Liquid Biopsy for Solid Ophthalmic Malignancies: An Updated Review and Perspectives

 ,
,  , ,
, , 
Simple Summary
Abstract
1. Introduction
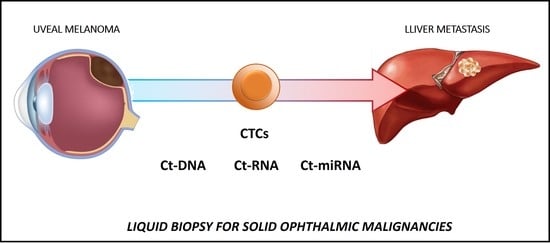
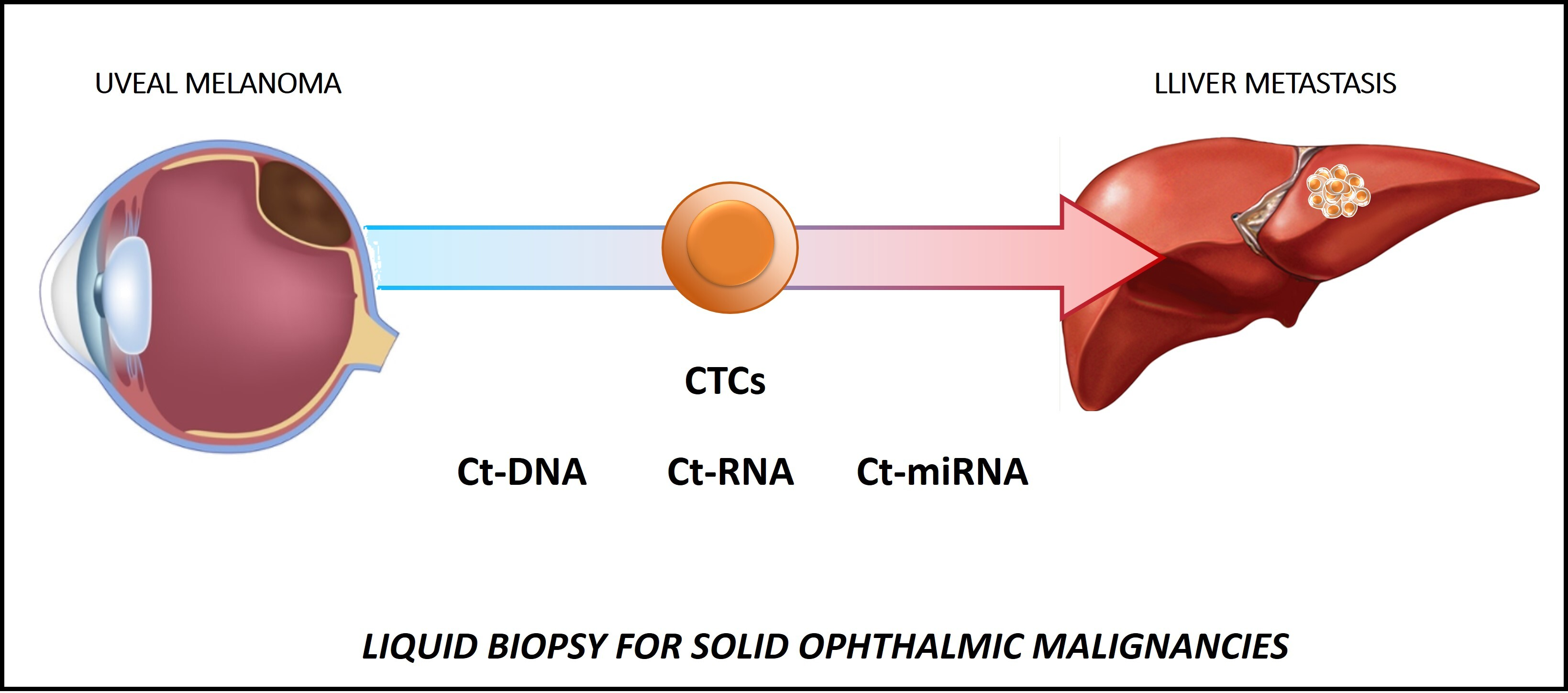
2. Liquid Biopsy in Uveal Melanoma (UM)
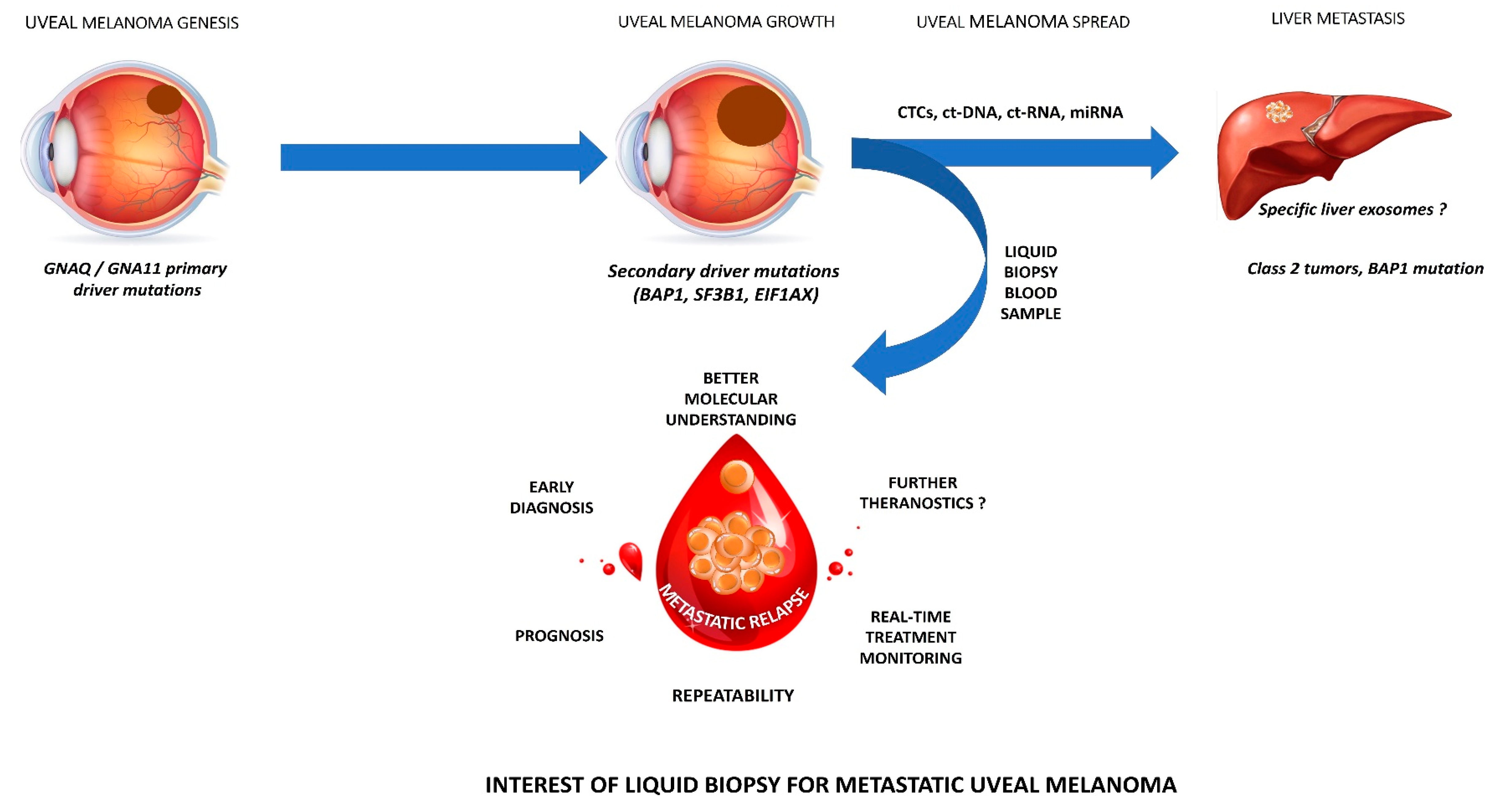
2.1. Molecular Characteristics of UM
2.2. CTCs
2.2.1. CTC Isolation and Identification
2.2.2. Main Clinical Findings
2.3. Ct-DNA and ct-RNA
2.3.1. Ct-DNA and ct-RNA Detection
2.3.2. Main Clinical Findings
2.4. Non-Coding RNAs
2.4.1. Non-Coding RNAs Detection
2.4.2. Main Clinical Findings
2.5. Tumor-Related Exosomes (TREs)
2.5.1. TRE Detection
2.5.2. Main Clinical Findings
2.6. Tumor-Educated Platelets (TEPs)
2.7. Future Perspectives: Towards a Better UM Understanding?
2.8. Limitations
2.9. Conclusion
3. Retinoblastoma (RB)
4. LB in Conjunctival Malignancies
5. LB in Choroidal Metastases
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Scarlotta, M.; Simsek, C.; Kim, A.K. Liquid Biopsy in Solid Malignancy. Genet. Test. Mol. Biomark. 2019, 23, 284–296. [Google Scholar] [CrossRef] [PubMed]
- AlAli, A.; Kletke, S.; Gallie, B.; Lam, W.-C. Retinoblastoma for Pediatric Ophthalmologists. Asia Pac. J. Ophthalmol. 2018, 7, 160–168. [Google Scholar] [CrossRef]
- León-Mateos, L.; Vieito, M.; Anido, U.; López López, R.; Muinelo Romay, L. Clinical Application of Circulating Tumour Cells in Prostate Cancer: From Bench to Bedside and Back. Int. J. Mol. Sci. 2016, 17, 1580. [Google Scholar] [CrossRef]
- Payne, K.; Brooks, J.; Spruce, R.; Batis, N.; Taylor, G.; Nankivell, P.; Mehanna, H. Circulating Tumour Cell Biomarkers in Head and Neck Cancer: Current Progress and Future Prospects. Cancers 2019, 11, 1115. [Google Scholar] [CrossRef]
