Blood Free-Circulating DNA Testing of Methylated RUNX3 Is Useful for Diagnosing Early Gastric Cancer

 , , , ,
, , , , 
Abstract
1. Introduction
2. Results
2.1. CEA, CA19-9, and Serum Anti-H. Pylori Antibody Titer
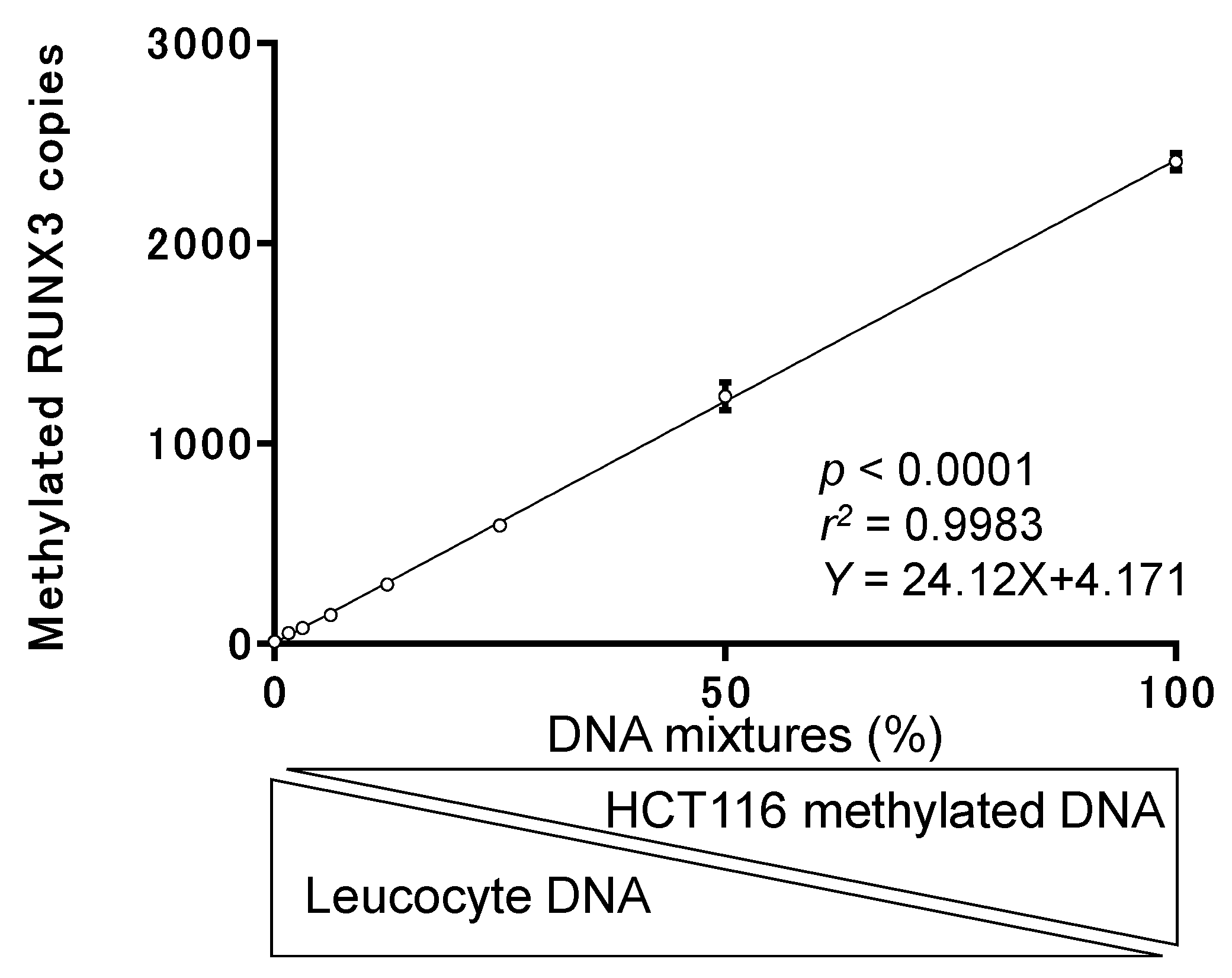
2.2. Basic Performance Test of the CORD Assay
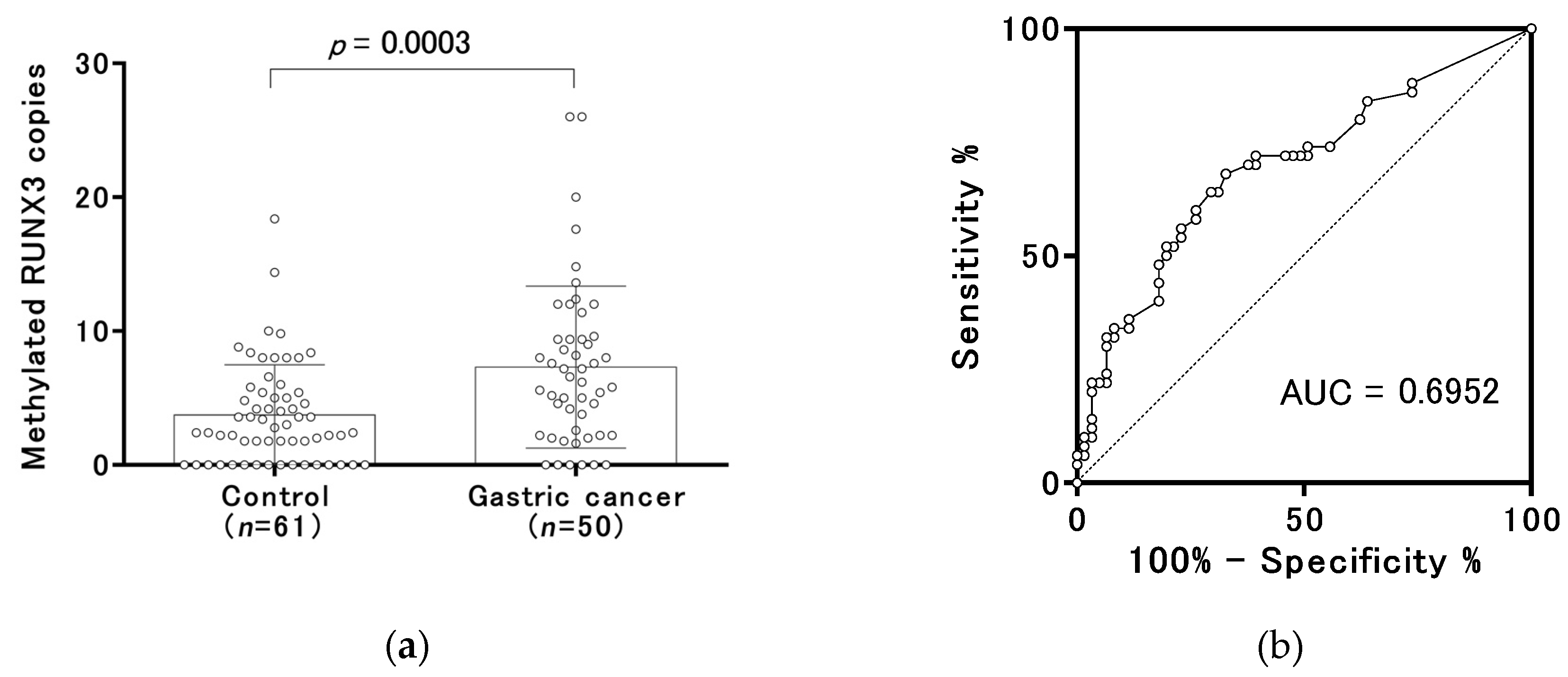
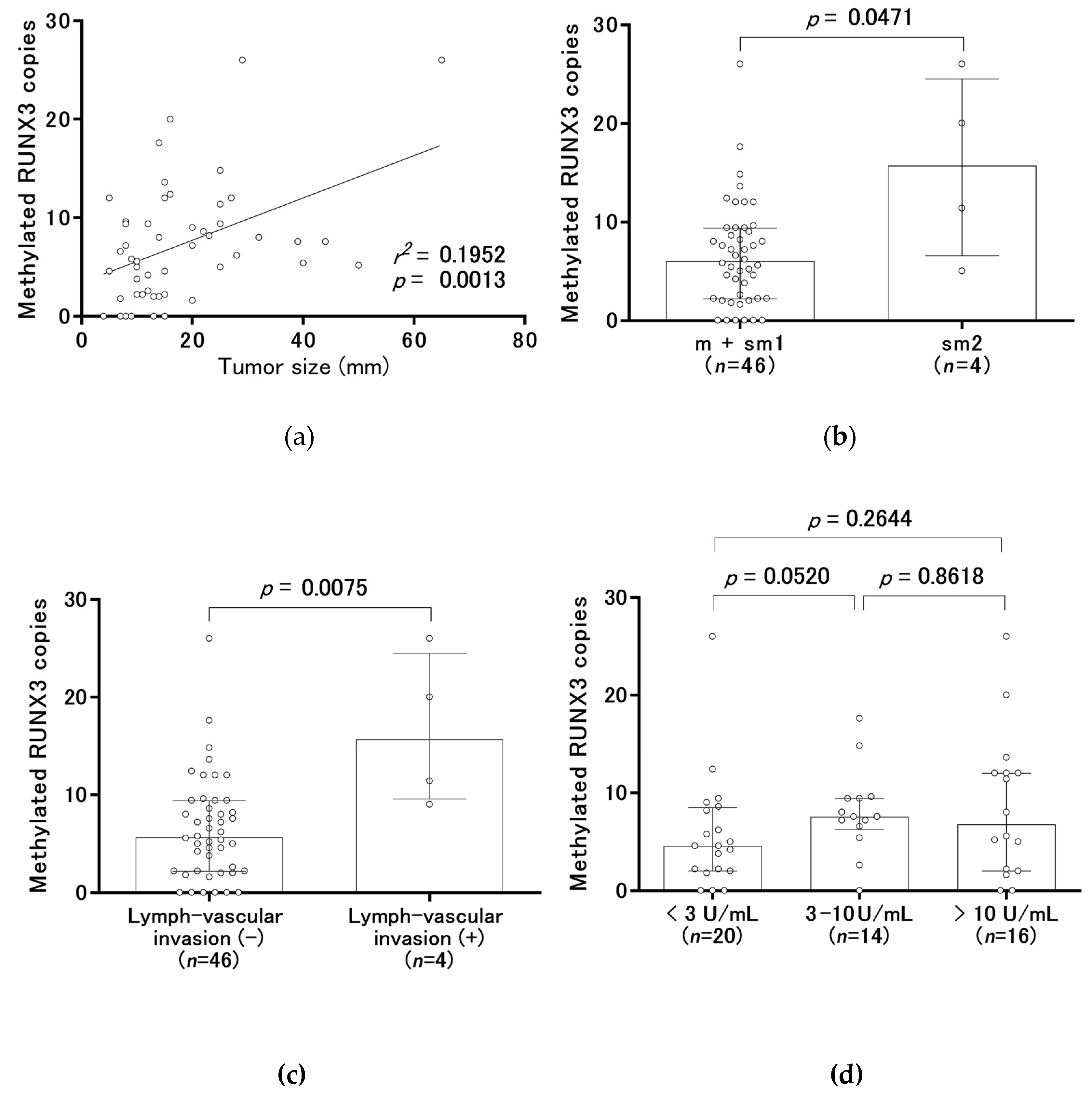
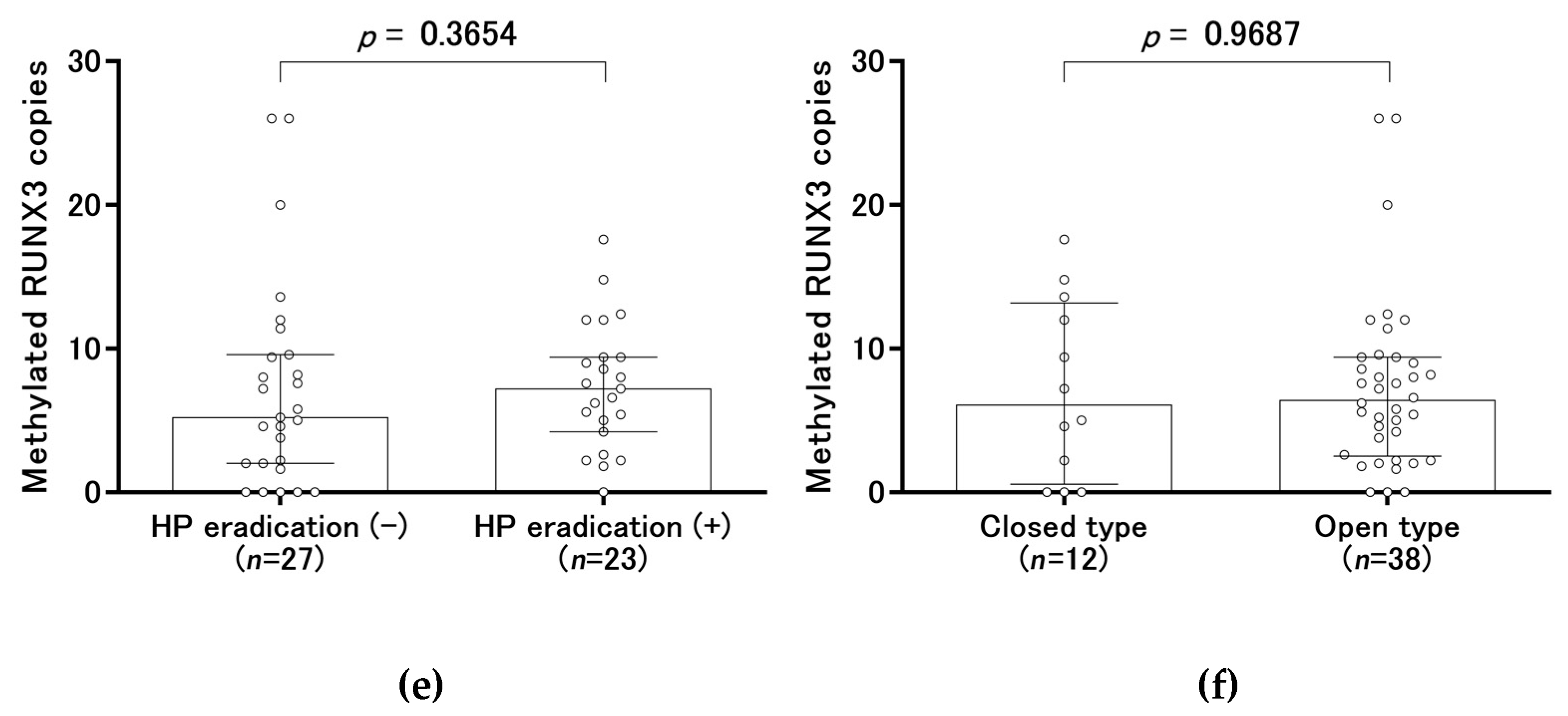
2.3. Methylated RUNX3 as a Biomarker of Early Gastric Cancer
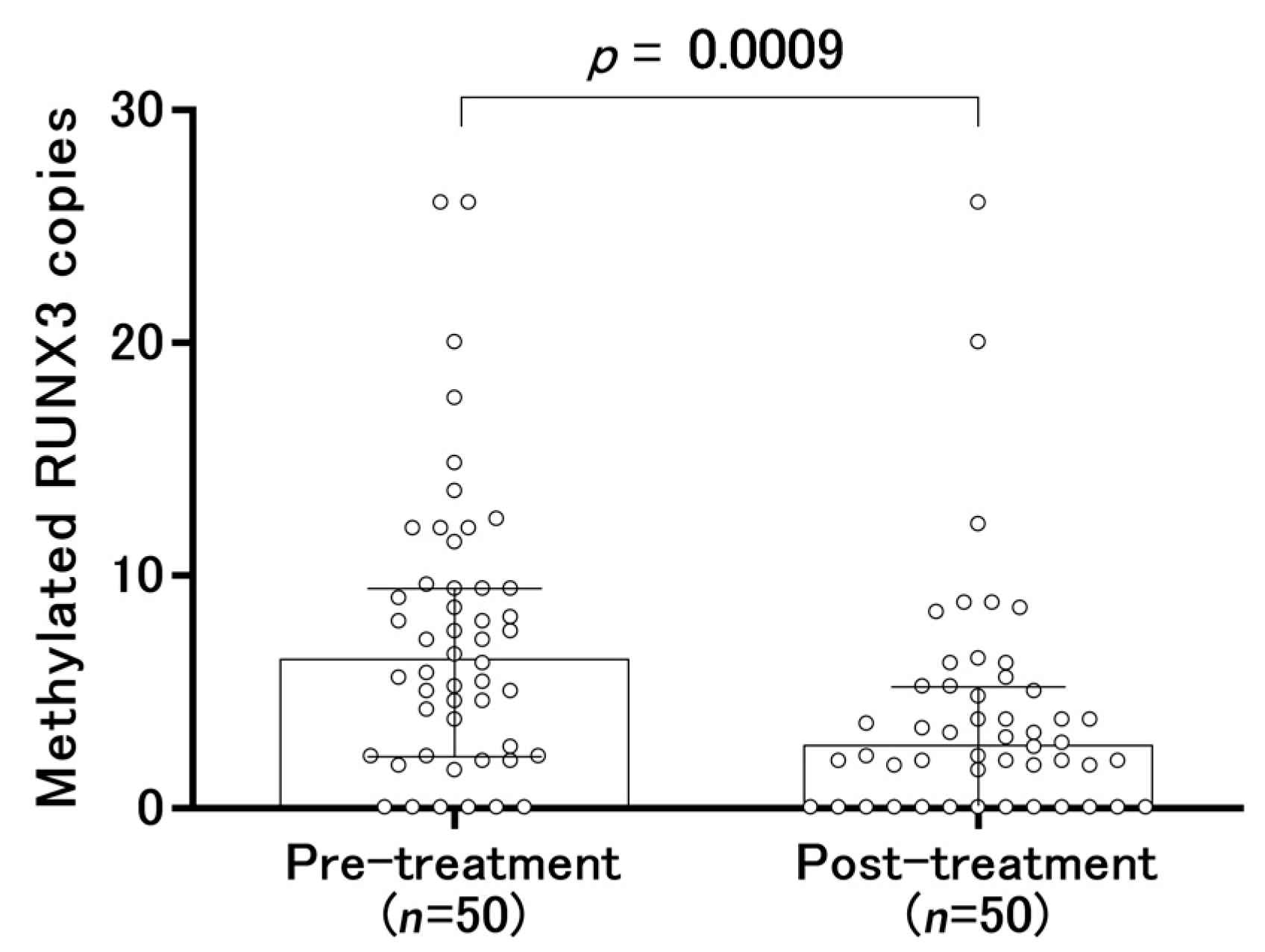
2.4. Changes in Serum-Methylated RUNX3 Copies Before and After Treatment
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Carcinoembryonic Antigen
4.3. Serum Carbohydrate Antigen 19-9
4.4. Serum Anti-H. Pylori Antibody Titer
4.5. Preparation of Samples and DNA Extraction
4.6. CORD Assay
4.7. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Hotta, T. Cancer Statistics in Japan-2018; Hotta, T., Ed.; Foundation for Promotion of Cancer Research: Tokyo, Japan, 2019. [Google Scholar]
- Takahashi, Y.; Takeuchi, T.; Sakamoto, J.; Touge, T.; Mai, M.; Ohkura, H.; Kodaira, S.; Okajima, K.; Nakazato, H.; Tumor Marker Committee. The usefulness of CEA and/or CA19-9 in monitoring for recurrence in gastric cancer patients: A prospective clinical study. Gastric Cancer 2003, 6, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Strong, V.E.; D’Amico, T.A.; Kleinberg, L.; Ajani, J. Impact of the 7th Edition AJCC staging classification on the NCCN clinical practice guidelines in oncology for gastric and esophageal cancers. J. Natl. Compr. Cancer Netw. 2013, 11, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.O.O. Gastric Cancer Screening [UpToDate®]. 2018 [Updated Feb 01, 2018]. Available online: https://www.uptodate.com/contents/gastric-cancer-screening (accessed on 10 December 2019).
