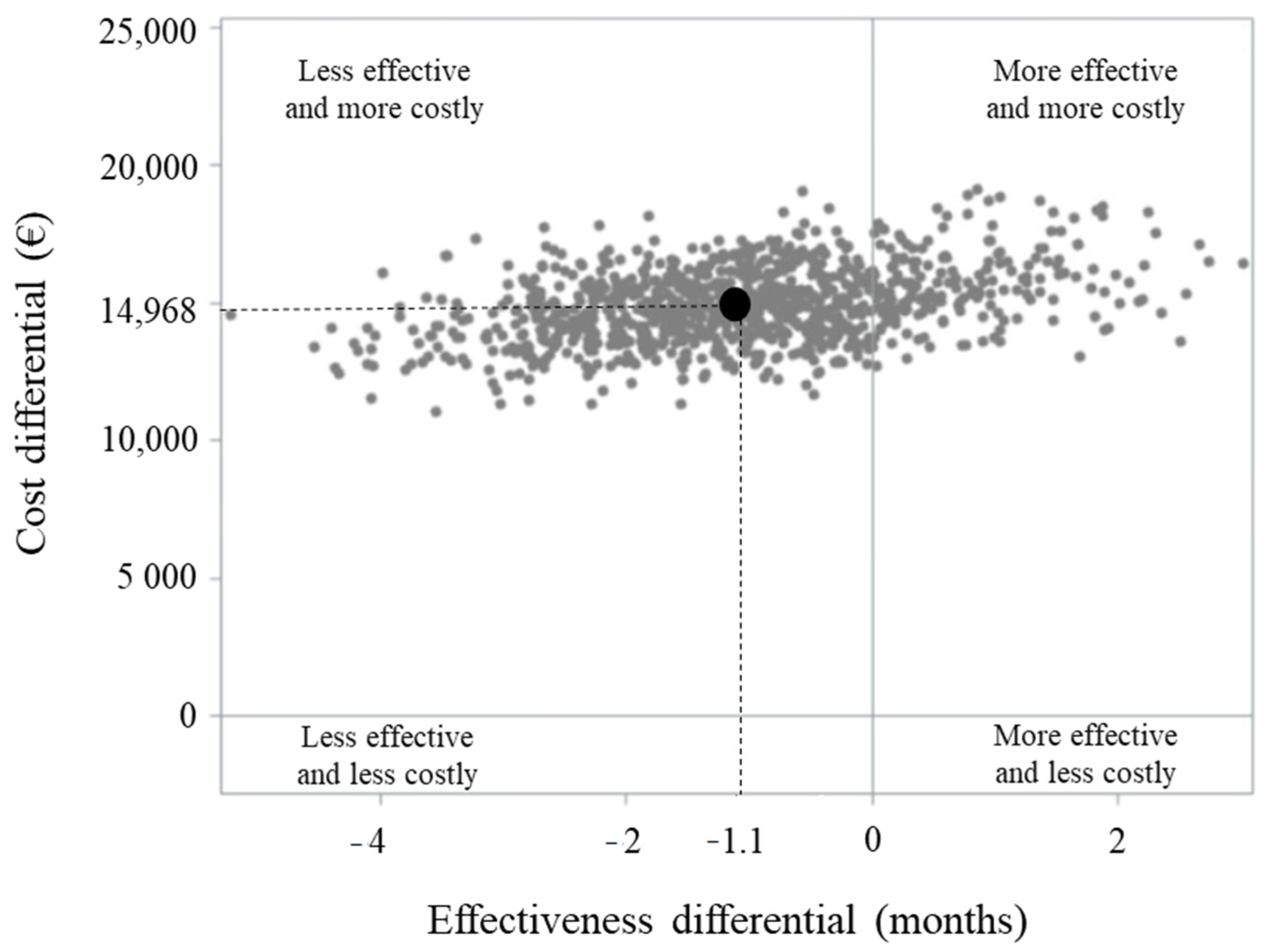
2.3. Comparing Healthcare Costs
3. Discussion
4. Materials and Methods
4.1. Data Sources
4.2. The FABIO Network
4.3. Designing, Harmonizing and Achieving Regional Cancer Research Platforms
4.4. Cohort Selection, Exposure Definition and Follow-Up
4.5. Covariates
4.6. Matching Cohort Arms
4.7. Statistical Analyses
4.8. Ethical Issues
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Kabbinavar, F.F.; Hambleton, J.; Mass, R.D.; Hurwitz, H.I.; Bergsland, E.; Sarkar, S. Combined analysis of efficacy: The addition of bevacizumab to fluorouracil/leucovorin improves survival for patients with metastatic colorectal cancer. J. Clin. Oncol. 2005, 23, 3706–3712. [Google Scholar] [CrossRef] [PubMed]
- Saltz, L.B.; Clarke, S.; Díaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.S.; Rivera, F.; et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: A randomized phase III study. J. Clin. Oncol. 2008, 26, 2013–2019. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Köhne, C.H.; Hitre, E.; Zaluski, J.; Chang Chien, C.R.; Makhson, A.; D’Haens, G.; Pintér, T.; Lim, R.; Bodoky, G.; et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N. Engl. J. Med. 2009, 360, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, C.; Bondarenko, I.; Makhson, A.; Hartmann, J.T.; Aparicio, J.; de Braud, F.; Donea, S.; Ludwig, H.; Schuch, G.; Stroh, C.; et al. Fluorouracil, leucovorin, and oxaliplatin with and without cetuximab in the first-line treatment of metastatic colorectal cancer. J. Clin. Oncol. 2009, 27, 663–671. [Google Scholar] [CrossRef]
- Franchi, M.; Barni, S.; Tagliabue, G.; Ricci, P.; Mazzucco, W.; Tumino, R.; Caputo, A.; Corrao, G.; GRETA working group. Effectiveness of First-Line Bevacizumab in Metastatic Colorectal Cancer: The Observational Cohort Study GRETA. Oncologist 2019, 24, 358–365. [Google Scholar] [CrossRef]
- Meyerhardt, J.A.; Li, L.; Sanoff, H.K.; Carpenter, W., 4th; Schrag, D. Effectiveness of bevacizumab with first-line combination chemotherapy for Medicare patients with stage IV colorectal cancer. J. Clin. Oncol. 2012, 30, 608–615. [Google Scholar] [CrossRef]
- Renouf, D.J.; Lim, H.J.; Speers, C.; Villa, D.; Gill, S.; Blanke, C.D.; O’Reilly, S.E.; Kennecke, H. Survival for metastatic colorectal cancer in the bevacizumab era: A population-based analysis. Clin. Colorectal Cancer. 2011, 10, 97–101. [Google Scholar] [CrossRef]
