Avoiding Axillary Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy in Breast Cancer: Rationale for the Prospective, Multicentric EUBREAST-01 Trial


Abstract
:Simple Summary
Abstract
1. Introduction
2. Evidence for Axillary Surgery and Lymph Node Involvement in Patients with Breast pCR after NAST
2.1. Guidelines and Reviews
2.2. Retrospective Analyses Using Cancer Registry Data
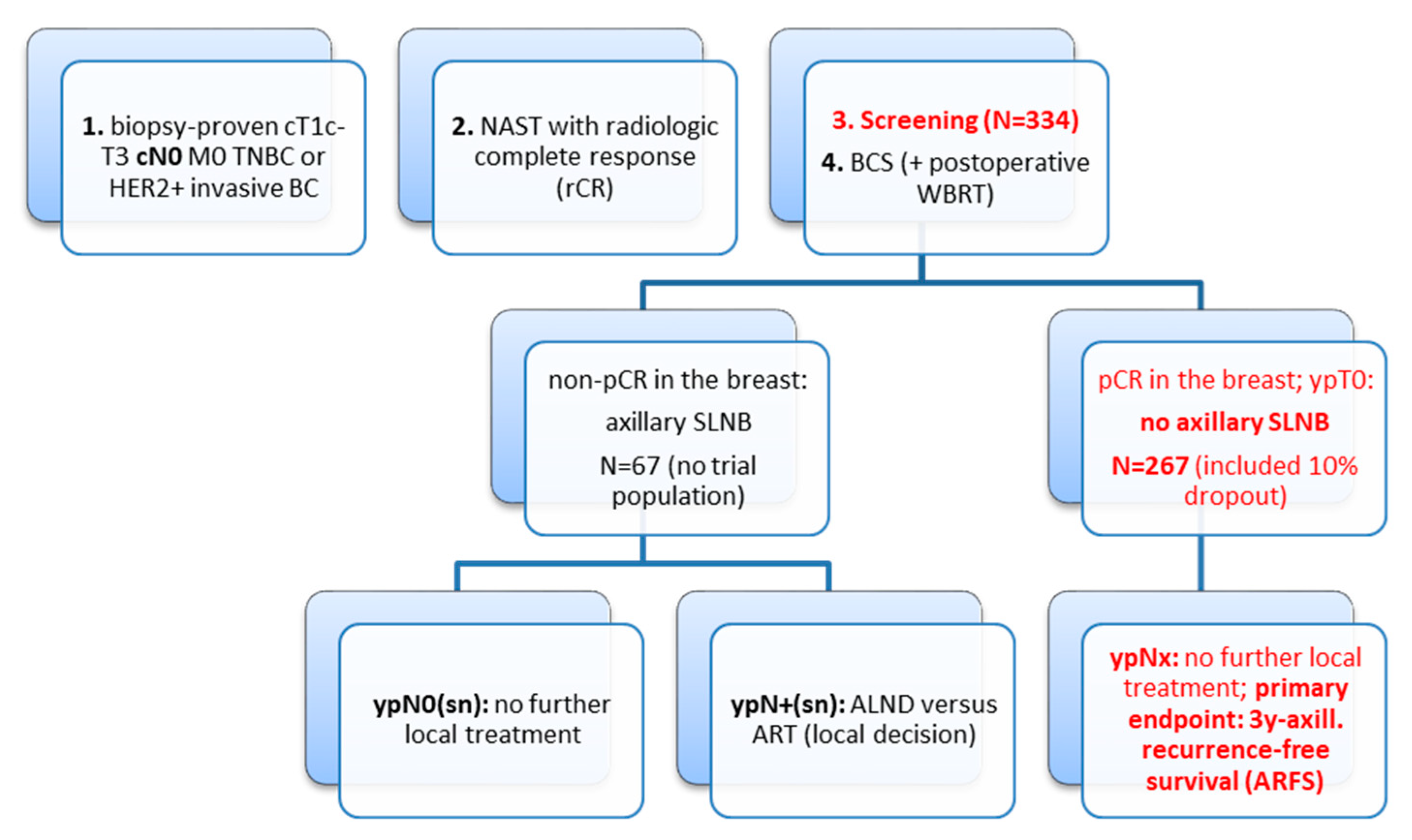
3. Discussion of the Study Design
3.1. Time Lines
- First patient in: Q1/2021
- Last patient in: Q4/2022
- First analysis: Q4/2025
- Final analysis: Q4/2027
3.2. Current Sstandard Treatment
3.3. Experimental Study Arm
3.4. Selection of Study Population
4. Primary Endpoint
5. Secondary Endpoints
- 5-year invasive disease-free survival
- 5-year overall survival
- 5-year locoregional disease-free survival
- 5-year distant disease-free survival
- 5-year ARFS
- 5-year ipsilateral axillary recurrence rate
- Diagnostic accuracy of imaging methods for pathologic complete response (breast pCR) after NAST. Regarding the secondary outcome of diagnostic accuracy of imaging methods, the potential value when using optional breast MRI will be evaluated.
