Gonadotroph Tumors Show Subtype Differences that Might Have Implications for Therapy

 ,
,
Abstract
1. Introduction
2. Results
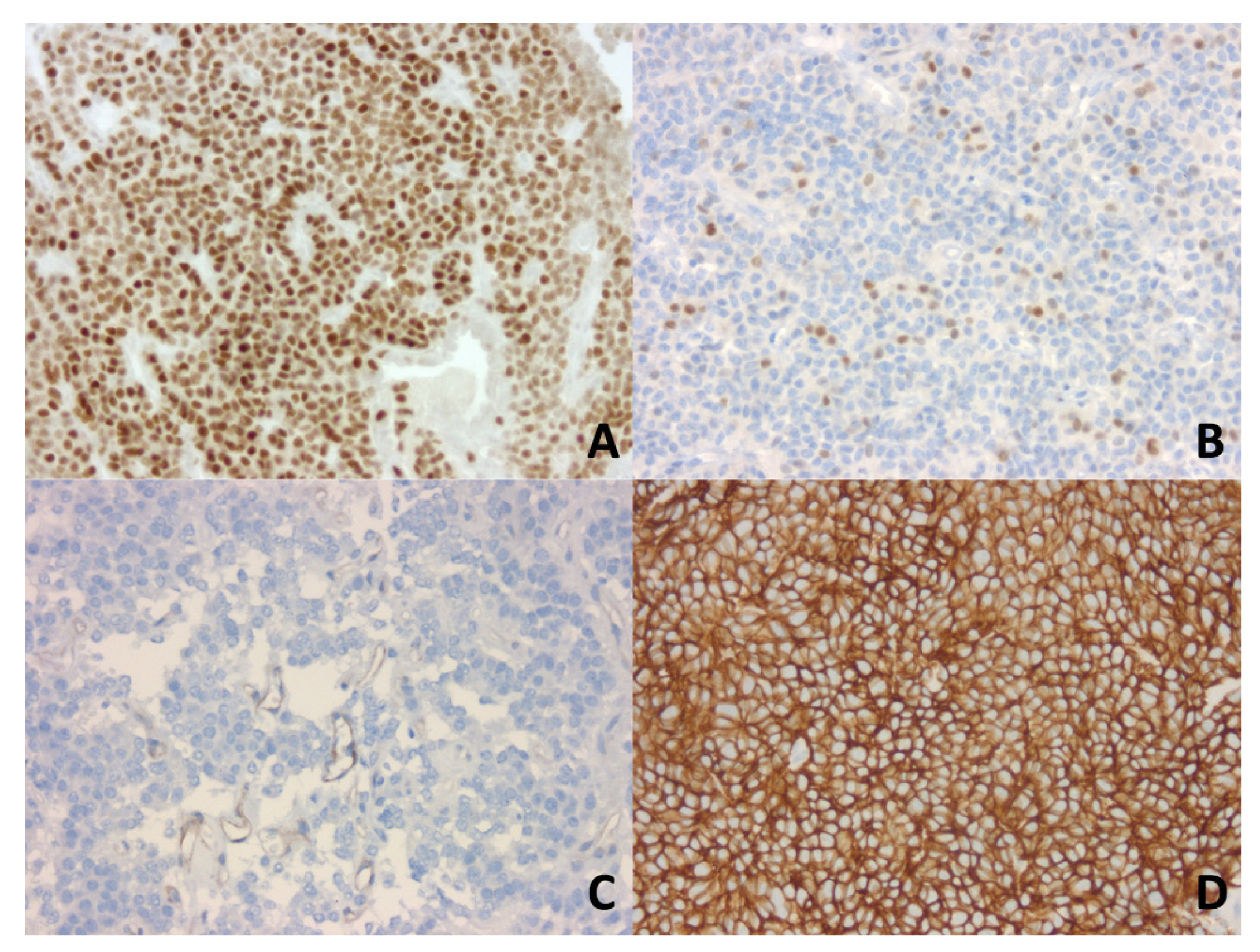
2.1. Larger Gonadotroph Tumors in Men Compared to Women
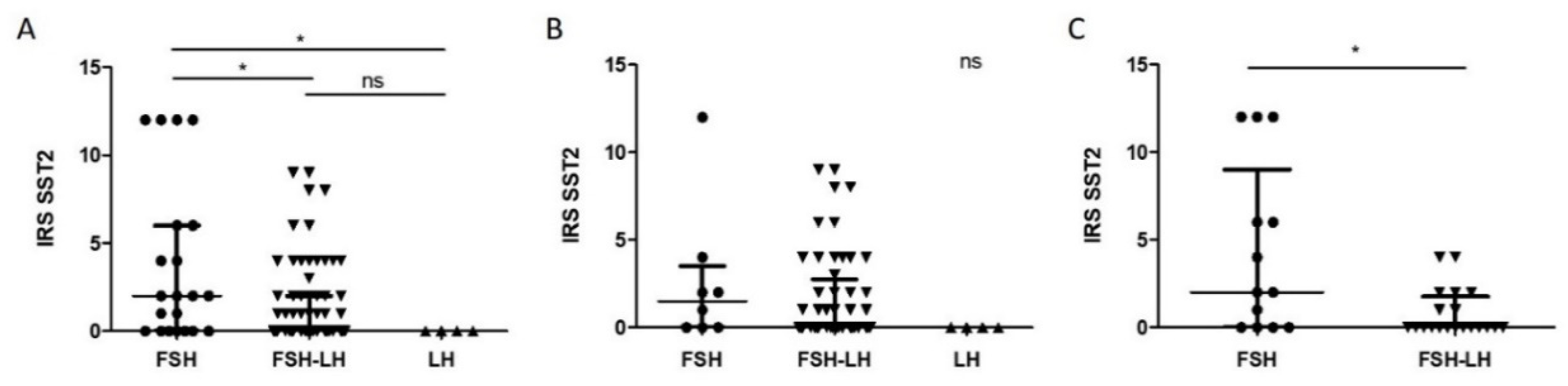
2.2. Higher IRS SST2 in FSH Compared to FSH-LH and LH Tumors
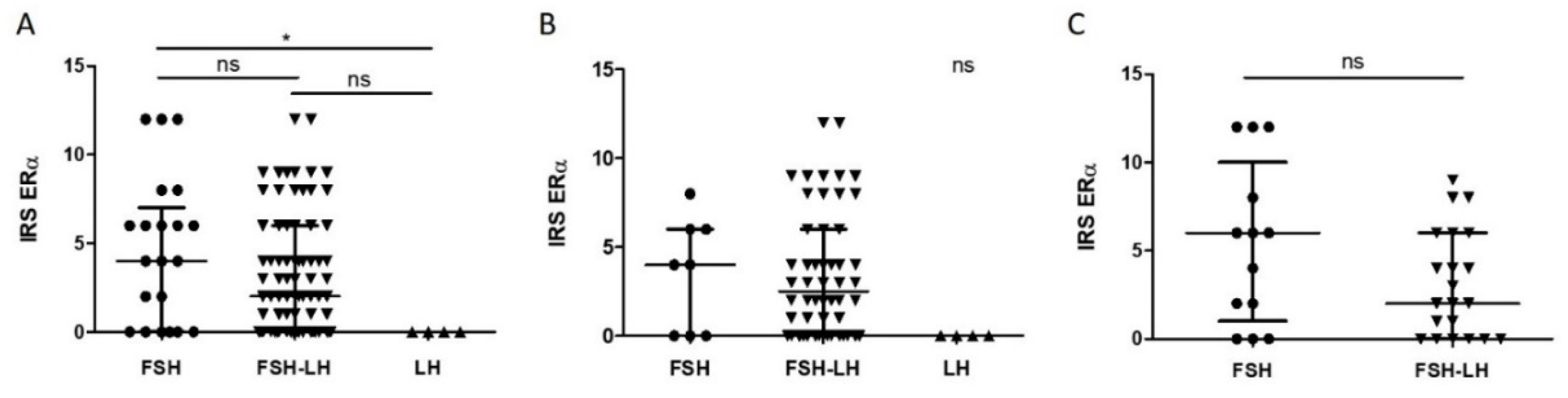
2.3. Higher IRS ERα in FSH Compared to LH Tumors
2.4. IRS ERα Correlates with IRS SST2 Especially in Men and with FSH Percentage Especially in Women
3. Discussion
4. Materials and Methods
4.1. Gonadotroph Tumor Samples
4.2. Clinicopathological Data
4.3. Automated DAB Chromogen IHC
4.4. IRS ERα, SST2 and SST5
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Asa, S.L.; Casar-Borota, O.; Chanson, P.; Delgrange, E.; Earls, P.; Ezzat, S.; Grossman, A.; Ikeda, H.; Inoshita, N.; Karavitaki, N.; et al. From pituitary adenoma to pituitary neuroendocrine tumor (PitNET): An International Pituitary Pathology Club proposal. Endocr. Relat. Cancer 2017, 24, C5–C8. [Google Scholar] [CrossRef] [PubMed]
- Villa, C.; Vasiljevic, A.; Jaffrain-Rea, M.L.; Ansorge, O.; Asioli, S.; Barresi, V.; Chinezu, L.; Gardiman, M.P.; Lania, A.; Lapshina, A.M.; et al. A standardised diagnostic approach to pituitary neuroendocrine tumours (PitNETs): A European Pituitary Pathology Group (EPPG) proposal. Virchows Arch. 2019, 475, 687–692. [Google Scholar] [CrossRef]
- Nishioka, H.; Inoshita, N.; Mete, O.; Asa, S.L.; Hayashi, K.; Takeshita, A.; Fukuhara, N.; Yamaguchi-Okada, M.; Takeuchi, Y.; Yamada, S. The Complementary Role of Transcription Factors in the Accurate Diagnosis of Clinically Nonfunctioning Pituitary Adenomas. Endocr. Pathol. 2015, 26, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Drummond, J.; Roncaroli, F.; Grossman, A.B.; Korbonits, M. Clinical and Pathological Aspects of Silent Pituitary Adenomas. J. Clin. Endocrinol. Metab. 2019, 104, 2473–2489. [Google Scholar] [CrossRef] [PubMed]
