Prognostic Factors Involved in the Epithelial–Mesenchymal Transition Process in Colorectal Cancer Have a Preponderant Role in Oxidative Stress: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Simple Summary
Abstract

1. Introduction
2. Results
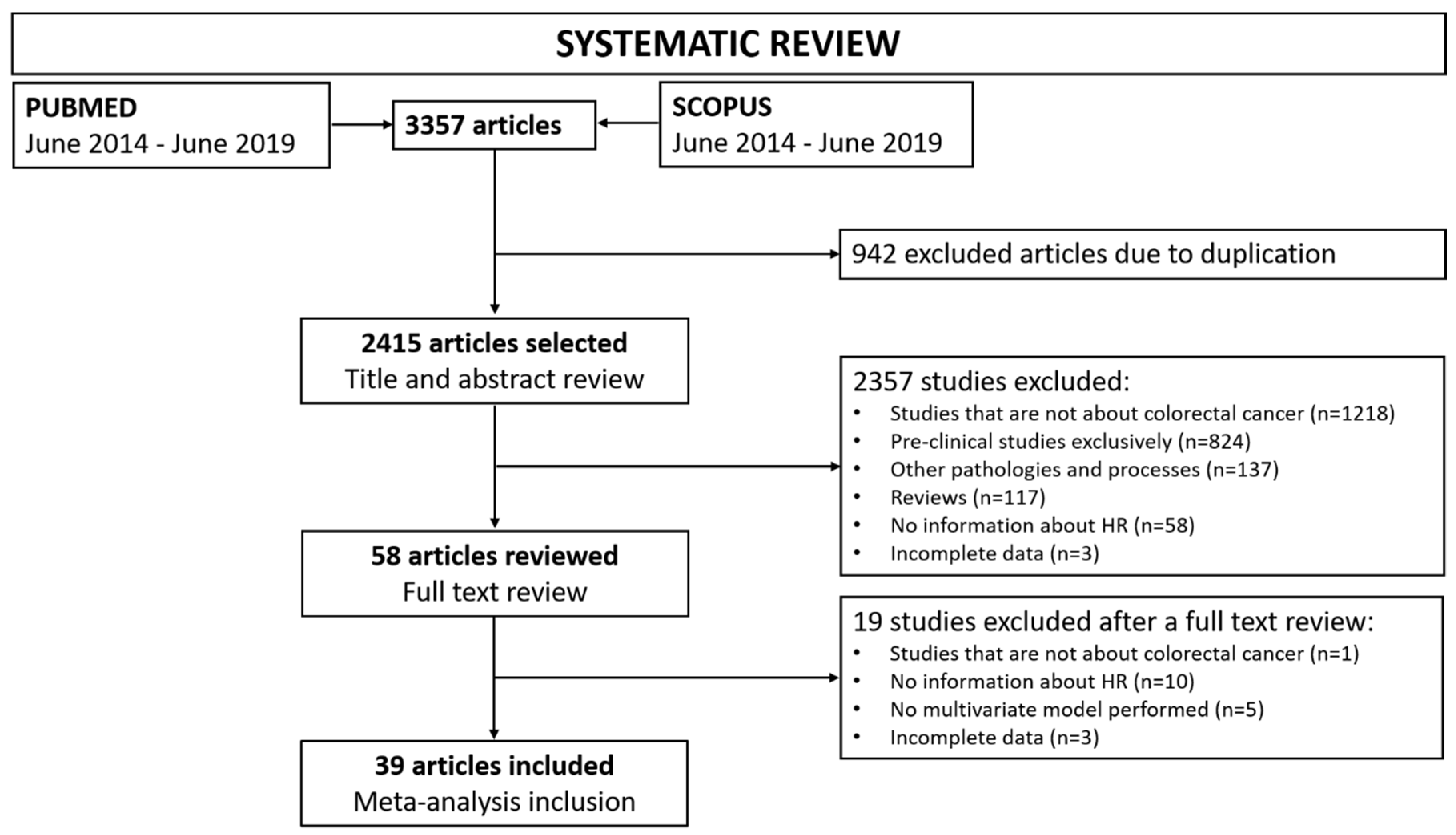
2.1. Search Results
2.2. Review of Eligible Studies
2.3. Meta-Analysis of the EMT-Related Prognostic Biomarkers in CRC
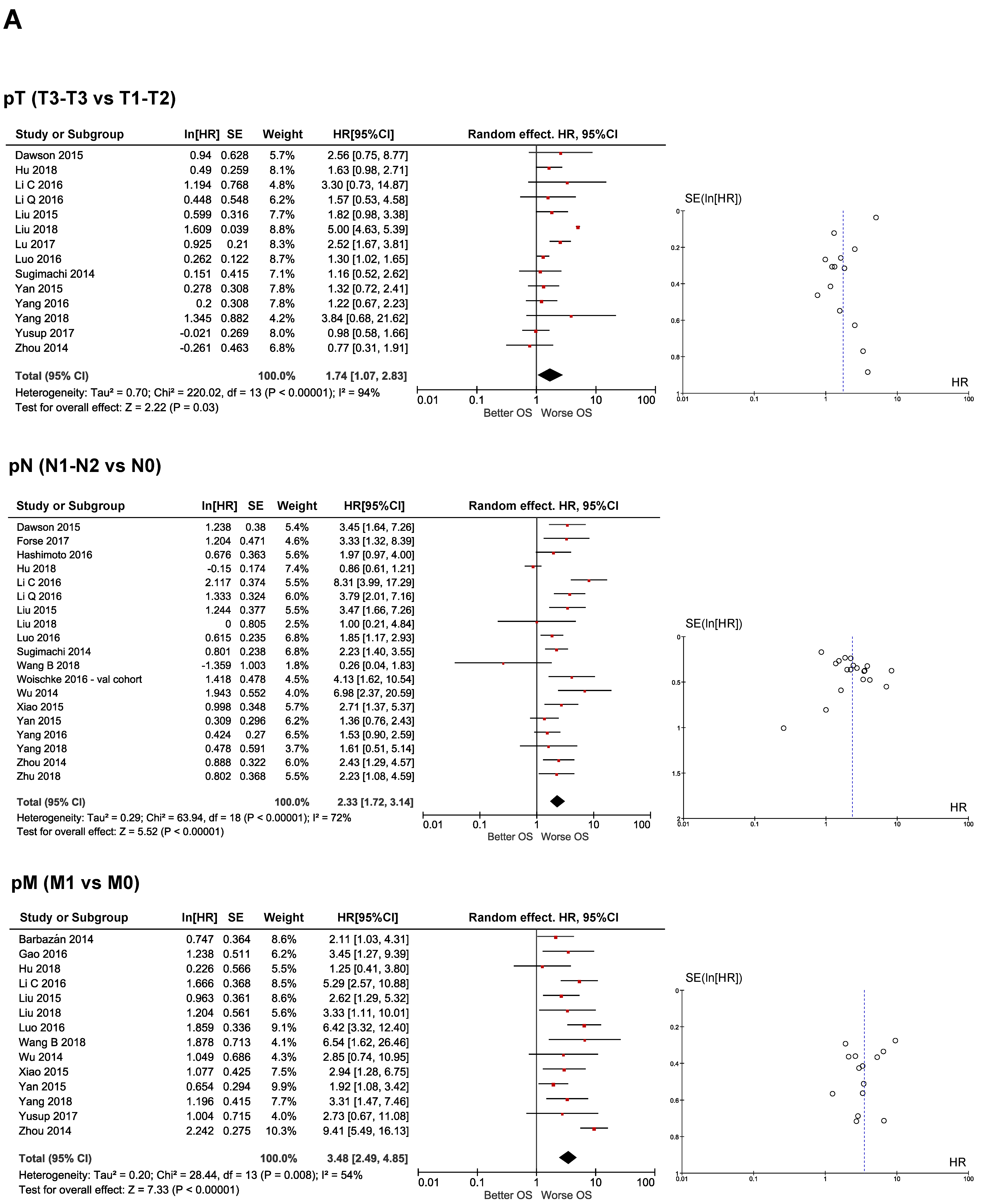
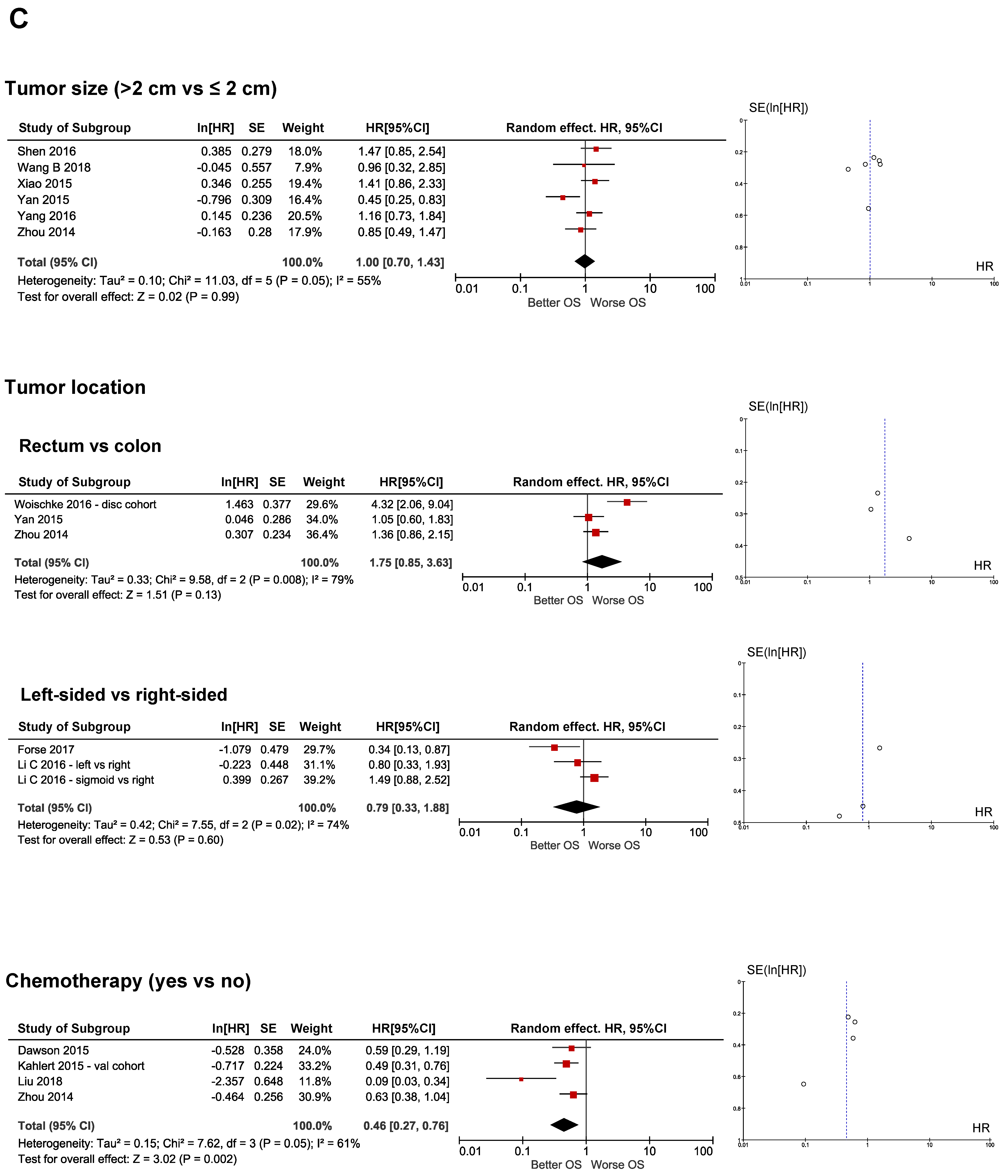
2.3.1. Clinical Prognostic Biomarkers
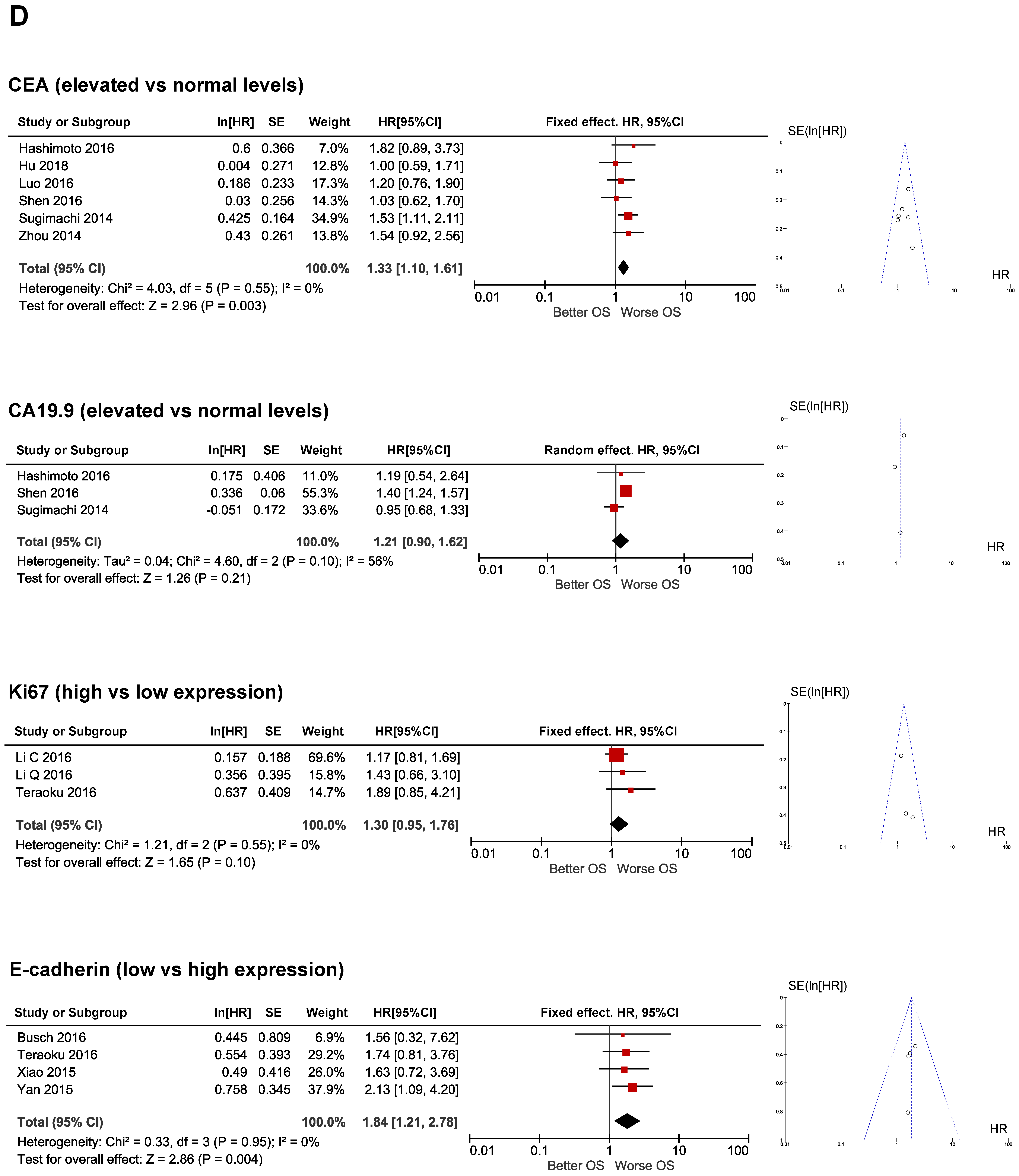
2.3.2. Molecular Prognostic Biomarkers
2.4. EMT-Related Molecular Biomarkers in CRC
2.5. Functional Enrichment Analysis
3. Discussion
4. Materials and Methods
4.1. Eligibility Criteria for Study Inclusion
4.2. Literature Search and Systematic Review Procedure
4.3. Statistical Analysis of the Meta-Analysis
4.4. GO Profiler Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Cunningham, D.; Atkin, W.; Lenz, H.J.; Lynch, H.T.; Minsky, B.; Nordlinger, B.; Starling, N. Colorectal cancer. Lancet 2010, 64, 104–117. [Google Scholar] [CrossRef]
- Cao, H.; Xu, E.; Liu, H.; Wan, L.; Lai, M. Epithelial-mesenchymal transition in colorectal cancer metastasis: A system review. Pathol. Res. Pract. 2015, 211, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.H.; Yang, J. Epithelial-mesenchymal plasticity in carcinoma metastasis. Genes Dev. 2013, 27, 2192–2206. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The american joint committee on cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Compton, C.C.; Fielding, L.P.; Burgart, L.J.; Conley, B.; Cooper, H.S.; Hamilton, S.R.; Hammond, M.E.H.; Henson, D.E.; Hutter, R.V.P.; Nagle, R.B.; et al. Prognostic factors in colorectal cancer: College of American Pathologists consensus statement. Archiv. Pathol. Lab. Med. 2000, 124, 979–994. [Google Scholar]
- Bender, U.; Rho, Y.S.; Barrera, I.; Aghajanyan, S.; Acoba, J.; Kavan, P. Adjuvant therapy for stages ii and iii colon cancer: Risk stratification, treatment duration, and future directions. Curr. Oncol. 2019, 26, S43–S52. [Google Scholar] [CrossRef] [PubMed]
- Fotheringham, S.; Mozolowski, G.A.; Murray, E.M.A.; Kerr, D.J. Challenges and solutions in patient treatment strategies for stage II colon cancer. Gastroenterol. Rep. 2019, 7, 151–161. [Google Scholar] [CrossRef]
- Labianca, R.; Nordlinger, B.; Beretta, G.D.; Mosconi, S.; Mandalà, M.; Cervantes, A.; Arnold, D. Early colon cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24 (Suppl. 6), vi64–vi72. [Google Scholar] [CrossRef]
- Zafar, S.N.; Hu, C.Y.; Snyder, R.A.; Cuddy, A.; You, Y.N.; Lowenstein, L.M.; Volk, R.J.; Chang, G.J. Predicting Risk of Recurrence After Colorectal Cancer Surgery in the United States: An Analysis of a Special Commission on Cancer National Study. Ann. Surg. Oncol. 2020, 27, 2740–2749. [Google Scholar] [CrossRef]
- Jen, J.; Kim, H.; Piantadosi, S.; Liu, Z.-F.; Levitt, R.C.; Sistonen, P.; Kinzler, K.W.; Vogelstein, B.; Hamilton, S.R. Allelic Loss of Chromosome 18q and Prognosis in Colorectal Cancer. N. Engl. J. Med. 1994, 331, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, H.; Zaanan, A.; Sinicrope, F.A. Microsatellite Instability Testing and Its Role in the Management of Colorectal Cancer. Curr. Treat. Options Oncol. 2015, 16, 30. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Wang, L.; Tan, S.; Kim, G.P.; Dou, R.; Chen, D.; Cai, Y.; Fu, X.; Wang, L.; Zhu, J.; et al. KRAS as a predictor of poor prognosis and benefit from postoperative FOLFOX chemotherapy in patients with stage II and III colorectal cancer. Mol. Oncol. 2015, 9, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Bazan, V.; Iacopetta, B.; Kerr, D.; Soussi, T.; Gebbia, N. TP53-CRC Collaborative Study Group. The TP53 colorectal cancer international collaborative study on the prognostic and predictive significance of p53 mutation: Influence of tumor site, type of mutation, and adjuvant treatment. J. Clin. Oncol. 2005, 23, 7518–7528. [Google Scholar] [CrossRef] [PubMed]
- Christou, N.; Perraud, A.; Blondy, S.; Jauberteau, M.O.; Battu, S.; Mathonnet, M. E-cadherin: A potential biomarker of colorectal cancer prognosis. Oncol. Lett. 2017, 13, 4571–4576. [Google Scholar] [CrossRef]
- Yan, X.; Yan, L.; Liu, S.; Shan, Z.; Tian, Y.; Jin, Z. N-cadherin, a novel prognostic biomarker, drives malignant progression of colorectal cancer. Mol. Med. Rep. 2015, 12, 2999–3006. [Google Scholar] [CrossRef]
- Toiyama, Y.; Yasuda, H.; Saigusa, S.; Tanaka, K.; Inoue, Y.; Goel, A.; Kusunoki, M. Increased expression of slug and vimentin as novel predictive biomarkers for lymph node metastasis and poor prognosis in colorectal cancer. Carcinogenesis 2013, 34, 2548–2557. [Google Scholar] [CrossRef]
- Salazar, R.; Roepman, P.; Capella, G.; Moreno, V.; Simon, I.; Dreezen, C.; Lopez-Doriga, A.; Santos, C.; Marijnen, C.; Westerga, J.; et al. Gene expression signature to improve prognosis prediction of stage II and III colorectal cancer. J. Clin. Oncol. 2011, 29, 17–24. [Google Scholar] [CrossRef]
- Wang, L.; Shen, X.; Wang, Z.; Xiao, X.; Wei, P.; Wang, Q.; Ren, F.; Wang, Y.; Liu, Z.; Sheng, W.; et al. A molecular signature for the prediction of recurrence in colorectal cancer. Mol. Cancer 2015, 14, 1–10. [Google Scholar] [CrossRef]
