The Impact of Surgical Margins and Adjuvant Radiotherapy in Patients with Undifferentiated Pleomorphic Sarcomas of the Extremities: A Single-Institutional Analysis of 192 Patients

 ,
, 
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Treatment
2.3. Histopathological Classification
2.4. Statistical Analysis
3. Results
3.1. Follow-Up and Patient Characteristics
3.2. Treatment Characteristics
3.3. Univariate Analysis of LRFS
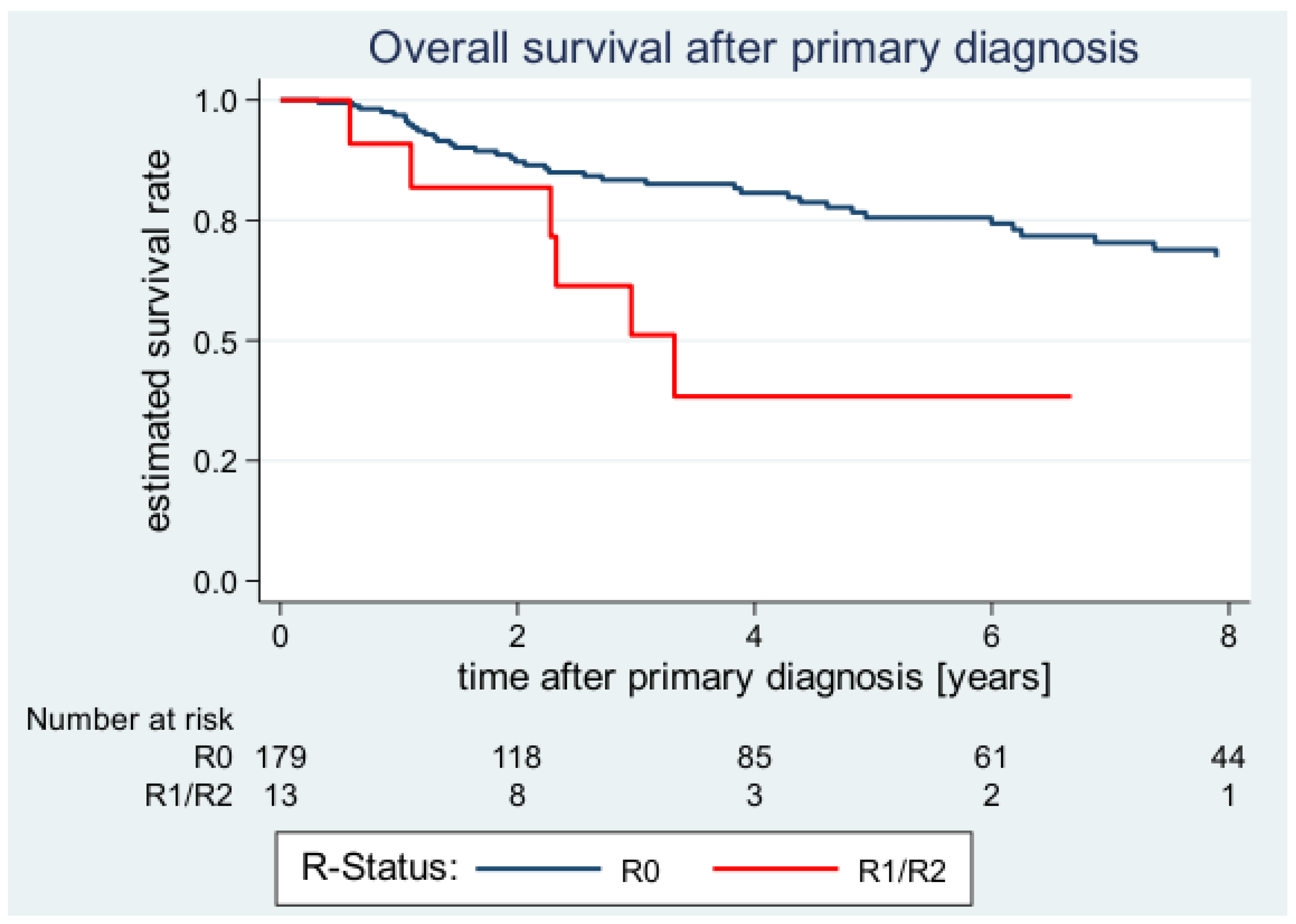
3.4. Univariate Analysis of OS
3.5. Multivariate Analysis of LRFS
3.6. Multivariate Analysis of OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Saltus, C.W.; Calingaert, B.; Candrilli, S.; Lorenzo, M.; D’Yachkova, Y.; Otto, T.; Wagner, U.; Kaye, J.A. Epidemiology of Adult Soft-Tissue Sarcomas in Germany. Sarcoma 2018, 2018, 5671926. [Google Scholar] [CrossRef]
- Jemal, A.; Siegel, R.; Ward, E.; Murray, T.; Xu, J.; Thun, M.J. Cancer statistics, 2007. CA Cancer J. Clin. 2007, 57, 43–66. [Google Scholar] [CrossRef]
- Katz, D.; Palmerini, E.; Pollack, S.M. More Than 50 Subtypes of Soft Tissue Sarcoma: Paving the Path for Histology-Driven Treatments. ASCO 2018, 38, 925–938. [Google Scholar] [CrossRef]
- Brennan, M.F.; Antonescu, C.R.; Moraco, N.; Singer, S. Lessons learned from the study of 10,000 patients with soft tissue sarcoma. Ann. Surg. 2014, 260, 416–421. [Google Scholar] [CrossRef]
- Dineen, S.P.; Roland, C.L.; Feig, R.; May, C.; Zhou, S.; Demicco, E.; Sannaa, G.A.; Ingram, D.; Wang, W.L.; Ravi, V.; et al. Radiation-Associated Undifferentiated Pleomorphic Sarcoma is Associated with Worse Clinical Outcomes than Sporadic Lesions. Ann. Surg. Oncol. 2015, 22, 3913–3920. [Google Scholar] [CrossRef]
- Lazar, A.J.; McLellan, M.D.; Bailey, M.H.; Miller, C.A.; Appelbaum, E.L.; Cordes, M.G.; Fronick, C.C.; Fulton, L.A.; Fulton, R.S.; Mardis, E.R.; et al. Comprehensive and Integrated Genomic Characterization of Adult Soft Tissue Sarcomas. Cell 2017, 171, 950–965. [Google Scholar] [CrossRef]
- Taylor, B.S.; Barretina, J.; Maki, R.G.; Antonescu, C.R.; Singer, S.; Ladanyi, M. Advances in sarcoma genomics and new therapeutic targets. Nat. Rev. Cancer 2011, 11, 541–557. [Google Scholar] [CrossRef]
- Barretina, J.; Taylor, B.S.; Banerji, S.; Ramos, A.H.; Lagos-Quintana, M.; Decarolis, P.L.; Shah, K.; Socci, N.D.; Weir, B.A.; Ho, A.; et al. Subtype-specific genomic alterations define new targets for soft-tissue sarcoma therapy. Nat. Genet. 2010, 42, 715–721. [Google Scholar] [CrossRef]