6. Inclusion Criteria
- Written informed consent prior to BCS
- Histologically confirmed unilateral primary invasive carcinoma of the breast (core biopsy). Multifocal or multicentric tumors are allowed if BCS is planned.
- Age at diagnosis at least 18 years
- Imaging techniques with estimated tumor stage between cT1c-T3 prior to NAST
- Triple-negative or HER2-positive invasive breast cancer
- Clinically and sonographically tumor-free axilla prior to core biopsy (cN0/iN0)
- In cases with cN0 and iN+, a negative core biopsy or FNA of the sonographically suspected lymph node is required
- No evidence for distant metastasis (M0)
- standard NAST with radiologic complete response (rCR)
- Planned BCS with postoperative external whole-breast irradiation (conventional fractionation or hypofractionation)
7. Exclusion Criteria
- History of malignancy within the last 5 years, except curatively treated basalioma of the skin and carcinoma in situ of the cervix
- Time since last cycle of NAST > 3 months (optimal <1 month)
- Histologically non-invasive breast carcinoma
- Hormone receptor-positive/HER2-negative disease (triple-positive tumors are allowed)
- cT4 or iT4 tumors
- Pregnant or lactating patients
- No radiological complete response at the end of NAST
- Planned total mastectomy after NAST
- Planned intraoperative radiotherapy (e.g., Intrabeam) or postoperative partial breast irradiation (e.g., multicatheter technique) alone; both procedures are allowed as boost techniques
- Male patients
8. Imaging of Response to Standard NAST
9. Screening Phase
10. Surgical Therapy
11. Postoperative Radiotherapy
12. Pre- and Postoperative Systemic Therapy
- Hormone-sensitive (triple-positive) disease: patients should receive postoperative endocrine treatment according to current standard recommendations.
- All patients should receive neoadjuvant chemotherapy according to the current standard recommendations. Currently, postoperative chemotherapy is not indicated for patients with breast pCR after NAST.
- HER2-positive disease: all patients should receive anti-HER2-treatment according to current standard recommendations as neoadjuvant and post-neoadjuvant therapy; including routine cardiac assessment.
- Novel therapeutic modalities: PARP-inhibitors or immune checkpoint-inhibitors are allowed as treatment in clinical trials when ypNx status is not an exclusion criterion. If approved for the neoadjuvant or post-neoadjuvant setting, PARP-inhibitors or immune checkpoint-inhibitors are allowed as treatment according to standard recommendations.
- Bone modifying agents (bisphosphonates, denosumab) are allowed according to current treatment guidelines.
13. Sample Size Determination
14. Statistical Analyses
14.1. Evaluation of Primary Endpoint
14.2. Evaluation of Secondary Endpoints
15. Conclusions
- The experimental arm (no axillary SLNB) shows a high 3-year ARFS (≥98.5%). Omitting the axillary SLNB according to the inclusion criteria would be then considered as a new standard option for BCS of patients with neoadjuvant treated, primary breast cancer.
- The experimental arm (no axillary SLNB) shows an unacceptable 3-year ARFS rate of ≤96%. In this setting the current guidelines for SLNB are confirmed.
- The experimental arm (no axillary SLNB) shows an intermediate 3-year ARFS rate (96.1–98.4%). No final conclusion for routine clinical practice can be given; the conduction of a randomized clinical trial must be discussed.