- Longo, W.E.; Zucker, K.A.; Zdon, M.J.; Modlin, I.M. Detection of early gastric cancer in an aggressive endoscopy unit. Am. Surg. 1989, 55, 100–104. [Google Scholar] [PubMed]
- Dooley, C.P.; Larson, A.W.; Stace, N.H.; Renner, I.G.; Valenzuela, J.E.; Eliasoph, J.; Colletti, P.M.; Halls, J.M.; Weiner, J.M. Double-contrast barium meal and upper gastrointestinal endoscopy. A comparative study. Ann Intern. Med. 1984, 101, 538–545. [Google Scholar] [CrossRef]
- Tan, S.H.; Ida, H.; Lau, Q.C.; Goh, B.C.; Chieng, W.S.; Loh, M.; Ito, Y. Detection of promoter hypermethylation in serum samples of cancer patients by methylation-specific polymerase chain reaction for tumour suppressor genes including RUNX3. Oncol. Rep. 2007, 18, 1225–1230. [Google Scholar] [CrossRef]
- Lu, X.X.; Yu, J.L.; Ying, L.S.; Han, J.; Wang, S.; Yu, Q.M.; Wang, X.B.; Fang, X.H.; Ling, Z.Q. Stepwise cumulation of RUNX3 methylation mediated by Helicobacter pylori infection contributes to gastric carcinoma progression. Cancer 2012, 118, 5507–5517. [Google Scholar] [CrossRef]
- Llorca-Cardeñosa, M.J.; Fleitas, T.; Ibarrola-Villava, M.; Peña-Chilet, M.; Mongort, C.; Martinez-Ciarpaglini, C.; Navarro, L.; Gambardella, V.; Castillo, J.; Roselló, S.; et al. Epigenetic changes in localized gastric cancer: The role of RUNX3 in tumor progression and the immune microenvironment. Oncotarget 2016, 7, 63424–63436. [Google Scholar] [CrossRef]
- Shuto, M.; Fujioka, T.; Matsunari, O.; Okamoto, K.; Mizukami, K.; Okimoto, T.; Kodama, M.; Takigami, S.; Seguchi, C.; Nonaka, Y.; et al. Association between gastric cancer risk and serum Helicobacter pylori antibody titers. Gastroenterol. Res. Pr. 2017, 2017, 1286198. [Google Scholar] [CrossRef]