- Helias-Rodzewicz, Z.; Perot, G.; Chibon, F.; Ferreira, C.; Lagarde, P.; Terrier, P.; Coindre, J.M.; Aurias, A. YAP1 and VGLL3, encoding two cofactors of TEAD transcription factors, are amplified and overexpressed in a subset of soft tissue sarcomas. Genes Chromosome Cancer 2010, 49, 1161–1171. [Google Scholar] [CrossRef]
- Kakiuchi-Kiyota, S.; Schutten, M.M.; Zhong, Y.; Crawford, J.J.; Dey, A. Safety Considerations in the Development of Hippo Pathway Inhibitors in Cancers. Front. Cell Dev. Biol. 2019, 7, 156. [Google Scholar] [CrossRef]
- Kawaguchi, K.; Igarashi, K.; Kiyuna, T.; Miyake, K.; Miyake, M.; Murakami, T.; Chmielowski, B.; Nelson, S.D.; Russell, T.A.; Dry, S.M.; et al. Individualized doxorubicin sensitivity testing of undifferentiated soft tissue sarcoma (USTS) in a patient-derived orthotopic xenograft (PDOX) model demonstrates large differences between patients. Cell Cycle 2018, 17, 627–633. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): A multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef]
- Stojadinovic, A.; Leung, D.H.; Hoos, A.; Jaques, D.P.; Lewis, J.J.; Brennan, M.F. Analysis of the prognostic significance of microscopic margins in 2084 localized primary adult soft tissue sarcomas. Ann. Surg. 2002, 235, 424–434. [Google Scholar] [CrossRef]
- Zagars, G.K.; Ballo, M.T.; Pisters, P.W.; Pollock, R.E.; Patel, S.R.; Benjamin, R.S.; Evans, H.L. Prognostic factors for patients with localized soft-tissue sarcoma treated with conservation surgery and radiation therapy: An analysis of 1225 patients. Cancer 2003, 97, 2530–2543. [Google Scholar] [CrossRef]
- Lehnhardt, M.; Daigeler, A.; Homann, H.H.; Schwaiberger, V.; Goertz, O.; Kuhnen, C.; Steinau, H.U. MFH revisited: Outcome after surgical treatment of undifferentiated pleomorphic or not otherwise specified (NOS) sarcomas of the extremities—An analysis of 140 patients. Langenbecks Arch. Surg. 2009, 394, 313–320. [Google Scholar] [CrossRef]
- Callegaro, D.; Miceli, R.; Bonvalot, S.; Ferguson, P.; Strauss, D.C.; Levy, A.; Griffin, A.; Hayes, A.J.; Stacchiotti, S.; Pechoux, C.L.; et al. Development and external validation of two nomograms to predict overall survival and occurrence of distant metastases in adults after surgical resection of localised soft-tissue sarcomas of the extremities: A retrospective analysis. Lancet Oncol. 2016, 17, 671–680. [Google Scholar] [CrossRef]
- Pisters, P.W.; Leung, D.H.; Woodruff, J.; Shi, W.; Brennan, M.F. Analysis of prognostic factors in 1041 patients with localized soft tissue sarcomas of the extremities. J. Clin. Oncol. 1996, 14, 1679–1689. [Google Scholar] [CrossRef]