- Raverot, G.; Vasiljevic, A.; Jouanneau, E. Prognostic factors of regrowth in nonfunctioning pituitary tumors. Pituitary 2018, 21, 176–182. [Google Scholar] [CrossRef]
- Gheorghiu, M.L.; Negreanu, F.; Fleseriu, M. Updates in the Medical Treatment of Pituitary Adenomas. Horm. Metab. Res. 2020, 52, 8–24. [Google Scholar] [CrossRef]
- McCormack, A.; Dekkers, O.M.; Petersenn, S.; Popovic, V.; Trouillas, J.; Raverot, G.; Burman, P. Treatment of aggressive pituitary tumours and carcinomas: Results of a European Society of Endocrinology (ESE) survey 2016. Eur. J. Endocrinol. 2018, 178, 265–276. [Google Scholar] [CrossRef]
- Ilie, M.D.; Lasolle, H.; Raverot, G. Emerging and Novel Treatments for Pituitary Tumors. J. Clin. Med. 2019, 8, 1107. [Google Scholar] [CrossRef]
- Øystese, K.A.; Casar-Borota, O.; Normann, K.R.; Zucknick, M.; Berg, J.P.; Bollerslev, J. Estrogen Receptor α, a Sex-Dependent Predictor of Aggressiveness in Nonfunctioning Pituitary Adenomas: SSTR and Sex Hormone Receptor Distribution in NFPA. J. Clin. Endocrinol. Metab. 2017, 102, 3581–3590. [Google Scholar] [CrossRef]
- Ilie, M.D.; Vasiljevic, A.; Raverot, G.; Bertolino, P. The Microenvironment of Pituitary Tumors—Biological and Therapeutic Implications. Cancers 2019, 11, 1605. [Google Scholar] [CrossRef]
- Ho, D.M.-T.; Hsu, C.; Ting, L.-T.; Chiang, H. The clinicopathological characteristics of gonadotroph cell adenoma: A study of 118 cases. Hum. Pathol. 1997, 28, 905–911. [Google Scholar] [CrossRef]
- Young, W.F.; Scheithauer, B.W.; Kovacs, K.T.; Horvath, E.; Davis, D.H.; Randall, R.V. Gonadotroph Adenoma of the Pituitary Gland: A Clinicopathologic Analysis of 100 Cases. Mayo Clin. Proc. 1996, 71, 649–656. [Google Scholar] [CrossRef]
- Trouillas, J.; Girod, C.; Sassolas, G.; Claustrat, B. The human gonadotropic adenoma: Pathologic diagnosis and hormonal correlations in 26 tumors. Semin Diagn. Pathol. 1986, 3, 42–57. [Google Scholar] [PubMed]