- Weiser, M.R. AJCC 8th Edition: Colorectal Cancer. Ann. Surg. Oncol. 2018, 25, 1454–1455. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; UICC; Brierley, J.; Gospodarowicz, M.K. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Oxford, UK; Hoboken, NJ, USA, 2016; 253p. [Google Scholar]
- Dukes, C. The classification of cancer of the rectum. J. Pathol. Bacteriol. 1932, 35, 323–332. [Google Scholar] [CrossRef]
- Barbazan, J.; Muinelo-Romay, L.; Vieito, M.; Candamio, S.; Diaz-Lopez, A.; Cano, A.; Gomez-Tato, A.; De Los Angeles Casares De Cal, M.; Abal, M.; Lopez-Lopez, R. A multimarker panel for circulating tumor cells detection predicts patient outcome and therapy response in metastatic colorectal cancer. Int. J. Cancer 2014, 135, 2633–2643. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.H.; Lu, C.; Wang, Z.N.; Song, Y.X.; Zhu, J.L.; Gao, P.; Sun, J.X.; Chen, X.W.; Wang, M.X.; Dong, Y.L.; et al. ILEI: A novel marker for epithelial-mesenchymal transition and poor prognosis in colorectal cancer. Histopathology 2014, 65, 527–538. [Google Scholar] [CrossRef]
- Sugimachi, K.; Yokobori, T.; Iinuma, H.; Ueda, M.; Ueo, H.; Shinden, Y.; Eguchi, H.; Sudo, T.; Suzuki, A.; Maehara, Y.; et al. Aberrant Expression of Plastin-3 Via Copy Number Gain Induces the Epithelial–Mesenchymal Transition in Circulating Colorectal Cancer Cells. Ann. Surg. Oncol. 2014, 21, 3680–3690. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.E.H.; Wang, X.L.; Tang, H.M.; Jiang, T.; Chen, J.; Lu, S.U.; Qiu, G.Q.; Peng, Z.H.; Yan, D.W. Long non-coding RNA HOTAIR is a powerful predictor of metastasis and poor prognosis and is associated with epithelial-mesenchymal transition in colon cancer. Oncol. Rep. 2014, 32, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wu, J.; Fu, X.; Du, W.; Zhou, L.; Meng, X.; Yu, H.; Lin, J.; Ye, W.; Liu, J.; et al. OTUB1 promotes metastasis and serves as a marker of poor prognosis in colorectal cancer. Mol. Cancer 2014, 13, 258. [Google Scholar] [CrossRef]
- Dawson, H.; Grundmann, S.; Koelzer, V.H.; Galván, J.A.; Kirsch, R.; Karamitopoulou, E.; Lugli, A.; Inderbitzin, D.; Zlobec, I. Tyrosine kinase receptor B (TrkB) expression in colorectal cancers highlights anoikis resistance as a survival mechanism of tumour budding cells. Histopathology 2015, 66, 715–725. [Google Scholar] [CrossRef]
- Kahlert, C.; Lerbs, T.; Pecqueux, M.; Herpel, E.; Hoffmeister, M.; Jansen, L.; Brenner, H.; Chang-Claude, J.; Bläker, H.; Kloor, M.; et al. Overexpression of SIX1 is an independent prognostic marker in stage I-III colorectal cancer. Int. J. Cancer 2015, 137, 2104–2113. [Google Scholar] [CrossRef]
- Liu, G.; Zhu, J.; Yu, M.; Cai, C.; Zhou, Y.; Yu, M.; Fu, Z.; Gong, Y.; Yang, B.; Li, Y.; et al. Glutamate dehydrogenase is a novel prognostic marker and predicts metastases in colorectal cancer patients. J. Transl. Med. 2015, 13, 144. [Google Scholar] [CrossRef]
- Xiao, S.; Liu, L.; Lu, X.; Long, J.; Zhou, X.; Fang, M. The prognostic significance of bromodomain PHD-finger transcription factor in colorectal carcinoma and association with vimentin and E-cadherin. J. Cancer Res. Clin. Oncol. 2015, 141, 1465–1474. [Google Scholar] [CrossRef]
- Busch, E.L.; Keku, T.O.; Richardson, D.B.; Cohen, S.M.; Eberhard, D.A.; Avery, C.L.; Sandler, R.S. Evaluating markers of epithelial-mesenchymal transition to identify cancer patients at risk for metastatic disease. Clin. Exp. Metastasis 2016, 33, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Gao, T.; Wang, M.; Xu, L.; Wen, T.; Liu, J.; An, G. DCLK1 is up-regulated and associated with metastasis and prognosis in colorectal cancer. J. Cancer Res. Clin. Oncol. 2016, 142, 2131–2140. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, M.; Kobayashi, T.; Tashiro, H.; Arihiro, K.; Kikuchi, A.; Ohdan, H. h-Prune is associated with poor prognosis and epithelial–mesenchymal transition in patients with colorectal liver metastases. Int. J. Cancer 2016, 139, 812–823. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wei, P.; Huang, B.; Xu, Y.; Li, X.; Li, Y.; Cai, S.; Li, D. MAEL expression links epithelial-mesenchymal transition and stem cell properties in colorectal cancer. Int. J. Cancer 2016, 139, 2502–2511. [Google Scholar] [CrossRef]
- Li, C.; Chen, J.; Wang, Y.; Song, G.; Xiao, C.; Yan, D.; Zhong, L.; Sun, X.; Wang, X.; Yu, F.; et al. High-level expression of P21-Cdc/Rac-actived kinase 7 is closely related to metastatic potential and poor prognosis of colon carcinoma. Oncotarget 2016, 7, 46042–46055. [Google Scholar] [CrossRef]
- Luo, Y.; Ye, G.Y.; Qin, S.L.; Mu, Y.F.; Zhang, L.; Qi, Y.; Qiu, Y.E.; Yu, M.H.; Zhong, M. High expression of Rab3D predicts poor prognosis and associates with tumor progression in colorectal cancer. Int. J. Biochem. Cell Biol. 2016, 75, 53–62. [Google Scholar] [CrossRef]
- Matsusaka, S.; Zhang, W.; Cao, S.; Hanna, D.L.; Sunakawa, Y.; Sebio, A.; Ueno, M.; Yang, D.; Ning, Y.; Parekh, A.; et al. TWIST1 Polymorphisms Predict Survival in Patients with Metastatic Colorectal Cancer Receiving First-Line Bevacizumab plus Oxaliplatin-Based Chemotherapy. Mol. Cancer Ther. 2016, 15, 1405–1411. [Google Scholar] [CrossRef]