- Vodanovich, D.A.; Spelman, T.; May, D.; Slavin, J.; Choong, P.F.M. Predicting the prognosis of undifferentiated pleomorphic soft tissue sarcoma: A 20-year experience of 266 cases. ANZ J. Surg. 2019. [Google Scholar] [CrossRef]
- Kamat, N.V.; Million, L.; Yao, D.H.; Donaldson, S.S.; Mohler, D.G.; van de Rijn, M.; Avedian, R.S.; Kapp, D.S.; Ganjoo, K.N. The Outcome of Patients with Localized Undifferentiated Pleomorphic Sarcoma of the Lower Extremity Treated at Stanford University. Am. J. Clin. Oncol. 2019, 42, 166–171. [Google Scholar] [CrossRef]
- Vasileios, K.A.; Eward, W.C.; Brigman, B.E. Surgical treatment and prognosis in patients with high-grade soft tissue malignant fibrous histiocytoma of the extremities. Arch. Orthop. Trauma Surg. 2012, 132, 955–961. [Google Scholar] [CrossRef]
- Le Doussal, V.; Coindre, J.M.; Leroux, A.; Hacene, K.; Terrier, P.; Bui, N.B.; Bonichon, F.; Collin, F.; Mandard, A.M.; Contesso, G. Prognostic factors for patients with localized primary malignant fibrous histiocytoma: A multicenter study of 216 patients with multivariate analysis. Cancer 1996, 77, 1823–1830. [Google Scholar] [CrossRef]
- Coindre, J.M. Grading of soft tissue sarcomas: Review and update. Arch. Pathol. Lab. Med. 2006, 130, 1448–1453. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D. The evolving classification of soft tissue tumours–An update based on the new 2013 WHO classification. Histopathology 2014, 64, 2–11. [Google Scholar] [CrossRef]
- Harati, K.; Kolbenschlag, J.; Bohm, J.; Niggemann, H.; Joneidi-Jafari, H.; Stricker, I.; Lehnhardt, M.; Daigeler, A. Long-term outcomes of patients with soft tissue sarcoma of the chest wall: Analysis of the prognostic significance of microscopic margins. Oncol. Lett. 2018, 15, 2179–2187. [Google Scholar] [CrossRef]
- Harati, K.; Goertz, O.; Pieper, A.; Daigeler, A.; Joneidi-Jafari, H.; Niggemann, H.; Stricker, I.; Lehnhardt, M. Soft Tissue Sarcomas of the Extremities: Surgical Margins Can Be Close as Long as the Resected Tumor Has No Ink on It. Oncologist 2017. [Google Scholar] [CrossRef]
- Harati, K.; Daigeler, A.; Goertz, O.; Bohm, J.; Lange, K.; Stricker, I.; Kolbenschlag, J.; Lehnhardt, M. Primary and Secondary Soft Tissue Angiosarcomas: Prognostic Significance of Surgical Margins in 43 Patients. Anticancer Res. 2016, 36, 4321–4328. [Google Scholar]
- Lehnhardt, M.; Bohm, J.; Hirsch, T.; Behr, B.; Daigeler, A.; Harati, K. Radiation-induced angiosarcoma of the breast. HaMiPla 2017, 49, 103–110. [Google Scholar] [CrossRef]
