Inflammation Is a Mediating Factor in the Association between Lifestyle and Fatigue in Colorectal Cancer Patients

 , , , , , ,
, , , , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
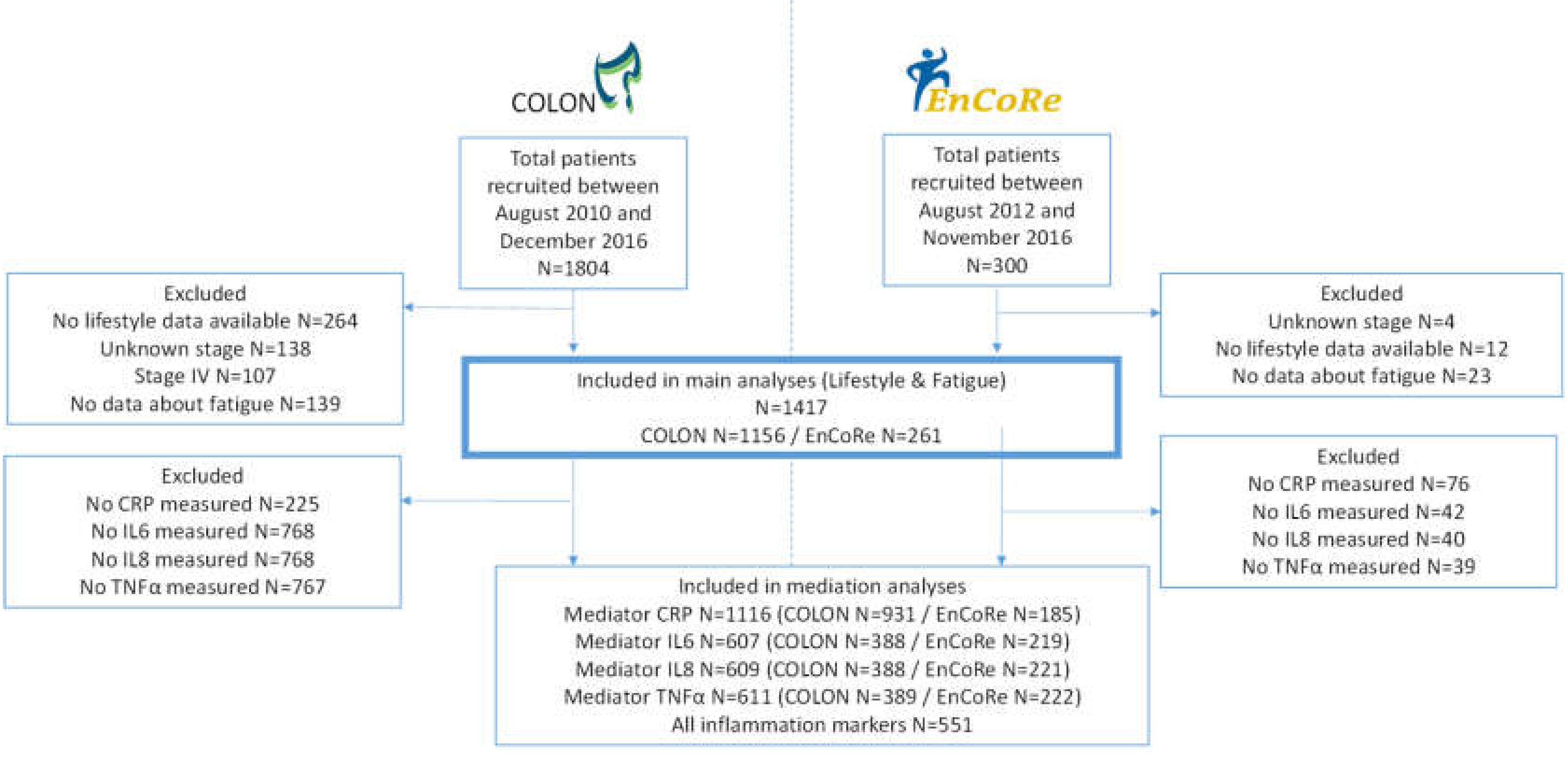
4.1. Study Population
4.2. WCRF/AICR Score
4.3. Fatigue
4.4. Blood Collection and Inflammatory Markers
4.5. Covariates
4.6. Data Analysis
4.7. Mediation Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bower, J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef]
- Lawrence, D.P.; Kupelnick, B.; Miller, K.; Devine, D.; Lau, J. Evidence Report on the Occurrence, Assessment, and Treatment of Fatigue in Cancer Patients. J. Natl. Cancer Inst. Monogr. 2004, 2004, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.A. Cancer-Related Fatigue: State of the Science. PM&R 2010, 2, 364–383. [Google Scholar]
- Aapro, M.; Scotte, F.; Bouillet, T.; Currow, D.; Vigano, A. A Practical Approach to Fatigue Management in Colorectal Cancer. Clin. Colorectal Cancer 2017, 16, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vissers, P.A.J.; Thong, M.S.Y.; Pouwer, F.; Zanders, M.M.J.; Coebergh, J.W.W.; Van De Poll-Franse, L.V. The impact of comorbidity on Health-Related Quality of Life among cancer survivors: Analyses of data from the PROFILES registry. J. Cancer Surviv. 2013, 7, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Mustian, K.M.; Alfano, C.M.; Heckler, C.; Kleckner, A.S.; Kleckner, I.R.; Leach, C.R.; Mohr, D.; Palesh, O.G.; Peppone, L.J.; Piper, B.F.; et al. Comparison of pharmaceutical, psychological, and exercise treatments for cancer-related fatigue: A meta-analysis. JAMA Oncol. 2017, 3, 961. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.-Y.; Ho, S.C.; Cheng, A.; Kwok, C.; Lee, C.-K.I.; Cheung, K.L.; Lee, R.; Loong, H.H.-F.; He, Y.-Q.; Yeo, W. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Guideline Is Associated With Better Health-Related Quality of Life Among Chinese Patients With Breast Cancer. J. Natl. Compr. Cancer Netw. 2018, 16, 275. [Google Scholar] [CrossRef] [PubMed]
- Breedveld-Peters, J.J.L.; Koole, J.L.; Müller-Schulte, E.; Van Der Linden, B.W.A.; Windhausen, C.; Bours, M.J.L.; Van Roekel, E.H.; Weijenberg, M.P. Colorectal cancers survivors’ adherence to lifestyle recommendations and cross-sectional associations with health-related quality of life. Br. J. Nutr. 2018, 120, 188. [Google Scholar] [CrossRef]