- Croue, A.; Beldent, V.; Rousselet, M.-C.; Guy, G.; Rohmer, V.; Bigorgne, J.-C.; Saint-Andre, J.-P. Contribution of immunohistochemistry, electron microscopy, and cell culture to the characterization of nonfunctioning pituitary adenomas: A study of 40 cases. Hum. Pathol. 1992, 23, 1332–1339. [Google Scholar] [CrossRef]
- Even-Zohar, N.; Greenman, Y. Management of NFAs: Medical treatment. Pituitary 2018, 21, 168–175. [Google Scholar] [CrossRef]
- Fusco, A.; Giampietro, A.; Bianchi, A.; Cimino, V.; Lugli, F.; Piacentini, S.; Lorusso, M.; Tofani, A.; Perotti, G.; Lauriola, L.; et al. Treatment with octreotide LAR in clinically non-functioning pituitary adenoma: Results from a case–control study. Pituitary 2012, 15, 571–578. [Google Scholar] [CrossRef]
- Zawada, N.B.; Kunert-Radek, J.; Pawlikowski, M.; Pisarek, H.; Radek, M. Ocena efektów leczenia analogami somatostatyny nieczynnych hormonalnie gruczolaków przysadki w porównaniu z akromegalią. Endokrynol. Pol. 2016, 67. [Google Scholar] [CrossRef]
- Colao, A.; Di Somma, C.; Pivonello, R.; Faggiano, A.; Lombardi, G.; Savastano, S. Medical therapy for clinically non-functioning pituitary adenomas. Endocr. Relat. Cancer 2008, 15, 905–915. [Google Scholar] [CrossRef]
- Lee, M.; Lupp, A.; Mendoza, N.; Martin, N.; Beschorner, R.; Honegger, J.; Schlegel, J.; Shively, T.; Pulz, E.; Schulz, S.; et al. SSTR3 is a putative target for the medical treatment of gonadotroph adenomas of the pituitary. Endocr. Relat. Cancer 2015, 22, 111–119. [Google Scholar] [CrossRef]
- Castellnou, S.; Vasiljevic, A.; Lapras, V.; Raverot, V.; Alix, E.; Borson-Chazot, F.; Jouanneau, E.; Raverot, G.; Lasolle, H. SST5 expression and USP8 mutation in functioning and silent corticotroph pituitary tumors. Endocr. Connect. 2020, 9, 243–253. [Google Scholar] [CrossRef]
- Neou, M.; Villa, C.; Armignacco, R.; Jouinot, A.; Raffin-Sanson, M.-L.; Septier, A.; Letourneur, F.; Diry, S.; Diedisheim, M.; Izac, B.; et al. Pangenomic Classification of Pituitary Neuroendocrine Tumors. Cancer Cell 2020, 37, 123–134.e5. [Google Scholar] [CrossRef] [PubMed]