- Ning, Y.; Zhang, W.; Hanna, D.L.; Yang, D.; Okazaki, S.; Berger, M.D.; Miyamoto, Y.; Suenaga, M.; Schirripa, M.; El-Khoueiry, A.; et al. Clinical relevance of EMT and stem-like gene expression in circulating tumor cells of metastatic colorectal cancer patients. Pharmacogenomics J. 2018, 18, 29–34. [Google Scholar] [CrossRef]
- Satelli, A.; Batth, I.S.; Brownlee, Z.; Rojas, C.; Meng, Q.H.; Kopetz, S.; Li, S. Potential role of nuclear PD-L1 expression in cell-surface vimentin positive circulating tumor cells as a prognostic marker in cancer patients. Sci. Rep. 2016, 6, 28910. [Google Scholar] [CrossRef]
- Shen, Z.Y.; Fang, Y.; Zhen, L.; Zhu, X.J.; Chen, H.; Liu, H.; Jiang, B.; Li, G.X.; Deng, H.J. Analysis of the predictive efficiency of S100P on adverse prognosis and the pathogenesis of S100P-mediated invasion and metastasis of colon adenocarcinoma. Cancer Genet. 2016, 209, 143–153. [Google Scholar] [CrossRef]
- Teraoku, H.; Morine, Y.; Ikemoto, T.; Saito, Y.; Yamada, S.; Yoshikawa, M.; Takasu, C.; Higashijima, J.; Imura, S.; Shimada, M. Role of thrombospondin-1 expression in colorectal liver metastasis and its molecular mechanism. J. Hepatobiliary Pancreat. Sci. 2016, 23, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Woischke, C.; Blaj, C.; Schmidt, E.M.; Lamprecht, S.; Engel, J.; Hermeking, H.; Kirchner, T.; Horst, D. CYB5R1 links epithelial-mesenchymal transition and poor prognosis in colorectal cancer. Oncotarget 2016, 7, 31350–31360. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Chen, T.; Xu, Z.; Zhu, H.; Wang, J.; He, Z. Long noncoding RNA GAPLINC promotes invasion in colorectal cancer by targeting SNAI2 through binding with PSF and NONO. Oncotarget 2016, 7, 42183–42194. [Google Scholar] [CrossRef] [PubMed]
- Yokota, M.; Kojima, M.; Higuchi, Y.; Nishizawa, Y.; Kobayashi, A.; Ito, M.; Saito, N.; Ochiai, A. Gene expression profile in the activation of subperitoneal fibroblasts reflects prognosis of patients with colon cancer. Int. J. Cancer 2016, 138, 1422–1431. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhu, Y.; Dong, Y.; Zhang, P.; Han, X.; Jin, J.; Ma, X. Overexpression of TrpC5 promotes tumor metastasis via the HIF-1α-Twist signaling pathway in colon cancer. Clin. Sci. 2017, 131, 2439–2450. [Google Scholar] [CrossRef]
- Forse, C.L.; Rahimi, M.; Diamandis, E.P.; Assarzadegan, N.; Dawson, H.; Grin, A.; Kennedy, E.; O’Connor, B.; Messenger, D.E.; Riddell, R.H.; et al. HtrA3 stromal expression is correlated with tumor budding in stage II colorectal cancer. Exp. Mol. Pathol. 2017, 103, 94–100. [Google Scholar] [CrossRef]
- Lu, M.; Liu, Z.; Li, B.; Wang, G.; Li, D.; Zhu, Y. The high expression of long non-coding RNA PANDAR indicates a poor prognosis for colorectal cancer and promotes metastasis by EMT pathway. J. Cancer Res. Clin. Oncol. 2017, 143, 71–81. [Google Scholar] [CrossRef]
- Miyoshi, J.; Toden, S.; Yoshida, K.; Toiyama, Y.; Alberts, S.R.; Kusunoki, M.; Sinicrope, F.A.; Goel, A. MiR-139-5p as a novel serum biomarker for recurrence and metastasis in colorectal cancer. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Hu, X.; Jiang, Y.; Hu, Y.; Liu, Z.; Liu, J.; Wen, T.; Ma, Y.; An, G.; et al. Upregulated NNT-AS1, a long noncoding RNA, contributes to proliferation and migration of colorectal cancer cells in vitro and in vivo. Oncotarget 2017, 8, 3441–3453. [Google Scholar] [CrossRef]
- Yusup, A.; Huji, B.; Fang, C.; Wang, F.; Dadihan, T.; Wang, H.J.; Upur, H. Expression of trefoil factors and TWIST1 in colorectal cancer and their correlation with metastatic potential and prognosis. World J. Gastroenterol. 2017, 23, 110–120. [Google Scholar] [CrossRef]
- Zhao, J.; Ou, B.; Han, D.; Wang, P.; Zong, Y.; Zhu, C.; Liu, D.; Zheng, M.; Sun, J.; Feng, H.; et al. Tumor-derived CXCL5 promotes human colorectal cancer metastasis through activation of the ERK/Elk-1/Snail and AKT/GSK3β/β-catenin pathways. Mol. Cancer 2017, 16, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Kim, J.S.; Eun, H.S.; Kang, S.H.; Lee, E.S.; Kim, S.H.; Sung, J.K.; Lee, B.S.; Jeong, H.Y.; Moon, H.S. Expression of NOX Family Genes and Their Clinical Significance in Colorectal Cancer. Dig. Dis. Sci. 2018, 63, 2332–2340. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Li, Y.Q.; Li, Q.G.; Ma, Y.L.; Peng, J.J.; Cai, S.J. ITGAE Defines CD8+ Tumor-Infiltrating Lymphocytes Predicting a better Prognostic Survival in Colorectal Cancer. EBioMedicine 2018, 35, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Konishi, Y.; Kawamata, F.; Nishihara, H.; Homma, S.; Kato, Y.; Tsuda, M.; Kohsaka, S.; Einama, T.; Liu, C.; Yoshida, T.; et al. Tumor budding and human chorionic gonadotropin-β expression correlate with unfavorable patient outcome in colorectal carcinoma. Med. Oncol. 2018, 35, 104. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhang, X.; Cai, J.; Li, Y.; Luo, Q.; Wu, H.; Yang, Z.; Wang, L.; Chen, D. Downregulation of TRIM58 expression is associated with a poor patient outcome and enhances colorectal cancer cell invasion. Oncol. Rep. 2018, 40, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wan, L.; Wu, S.; Yang, J.; Zhou, Y.; Liu, F.; Wu, Z.; Cheng, Y. Mesenchymal marker and LGR5 expression levels in circulating tumor cells correlate with colorectal cancer prognosis. Cell. Oncol. 2018, 41, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Mujun, Y.; Cheng, C.; Jiang, H.; Jiang, K.; Shen, Z.; Yingjiang, Y.; Wang, S. Decreased expression of miR-490-3p in colorectal cancer predicts poor prognosis and promotes cell proliferation and invasion by targeting RAB14. Int. J. Oncol. 2018, 53, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Zhang, C.; Qi, W.; Cui, C.; Cui, Y.; Xuan, Y. Tenascin-C as a prognostic determinant of colorectal cancer through induction of epithelial-to-mesenchymal transition and proliferation. Exp. Mol. Pathol. 2018, 105, 216–222. [Google Scholar] [CrossRef]