- Van Veen, M.R.; Mols, F.; Bours, M.J.L.; Weijenberg, M.P.; Kampman, E.; Beijer, S. Adherence to the World Cancer Research Fund/American Institute for Cancer Research recommendations for cancer prevention is associated with better health–related quality of life among long-term colorectal cancer survivors: Results of the PROFILES registry. Support. Care Cancer 2019, 27, 4565. [Google Scholar] [CrossRef] [Green Version]
- Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients 2019, 11, 1572. [Google Scholar] [CrossRef] [Green Version]
- Baguley, B.J.; Bolam, K.A.; Wright, O.; Skinner, T.L. The Effect of Nutrition Therapy and Exercise on Cancer-Related Fatigue and Quality of Life in Men with Prostate Cancer: A Systematic Review. Nutrients 2017, 9, 1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meneses-Echavez, J.F.; Correa-Bautista, J.E.; González-Jiménez, E.; Schmidt-RioValle, J.; Elkins, M.R.; Lobelo, F.; Ramírez-Vélez, R. The Effect of Exercise Training on Mediators of Inflammation in Breast Cancer Survivors: A Systematic Review with Meta-analysis. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Himbert, C.; Ose, J.; Lin, T.; Warby, C.A.; Gigic, B.; Steindorf, K.; Schrotz-King, P.; Abbenhardt-Martin, C.; Zielske, L.; Boehm, J.; et al. Inflammation- and angiogenesis-related biomarkers are correlated with cancer-related fatigue in colorectal cancer patients: Results from the ColoCare Study. Eur. J. Cancer Care 2019, 28, e13055. [Google Scholar] [CrossRef] [PubMed]
- Kessels, E.; Husson, O.; Feltz-Cornelis, C.M.V.D. The effect of exercise on cancer-related fatigue in cancer survivors: A systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 2018, 14, 479. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.E.; Chang-Claude, J.; Seibold, P.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Steindorf, K. Determinants of long-term fatigue in breast cancer survivors: Results of a prospective patient cohort study. Psycho-Oncology 2015, 24, 40–46. [Google Scholar] [CrossRef]
- Courneya, K.S.; Karvinen, K.H.; Campbell, K.L.; Pearcey, R.G.; Dundas, G.; Capstick, V.; Tonkin, K.S. Associations among exercise, body weight, and quality of life in a population-based sample of endometrial cancer survivors. Gynecol. Oncol. 2005, 97, 422–430. [Google Scholar] [CrossRef]
- Oldenburg, C.S.; Boll, D.; Nicolaije, K.A.; Vos, M.C.; Pijnenborg, J.M.; Coebergh, J.W.; Beijer, S.; Poll-Franse, L.V.V.D.; Ezendam, N.P. The relationship of body mass index with quality of life among endometrial cancer survivors: A study from the population-based PROFILES registry. Gynecol. Oncol. 2013, 129, 216–221. [Google Scholar] [CrossRef]
- Smits, A.; Lopes, A.; Das, N.; Bekkers, R.; Galaal, K. The impact of BMI on quality of life in obese endometrial cancer survivors: Does size matter? Gynecol. Oncol. 2014, 132, 137–141. [Google Scholar] [CrossRef]