- Suehiro, Y.; Zhang, Y.; Hashimoto, S.; Takami, T.; Higaki, S.; Shindo, Y.; Suzuki, N.; Hazama, S.; Oka, M.; Nagano, H.; et al. Highly sensitive faecal DNA testing of TWIST1 methylation in combination with faecal immunochemical test for haemoglobin is a promising marker for detection of colorectal neoplasia. Ann. Clin. Biochem. 2018, 55, 59–68. [Google Scholar] [CrossRef]
- Suehiro, Y.; Hashimoto, S.; Higaki, S.; Fujii, I.; Suzuki, C.; Hoshida, T.; Matsumoto, T.; Yamaoka, Y.; Takami, T.; Sakaida, I.; et al. Blood free-circulating DNA testing by highly sensitive methylation assay to diagnose colorectal neoplasias. Oncotarget 2018, 9, 16974–16987. [Google Scholar] [CrossRef]
- Kotoh, Y.; Suehiro, Y.; Saeki, I.; Hoshida, T.; Maeda, M.; Iwamoto, T.; Matsumoto, T.; Hidaka, I.; Ishikawa, T.; Takami, T.; et al. Novel liquid biopsy test based on a sensitive methylated SEPT9 assay for diagnosing hepatocellular carcinoma. Hepatol. Commun. 2020, in press. [Google Scholar] [CrossRef]
- Iino, C.; Shimoyama, T.; Oyama, T.; Chiba, D.; Umeda, T.; Takahashi, I.; Matsuzaka, M.; Iwane, K.; Fukuda, S. Evaluation of the appropriate cut-off value for serological diagnosis of Helicobacter pylori infection by comparison with a stool antigen test. Hirosaki Med. J. 2012, 63, 48–54. [Google Scholar]
- Raizis, A.M.; Schmitt, F.; Jost, J.P. A bisulfite method of 5-methylcytosine mapping that minimizes template degradation. Anal. Biochem. 1995, 226, 161–166. [Google Scholar] [CrossRef]
- Grunau, C.; Clark, S.J.; Rosenthal, A. Bisulfite genomic sequencing: Systematic investigation of critical experimental parameters. Nucleic Acids Res. 2001, 29, E65. [Google Scholar] [CrossRef]