- Harati, K.; Lange, K.; Goertz, O.; Lahmer, A.; Kapalschinski, N.; Stricker, I.; Lehnhardt, M.; Daigeler, A. A single-institutional review of 68 patients with dermatofibrosarcoma protuberans: Wide re-excision after inadequate previous surgery results in a high rate of local control. World J. Surg. Oncol. 2017, 15, 5. [Google Scholar] [CrossRef]
- Beane, J.D.; Yang, J.C.; White, D.; Steinberg, S.M.; Rosenberg, S.A.; Rudloff, U. Efficacy of adjuvant radiation therapy in the treatment of soft tissue sarcoma of the extremity: 20-year follow-up of a randomized prospective trial. Ann. Surg. Oncol. 2014, 21, 2484–2489. [Google Scholar] [CrossRef]
- Koshy, M.; Rich, S.E.; Mohiuddin, M.M. Improved survival with radiation therapy in high-grade soft tissue sarcomas of the extremities: A SEER analysis. IJROBP 2010, 77, 203–209. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | N | % of Total |
|---|---|---|
| Total | 192 | |
| Age (years) | ||
| ≤60 | 72 | 37.5 |
| >60 | 120 | 62.5 |
| Sex | ||
| Female | 86 | 44.8 |
| Male | 106 | 55.2 |
| Tumor size | ||
| ≤5 cm | 69 | 36.0 |
| >5 cm | 123 | 64.0 |
| Tumor depth | ||
| Epifascial | 47 | 24.5 |
| Subfascial | 145 | 75.5 |
| Tumor site | ||
| Upper extremity | 66 | 34.4 |
| Lower extremity | 126 | 65.6 |
| Grading | ||
| G1 | 8 | 4.2 |
| G2 | 69 | 35.9 |
| G3 | 115 | 59.9 |
| Margin status (Primary tumor) | ||
| R0 | 179 | 93.2 |
| R1 | 11 | 5.7 |
| R2 | 2 | 1.0 |
| Adjuvant radiotherapy (Primary tumor) | ||
| No | 89 | 46.4 |
| Yes | 103 | 53.6 |
| Neoadjuvant radiotherapy (Primary tumor) | ||
| No | 180 | 93.8 |
| Yes | 12 | 6.2 |
| Adjuvant chemotherapy (Primary tumor) | ||
| No | 180 | 93.8 |
| Yes | 12 | 6.2 |
| Neoadjuvant chemotherapy (Primary tumor) | ||
| No | 188 | 97.9 |
| Yes | 4 | 2.1 |
| Status | ||
| No evidence of disease | 119 | 62.0 |
| Alive with local recurrent disease | 11 | 5.7 |
| Alive with distant metastases | 13 | 6.8 |
| Died due to UPS | 37 | 19.3 |
| Died due to other causes | 12 | 6.3 |
| Characteristic | N | No. of Local Recurrence | 1-Year LRFS (95%-CI) | 2-Year LRFS (95%-CI) | 5-Year LRFS (95%-CI) | p (Log-Rank) |
|---|---|---|---|---|---|---|
| All patients | 192 | 68 | 84.4 (78.1–89.0) | 74.1 (66.5–80.2) | 58.2 (49.3–66.0) | |
| Age (years) | ||||||
| ≤60 | 72 | 25 | 90.8 (80.7–95.8) | 72.0 (58.7–81.6) | 62.4 (48.4–73.5) | |
| >60 | 120 | 43 | 80.5 (71.6–86.8) | 76.0 (66.4–83.1) | 55.3 (43.4–65.7) | 0.371 |
| Sex | ||||||
| Female | 86 | 27 | 88.2 (78.5–93.7) | 81.9 (70.8–89.1) | 63.3 (49.6–74.2) | |
| Male | 106 | 41 | 81.5 (72.3–88.0) | 67.9 (57.0–76.6) | 53.9 (41.9–64.5) | 0.194 |