- Pinto, C.; Di Fabio, F.; Rosati, G.; Lolli, I.R.; Ruggeri, E.M.; Ciuffreda, L.; Ferrari, D.; Lo Re, G.; Rosti, G.; Tralongo, P.; et al. Observational study on quality of life, safety, and effectiveness of first-line cetuximab plus chemotherapy in KRAS wild-type metastatic colorectal cancer patients: The ObservEr Study. Cancer Med. 2016, 5, 3272–3281. [Google Scholar] [CrossRef]
- Muro, K.; Itabashi, M.; Hashida, H.; Masuishi, T.; Bando, H.; Denda, T.; Yamanaka, T.; Ohashi, Y.; Sugihara, K. Observational study of first-line chemotherapy including cetuximab in patients with metastatic colorectal cancer: CORAL trial. J. Clin. Oncol. 2019, 49, 339–346. [Google Scholar] [CrossRef]
- Goldstein, D.A.; Chen, Q.; Ayer, T.; Chan, K.K.W.; Virik, K.; Hammerman, A.; Brenner, B.; Flowers, C.R.; Hall, P.S. Bevacizumab for Metastatic Colorectal Cancer: A Global Cost-Effectiveness Analysis. Oncologist 2017, 22, 694–699. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Park, T.; Choi, C.J.; Choi, Y.; Suh, D.C. Cost-effectiveness of cetuximab for colorectal cancer. Expert Rev. Pharmacoecon. Outcomes Res. 2016, 16, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Huxley, N.; Crathorne, L.; Varley-Campbell, J.; Tikhonova, I.; Snowsill, T.; Briscoe, S.; Peters, J.; Bond, M.; Napier, M.; Hoyle, M. The clinical effectiveness and cost-effectiveness of cetuximab (review of technology appraisal no. 176) and panitumumab (partial review of technology appraisal no. 240) for previously untreated metastatic colorectal cancer: A systematic review and economic evaluation. Health Technol. Assess. 2017, 21, 1–294. [Google Scholar] [PubMed]
- Iannazzo, S.; Distante, C.; Lopatriello, S.; Bordonaro, R. A cost comparison of biologic treatment regimens for metastatic colorectal cancer in Italy. Glob. Reg. Health Technol. Assess. 2017, 4, e221–e226. [Google Scholar] [CrossRef][Green Version]
- Corrao, G.; Rea, F.; Di Martino, M.; De Palma, R.; Scondotto, S.; Fusco, D.; Lallo, A.; Belotti, L.M.B.; Ferrante, M.; Pollina Addario, S.; et al. Developing and validating a novel multisource comorbidity score from administrative data: A large population-based cohort study from Italy. BMJ Open 2017, 7, e019503. [Google Scholar] [CrossRef]