- Fantony, J.J.; Abern, M.R.; Gopalakrishna, A.; Owusu, R.; Tay, K.J.; Lance, R.S.; Inman, B.A. Multi-institutional external validation of urinary TWIST1 and NID2 methylation as a diagnostic test for bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 387.e1–387.e6. [Google Scholar] [CrossRef]
- Hindson, B.J.; Ness, K.D.; Masquelier, D.A.; Belgrader, P.; Heredia, N.J.; Makarewicz, A.J.; Bright, I.J.; Lucero, M.Y.; Hiddessen, A.L.; Legler, T.C.; et al. High-throughput droplet digital PCR system for absolute quantitation of DNA copy number. Anal. Chem. 2011, 83, 8604–8610. [Google Scholar] [CrossRef] [PubMed]
- Imperiale, T.F.; Ransohoff, D.F.; Itzkowitz, S.H.; Levin, T.R.; Lavin, P.; Lidgard, G.P.; Ahlquist, D.A.; Berger, B.M. Multitarget stool DNA testing for colorectal-cancer screening. N. Engl. J. Med. 2014, 370, 1287–1297. [Google Scholar] [CrossRef] [PubMed]
- Potter, N.T.; Hurban, P.; White, M.N.; Whitlock, K.D.; Lofton-Day, C.E.; Tetzner, R.; Koenig, T.; Quigley, N.B.; Weiss, G. Validation of a real-time PCR-based qualitative assay for the detection of methylated SEPT9 DNA in human plasma. Clin. Chem. 2014, 60, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.M.; Ho, T.; Brown, G.S.; Baker, R.T.; Thomas, M.L.; McEvoy, A.; Xu, Z.Z.; Ross, J.P.; Lockett, T.J.; Young, G.P.; et al. Evaluation of methylation biomarkers for detection of circulating tumor DNA and application to colorectal cancer. Genes 2016, 7, 125. [Google Scholar] [CrossRef]
- Lin, Z.; Luo, M.; Chen, X.; He, X.; Qian, Y.; Lai, S.; Si, J.; Chen, S. Combined detection of plasma ZIC1, HOXD10 and RUNX3 methylation is a promising strategy for early detection of gastric cancer and precancerous lesions. J. Cancer 2017, 8, 1038–1044. [Google Scholar] [CrossRef] [PubMed]