| Tumor size | ||||||
| ≤5 cm | 69 | 22 | 84.0 (72.3–91.1) | 75.4 (62.5–84.4) | 70.0 (56.6–80.0) | |
| >5 cm | 123 | 46 | 84.6 (76.3–90.1) | 72.9 (62.8–80.7) | 49.0 (37.1–59.8) | 0.141 |
| Tumor depth | ||||||
| Epifascial | 47 | 17 | 86.6 (72.6–93.8) | 76.5 (60.7–86.7) | 65.4 (48.3–78.0) | |
| Subfascial | 145 | 51 | 83.6 (75.9–89.0) | 73.2 (64.1–80.3) | 55.5 (44.9–64.8) | 0.708 |
| Tumor site | ||||||
| Upper extremity | 66 | 31 | 84.3 (72.8–91.2) | 73.6 (60.4–83.0) | 49.8 (35.1–62.8) | |
| Lower extremity | 126 | 37 | 84.4 (76.1–90.0) | 74.3 (64.5–81.8) | 63.6 (52.6–72.7) | 0.169 |
| Grading | ||||||
| G1 | 8 | 4 | 87.5 (38.7–98.1) | 87.5 (38.7–98.1) | 72.9 (27.6–92.5) | |
| G2 | 69 | 31 | 84.8 (73.5–91.5) | 74.7 (62.1–83.7) | 55.0 (41.3–66.7) | |
| G3 | 115 | 33 | 83.9 (75.0–89.8) | 72.6 (62.0–80.7) | 60.4 (47.9–70.8) | 0.799 * |
| Margin status (Primary tumor) | ||||||
| R0 | 179 | 61 | 85.9 (79.5–90.4) | 75.7 (67.9–81.8) | 60.9 (51.8–68.7) | |
| R1/R2 | 13 | 7 | 61.4 (26.6–83.5) | 49.1 (16.7–75.3) | (–) | 0.013 |
| Negative margin width | ||||||
| ≤1 mm | 88 | 26 | 90.2 (81.3–95.0) | 78.2 (66.7–86.1) | 64.1 (50.2–75.0) | |
| >1 mm and ≤5 mm | 36 | 5 | 96.3 (76.5–99.5) | 86.9 (64.3–95.6) | 76.6 (52.1–89.7) | |
| >5 mm | 16 | 5 | 75.0 (46.3–89.8) | 75.0 (46.3–89.8) | 68.2 (39.5–85.4) | 0.272 * |
| Adjuvant radiotherapy (Primary tumor) | ||||||
| No | 89 | 44 | 79.3 (68.8–86.6) | 66.5 (54.7–75.9) | 48.4 (36.0–59.7) | |
| Yes | 103 | 24 | 89.0 (80.5–93.9) | 81.1 (70.8–88.0) | 67.6 (55.0–77.3) | <0.001 |
| Neoadjuvant radiotherapy (Primary tumor) | ||||||
| No | 180 | 63 | 83.9 (77.2–88.7) | 74.9 (67.1–81.1) | 58.3 (49.1–66.5) | |
| Yes | 12 | 5 | 91.7 (53.9–98.8) | 66.7 (33.7–86.0) | 57.1 (25.4–79.6) | 0.953 |
| Adjuvant chemotherapy (Primary tumor) | ||||||
| No | 180 | 62 | 80.5 (68.2–88.5) | 71.1 (57.6–81.0) | 63.2 (48.1–75.0) | |
| Yes | 12 | 6 | 86.3 (78.3–91.5) | 75.3 (65.5–82.7) | 56.0 (44.7–65.8) | 0.656 |
| Neoadjuvant chemotherapy (Primary tumor) | ||||||
| No | 188 | 66 | 84.0 (77.6–88.8) | 74.1 (66.4–80.3) | 58.4 (49.4–66.4) | |
| Yes | 4 | 2 | 100 (–) | 75.0 (12.8–96.1) | 50.0 (5.8–84.5) | - |
| Characteristic | N | No. of Deaths | 1-Year OS (95%-CI) | 2-Year OS (95%-CI) | 5-Year OS (95%-CI) | P (Log-Rank) |
|---|---|---|---|---|---|---|
| All patients | 192 | 50 | 96.5 (92.4–98.4) | 86.8 (80.5–91.2) | 73.0 (64.5–79.7) | |
| Age (years) | ||||||
| ≤60 | 72 | 16 | 100 (–) | 91.2 (80.1–96.3) | 79.9 (65.4–88.8) | |
| >60 | 120 | 34 | 94.4 (87.9–97.4) | 84.1 (75.4–90.0) | 69.0 (57.9–77.6) | 0.192 |
| Sex | ||||||