- Basen-Engquist, K.M.; Scruggs, S.; Jhingran, A.; Bodurka, D.C.; Lu, K.; Ramondetta, L.; Hughes, D.; Taylor, C.C. Physical activity and obesity in endometrial cancer survivors: Associations with pain, fatigue, and physical functioning. Am. J. Obstet. Gynecol. 2009, 200, e1–e8. [Google Scholar] [CrossRef] [Green Version]
- Baguley, B.J.; Skinner, T.L.; Wright, O.R.L. Nutrition therapy for the management of cancer-related fatigue and quality of life: A systematic review and meta-analysis. Br. J. Nutr. 2019, 122, 527. [Google Scholar] [CrossRef]
- LaVoy, E.C.; Fagundes, C.P.; Dantzer, R. Exercise, inflammation, and fatigue in cancer survivors. Exerc. Immunol. Rev. 2016, 22, 82. [Google Scholar] [PubMed]
- Ibrahim, M.M. Subcutaneous and visceral adipose tissue: Structural and functional differences. Obes. Rev. 2010, 11, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Bruun, J.M.; Lihn, A.S.; Madan, A.K.; Pedersen, S.B.; Schiøtt, K.M.; Fain, J.N.; Richelsen, B. Higher production of IL-8 in visceral vs. subcutaneous adipose tissue. Implication of nonadipose cells in adipose tissue. Am. J. Physiol. Endocrinol. Metab. 2004, 286, E8–E13. [Google Scholar] [CrossRef] [PubMed]
- Galland, L. Diet and Inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- Zick, S.M.; Colacino, J.A.; Cornellier, M.; Khabir, T.; Surnow, K.; Djuric, Z. Fatigue reduction diet in breast cancer survivors: A pilot randomized clinical trial. Breast Cancer Res. Treat. 2017, 161, 299. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process. Analysis Second Edition: A Regression-Based Approach; Ebook The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Turnes, P.B.; Ernst, R. The Use of Longitudinal Mediation Models for Testing Causal Effects and Measuring Direct and Indirect Effects. China USA Bus. Rev. 2016, 15, 1. [Google Scholar]
- Bower, J.E.; Ganz, P.A.; Irwin, M.R.; Arevalo, J.M.; Cole, S.W. Fatigue and gene expression in human leukocytes: Increased NF-κB and decreased glucocorticoid signaling in breast cancer survivors with persistent fatigue. Brain Behav. Immun. 2011, 25, 147–150. [Google Scholar] [CrossRef] [Green Version]
- Karshikoff, B.; Sundelin, T.; Lasselin, J. Role of Inflammation in Human Fatigue: Relevance of Multidimensional Assessments and Potential Neuronal Mechanisms. Front. Immunol. 2017, 8, 21. [Google Scholar] [CrossRef] [Green Version]