- Hofman, P. Liquid biopsy for early detection of lung cancer. Curr. Opin. Oncol. 2017, 29, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.L.; Xu, L.; Polski, A.; Jubran, R.; Kuhn, P.; Kim, J.W.; Hicks, J. Aqueous Humor Is Superior to Blood as a Liquid Biopsy for Retinoblastoma. Ophthalmology 2020, 127, 552–554. [Google Scholar] [CrossRef]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal melanoma: Trends in incidence, treatment, and survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef]
- Cohen, V.M.; Dinakaran, S.; Parsons, M.A.; Rennie, I.G. Transvitreal fine needle aspiration biopsy: The influence of intraocular lesion size on diagnostic biopsy result. Eye 2001, 15, 143–147. [Google Scholar] [CrossRef]
- Eide, N.; Walaas, L. Fine-needle aspiration biopsy and other biopsies in suspected intraocular malignant disease: A review. Acta Ophthalmol. 2009, 87, 588–601. [Google Scholar] [CrossRef]
- Bensoussan, E.; Thariat, J.; Maschi, C.; Delas, J.; Schouver, E.D.; Hérault, J.; Baillif, S.; Caujolle, J.-P. Outcomes after Proton Beam Therapy for Large Choroidal Melanomas in 492 Patients. Am. J. Ophthalmol. 2016, 165, 78–87. [Google Scholar] [CrossRef]
- Sellam, A.; Desjardins, L.; Barnhill, R.; Plancher, C.; Asselain, B.; Savignoni, A.; Pierron, G.; Cassoux, N. Fine Needle Aspiration Biopsy in Uveal Melanoma: Technique, Complications, and Outcomes. Am. J. Ophthalmol. 2016, 162, 28–34. [Google Scholar] [CrossRef]
- Onken, M.D.; Worley, L.A.; Char, D.H.; Augsburger, J.J.; Correa, Z.M.; Nudleman, E.; Aaberg, T.M.; Altaweel, M.M.; Bardenstein, D.S.; Finger, P.T.; et al. Collaborative Ocular Oncology Group report number 1: Prospective validation of a multi-gene prognostic assay in uveal melanoma. Ophthalmology 2012, 119, 1596–1603. [Google Scholar] [CrossRef]
- Kujala, E.; Mäkitie, T.; Kivelä, T. Very long-term prognosis of patients with malignant uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef]