- Sakakura, C.; Hamada, T.; Miyagawa, K.; Nishio, M.; Miyashita, A.; Nagata, H.; Ida, H.; Yazumi, S.; Otsuji, E.; Chiba, T.; et al. Quantitative analysis of tumor-derived methylated RUNX3 sequences in the serum of gastric cancer patients. Anticancer. Res. 2009, 29, 2619–2625. [Google Scholar] [PubMed]
- Yamao, T.; Shirao, K.; Ono, H.; Kondo, H.; Saito, D.; Yamaguchi, H.; Sasako, M.; Sano, T.; Ochiai, A.; Yoshida, S. Risk factors for lymph node metastasis from intramucosal gastric carcinoma. Cancer 1996, 77, 602–606. [Google Scholar] [CrossRef]
- Gotoda, T.; Yanagisawa, A.; Sasako, M.; Ono, H.; Nakanishi, Y.; Shimoda, T.; Kato, Y. Incidence of lymph node metastasis from early gastric cancer: Estimation with a large number of cases at two large centers. Gastric Cancer 2000, 3, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Abe, N.; Sugiyama, M.; Masaki, T.; Ueki, H.; Yanagida, O.; Mori, T.; Watanabe, T.; Atomi, Y. Predictive factors for lymph node metastasis of differentiated submucosally invasive gastric cancer. Gastrointest. Endosc. 2004, 60, 242–245. [Google Scholar] [CrossRef]
- Hamabe, K.; Nishikawa, J.; Kiyotoki, S.; Saito, M.; Okamoto, T.; Yanai, H.; Hirahashi, M.; Oda, Y.; Matsusaki, K.; Kawano, T.; et al. endoscopic resection is infeasible for early gastric cancers with undifferentiated components. Hepatogastroenterology 2014, 61, 594–598. [Google Scholar]
- Tada, M.; Murakami, A.; Karita, M.; Yanai, H.; Okita, K. Endoscopic resection of early gastric cancer. Endoscopy 1993, 25, 445–450. [Google Scholar] [CrossRef]
- Nagai, A.; Hirata, M.; Kamatani, Y.; Muto, K.; Matsuda, K.; Kiyohara, Y.; Ninomiya, T.; Tamakoshi, A.; Yamagata, Z.; Mushiroda, T.; et al. Overview of the BioBank Japan Project: Study design and profile. J. Epidemiol. 2017, 27, S2–S8. [Google Scholar] [CrossRef]