Author Contributions
Funding
Conflicts of Interest
References
- Schwartz, G.F.; Guiliano, A.E.; Veronesi, U.; Consensus Conference Committee. Proceeding of the consensus conference of the role of sentinel lymph node biopsy in carcinoma or the breast April 19–22, 2001, Philadelphia, PA, USA. Breast J. 2002, 8, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Giuliano, A.E.; Somerfield, M.R.; Benson, A.B.; Bodurka, D.C., 3rd; Burstein, H.J.; Cochran, A.J.; Cody, H.S.; Edge, S.B., 3rd; Galper, S.; et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J. Clin. Oncol. 2005, 23, 7703–7720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krag, D.N.; Anderson, S.J.; Julian, T.B.; Brown, A.M.; Harlow, S.P.; Costantino, J.P.; Ashikaga, T.; Weaver, D.L.; Mamounas, E.P.; Jalovec, L.M.; et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: Overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010, 11, 927–933. [Google Scholar] [CrossRef] [Green Version]
- Crane-Okada, R.; Wascher, R.A.; Elashoff, D.; Giuliano, A.E. Long-term morbidity of sentinel node biopsy versus complete axillary dissection for unilateral breast cancer. Ann. Surg. Oncol. 2008, 15, 1996–2005. [Google Scholar] [CrossRef] [PubMed]
- Masuda, N.; Lee, S.J.; Ohtani, S.; Im, Y.H.; Lee, E.S.; Yokota, I.; Kuroi, K.; Im, S.A.; Park, B.W.; Kim, S.B.; et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef] [PubMed]
- von Minckwitz, G.; Huang, C.S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef]
- Curigliano, G.; Burstein, H.J.; Winer, E.P.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.J.; et al. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the primary therapy of early breast cancer 2017. Ann. Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Somerfield, M.R.; Bosserman, L.D.; Perkins, C.L.; Weaver, D.L.; Giuliano, A.E. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2014, 32, 1365–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Interdisciplinary German S3-Guideline for Screening, Diagnosis, Therapy and Follow-up in Breast Cancer. Version 4.0, December 2017, AWMF Registry Number 032-045OL. Available online: www.awmf.org (accessed on 30 October 2020).
- Pilewskie, M.; Morrow, M. Axillary nodal management following neoadjuvant chemotherapy: A review. JAMA Oncol. 2017, 3, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Hunt, K.K.; Yi, M.; Mittendorf, E.A.; Guerrero, C.; Babiera, G.V.; Bedrosian, I.; Hwang, R.F.; Kuerer, H.M.; Ross, M.I.; Meric-Bernstam, F. Sentinel lymph node surgery after neoadjuvant chemotherapy is accurate and reduces the need for axillary dissection in breast cancer patients. Ann. Surg. 2009, 250, 558–566. [Google Scholar] [CrossRef]
- Mamounas, E.P.; Anderson, S.J.; Dignam, J.J.; Bear, H.D.; Julian, T.B.; Geyer, C.E., Jr.; Taghian, A.; Wickerham, D.L.; Wolmark, N. Predictors of locoregional recurrence after neoadjuvant chemotherapy: Results from combined analysis of National Surgical Adjuvant Breast and Bowel Project B-18 and B-27. J. Clin. Oncol. 2012, 30, 3960–3966. [Google Scholar] [CrossRef] [PubMed]
- Morrow, M. Leveraging the benefits of systemic therapy to tailor surgery. JAMA Surg. 2017, 152, 671. [Google Scholar] [CrossRef] [PubMed]
- Tadros, A.B.; Yang, W.T.; Krishnamurthy, S.; Rauch, G.M.; Smith, B.D.; Valero, V.; Black, D.M.; Lucci, A., Jr.; Caudle, A.S.; DeSnyder, S.M.; et al. Identification of patients with documented pathologic complete response in the breast after neoadjuvant chemotherapy for omission of axillary surgery. JAMA Surg. 2017, 152, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Houssami, N.; Macaskill, P.; von Minckwitz, G.; Marinovich, M.L.; Mamounas, E. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoadjuvant chemotherapy. Eur. J. Cancer 2012, 48, 3342–3354. [Google Scholar] [CrossRef] [PubMed]
- Van der Noordaa, M.E.M.; van Duijnhoven, F.H.; Cuijpers, F.N.E.; van Werkhoven, E.; Wiersma, T.G.; Elkhuizen, P.H.M.; Winter-Warnars, G.; Dezentje, V.; Sonke, G.S.; Groen, E.J.; et al. Toward omitting sentinel lymph node biopsy after neoadjuvant chemotherapy in patients with clinically node-negative breast cancer. Br. J. Surg. 2020. [Google Scholar] [CrossRef]