- Lacourt, T.E.; Vichaya, E.G.; Chiu, G.S.; Dantzer, R.; Heijnen, C.J. The High Costs of Low-Grade Inflammation: Persistent Fatigue as a Consequence of Reduced Cellular-Energy Availability and Non-adaptive Energy Expenditure. Front. Behav. Neurosci. 2018, 12, 78. [Google Scholar] [CrossRef] [Green Version]
- Winkels, R.M.; Heine-Bröring, R.C.; Van Zutphen, M.; Van Harten-Gerritsen, S.; Kok, D.E.; Van Duijnhoven, F.J.; Kampman, E. The COLON study: Colorectal cancer: Longitudinal, Observational study on Nutritional and lifestyle factors that may influence colorectal tumour recurrence, survival and quality of life. BMC Cancer 2014, 14, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Roekel, E.H.; Bours, M.J.L.; De Brouwer, C.P.M.; Napel, H.T.; Sanduleanu, S.; Beets, G.L.; Kant, I.J.; Weijenberg, M.P. The Applicability of the International Classification of Functioning, Disability, and Health to Study Lifestyle and Quality of Life of Colorectal Cancer Survivors. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1394–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund; American Institute for Cancer Research. Recommendations and Public Health and Policy Implications; Continuous Update Project Report 2018; World Cancer Research Fund: London, UK, 2018. [Google Scholar]
- Feunekes, I.J.; Van Staveren, W.A.; Graveland, F.; De Vos, J.; Burema, J. Reproducibility of a semiquantitative food frequency questionnaire to assess the intake of fats and cholesterol in The Netherlands. Int. J. Food Sci. Nutr. 1995, 46, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Verkleij-Hagoort, A.C.; De Vries, J.H.M.; Stegers, M.P.G.; Lindemans, J.; Ursem, N.T.C.; Steegers-Theunissen, R.P.M. Validation of the assessment of folate and vitamin B12 intake in women of reproductive age: The method of triads. Eur. J. Clin. Nutr. 2006, 61, 610–615. [Google Scholar] [CrossRef] [Green Version]
- Koole, J.L.; Bours, M.J.; Breedveld-Peters, J.J.; van Roekel, E.H.; van Dongen, M.C.; Eussen, S.J.; Van Zutphenet, M.; van Duijnhoven, F.J.B.; Boshuizen, H.C.; Weijenberg, M.P. Evaluating the validity of a food frequency questionnaire in comparison with a 7-day dietary record for measuring dietary intake in a population of survivors of colorectal cancer. J. Acad. Nutr. Diet. 2020, 120, 245. [Google Scholar] [CrossRef]
- Dutch Nutrition Center. NEVO Nederlandse Voedingsmiddelen Tabel; (In Englisch: Dutch Food Composition Table); NEVO table: Bilthoven, The Netherlands, 2011. [Google Scholar]
- Wendel-Vos, G.C.W.; Schuit, A.J.; Saris, W.H.M.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Giesinger, J.M.; Kuijpers, W.; Young, T.; Tomaszewski, K.A.; Friend, E.; Zabernigg, A.; Holzner, B.; Aaronson, N.K. Thresholds for clinical importance for four key domains of the EORTC QLQ-C30: Physical functioning, emotional functioning, fatigue and pain. Health Qual. Life Outcomes 2016, 14, 1. [Google Scholar] [CrossRef] [Green Version]