- Shields, C.L.; Say, E.A.T.; Hasanreisoglu, M.; Saktanasate, J.; Lawson, B.M.; Landy, J.E.; Badami, A.U.; Sivalingam, M.D.; Hauschild, A.J.; House, R.J.; et al. Personalized Prognosis of Uveal Melanoma Based on Cytogenetic Profile in 1059 Patients over an 8-Year Period. Ophthalmology 2017, 124, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Goh, A.Y.; Layton, C.J. Evolving systemic targeted therapy strategies in uveal melanoma and implications for ophthalmic management: A review. Clin. Exp. Ophthalmol. 2016, 44, 509–519. [Google Scholar] [CrossRef]
- Xu, L.T.; Funchain, P.F.; Bena, J.F.; Li, M.; Tarhini, A.; Berber, E.; Singh, A.D. Uveal Melanoma Metastatic to the Liver: Treatment Trends and Outcomes. Ocul. Oncol. Pathol. 2019, 5, 323–332. [Google Scholar] [CrossRef]
- Shoushtari, A.N.; Carvajal, R.D. Treatment of Uveal Melanoma. Cancer Treat. Res. 2016, 167, 281–293. [Google Scholar] [CrossRef]
- Bande Rodríguez, M.F.; Fernandez Marta, B.; Lago Baameiro, N.; Santiago-Varela, M.; Silva-Rodríguez, P.; Blanco-Teijeiro, M.J.; Pardo Perez, M.; Piñeiro Ces, A. Blood Biomarkers of Uveal Melanoma: Current Perspectives. Clin. Ophthalmol. 2020, 14, 157–169. [Google Scholar] [CrossRef]
- Onken, M.D.; Worley, L.A.; Long, M.D.; Duan, S.; Council, M.L.; Bowcock, A.M.; Harbour, J.W. Oncogenic mutations in GNAQ occur early in uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5230–5234. [Google Scholar] [CrossRef]
- Pandiani, C.; Béranger, G.E.; Leclerc, J.; Ballotti, R.; Bertolotto, C. Focus on cutaneous and uveal melanoma specificities. Genes Dev. 2017, 31, 724–743. [Google Scholar] [CrossRef]
- Smit, K.N.; Jager, M.J.; de Klein, A.; Kiliç, E. Uveal melanoma: Towards a molecular understanding. Prog. Retin. Eye Res. 2020, 75, 100800. [Google Scholar] [CrossRef]