- Pedersen, S.K.; Baker, R.T.; McEvoy, A.; Murray, D.H.; Thomas, M.; Molloy, P.L.; Mitchell, S.; Lockett, T.; Young, G.P.; LaPointe, L.C. A two-gene blood test for methylated DNA sensitive for colorectal cancer. PLoS ONE 2015, 10, e0125041. [Google Scholar] [CrossRef]
- Goto, A.; Nishikawa, J.; Hideura, E.; Ogawa, R.; Nagao, M.; Sasaki, S.; Kawasato, R.; Hashimoto, S.; Okamoto, T.; Ogihara, H.; et al. Lymph node metastasis can be determined by just tumor depth and lymphovascular invasion in early gastric cancer patients after endoscopic submucosal dissection. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1346–1350. [Google Scholar] [CrossRef]
- Kimura, K.; Satoh, K.; Ido, K.; Taniguchi, Y.; Takimoto, T.; Takemoto, T. Gastritis in the Japanese stomach. Scand. J. Gastroenterol. 1996, 214, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Brierley, J.D., Gospodarowicz, M.K., Wittekind, C., Eds.; Wiley-Blackwell: Hobolen, NJ, USA, 2016. [Google Scholar]
- Kotachi, T.; Ito, M.; Yoshihara, M.; Boda, T.; Kiso, M.; Masuda, K.; Matsuo, T.; Tanaka, S.; Chayama, K. Serological evaluation of gastric cancer risk based on pepsinogen and helicobacter pylori antibody: Relationship to endoscopic findings. Digestion 2017, 95, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Kishikawa, H.; Kimura, K.; Takarabe, S.; Kaida, S.; Nishida, J. Helicobacter pylori Antibody Titer and Gastric Cancer Screening. Dis. Markers 2015, 2015, 156719. [Google Scholar] [CrossRef] [PubMed]