- Zhu, B.; Wang, Y.; Wang, X.; Wu, S.; Zhou, L.; Gong, X.; Song, W.; Wang, D. Evaluation of the correlation of MACC1, CD44, Twist1, and KiSS-1 in the metastasis and prognosis for colon carcinoma. Diagn. Pathol. 2018, 13, 45. [Google Scholar] [CrossRef]
- Gunderson, L.L.; Jessup, J.M.; Sargent, D.J.; Greene, F.L.; Stewart, A.K. Revised TN categorization for colon cancer based on national survival outcomes data. J. Clin. Oncol. 2010, 28, 264–271. [Google Scholar] [CrossRef]
- Greene, F.L.; Stewart, A.K.; Norton, H.J.; Cohen, A.M. A new TNM staging strategy for node-positive (stage III) colon cancer: An analysis of 50,042 patients. Ann. Surg. 2002, 236, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Guo, B.C.; Sun, L.R.; Wang, J.W.; Fu, X.H.; Zhang, S.Z.; Poston, G.; Ding, K.F. TNM staging of colorectal cancer should be reconsidered by T stage weighting. World J. Gastroenterol. 2014, 20, 5104–5112. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.N.; Carr, P.R.; Jansen, L.; Chang-Claude, J.; Weitz, J.; Hoffmeister, M.; Brenner, H. Time of Metastasis and Outcome in Colorectal Cancer. Ann. Surg. 2019, 269, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Vatandoust, S.; Price, T.J.; Karapetis, C.S. Colorectal cancer: Metastases to a single organ. World J. Gastroenterol. 2015, 21, 11767–11776. [Google Scholar] [CrossRef]
- Marzouk, O.; Schofield, J. Review of histopathological and molecular prognostic features in colorectal cancer. Cancers 2011, 3, 2767–2810. [Google Scholar] [CrossRef]
- Ueno, H.; Shinto, E.; Kajiwara, Y.; Fukazawa, S.; Shimazaki, H.; Yamamoto, J.; Hase, K. Prognostic impact of histological categorisation of epithelial-mesenchymal transition in colorectal cancer. Br. J. Cancer 2014, 111, 2082–2090. [Google Scholar] [CrossRef]
- Sargent, D.; Sobrero, A.; Grothey, A.; O’Connell, M.J.; Buyse, M.; Andre, T.; Zheng, Y.; Green, E.; Labianca, R.; O’Callaghan, C.; et al. Evidence for cure by adjuvant therapy in colon cancer: Observations based on individual patient data from 20,898 patients on 18 randomized trials. J. Clin. Oncol. 2009, 27, 872–877. [Google Scholar] [CrossRef]
- Shah, M.A.; Renfro, L.A.; Allegra, C.J.; André, T.; De Gramont, A.; Schmoll, H.J.; Haller, D.G.; Alberts, S.R.; Yothers, G.; Sargent, D.J. Impact of patient factors on recurrence risk and time dependency of oxaliplatin benefit in patients with colon cancer: Analysis from modern-era adjuvant studies in the adjuvant colon cancer end points (ACCENT) database. J. Clin. Oncol. 2016, 34, 843–853. [Google Scholar] [CrossRef]
- Barone, C.; Nuzzo, G.; Cassano, A.; Basso, M.; Schinzari, G.; Giuliante, F.; D’Argento, E.; Trigila, N.; Astone, A.; Pozzo, C. Final analysis of colorectal cancer patients treated with irinotecan and 5-fluorouracil plus folinic acid neoadjuvant chemotherapy for unresectable liver metastases. Br. J. Cancer 2007, 97, 1035–1039. [Google Scholar] [CrossRef]
- Harris, E.I.; Lewin, D.N.; Wang, H.L.; Lauwers, G.Y.; Srivastava, A.; Shyr, Y.; Shakhtour, B.; Revetta, F.; Washington, M.K. Lymphovascular invasion in colorectal cancer: An interobserver variability study. Am. J. Surg. Pathol. 2008, 32, 1816–1821. [Google Scholar] [CrossRef]
- Jiang, H.H.; Zhang, Z.Y.; Wang, X.Y.; Tang, X.; Liu, H.L.; Wang, A.L.; Li, H.G.; Tang, E.J.; Lin, M. Bin Prognostic significance of lymphovascular invasion in colorectal cancer and its association with genomic alterations. World J. Gastroenterol. 2019, 25, 2489–2502. [Google Scholar] [CrossRef] [PubMed]
- Barresi, V.; Reggiani Bonetti, L.; Vitarelli, E.; Di Gregorio, C.; Ponz De Leon, M.; Barresi, G. Immunohistochemical assessment of lymphovascular invasion in stage i colorectal carcinoma: Prognostic relevance and correlation with nodal micrometastases. Am. J. Surg. Pathol. 2012, 36, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Sutoh, T.; Morita, H.; Yajima, R.; Yamaguchi, S.; Tsutsumi, S.; Asao, T.; Kuwano, H. Vascular invasion, but not lymphatic invasion, of the primary tumor is a strong prognostic factor in patients with colorectal cancer. Anticancer Res. 2014, 34, 3147–3151. [Google Scholar] [PubMed]
- Crozier, J.E.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Anderson, J.H.; Horgan, P.G.; McKee, R.F. Tumor size is associated with the systemic inflammatory response but not survival in patients with primary operable colorectal cancer. J. Gastroenterol. Hepatol. 2007, 22, 2288–2291. [Google Scholar] [CrossRef]