| Female | 86 | 20 | 100 (–) | 92.5 (82.9–96.8) | 71.9 (57.9–81.9) | |
| Male | 106 | 30 | 93.9 (86.9–97.2) | 82.5 (72.9–88.9) | 74.1 (63.1–82.3) | 0.274 |
| Tumor size | ||||||
| ≤5 cm | 69 | 11 | 98.5 (89.6–99.8) | 93.4 (83.2–97.5) | 89.1 (77.0–95.0) | |
| >5 cm | 123 | 39 | 95.4 (89.2–98.0) | 82.9 (73.8–89.0) | 62.6 (50.9–72.2) | 0.002 |
| Tumor depth | ||||||
| Epifascial | 47 | 5 | 100 (–) | 97.5 (83.5–99.6) | 91.7 (76.3–97.3) | |
| Subfascial | 145 | 45 | 95.3 (89.8–97.8) | 83.0 (74.9–88.7) | 66.1 (55.6–74.6) | 0.003 |
| Tumor site | ||||||
| Upper extremity | 66 | 20 | 96.7 (87.4–99.2) | 86.4 (74.6–93.0) | 69.9 (55.2–80.6) | |
| Lower extremity | 126 | 30 | 96.4 (90.8–98.6) | 87.1 (78.7–92.3) | 75.0 (64.1–82.9) | 0.561 |
| Grading | ||||||
| G1 | 8 | 4 | 100 (–) | 87.5 (38.7–98.1) | 60.0 (19.5–85.2) | |
| G2 | 69 | 14 | 100 (–) | 100 (–) | 82.9 (68.7–91.1) | |
| G3 | 115 | 32 | 93.9 (86.9–97.2) | 77.8 (67.6–85.1) | 67.9 (56.4–76.9) | 0.017 * |
| Margin status (Primary tumor) | ||||||
| R0 | 179 | 44 | 96.9 (92.6–98.7) | 87.2 (80.6–91.6) | 75.5 (66.9–82.2) | |
| R1/R2 | 13 | 6 | 90.9 (50.8–98.7) | 81.8 (44.7–95.1) | 38.4 (10.3–66.8) | 0.001 |
| Negative margin width | ||||||
| ≤1 mm | 88 | 22 | 96.3 (89.1–98.8) | 84.0 (73.5–90.6) | 76.8 (64.6–85.3) | |
| >1 mm and ≤5 mm | 36 | 4 | 93.2 (75.4–98.3) | 89.6 (71.1–96.5) | 83.2 (59.4–93.7) | |
| >5 mm | 16 | 1 | 100 (–) | 100 (–) | 92.3 (56.6–98.9) | 0.070 * |
| Adjuvant radiotherapy (Primary tumor) | ||||||
| No | 89 | 31 | 96.3 (88.9–98.8) | 81.7 (71.0–88.8) | 61.8 (48.2–72.8) | |
| Yes | 103 | 19 | 96.7 (90.2–98.9) | 91.7 (83.3–96.0) | 82.8 (72.1–89.8) | 0.016 |
| Neoadjuvant radiotherapy (Primary tumor) | ||||||
| No | 180 | 46 | 96.2 (91.8–98.3) | 86.5 (79.8–91.1) | 73.8 (65.0–80.7) | |
| Yes | 12 | 4 | 100 (–) | 91.7 (53.9–98.8) | 66.7 (33.7–86.0) | 0.997 |
| Adjuvant chemotherapy (Primary tumor) | ||||||
| No | 180 | 43 | 96.4 (90.7–98.6) | 86.6 (78.3–91.8) | 73.9 (63.3–81.8) | |
| Yes | 12 | 7 | 96.7 (87.4–99.2) | 87.4 (75.3–93.8) | 72.0 (56.7–82.7) | 0.885 |
| Neoadjuvant chemotherapy (Primary tumor) | ||||||
| No | 188 | 48 | 96.4 (92.2–98.4) | 87.2 (80.8–91.5) | 73.8 (65.2–80.5) | |
| Yes | 4 | 2 | 100 (–) | 75.0 (12.8–96.1) | 50.0 (5.8–84.5) | - |
| Category (Reference) | LRFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Depth: subfascial (vs. epifascial) | - | - | 4.65 (1.77–12.16) | 0.002 |
| Size: >5 cm (vs. ≤5 cm) | - | - | 1.63 (0.73–3.63) | 0.230 |
| Grade: G3 (vs. G1) | - | - | 2.65 (1.45–4.83) | 0.001 |