- Greenman, Y.; Cooper, O.; Yaish, I.; Robenshtok, E.; Sagiv, N.; Jonas-Kimchi, T.; Yuan, X.; Gertych, A.; Shimon, I.; Ram, Z.; et al. Treatment of clinically nonfunctioning pituitary adenomas with dopamine agonists. Eur. J. Endocrinol. 2016, 175, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Vieira Neto, L.; Wildemberg, L.E.; Moraes, A.B.; Colli, L.M.; Kasuki, L.; Marques, N.V.; Gasparetto, E.L.; de Castro, M.; Takiya, C.M.; Gadelha, M.R. Dopamine receptor subtype 2 expression profile in nonfunctioning pituitary adenomas and in vivo response to cabergoline therapy. Clin. Endocrinol. (Oxf.) 2015, 82, 739–746. [Google Scholar] [CrossRef]
- Garcia, E.C.; Naves, L.A.; Silva, A.O.; de Castro, L.F.; Casulari, L.A.; Azevedo, M.F. Short-term treatment with cabergoline can lead to tumor shrinkage in patients with nonfunctioning pituitary adenomas. Pituitary 2013, 16, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Batista, R.L.; Musolino, N.R.C.; Cescato, V.A.S.; da Silva, G.O.; Medeiros, R.S.S.; Herkenhoff, C.G.B.; Trarbach, E.B.; Cunha-Neto, M.B. Cabergoline in the Management of Residual Nonfunctioning Pituitary Adenoma: A Single-Center, Open-Label, 2-Year Randomized Clinical Trial. Am. J. Clin. Oncol. 2019, 42, 221–227. [Google Scholar] [CrossRef]
- Pivonello, R.; Matrone, C.; Filippella, M.; Cavallo, L.M.; Di Somma, C.; Cappabianca, P.; Colao, A.; Annunziato, L.; Lombardi, G. Dopamine Receptor Expression and Function in Clinically Nonfunctioning Pituitary Tumors: Comparison with the Effectiveness of Cabergoline Treatment. J. Clin. Endocrinol. Metab. 2004, 89, 1674–1683. [Google Scholar] [CrossRef]
- Delgrange, E.; Vasiljevic, A.; Wierinckx, A.; François, P.; Jouanneau, E.; Raverot, G.; Trouillas, J. Expression of estrogen receptor alpha is associated with prolactin pituitary tumor prognosis and supports the sex-related difference in tumor growth. Eur. J. Endocrinol. 2015, 172, 791–801. [Google Scholar] [CrossRef]