- Rea, F.; Ieva, F.; Pastorino, U.; Apolone, G.; Barni, S.; Merlino, L.; Franchi, M.; Corrao, G. Number of lung resections performed and long-term mortality rates of patients after lung cancer surgery: Evidence from an Italian investigation. Eur. J. Cardio-Thorac. Surg. 2020, ezaa031. [Google Scholar] [CrossRef]
- Haukoos, J.S.; Lewis, R.J. The propensity score. JAMA 2015, 314, 1637–1638. [Google Scholar] [CrossRef]
- Guyot, P.; Ades, A.E.; Ouwens, M.J.; Welton, N.J. Enhanced secondary analysis of survival data: Reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef]
- Kim, D.H.; Uno, H.; Wei, L.J. Restricted mean survival time as a measure to interpret clinical trial results. JAMA Cardiol. 2017, 2, 1179–1180. [Google Scholar] [CrossRef]
- Zhao, L.; Claggett, B.; Tian, L.; Uno, H.; Pfeffer, M.A.; Solomon, S.D.; Trippa, L.; Wei, L.J. On the restricted mean survival time curve in survival analysis. Biometrics 2016, 72, 215–221. [Google Scholar] [CrossRef]
- Pak, K.; Uno, H.; Kim, D.H.; Tian, L.; Kane, R.C.; Takeuchi, M.; Fu, H.; Claggett, B.; Wei, L.J. Interpretability of cancer clinical trial results using restricted mean survival time as an alternative to the hazard ratio. JAMA Oncol. 2017, 3, 1692–1696. [Google Scholar] [CrossRef] [PubMed]
- Bang, H.; Tsiatis, A.A. Median regression with censored cost data. Biometrics 2002, 58, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhao, H. A study on confidence intervals for incremental cost-effectiveness ratios. Biom. J. 2008, 50, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Canivet, C.; Costa, N.; Ory-Magne, F.; Arcari, C.; Mohara, C.; Pourcel, L.; Derumeaux, H.; Bérard, E.; Bourrel, R.; Molinier, L.; et al. Clinical impact and cost-effectiveness of an education program for PD patients: A randomized controlled trial. PLoS ONE 2016, 11, e0162646. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Original Cohort Members | PS-Matched Cohort Members | ||
|---|---|---|---|---|
| Bevacizumab- or cetuximab-based therapy (N = 1926) | Standard chemotherapy only (N = 6321) | Bevacizumab- or cetuximab-based therapy (N = 1896) | Standard chemotherapy only (N = 5678) | |
| Sex | ||||
| Men | 1109 (57.6) | 3608 (57.1) | 1107 (58.4) | 3316 (60.4) |
| Women | 817 (42.4) | 2713 (42.9) | 789 (41.6) | 2362 (39.6) |
| p-value† | 0.697 | 0.991 | ||
| Age at diagnosis (years) | ||||