- Saha, S.; Shaik, M.; Johnston, G.; Saha, S.K.; Berbiglia, L.; Hicks, M.; Gernand, J.; Grewal, S.; Arora, M.; Wiese, D. Tumor size predicts long-term survival in colon cancer: An analysis of the National Cancer Data Base. Am. J. Surg. 2015, 209, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; An, B.; Ma, J.; He, B.; Qi, J.; Wang, W.; Qin, C.; Zhao, Q. Prognostic value of the tumor size in resectable colorectal cancer with different primary locations: A retrospective study with the propensity score matching. J. Cancer 2019, 10, 313–322. [Google Scholar] [CrossRef]
- Loupakis, F.; Yang, D.; Yau, L.; Feng, S.; Cremolini, C.; Zhang, W.; Maus, M.K.H.; Antoniotti, C.; Langer, C.; Scherer, S.J.; et al. Primary tumor location as a prognostic factor in metastatic colorectal cancer. J. Natl. Cancer Inst. 2015, 107, dju427. [Google Scholar] [CrossRef]
- Wang, C.B.; Shahjehan, F.; Merchea, A.; Li, Z.; Bekaii-Saab, T.S.; Grothey, A.; Colibaseanu, D.T.; Kasi, P.M. Impact of tumor location and variables associated with overall survival in patients with colorectal cancer: A mayo clinic colon and rectal cancer registry study. Front. Oncol. 2019, 9, 76. [Google Scholar]
- Patel, M.; McSorley, S.T.; Park, J.H.; Roxburgh, C.S.D.; Edwards, J.; Horgan, P.G.; McMillan, D.C. The relationship between right-sided tumour location, tumour microenvironment, systemic inflammation, adjuvant therapy and survival in patients undergoing surgery for colon and rectal cancer. Br. J. Cancer 2018, 118, 705–712. [Google Scholar] [CrossRef]
- Bajenova, O.; Chaika, N.; Tolkunova, E.; Davydov-Sinitsyn, A.; Gapon, S.; Thomas, P.; O’Brien, S. Carcinoembryonic antigen promotes colorectal cancer progression by targeting adherens junction complexes. Exp. Cell Res. 2014, 324, 115–123. [Google Scholar] [CrossRef]
- Yoshikawa, M.; Morine, Y.; Ikemoto, T.; Imura, S.; Higashijima, J.; Iwahashi, S.; Saito, Y.; Takasu, C.; Yamada, S.; Ishikawa, D.; et al. Elevated preoperative serum cea level is associated with poor prognosis in patients with hepatocellular carcinoma through the epithelial-mesenchymal transition. Anticancer Res. 2017, 37, 1169–1175. [Google Scholar] [CrossRef]
- Destri, G.L.; Rubino, A.S.; Latino, R.; Giannone, F.; Lanteri, R.; Scilletta, B.; Di Cataldo, A. Preoperative carcinoembryonic antigen and prognosis of colorectal cancer. An independent prognostic factor still reliable. Int. Surg. 2015, 100, 617–625. [Google Scholar] [CrossRef]
- Bhatti, I.; Patel, M.; Dennison, A.R.; Thomas, M.W.; Garcea, G. Utility of postoperative CEA for surveillance of recurrence after resection of primary colorectal cancer. Int. J. Surg. 2015, 16, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Poruk, E.K.; Gay, Z.D.; Brown, K.D.; Mulvihill, J.; Boucher, M.K.; Scaife, L.C.; Firpo, A.M.; Mulvihill, J.S. The Clinical Utility of CA 19-9 in Pancreatic Adenocarcinoma: Diagnostic and Prognostic Updates. Curr. Mol. Med. 2013, 13, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Stiksma, J.; Grootendorst, D.C.; Van Der Linden, P.W.G. CA 19-9 as a marker in addition to CEA to monitor colorectal cancer. Clin. Colorectal Cancer 2014, 13, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Hirakawa, M.; Takimoto, R.; Tamura, F.; Yoshida, M.; Ono, M.; Murase, K.; Sato, Y.; Osuga, T.; Sato, T.; Iyama, S.; et al. Fucosylated TGF-β receptors transduces a signal for epithelial-mesenchymal transition in colorectal cancer cells. Br. J. Cancer 2014, 110, 156–163. [Google Scholar] [CrossRef]
- Li, L.T.; Jiang, G.; Chen, Q.; Zheng, J.N. Predic Ki67 is a promising molecular target in the diagnosis of cancer (Review). Mol. Med. Rep. 2015, 11, 1566–1572. [Google Scholar] [CrossRef]
- Luo, Z.W.; Zhu, M.G.; Zhang, Z.Q.; Ye, F.J.; Huang, W.H.; Luo, X.Z. Increased expression of Ki-67 is a poor prognostic marker for colorectal cancer patients: A meta analysis. BMC Cancer 2019, 19, 123. [Google Scholar] [CrossRef]
- Tong, G.; Zhang, G.; Liu, J.; Zheng, Z.; Chen, Y.; Niu, P.; Xu, X. Cutoff of 25% for Ki67 expression is a good classification tool for prognosis in colorectal cancer in the AJCC-8 stratification. Oncol. Rep. 2020, 43, 1187–1198. [Google Scholar] [CrossRef]
- Melling, N.; Kowitz, C.M.; Simon, R.; Bokemeyer, C.; Terracciano, L.; Sauter, G.; Izbicki, J.R.; Marx, A.H. High Ki67 expression is an independent good prognostic marker in colorectal cancer. J. Clin. Pathol. 2016, 69, 209–214. [Google Scholar] [CrossRef]
- Gasinska, A.; Jaszczynski, J.; Adamczyk, A.; Janecka-Widla, A.; Wilk, W.; Cichocka, A.; Stelmach, A. Biomarkers of epithelial-mesenchymal transition in localized, surgically treated clear-cell renal cell carcinoma. Folia Histochem. Cytobiol. 2019, 56, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Hemalatha, A.; Suresh, T.N.; Harendra Kumar, M.L. Expression of vimentin in breast carcinoma, its correlation with Ki67 and other histopathological parameters. Indian J. Cancer 2013, 50, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Onder, T.T.; Gupta, P.B.; Mani, S.A.; Yang, J.; Lander, E.S.; Weinberg, R.A. Loss of E-cadherin promotes metastasis via multiple downstream transcriptional pathways. Cancer Res. 2008, 68, 3645–3654. [Google Scholar] [CrossRef] [PubMed]
- Schetter, A.J.; Okayama, H.; Harris, C.C. The role of MicroRNAs in colorectal cancer. Cancer J. 2012, 18, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Zaravinos, A. The regulatory role of MicroRNAs in EMT and cancer. J. Oncol. 2015, 2015, 865816. [Google Scholar] [CrossRef]