- Wesselink, E.; Balvers, M.; Bours, M.J.L.; De Wilt, J.H.W.; Witkamp, R.F.; Van Baar, H.; Geijsen, A.J.M.R.; Van Halteren, H.; Keulen, E.T.P.; Kok, D.E.; et al. The association between circulating levels of vitamin D and inflammatory markers in the first 2 years after colorectal cancer diagnosis. Ther. Adv. Gastroenterol. 2020, 13. [Google Scholar] [CrossRef]
- De Jager, W.; Bourcier, K.; Rijkers, G.T.; Prakken, B.J.; Seyfert-Margolis, V. Prerequisites for cytokine measurements in clinical trials with multiplex immunoassays. BMC Immunol. 2009, 10, 52. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.; Ueland, P.M. Targeted Quantification of C-Reactive Protein and Cystatin C and Its Variants by Immuno-MALDI-MS. Anal. Chem. 2014, 86, 5807–5814. [Google Scholar] [CrossRef]
- Van Leersum, N.; Snijders, H.S.; Henneman, D.; Kolfschoten, N.; Gooiker, G.A.; Berge, M.G.T.; Eddes, E.H.; Wouters, M.W.J.M.; Tollenaar, R.A.E.M.; Bemelman, W.A.; et al. The Dutch Surgical Colorectal Audit. Eur. J. Surg. Oncol. EJSO 2013, 39, 1063–1070. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients Characteristics | Total Population (n = 1417) | Low WCRF/AICR-Score ≤3 (Tertile 1) (n = 548) | Medium WCRF/AICR-Score >3–3.75 (Tertile 2) (n = 485) | High WCRF/AICR-Score ≥3.75 (Tertile 3) (n = 384) |
|---|---|---|---|---|
| Age (years) | 66.1 (61.2–71.5) | 65.8 (60.4–71.2) | 66.5 (61.8–71.5) | 66.8 (61.4–72.0) |
| Sex (female) | 514 (36) | 175 (32) | 170 (35) | 169 (44) |
| Education level * | ||||
| low | 536 (38) | 215 (39) | 180 (37) | 141 (37) |
| medium | 412 (29) | 168 (31) | 147 (30) | 97 (25) |
| high | 467 (33) | 164 (30) | 157 (32) | 146 (38) |
| Smoking * | ||||
| current | 155 (11) | 60 (11) | 58 (12) | 37 (10) |
| former | 811 (58) | 322 (60) | 280 (58) | 209 (55) |
| never | 436 (31) | 155 (29) | 144 (30) | 137 (36) |
| BMI (kg/m2) * | 26.4 (24.2–29.4) | 28.4 (26.2–31.5) | 26.0 (24.1–28.4) | 24.3 (22.5–26.4) |
| Waist circumference (cm) | 97 (90–105) | 103 (96–110) | 95 (89–103) | 91 (83–97) |
| Total moderate-vigorous physical activity (hours/week) | 11.0 (5.5–19.0) | 8.5 (3.5–17.5) | 12 (7.0–20.3) | 13 (6.5–21.0) |
| Dietary intake | ||||
| Fruit and vegetable (g/day) | 260 (160–366) | 187 (121–298) | 260 (179–348) | 352 (244–447) |
| Total fibre (g/day) | 21 (17–26) | 19 (16–24) | 21 (17–25) | 23 (18–28) |
| Percentage of total kcal from ultra-processed foods | 28 (21–35) | 33 (26–39) | 27 (21–33) | 22 (18–28) |