- Nygren, A.O.; Dean, J.; Jensen, T.J.; Kruse, S.; Kwong, W.; van den Boom, D.; Ehrich, M. Quantification of fetal DNA by use of methylation-based DNA discrimination. Clin. Chem. 2010, 56, 1627–1635. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Mixtures (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| 0 | 1.56 | 3.13 | 6.25 | 12.5 | 25 | 50 | 100 | |
| Amount of template DNAs (pg) | ||||||||
| HCT116 methylated DNA | 0 | 59 | 117 | 234 | 469 | 938 | 1875 | 3750 |
| Leukocyte DNA | 3750 | 3691 | 3633 | 3516 | 3281 | 2813 | 1875 | 0 |
| Measured methylated RUNX3 | ||||||||
| Mean copy numbers | 11 | 54 | 78 | 144 | 296 | 592 | 1237 | 2408 |
| SD | 3.4 | 10.6 | 9.8 | 13.4 | 27.5 | 28.9 | 69.7 | 43.8 |
| Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age in years | 1.11 (1.06–1.16) | < 0.001 | 1.09 (1.03–1.15) | 0.0048 |
| Gender | ||||
| Male | 4.13 (1.71–9.95) | 0.0013 | 7.47 (2.05–27.23) | 0.0023 |
| Female | Reference | |||
| Gastric atrophy | ||||
| Open type | 18.30 (7.00–47.80) | <0.001 | 9.50 (2.97–30.35) | < 0.001 |
| Closed type | Reference | |||
| Methylated RUNX3 level | ||||
| >6.4 copies | 4.08 (1.76–9.46) | 0.0011 | 4.43 (1.38–14.28) | 0.0126 |
| ≤6.4 copies | Reference | |||
| Parameters | Category | Gastric Cancer (n = 50) | Control (n = 61) | p-Value |
|---|---|---|---|---|
| Age in years | Median (range) | 72.2 (34–90) | 58 (39–86) | <0.0001 |
| Sex | Male | 41 | 32 | 0.0013 |
| Female | 9 | 29 | ||
| Methylated RUNX3 | Median (range) | 6.4 (0.0–26.0) | 2.8 (0.0–18.4) | 0.0003 |
| Gastric atrophy | Closed type | 12 | 52 | <0.0001 |
| Open type | 38 | 9 | ||
| Tumor size (mm) | Median (range) | 14.5 (4.0–65.0) | NA | NA |
| Depth of tumor invasion | m | 42 | NA | NA |
| sm1 | 4 | |||
| sm2 | 4 | |||
| Tumor differentiation | Differentiated | 46 | NA | NA |
| Undifferentiated | 4 | |||