- Manoranjan, B.; Salehi, F.; Scheithauer, B.W.; Rotondo, F.; Kovacs, K.; Cusimano, M.D. Estrogen receptors alpha and beta immunohistochemical expression: Clinicopathological correlations in pituitary adenomas. Anticancer Res. 2010, 30, 2897–2904. [Google Scholar]
- Nishioka, H.; Tamura, K.; Iida, H.; Kutsukake, M.; Endo, A.; Ikeda, Y.; Haraoka, J. Co-expression of somatostatin receptor subtypes and estrogen receptor-α mRNAs by non-functioning pituitary adenomas in young patients. Mol. Cell. Endocrinol. 2011, 331, 73–78. [Google Scholar] [CrossRef]
- Xu, Y.; Song, J.; Berelowitz, M.; Bruno, J.F. Estrogen regulates somatostatin receptor subtype 2 messenger ribonucleic acid expression in human breast cancer cells. Endocrinology 1996, 137, 5634–5640. [Google Scholar] [CrossRef]
- Kimura, N.; Takamatsu, N.; Yaoita, Y.; Osamura, R.Y.; Kimura, N. Identification of transcriptional regulatory elements in the human somatostatin receptor sst2 promoter and regions including estrogen response element half-site for estrogen activation. J. Mol. Endocrinol. 2008, 40, 75–91. [Google Scholar] [CrossRef] [PubMed]
- Kumar, U.; Grigorakis, S.I.; Watt, H.L.; Sasi, R.; Snell, L.; Watson, P.; Chaudhari, S. Somatostatin receptors in primary human breast cancer: Quantitative analysis of mRNA for subtypes 1–5 and correlation with receptor protein expression and tumor pathology. Breast Cancer Res. Treat. 2005, 92, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Imani, M.; Khamseh, M.E.; Asadi, P.; Ghorbani, M.; Akbari, H.; Alaei-Shahmiri, F.; Honardoost, M.; Kaynama, M.R.; Malek, M. Comparison of cabergoline versus raloxifene add-on therapy to long-acting somatostatin analogue in patients with inadequately controlled acromegaly: A randomized open label clinical trial. Endocr. Pract. 2018, 24, 542–547. [Google Scholar] [CrossRef]
- Tiburio Therapeutics. Available online: https://www.tiburio.com/our-programs/tbr-760/ (accessed on 14 March 2020).