- Barron, A.U.; Hoskin, T.L.; Day, C.N.; Hwang, E.S.; Kuerer, H.M.; Boughey, J.C. Association of low nodal positivity rate among patients with erbB2-positive or triple-negative breast cancer and breast pathologic complete response to neoadjuvant chemotherapy. JAMA Surg. 2018, 153, 1120–1126. [Google Scholar] [CrossRef] [Green Version]
- Samiei, S.; van Nijnatten, T.; de Munck, L.; Keymeulen, K.; Simons, J.M.; Kooreman, L.; Siesling, S.; Lobbes, M.; Smidt, M.L. Correlation between pathologic complete response in the breast and absence of axillary lymph node metastases after neoadjuvant systemic therapy. Ann. Surg. 2020, 271, 574–580. [Google Scholar] [CrossRef]
- Tolaney, S.M.; Barry, W.T.; Dang, C.T.; Yardley, D.A.; Moy, B.; Marcom, P.K.; Albain, K.S.; Rugo, H.S.; Ellis, M.; Shapira, I.; et al. Adjuvant paclitaxel and trastuzumab for node-negative, HER2-positive breast cancer. N. Engl. J. Med. 2015, 372, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Qiu, S.Q.; Zhang, G.J.; Jansen, L.; de Vries, J.; Schröder, C.P.; de Vries, E.; van Dam, G.M. Sentinel lymph node biopsy in early breast cancer. Breast Care 2011, 6, 185–191. [Google Scholar]
- Kuehn, T.; Bembenek, A.; Decker, T.; Munz, D.L.; Sautter-Bihl, M.L.; Untch, M.; Wallwiener, D.; Consensus Committee of the German Society of Senology. A concept for the clinical implementation of sentinel lymph node biopsy in patients with breast carcinoma with special regard to quality assurance. Cancer 2005, 103, 451–461. [Google Scholar] [CrossRef]
- Guidelines of the AGO Breast Committee, Version 2020.1. Available online: http://www.ago-online.de/leitlinien-empfehlungen/leitlinien-empfehlungen/kommission-mamma (accessed on 30 October 2020).
- Fowler, A.M.; Mankoff, D.A.; Joe, B.N. Imaging neoadjuvant therapy response in breast cancer. Radiology 2017, 285, 358–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishino, M.; Jackman, D.M.; Hatabu, H.; Yeap, B.Y.; Cioffredi, L.A.; Yap, J.T.; Jänne, P.A.; Johnson, B.E.; Van den Abbeele, A.D. New response evaluation criteria in solid tumors: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar]
- Yuan, Y.; Chen, X.S.; Liu, S.Y.; Shen, K.W. Accuracy of MRI in prediction of pathologic complete remission in breast cancer after preoperative therapy: A meta-analysis. Am. J. Radiol. 2010, 195, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Semiglazov, V. RECIST for response (clinical and imaging) in neoadjuvant clinical trials in operable breast cancer. J. Natl. Cancer Inst. Monogr. 2015, 2015, 21–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCCN (National Comprehensive Cancer Network). NCCN Practice Guidelines in Oncology: Breast Cancer. Version 6. 2020. Available online: http://www.nccn.org (accessed on 30 October 2020).
- von Minckwitz, G.; Untch, M.; Blohmer, J.U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef] [Green Version]
- Stachs, A.; Göde, K.; Hartmann, S.; Stengel, B.; Nierling, U.; Dieterich, M.; Reimer, T.; Gerber, B. Accuracy of axillary ultrasound in preoperative nodal staging of breast cancer—Size of metastases as limiting factor. Springerplus 2013, 2. [Google Scholar] [CrossRef] [Green Version]
- Bossuyt, V.; Provenzano, E.; Symmans, W.F.; Boughey, J.C.; Coles, C.; Curigliano, G.; Dixon, J.M.; Esserman, L.J.; Fastner, G.; Kuehn, T.; et al. Recommendations for standardized pathological characterization of residual disease for neoadjuvant clinical trials of breast cancer by the BIG-NABCG collaboration. Ann. Oncol. 2015, 26, 1280–1291. [Google Scholar] [CrossRef]
- Sautter-Bihl, M.L.; Sedlmayer, F.; Budach, W.; Dunst, J.; Feyer, P.; Fietkau, R.; Fussl, C.; Haase, W.; Harms, W.; Piroth, M.D.; et al. DEGRO practical guidelines: Radiotherapy of breast cancer. I. Strahlenther Onkol. 2013, 189, 825–833. [Google Scholar] [CrossRef]
- Haviland, J.S.; Owen, J.R.; Dewar, J.A.; Agrawal, R.K.; Barrett, J.; Barrett-Lee, P.J.; Dobbs, H.J.; Hopwood, P.; Lawton, P.A.; Magee, B.J.; et al. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up result of two randomised controlled trials. Lancet Oncol. 2013, 14, 1086–1094. [Google Scholar] [CrossRef]