| Processed meat (g/day) | 29 (13–46) | 37 (22–52) | 28 (15–46) | 14 (4–34) |
| Red meat (g/day) | 38 (23–56) | 44 (29–61) | 39 (23–56) | 31 (17–49) |
| Sugary drinks (g/day) | 72 (14–167) | 108 (32–245) | 67 (13–152) | 42 (0–131) |
| Alcohol (g/day) | 8 (1–21) | 12 (2–24) | 8 (1–19) | 5 (0–17) |
| Inflammation markers | ||||
| IL6 (pg/mL) | 1.0 (0.7–1.6) | 1.1 (0.7–1.7) | 0.9 (0.7–1.6) | 0.9 (0.6–1.4) |
| IL8 (pg/mL) | 5.6 (4.2–8.0) | 5.6 (4.1–7.9) | 5.8 (4.3–8.1) | 5.6 (4.3–8.0) |
| TNFα (pg/mL) | 2.0 (1.6–2.6) | 2.1 (1.7–2.6) | 2.0 (1.5–2.6) | 1.9 (1.5–2.4) |
| hsCRP (μg/mL) | 2.7 (1.2–6.5) | 3.1 (1.5–7.4) | 2.6 (1.2–5.9) | 2.2 (1.0–6.3) |
| Type of Cancer | ||||
| colon | 929 (66) | 357 (65) | 322 (67) | 250 (65) |
| rectal | 488 (34) | 191 (35) | 163 (33) | 134 (35) |
| Type of treatment * | ||||
| Surgery only | 756 (54) | 292 (55) | 248 (52) | 216 (57) |
| chemotherapy | 301 (22) | 117 (22) | 109 (23) | 75 (20) |
| radiotherapy | 224 (16) | 89 (17) | 72 (15) | 63 (16) |
| chemoradiation | 107 (8) | 34 (6) | 47 (10) | 26 (7) |
| Tumor stage | ||||
| I | 385 (27) | 141 (26) | 131 (27) | 113 (29) |
| II | 403 (28) | 149 (27) | 143 (29) | 111 (29) |
| III | 629 (44) | 258 (47) | 211 (44) | 160 (42) |
| Comorbidities (yes) * | 968 (69) | 389 (71) | 337 (70) | 242 (63) |
| Fatigue (yes) | 365 (26) | 157 (29) | 115 (24) | 93 (24) |
| Recurrence within one year (yes) | 81 (6) | 31 (6) | 25 (27) | 25 (7) |
| Daily use of NSAIDs (yes) | 110 (8) | 45 (8) | 37 (8) | 28 (7) |
| Cohort | ||||
| COLON | 1156 (82) | 421 (77) | 399 (82) | 336 (88) |
| EnCoRe | 261 (18) | 127 (23) | 86 (18) | 48 (13) |
| Inflammation 6 Months after Diagnosis | N | Crude Beta 95% CI | Adjusted * Beta 95% CI | |
|---|---|---|---|---|
| IL6 | ||||
| WCRF/AICR-score | 607 | −0.11 (−0.19; −0.04) | −0.10 (−0.17; −0.03) | |
| IL8 | ||||
| WCRF/AICR-score | 609 | −0.05 (−0.10; −0.00) | −0.05 (−0.09; 0.00) | |
| TNFα | ||||
| WCRF/AICR-score | 611 | −0.08 (−0.11; −0.05) | −0.07 (−0.10; −0.04) | |
| hsCRP | ||||
| WCRF/AICR-score | 1116 | −0.20 (−0.28; −0.13) | −0.20 (−0.28; −0.12) | |
| Fatigue after 6 Months | N | Crude Beta 95% CI | Adjusted * Beta 95% CI |
|---|---|---|---|
| IL6 | 607 | 5.49 (3.03; 7.95) | 5.05 (2.54; 7.57) |
| IL8 | 609 | 1.41 (−2.34; 5.15) | 1.62 (−2.07; 5.31) |
| TNFα | 611 | 1.01 (−4.50; 6.51) | 3.03 (−2.84; 8.90) |
| hsCRP | 1116 | 3.57 (2.30; 4.83) | 3.57 (2.37; 4.78) |
| Fatigue 6 Months after Diagnosis | N | Β (95%CI) | |
|---|---|---|---|
| IL6 | Total association | 607 | −2.17 (−4.44; 0.10) |
| Direct association | 607 | −1.69 (−3.95; 0.56) | |