- Trouillas, J.; Roy, P.; Sturm, N.; Dantony, E.; Viennet, G.; Bonneville, J.-F.; Assaker, R.; Auger, C.; Brue, T.; Cornelius, A.; et al. A new prognostic clinicopathological classification of pituitary adenomas: A multicentric case–control study of 410 patients with 8 years post-operative follow-up. Acta Neuropathol. (Berl.) 2013, 126, 123–135. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | All Tumors | Males | Females | p-Value (Males vs. Females) |
|---|---|---|---|---|
| Age at surgery time (years) (n = 98/64/34) | 63 (33–86) | 63 (37–86) | 61 (33–80) | 0.44 |
| Maximal diameter (mm) (n = 98/64/34) | 27 (13–51) | 28 (13–51) | 24 (13–41) | 0.01 |
| Histological subtype (n = 98/64/34) | ||||
| FSH | 21 (21.4%) | 8 (12.5%) | 13 (38.2%) | ND |
| FSH-LH | 73 (74.5%) | 52 (81.25%) | 21 (61.8%) | |
| LH | 4 (4.1%) | 4 (6.25%) | 0 (0%) | |
| Ki67 index (n = 98/64/34) | ||||
| <3 | 84 (85.7%) | 55 (85.9%) | 29 (85.3%) | 0.93 |
| ≥3 | 14 (14.3%) | 9 (14.1%) | 5 (14.7%) | |
| Mitoses (n = 98/64/34) | ||||
| ≤2 | 89 (90.8%) | 60 (93.75%) | 29 (85.3%) | 0.26 |
| >2 | 9 (9.2%) | 4 (6.25%) | 5 (14.7%) | |
| p53 (n = 98/64/34) | ||||
| negative | 60 (61.2%) | 40 (62.5%) | 20 (58.8%) | 0.72 |
| positive | 38 (38.8%) | 24 (37.5%) | 14 (41.2%) | |
| Proliferation (n = 98/64/34) | ||||
| No | 84 (85.7%) | 56 (87.5%) | 28 (82.4%) | 0.48 |
| Yes | 14 (14.3%) | 8 (12.5%) | 6 (17.6%) | |
| Invasion (n = 94/62/32) | ||||
| Yes | 53 (56.4%) | 37 (59.7%) | 16 (50%) | 0.37 |
| No | 41 (43.6%) | 25 (40.3%) | 16 (50%) | |
| Grade (n = 94/62/32) | ||||
| 1a | 35 (37.2%) | 23 (37.1%) | 12 (37.5%) | ND |
| 1b | 6 (6.4%) | 2 (3.2%) | 4 (12.5%) | |
| 2a | 47 (50%) | 32 (51.6%) | 15 (46.9%) | |
| 2b | 6 (6.4%) | 5 (8.1%) | 1 (3.1%) | |
| IRS ERα (n = 98/64/34) | 2.5 (0–12) | 2 (0–12) | 3.5 (0–12) | 0.35 |
| IRS SST2 (n = 97/64/33) | 0 (0–12) | 0 (0–12) | 0 (0–12) | 0.58 |
| IRS SST5 (n = 21/11/10) | 0 (0–0) | 0 (0–0) | 0 (0–0) | ND |
| Complete surgical removal (n = 93/60/33) | ||||
| Yes | 57 (61.3%) | 36 (60%) | 21 (63.6%) | 0.73 |
| No | 36 (38.7%) | 24 (40%) | 12 (36.4%) | |
| Follow-up > 1 year (months) (n = 62/42/20, of which n = 2/1/1 had adjuvant RT) | 43.0 (12.6–88.2) | 46.3 (12.6–88.2) | 37.6 (14.1–69.2) | |