| Lymph-vascular invasion | Present | 4 | NA | NA |
| Absent | 46 | |||
| History of H. pylori eradication | Present | 23 | NA | NA |
| Absent | 27 | |||
| Anti-H. pylori antibody titer | >10 U/mL | 16 | NA | NA |
| 3–10 U/mL | 14 | |||
| <3 U/mL | 20 | |||
| CEA | >6.0 ng/mL | 2 | NA | NA |
| ≤6.0 ng/mL | 48 | |||
| CA19-9 | >37.0 U/mL | 0 | NA | NA |
| ≤37.0 U/mL | 50 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hideura, E.; Suehiro, Y.; Nishikawa, J.; Shuto, T.; Fujimura, H.; Ito, S.; Goto, A.; Hamabe, K.; Saeki, I.; Okamoto, T.; et al. Blood Free-Circulating DNA Testing of Methylated RUNX3 Is Useful for Diagnosing Early Gastric Cancer. Cancers 2020, 12, 789. https://doi.org/10.3390/cancers12040789
Hideura E, Suehiro Y, Nishikawa J, Shuto T, Fujimura H, Ito S, Goto A, Hamabe K, Saeki I, Okamoto T, et al. Blood Free-Circulating DNA Testing of Methylated RUNX3 Is Useful for Diagnosing Early Gastric Cancer. Cancers. 2020; 12(4):789. https://doi.org/10.3390/cancers12040789
Chicago/Turabian StyleHideura, Eizaburou, Yutaka Suehiro, Jun Nishikawa, Takuya Shuto, Hiroyuki Fujimura, Shunsuke Ito, Atsushi Goto, Kouichi Hamabe, Issei Saeki, Takeshi Okamoto, and et al. 2020. "Blood Free-Circulating DNA Testing of Methylated RUNX3 Is Useful for Diagnosing Early Gastric Cancer" Cancers 12, no. 4: 789. https://doi.org/10.3390/cancers12040789
APA StyleHideura, E., Suehiro, Y., Nishikawa, J., Shuto, T., Fujimura, H., Ito, S., Goto, A., Hamabe, K., Saeki, I., Okamoto, T., Higaki, S., Fujii, I., Suzuki, C., Hoshida, T., Matsumoto, T., Takami, T., Sakaida, I., & Yamasaki, T. (2020). Blood Free-Circulating DNA Testing of Methylated RUNX3 Is Useful for Diagnosing Early Gastric Cancer. Cancers, 12(4), 789. https://doi.org/10.3390/cancers12040789