- Luo, X.; Burwinkel, B.; Tao, S.; Brenner, H. MicroRNA signatures: Novel biomarker for colorectal cancer? Cancer Epidemiol. Biomarkers Prev. 2011, 20, 1272–1286. [Google Scholar] [CrossRef]
- Li, Q.; Liang, X.; Wang, Y.; Meng, X.; Xu, Y.; Cai, S.; Wang, Z.; Liu, J.; Cai, G. MiR-139-5p Inhibits the Epithelial-Mesenchymal Transition and Enhances the Chemotherapeutic Sensitivity of Colorectal Cancer Cells by Downregulating BCL2. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef]
- Xu, X.; Chen, R.; Li, Z.; Huang, N.; Wu, X.; Li, S.; Li, Y.; Wu, S. MicroRNA-490-3p inhibits colorectal cancer metastasis by targeting TGFβR1. BMC Cancer 2015, 15, 1023. [Google Scholar] [CrossRef]
- Gugnoni, M.; Ciarrocchi, A. Long noncoding RNA and epithelial mesenchymal transition in cancer. Int. J. Mol. Sci. 2019, 20, 1924. [Google Scholar] [CrossRef]
- Ge, X.S.; Ma, H.J.; Zheng, X.H.; Ruan, H.L.; Liao, X.Y.; Xue, W.Q.; Chen, Y.B.; Zhang, Y.; Jia, W.H. HOTAIR, a prognostic factor in esophageal squamous cell carcinoma, inhibits WIF-1 expression and activates Wnt pathway. Cancer Sci. 2013, 104, 1675–1682. [Google Scholar] [CrossRef]
- Guinney, J.; Dienstmann, R.; Wang, X.; De Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Mooi, J.K.; Wirapati, P.; Asher, R.; Lee, C.K.; Savas, P.; Price, T.J.; Townsend, A.; Hardingham, J.; Buchanan, D.; Williams, D.; et al. The prognostic impact of consensus molecular subtypes (CMS) and its predictive effects for bevacizumab benefit in metastatic colorectal cancer: Molecular analysis of the AGITG MAX clinical trial. Ann. Oncol. 2018, 29, 2240–2246. [Google Scholar] [CrossRef] [PubMed]
- Stintzing, S.; Wirapati, P.; Lenz, H.J.; Neureiter, D.; Fischer von Weikersthal, L.; Decker, T.; Kiani, A.; Kaiser, F.; Al-Batran, S.; Heintges, T.; et al. Consensus molecular subgroups (CMS) of colorectal cancer (CRC) and first-line efficacy of FOLFIRI plus cetuximab or bevacizumab in the FIRE3 (AIO KRK-0306) trial. Ann. Oncol. 2019, 30, 1796–1803. [Google Scholar] [CrossRef]
- Sosa, V.; Moliné, T.; Somoza, R.; Paciucci, R.; Kondoh, H.; LLeonart, M.E. Oxidative stress and cancer: An overview. Ageing Res. Rev. 2013, 12, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Sorolla, M.A.; Reverter-Branchat, G.; Tamarit, J.; Ferrer, I.; Ros, J.; Cabiscol, E. Proteomic and oxidative stress analysis in human brain samples of Huntington disease. Free Radic. Biol. Med. 2008, 45, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Bermejo, R.; Hernández-Hernández, A. The importance of NADPH oxidases and redox signaling in angiogenesis. Antioxidants 2017, 6, 32. [Google Scholar] [CrossRef]
- Arbiser, J.L.; Petros, J.; Klafter, R.; Govindajaran, B.; McLaughlin, E.R.; Brown, L.F.; Cohen, C.; Moses, M.; Kilroy, S.; Arnold, R.S.; et al. Reactive oxygen generated by Nox1 triggers the angiogenic switch. Proc. Natl. Acad. Sci. USA 2002, 99, 715–720. [Google Scholar] [CrossRef]
- Weyemi, U.; Lagente-Chevallier, O.; Boufraqech, M.; Prenois, F.; Courtin, F.; Caillou, B.; Talbot, M.; Dardalhon, M.; Al Ghuzlan, A.; Bidart, J.M.; et al. ROS-generating NADPH oxidase NOX4 is a critical mediator in oncogenic H-Ras-induced DNA damage and subsequent senescence. Oncogene 2012, 31, 1117–1129. [Google Scholar] [CrossRef]
- Jiang, J.; Wang, K.; Chen, Y.; Chen, H.; Nice, E.C.; Huang, C. Redox regulation in tumor cell epithelial–mesenchymal transition: Molecular basis and therapeutic strategy. Signal Transduct. Target. Ther. 2017, 2, 17036. [Google Scholar] [CrossRef]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F. Preferred reporting items for a systematic review and meta-analysis of individual participant data: The PRISMA-IPD statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Raudvere, U.; Kolberg, L.; Kuzmin, I.; Arak, T.; Adler, P.; Peterson, H.; Vilo, J. G:Profiler: A web server for functional enrichment analysis and conversions of gene lists (2019 update). Nucleic Acids Res. 2019, 41, W191–W198. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PMID | First Author | Year | Predicted Endpoint | Included Variables in Multivariate Logistic Model | Design | Valitation Cohort | Total Number of Patients | Clinical Stage | Sample/Technique | Tissue Analyzed |
|---|---|---|---|---|---|---|---|---|---|---|
| 24752533 | Barbazan [23] | 2014 | OS, PFS | 4-week CTC marker model, baseline CTC marker model, ECOG performance status, lung metastasis | Unicentric | No | 50 | TNM: IV: 50 | CTC/RTqPCR | Colon and rectum |
| 24738665 | Gao [24] | 2014 | OS | ILEI expresssion, TNM stage, peritumoral deposits, lymphatic invasion, venous invasion | Unicentric | No | 194 | TNM: I: 55; II: 59, III: 74, IV: 6 | Tumor/IHC | Colon and rectum |
| 24217791 | Sugimachi [25] | 2014 | OS | Plastin 3 expression, pT, pN, lymphatic invasion, venous invasion, Dukes stage, CEA and CA19.9 levels | Unicentric | No | 177 | Dukes: A–B: 101; C–D: 76 | Tumor and blood/RTqPCR | Colon and rectum |
| 24840737 | Wu [26] | 2014 | OS, MFS | HOTAIR gene expression, pN, pM, AJCC stage, HG | Unicentric | No | 120 | TNM: I: 13, II: 44, III: 49, IV: 14 | Tumor/RTqPCR | Colon |
| 25431208 | Zhou [27] | 2014 | OS, PFS | OTUB1 expression, age, gender, tumor location, tumor size, pT, pN, pM, CEA levels, therapy | Unicentric | No | 260 | TNM: I: 61, II: 63, III: 76, IV: 60 | Tumor/IHC | Colon and rectum |