| 18–49 | 238 (12.4) | 505 (8.0) | 237 (12.5) | 713 (12.6) |
| 50–59 | 441 (22.9) | 1049 (16.6) | 425 (22.4) | 1386 (24.4) |
| 60–69 | 669 (34.7) | 1826 (28.9) | 648 (34.2) | 1866 (32.9) |
| ≥70 | 578 (30.0) | 2941 (46.5) | 586 (30.9) | 1713 (30.2) |
| p-value† | <0.001 | 0.339 | ||
| Surgery at index hospital admission | ||||
| Yes | 1303 (67.7) | 3614 (57.2) | 1300 (68.6) | 3815 (67.2) |
| No | 623 (32.3) | 2707 (42.8) | 596 (31.4) | 1863 (32.8) |
| p-value † | <0.001 | 0.268 | ||
| Comorbidities (MCS) ‡ | ||||
| 0–2 | 1110 (57.6) | 2839 (44.9) | 1110 (58.6) | 3304 (58.2) |
| 3–5 | 632 (32.8) | 2077 (32.9) | 627 (33.1) | 1913 (33.7) |
| 6–8 | 147 (7.6) | 757 (12.0) | 126 (6.6) | 322 (5.7) |
| ≥9 | 38 (2.0) | 649 (10.3) | 33 (1.7) | 139 (2.4) |
| p-value † | <0.001 | 0.132 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franchi, M.; Garau, D.; Kirchmayer, U.; Di Martino, M.; Romero, M.; De Carlo, I.; Scondotto, S.; Corrao, G. Effectiveness and Costs Associated to Adding Cetuximab or Bevacizumab to Chemotherapy as Initial Treatment in Metastatic Colorectal Cancer: Results from the Observational FABIO Project. Cancers 2020, 12, 839. https://doi.org/10.3390/cancers12040839
Franchi M, Garau D, Kirchmayer U, Di Martino M, Romero M, De Carlo I, Scondotto S, Corrao G. Effectiveness and Costs Associated to Adding Cetuximab or Bevacizumab to Chemotherapy as Initial Treatment in Metastatic Colorectal Cancer: Results from the Observational FABIO Project. Cancers. 2020; 12(4):839. https://doi.org/10.3390/cancers12040839
Chicago/Turabian StyleFranchi, Matteo, Donatella Garau, Ursula Kirchmayer, Mirko Di Martino, Marilena Romero, Ilenia De Carlo, Salvatore Scondotto, and Giovanni Corrao. 2020. "Effectiveness and Costs Associated to Adding Cetuximab or Bevacizumab to Chemotherapy as Initial Treatment in Metastatic Colorectal Cancer: Results from the Observational FABIO Project" Cancers 12, no. 4: 839. https://doi.org/10.3390/cancers12040839
APA StyleFranchi, M., Garau, D., Kirchmayer, U., Di Martino, M., Romero, M., De Carlo, I., Scondotto, S., & Corrao, G. (2020). Effectiveness and Costs Associated to Adding Cetuximab or Bevacizumab to Chemotherapy as Initial Treatment in Metastatic Colorectal Cancer: Results from the Observational FABIO Project. Cancers, 12(4), 839. https://doi.org/10.3390/cancers12040839