| Relapse or progression > 1 year (n = 60/41/19) | ||||
| Yes | 11 (18.3%) | 8 (19.5%) | 3 (15.8%) | 1 |
| No | 49 (81.7%) | 33 (80.5%) | 16 (84.2%) |
| Clinicopathological Characteristics | IRS SST2 | FSH (%) | LH (%) | Age (years) | Diameter (mm) |
|---|---|---|---|---|---|
| Spearman’s Rho/Adjusted p-Value (Holm’s Method)/n | |||||
| IRS ERα | |||||
| All | 0.44/<0.0001/97 | 0.40/0.0005/98 | −0.05/1/98 | 0.06/1/98 | 0.04/1/98 |
| Males | 0.51/0.0002/64 | 0.31/0.16/64 | 0.01/1/64 | 0.11/1/64 | 0.04/1/64 |
| Females | 0.32/0.83/33 | 0.58/0.004/34 | −0.16/1/34 | −0.006/1/34 | 0.13/1/34 |
| IRS SST2 | |||||
| All | 0.23/0.24/97 | −0.13/1/97 | 0.23/0.26/98 | −0.19/0.65/98 | |
| Males | 0.18/1/64 | −0.02/1/64 | 0.29/0.24/64 | −0.28/0.29/64 | |
| Females | 0.32/0.82/33 | −0.36/0.55/33 | 0.10/1/33 | 0.03/1/33 | |
| FSH (%) | |||||
| All | −0.04/1/98 | 0.13/1/98 | 0.02/1/98 | ||
| Males | 0.10/1/64 | 0.18/1/64 | 0.04/1/64 | ||
| Females | −0.30/0.92/34 | 0.05/1/34 | 0.07/1/34 | ||
| LH (%) | |||||
| All | 0.17/0.90/98 | 0.08/1/98 | |||
| Males | 0.13/1/64 | −0.01/1/64 | |||
| Females | 0.18/1/34 | 0.02/1/34 | |||
| Age (years) | |||||
| All | −0.03/1/98 | ||||
| Males | −0.12/1/64 | ||||
| Females | 0.12/1/34 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilie, M.D.; Vasiljevic, A.; Louvet, C.; Jouanneau, E.; Raverot, G. Gonadotroph Tumors Show Subtype Differences that Might Have Implications for Therapy. Cancers 2020, 12, 1012. https://doi.org/10.3390/cancers12041012
Ilie MD, Vasiljevic A, Louvet C, Jouanneau E, Raverot G. Gonadotroph Tumors Show Subtype Differences that Might Have Implications for Therapy. Cancers. 2020; 12(4):1012. https://doi.org/10.3390/cancers12041012
Chicago/Turabian StyleIlie, Mirela Diana, Alexandre Vasiljevic, Camille Louvet, Emmanuel Jouanneau, and Gérald Raverot. 2020. "Gonadotroph Tumors Show Subtype Differences that Might Have Implications for Therapy" Cancers 12, no. 4: 1012. https://doi.org/10.3390/cancers12041012
APA StyleIlie, M. D., Vasiljevic, A., Louvet, C., Jouanneau, E., & Raverot, G. (2020). Gonadotroph Tumors Show Subtype Differences that Might Have Implications for Therapy. Cancers, 12(4), 1012. https://doi.org/10.3390/cancers12041012