| 25382057 | Dawson [28] | 2015 | OS | mTrkB expression, pT, pN, adjuvant therapy | Unicentric | No | 211 | TN: I–III: 182, IV: 22, UNK: 7 | Tumor/IHC | Colon and rectum |
| 25951369 | Kahlert [29] | 2015 | OS | SIX1 expression, KRAS and MSI status, age, gender, HG, UICC stage, therapy | Multicentric | Yes Internal cohort: 817 patients | 945 | TNM: Cohort 1: I: 42,II: 45, III: 41.Cohort 2: I: 188, II: 314, III: 315 | Tumor/IHC, RTqPCR | Colon and rectum |
| 25947346 | Liu [30] | 2015 | OS, PFS | GDH expression, HG, pT, pN, pM, venous invasion, nervous invasion | Unicentric | No | 104 | TNM: I/II: 42, III/IV: 62 | Tumor/IHC | Colon and rectum |
| 25936636 | Yan [16] | 2015 | OS | N-cadherin and E-cadherin expression, age, gender, tumor location, HG, tumor size, pT, pN, pM | Unicentric | No | 102 | TNM: I–II–III: 53, IV: 49 | Tumor/IHC, RTqPCR | Colon and rectum |
| 25716692 | Xiao [31] | 2015 | OS | BTPF expression, vimentin expression, E-cadherin expression, age, gender, tumor size, HG, UICC stage, pN, pM, recurrence | Unicentric | No | 105 | TNM: I–II: 61, III–V: 44 | Tumor/IHC, RTqPCR | Colon and rectum |
| 26507436 | Busch [32] | 2016 | OS | E-cadherin and Snail expression | Multicentric | No | 190 | TNM: Local: 100 Regional: 66 Distant: 24 | Tumor/IHC | Colon and rectum |
| 27520310 | Gao [33] | 2016 | OS | DCLK1 expression, TNM stage, pM | Unicentric | No | 71 | TNM: I: 11, II: 17, III: 32, IV: 11 | Tumor/IHC RTqPCR | Colon and rectum |
| 27037526 | Hashimoto [34] | 2016 | OS, DFS | h-Prune expression, pN, pM, hepatectomy type, CEA and CA19-9 levels | Unicentric | No | 87 | TNM: IV: 87 | Tumor/IHC | Colon and rectum |
| 27537253 | Li [35] | 2016 | OS, PFS | Ki67 and MAEL expression, pT, pN, HG | Unicentric | No | 185 | TNM: I–II: 105, III: 80 | Tumor/IHC | Colon and rectum |
| 27323857 | Li [36] | 2016 | OS, MFS | PAK7 and Ki67 expression, age, gender, location, pT, pN, pM, AJCC stage, vascular invasion, HG | Unicentric | No | 203 | TNM: I: 24, II: 81, III: 80, IV: 18 | Tumor/IHC, RTqPCR | Colon |
| 27046094 | Luo [37] | 2016 | OS | Rab3D expression, pT, pN, pM and CEA levels | Unicentric | No | 300 | TNM: I: 48, II: 92, III: 103, IV: 7 | Tumor/IHC | Colon and rectum |
| 26983880 | Matsusaka [38] | 2016 | OS, PFS | TWIST1, SNAIL, ZEB1 and E-cadherin gene polymorphisms | Unicentric | No | 220 | TNM: Beva cohort: IV: 143 Cetu cohort: IV: 77 | Tumor/Sanger Seq | Colon and rectum |
| 27503579 | Ning [39] | 2016 | OS | ALDH1, PI3KCA and AKT2 gene expression in CTC’s | Unicentric | No | 78 | TNM: IV: 78 | CTC/RTqPCR | Colon and rectum |
| 27363678 | Satelli [40] | 2016 | OS, PFS | CTC counts, PD-L1 expression in CTC’s | Unicentric | No | 62 | TNM: IV: 62 | CTC/Flow cytometry, ICC | Colon |
| 26975699 | Shen [41] | 2016 | OS | S100P expression, CEA and CA19-9 levels, tumor size, HG, TNM stage | Unicentrico | No | 125 | TNM: I/II: 50 III/IV: 75 | Tumor/IHC RTqPCR | Colon |
| 27404020 | Teraoku [42] | 2016 | OS | HG, THBS1, Ki67 and E-cadherin expression | Unicentric | No | 94 | TNM: IV: 94 | Tumor/IHC | Colon and rectum |
| 27120783 | Woischke [43] | 2016 | CSS | CYB5R1 expression, age, gender, location, pT, HG | Unicentric | Yes: TCGA cohort: 457 patients | 678 | TNM: Dis cohort: I: 1, II: 35, III: 177, IV: 8 | Tumor/IHC | Colon and rectum |
| 27259250 | Yang [44] | 2016 | OS | GAPLINC gene expression, tumor size, pT, pN, HG | Unicentric | No | 180 | TNM: I: 13; II: 96, III: 66, IV: 3 | Tumor/ISH | Colon and rectum |
| 26370611 | Yokota [45] | 2016 | RFS | CTGF-CALD1-INHBA-TAGLN gene expression, PDLIM5-MAGL1-SPTBN-TAGLN gene expression and Dukes stage | Unicentric | Yes: Internal cohort: 113 patients | 339 | Dukes: Dis cohort: A: 41, B: 94, C: 91 TNM: Val cohort: I: 18, II: 45, III: 42, IV: 8 | Tumor and SPF/RTqPCR | Colon |
| 28864720 | Chen [46] | 2017 | OS, MFS | TrpC5 expression, AJCC stage, HG | Unicentric | No | 127 | TNM: I: 17, II: 52, III: 45, IV: 13 | Tumor/IHC | Colon |
| 28716573 | Forse [47] | 2017 | OS DFS | sHtrA3 expression, gender, pT, pN, tumor location, lymphovascular invasion | Unicentric | No | 172 | TNM: II: 172 | Tumor/IHC | Colon and rectum |
| 27629879 | Lu [48] | 2017 | OS | PANDAR gene expression, pT, TNM stage | Unicentric | No | 124 | TNM: I/II: 46 III/IV: 78 | Tumor/RTqPCR | Colon and rectum |
| 28262692 | Miyoshi [49] | 2017 | RFS | miR-139-5p gene expression, pT, pN | Multicentric | Yes: Internal cohorts 1 and 2 = 111 and 139 patients | 497 | TNM: Dis cohorts: MC: III: 100; TCGA: II: 42, III: 105; Val cohorts: Cohort 1: II: 60, III: 50 Cohort 2: I: 12, II: 67, III: 60 | Tumor and blood/RTqPCR | Colon and rectum |
| 27966450 | Wang [50] | 2017 | OS | NNT-AS1 gene expression, TNM stage, vascular invasion | Unicentric | No | 70 | TNM: I/II: 36 III/IV: 34 | Tumor/RTqPCR | Colon and rectum |
| 28104986 | Yusup [51] | 2017 | OS | TFF1, TFF3, TWIST1 expression, age, gender, histopathological type, HG, pT, pN, pM, TNM stage | Unicentric | No | 75 | TNM: I: 15, II: 27, III:27, IV: 6 | Tumor/IHC | Colon and rectum |
| 28356111 | Zhao [52] | 2017 | OS, DFS | CXCL5 expression, Dukes stage | Unicentric | No | 78 | TNM I: 15, II: 43, III: 24, IV: 6 | Tumor/IHC, RTqPCR | Colon and rectum |