| Indirect association | 607 | −0.48 (−1.05; −0.10) | |
| Proportion mediated * | 22% | ||
| IL8 | Total association | 609 | −2.19 (−4.45; 0.08) |
| Direct association | 609 | −2.12 (−4.39; 0.15) | |
| Indirect association | 609 | −0.06 (−0.31; 0.12) | |
| Proportion mediated * | 3% | ||
| TNFα | Total association | 611 | −2.19 (−4.45; 0.07) |
| Direct association | 611 | −2.05 (−4.35; 0.24) | |
| Indirect association | 611 | −0.14 (−0.69; 0.21) | |
| Proportion mediated * | 6% | ||
| hsCRP | Total association | 1116 | −2.11 (−3.74; −0.48) |
| Direct association | 1116 | −1.42 (−3.05; 0.21) | |
| Indirect association | 1116 | −0.68 (−1.10; −0.34) | |
| Proportion mediated * | 32% | ||
| Total inflammation (IL6, IL8, TNFα, and hsCRP) | Total association | 551 | −2.17 (−4.60; 0.25) |
| Direct association | 551 | −1.21 (−3.64; 1.25) | |
| Indirect association | 551 | −0.97 (−1.92; −0.21) | |
| Proportion mediated * | 45% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wesselink, E.; van Baar, H.; van Zutphen, M.; Tibosch, M.; Kouwenhoven, E.A.; Keulen, E.T.P.; Kok, D.E.; van Halteren, H.K.; Breukink, S.O.; de Wilt, J.H.W.; et al. Inflammation Is a Mediating Factor in the Association between Lifestyle and Fatigue in Colorectal Cancer Patients. Cancers 2020, 12, 3701. https://doi.org/10.3390/cancers12123701
Wesselink E, van Baar H, van Zutphen M, Tibosch M, Kouwenhoven EA, Keulen ETP, Kok DE, van Halteren HK, Breukink SO, de Wilt JHW, et al. Inflammation Is a Mediating Factor in the Association between Lifestyle and Fatigue in Colorectal Cancer Patients. Cancers. 2020; 12(12):3701. https://doi.org/10.3390/cancers12123701
Chicago/Turabian StyleWesselink, Evertine, Harm van Baar, Moniek van Zutphen, Meilissa Tibosch, Ewout A. Kouwenhoven, Eric T.P. Keulen, Dieuwertje E. Kok, Henk K. van Halteren, Stephanie O. Breukink, Johannes H. W. de Wilt, and et al. 2020. "Inflammation Is a Mediating Factor in the Association between Lifestyle and Fatigue in Colorectal Cancer Patients" Cancers 12, no. 12: 3701. https://doi.org/10.3390/cancers12123701
APA StyleWesselink, E., van Baar, H., van Zutphen, M., Tibosch, M., Kouwenhoven, E. A., Keulen, E. T. P., Kok, D. E., van Halteren, H. K., Breukink, S. O., de Wilt, J. H. W., Weijenberg, M. P., Kenkhuis, M.-F., Balvers, M. G. J., Witkamp, R. F., van Duijnhoven, F. J. B., Kampman, E., Beijer, S., Bours, M. J. L., & Winkels, R. M. (2020). Inflammation Is a Mediating Factor in the Association between Lifestyle and Fatigue in Colorectal Cancer Patients. Cancers, 12(12), 3701. https://doi.org/10.3390/cancers12123701