- Murray Brunt, A.; Haviland, J.S.; Wheatley, D.A.; Sydenham, M.A.; Alhasso, A.; Bloomfield, D.J.; Chan, C.; Churn, M.; Cleator, S.; Coles, C.; et al. Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects from a multicenter, non-inferiority, randomized, phase 3 trial. Lancet 2020, 395, 1613–1626. [Google Scholar] [CrossRef]
- Sedlmayer, F.; Sautter-Bihl, M.L.; Budach, W.; Dunst, J.; Feyer, P.; Fietkau, R.; Haase, W.; Harms, W.; Rödel, C.; Souchon, R.; et al. Is the simultaneously integrated boost (SIB) technique for early breast cancer ready to be adopted for routine adjuvant radiotherapy? Strahlenther Onkol. 2013, 189, 193–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agresti, R.; Martelli, G.; Sandri, M.; Tagliabue, E.; Carcangiu, M.L.; Maugeri, I.; Pellitteri, C.; Ferraris, C.; Capri, G.; Moliterni, A.; et al. Axillary lymph node dissection versus no dissection in patients with T1N0 breast cancer: A randomized clinical trial (INT09/98). Cancer 2014, 120, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Nogi, H.; Uchida, K.; Mimoto, R.; Kamio, M.; Shioya, H.; Toriumi, Y.; Suzuki, M.; Nagasaki, E.; Kobayashi, T.; Takeyama, H. Long-term follow-up of node-negative breast cancer patients evaluated via sentinel node biopsy after neoadjuvant chemotherapy. Clin. Breast Cancer 2017, 17, 644–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galimberti, V.; Ribeiro Fontana, S.K.; Maisonneuve, P.; Steccanella, F.; Vento, A.R.; Intra, M.; Naninato, P.; Caldarella, P.; Iorfida, M.; Colleoni, M.; et al. Sentinel node biopsy after neoadjuvant treatment in breast cancer: Five-year follow-up of patients with clinically node-negative or node-positive disease before treatment. Eur. J. Surg. Oncol. 2016, 42, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Weaver, D.L.; Ashikaga, T.; Krag, D.N.; Skelly, J.M.; Anderson, S.J.; Harlow, S.P.; Julian, T.B.; Mamounas, E.P.; Wolmark, N. Effect of occult metastases on survival in node-negative breast cancer. N. Engl. J. Med. 2011, 364, 412–421. [Google Scholar] [CrossRef] [Green Version]
- de Boniface, J.; Frisell, J.; Bergkvist, L.; Andersson, Y.; Swedish Breast Cancer Group and the Swedish Society of Breast Surgery. Ten-year report on axillary recurrence after negative sentinel node biopsy for breast cancer from the Swedish multicentre cohort study. Br. J. Surg. 2017, 104, 238–247. [Google Scholar] [CrossRef]


{kind=link}
| Study for ypN+ Rate in cN0 Patients with Breast pCR (N) after NAST | ER+/HER2− | HER2+ | TNBC |
|---|---|---|---|
| Barron et al. [17] n = 5377 | n.d. | 1.6% | 1.6% |
| Samiei et al. [18] n = 986 | 6.7% | ER+/HER2+: 1.6% ER−/HER2+: 0.0% | 1.5% |
| Tadros et al. [14] n = 116 | n.d. | 0.0% | 0.0% |
| Van der Noordaa et al. [16] n = 89 | 0.0% | 0.0% | 0.0% |
| Study Characteristics (cN0; SLNB Alone after NAST) | Follow-Up | Axillary Recurrence Rate |
|---|---|---|
| Nogi et al. [36] n = 183 | 51.1 months | 0.0% |
| Galimberti et al. [37] n = 396 | 61 months | 0.0% |
| Hunt et al. [11] n = 575 (n = 491 SLNB alone) | 47 months | 1.2% |
| Mamounas et al. [12] n = 1384 (ALND or SLNB) | 10 years | 0.5–2.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reimer, T.; Glass, A.; Botteri, E.; Loibl, S.; D. Gentilini, O. Avoiding Axillary Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy in Breast Cancer: Rationale for the Prospective, Multicentric EUBREAST-01 Trial. Cancers 2020, 12, 3698. https://doi.org/10.3390/cancers12123698
Reimer T, Glass A, Botteri E, Loibl S, D. Gentilini O. Avoiding Axillary Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy in Breast Cancer: Rationale for the Prospective, Multicentric EUBREAST-01 Trial. Cancers. 2020; 12(12):3698. https://doi.org/10.3390/cancers12123698
Chicago/Turabian StyleReimer, Toralf, Aenne Glass, Edoardo Botteri, Sibylle Loibl, and Oreste D. Gentilini. 2020. "Avoiding Axillary Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy in Breast Cancer: Rationale for the Prospective, Multicentric EUBREAST-01 Trial" Cancers 12, no. 12: 3698. https://doi.org/10.3390/cancers12123698