| 29781053 | Cho [53] | 2018 | OS | NOX1, NOX2, NOX3, NOX4, NOX5, DUOX1, DUOX2 gene expression | Unicentric | No | 458 | TNM: I: 76, II: 178, III: 129, IV: 65, UNK: 10 | Tumor/microaray mRNA expression | Colon and rectum |
| 30100393 | Hu [54] | 2018 | OS, PFS | ITGAE and TIL expression, TNM stage, pT, pN, pM, perineural invasion, vascular invasion, CEA levels | Unicentric | Yes: Internal cohort: 276 patients | 1154 | TNM: Val cohort: I: 21, II: 81, III: 132, IV: 42 | Tumor/IHC | Colon and rectum |
| 29892782 | Konishi [55] | 2018 | OS | hCGBb expression, vascular invasion, tumor budding | Unicentric | No | 80 | TNM: I–II: 53, III: 27 | Tumor/IHC | Colon and rectum |
| 29956813 | Liu [56] | 2018 | OS | TRIM58 expression, age, gender, therapy, HG, pT, pN, pM | Unicentric | Yes: Internal cohort: 152 patients | 313 | TNM: Val cohort: I: 26, II: 63, III: 59, IV:1, UNK: 3 | Tumor/RTqPCR | Colon and rectum |
| 29949050 | Wang [57] | 2018 | OS, PFS | Total CTC count, mesenchymal CTC count, LGR5 gene expression in CTC | Unicentric | No | 66 | TNM: I: 31, II: 15, III–IV: 20 | CTC/ISH | Colon and rectum |
| 29916545 | Wang [58] | 2018 | OS | miR-490-3p and RAB14 gene expression, age, gender, tumor size, HG, TNM stage, pN, pM | Unicentric | No | 50 | TNM: I–II: 23, III–IV: 27 | Tumor/RTqPCR | Colon and rectum |
| 30170017 | Yang [59] | 2018 | OS, PFS | Tenascin-C expression, age, pT, pN, pM | Unicentric | No | 100 | TNM: I: 8, II: 38, III: 21, IV: 33 | Tumor/IHC | Colon and rectum |
| 30021598 | Zhu [60] | 2018 | OS | MACC1, CD44, TWIST1 and KISS-1 expression, pN, TNM stage | Unicentric | No | 212 | TNM: I: 69, II: 67; III: 76 | Tumor/IHC | Colon |
| Clinical and Histological Markers | Predicted Variable | HR (95%CI) | Z (p-Value) | I2 (%) | Heterogeneity p-Value | Number of Studies/Cohorts | Number of Participants | Statistical Effect Model |
|---|---|---|---|---|---|---|---|---|
| pT (T3–T4 vs. T1–T2) | OS | 1.74 (1.07–2.83) | 0.03 | 94 | <0.01 | 14/14 | 2449 | Random |
| PFS | 1.53 (1.12–2.08) | <0.01 | 0 | 0.97 | 6/6 | 1196 | Fixed | |
| pN (N1–N2 vs. N0) | OS | 2.33 (1.72–3.14) | <0.01 | 72 | <0.01 | 19/19 | 3453 | Random |
| PFS | 2.79 (1.70–4.56) | <0.01 | 84 | <0.01 | 10/11 | 1757 | Random | |
| pM (M1 vs. M0) | OS | 3.48 (2.49–4.85) | <0.01 | 54 | <0.01 | 14/14 | 1968 | Random |
| PFS | 3.30 (2.11–5.18) | <0.01 | 56 | 0.03 | 7/7 | 113 | Random | |
| pStage (III–IV vs. I–II) | OS | 2.73 (2.37–3.14) | <0.01 | 28 | 0.10 | 21/23 | 3769 | Fixed |
| PFS | 3.19 (2.21–4.61) | <0.01 | 0 | 0.55 | 6/7 | 1054 | Fixed | |
| Lymphovascular Invasion (present vs. absent) | OS | 1.63 (1.12–2.37) | 0.01 | 71 | <0.01 | 9/10 | 1638 | Random |
| PFS | 1.53 (1.19–1.95) | <0.01 | 49 | 0.12 | 4/4 | 836 | Fixed | |
| Histological Grade (high vs. intermediate-low) | OS | 1.70 (1.47–1.97) | <0.01 | 7 | 0.37 | 14/15 | 2694 | Fixed |
| PFS | 2.29 (1.61–3.24) | <0.01 | 0 | 0.88 | 4/4 | 635 | Fixed | |
| Tumor location (left vs. right) | OS | 0.79 (0.33–1.88) | 0.6 | 74 | 0.02 | 2/3 | 578 | Random |
| Tumor location (rectum vs. colon) | OS | 1.75 (0.85–1.88) | 0.13 | 79 | 0.008 | 3/3 | 583 | Random |
| Tumor size (>2 vs. ≤2 cm) | OS | 1.00 (0.70–1.43) | 0.99 | 55 | 0.05 | 6/6 | 822 | Random |
| Chemotherapy (yes vs. no) | OS | 0.46 (0.27–0.76) | <0.01 | 61 | 0.05 | 4/4 | 1440 | Random |
| CEA (elevated vs. normal) | OS | 1.33 (1.10–1.61) | <0.01 | 0 | 0.55 | 6/6 | 1225 | Fixed |
| PFS | 1.48 (1.11–1.99) | <0.01 | 0 | 0.65 | 3/3 | 623 | Fixed | |
| CA19.9 (elevated vs. normal) | OS | 1.21 (0.90–1.62) | 0.21 | 56 | 0.10 | 3/3 | 389 | Random |
| E–cadherin (low vs. high) | OS | 1.84 (1.21–2.78) | <0.01 | 0 | 0.95 | 4/4 | 491 | Fixed |
| Ki67 (high vs. low) | OS | 1.30 (0.95–1.76) | 0.10 | 0 | 0.55 | 3/3 | 482 | Fixed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisi, E.; Sorolla, A.; Montal, R.; González-Resina, R.; Novell, A.; Salud, A.; Sorolla, M.A. Prognostic Factors Involved in the Epithelial–Mesenchymal Transition Process in Colorectal Cancer Have a Preponderant Role in Oxidative Stress: A Systematic Review and Meta-Analysis. Cancers 2020, 12, 3330. https://doi.org/10.3390/cancers12113330
Parisi E, Sorolla A, Montal R, González-Resina R, Novell A, Salud A, Sorolla MA. Prognostic Factors Involved in the Epithelial–Mesenchymal Transition Process in Colorectal Cancer Have a Preponderant Role in Oxidative Stress: A Systematic Review and Meta-Analysis. Cancers. 2020; 12(11):3330. https://doi.org/10.3390/cancers12113330
Chicago/Turabian StyleParisi, Eva, Anabel Sorolla, Robert Montal, Rita González-Resina, Anna Novell, Antonieta Salud, and Maria Alba Sorolla. 2020. "Prognostic Factors Involved in the Epithelial–Mesenchymal Transition Process in Colorectal Cancer Have a Preponderant Role in Oxidative Stress: A Systematic Review and Meta-Analysis" Cancers 12, no. 11: 3330. https://doi.org/10.3390/cancers12113330
APA StyleParisi, E., Sorolla, A., Montal, R., González-Resina, R., Novell, A., Salud, A., & Sorolla, M. A. (2020). Prognostic Factors Involved in the Epithelial–Mesenchymal Transition Process in Colorectal Cancer Have a Preponderant Role in Oxidative Stress: A Systematic Review and Meta-Analysis. Cancers, 12(11), 3330. https://doi.org/10.3390/cancers12113330