| Margin status: R1/R2 (vs. R0) | 3.08 (1.48–6.39) | 0.003 | 3.13 (1.54–6.38) | 0.002 |
| Adjuvant radiation: Yes (vs. no) | 0.41 (0.25–0.67) | <0.001 | 0.50 (0.28–0.89) | 0.019 |
| Sex: Male (vs. female) | 1.41 (0.86–2.33) | 0.175 | 1.04 (0.53–2.02) | 0.916 |
| Age: >60 (vs. ≤60) | 1.23 (0.76–2.00) | 0.396 | 2.32 (1.21–4.44) | 0.011 |
| Author (Year) | N | Site | Median FU (Years) | 5-LRFS (%) | 5-OS (%) | Independent Prognostic Effect of Microscopic Margins on | Independent Prognostic Effect of Adjuvant Radiotherapy on | ||
|---|---|---|---|---|---|---|---|---|---|
| LRFS | OS/DSS | LRFS | OS/DSS | ||||||
| Present study | 192 | Extremity | 5.1 | 58 | 73 | + | + | + | + |
| Kamat (2019) | 55 | Lower Extremity | 4.5 | 60 | 68 | − | + | + | − |
| Vasileios (2012) | 61 | Extremity | 4.3 | NA | 67 | − | − | − | − |
| Dineen (2015) | 148 a | Extremity, Trunk, Head/Neck | NA | 75 | 76 b | + | − | − | − |
| Vodanovich (2018) | 266 | Extremity, Trunk, Head/Neck | 7.0 | 85 | 60 | + | − | − | − |
| Le Doussal (1996) | 216 | Extremity, Trunk, Head/Neck | 3.5 | 63 | 70 b | − | − | + | − |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goertz, O.; Pieper, A.; von der Lohe, L.; Stricker, I.; Dadras, M.; Behr, B.; Lehnhardt, M.; Harati, K. The Impact of Surgical Margins and Adjuvant Radiotherapy in Patients with Undifferentiated Pleomorphic Sarcomas of the Extremities: A Single-Institutional Analysis of 192 Patients. Cancers 2020, 12, 362. https://doi.org/10.3390/cancers12020362
Goertz O, Pieper A, von der Lohe L, Stricker I, Dadras M, Behr B, Lehnhardt M, Harati K. The Impact of Surgical Margins and Adjuvant Radiotherapy in Patients with Undifferentiated Pleomorphic Sarcomas of the Extremities: A Single-Institutional Analysis of 192 Patients. Cancers. 2020; 12(2):362. https://doi.org/10.3390/cancers12020362
Chicago/Turabian StyleGoertz, Ole, Andreas Pieper, Leon von der Lohe, Ingo Stricker, Mehran Dadras, Björn Behr, Marcus Lehnhardt, and Kamran Harati. 2020. "The Impact of Surgical Margins and Adjuvant Radiotherapy in Patients with Undifferentiated Pleomorphic Sarcomas of the Extremities: A Single-Institutional Analysis of 192 Patients" Cancers 12, no. 2: 362. https://doi.org/10.3390/cancers12020362
APA StyleGoertz, O., Pieper, A., von der Lohe, L., Stricker, I., Dadras, M., Behr, B., Lehnhardt, M., & Harati, K. (2020). The Impact of Surgical Margins and Adjuvant Radiotherapy in Patients with Undifferentiated Pleomorphic Sarcomas of the Extremities: A Single-Institutional Analysis of 192 Patients. Cancers, 12(2), 362. https://doi.org/10.3390/cancers12020362