- Trolet, J.; Hupé, P.; Huon, I.; Lebigot, I.; Decraene, C.; Delattre, O.; Sastre-Garau, X.; Saule, S.; Thiéry, J.-P.; Plancher, C.; et al. Genomic profiling and identification of high-risk uveal melanoma by array CGH analysis of primary tumors and liver metastases. Investig. Ophthalmol. Vis. Sci. 2009, 50, 2572–2580. [Google Scholar] [CrossRef] [PubMed]
- Harbour, J.W.; Onken, M.D.; Roberson, E.D.O.; Duan, S.; Cao, L.; Worley, L.A.; Council, M.L.; Matatall, K.A.; Helms, C.; Bowcock, A.M. Frequent mutation of BAP1 in metastasizing uveal melanomas. Science 2010, 330, 1410–1413. [Google Scholar] [CrossRef]
- Nahon-Esteve, S.; Martel, A.; Maschi, C.; Caujolle, J.-P.; Baillif, S.; Lassalle, S.; Hofman, P. The Molecular Pathology of Eye Tumors: A 2019 Update Main Interests for Routine Clinical Practice. Curr. Mol. Med. 2019, 19, 632–664. [Google Scholar] [CrossRef]
- Rodrigues, M.; Rais, K.A.; Salviat, F.; Algret, N.; Simaga, F.; Barnhill, R.; Gardrat, S.; Servois, V.; Mariani, P.; Piperno-Neumann, S.; et al. Association of Partial Chromosome 3 Deletion in Uveal Melanomas with Metastasis-Free Survival. JAMA Ophthalmol. 2020. [Google Scholar] [CrossRef]
- Onken, M.D.; Worley, L.A.; Ehlers, J.P.; Harbour, J.W. Gene expression profiling in uveal melanoma reveals two molecular classes and predicts metastatic death. Cancer Res. 2004, 64, 7205–7209. [Google Scholar] [CrossRef]
- Hwang, W.L.; Hwang, K.L.; Miyamoto, D.T. The promise of circulating tumor cells for precision cancer therapy. Biomark. Med. 2016, 10, 1269–1285. [Google Scholar] [CrossRef] [PubMed]
- Mader, S.; Pantel, K. Liquid Biopsy: Current Status and Future Perspectives. Oncol. Res. Treat. 2017, 40, 404–408. [Google Scholar] [CrossRef]
- Anand, K.; Roszik, J.; Gombos, D.; Upshaw, J.; Sarli, V.; Meas, S.; Lucci, A.; Hall, C.; Patel, S. Pilot Study of Circulating Tumor Cells in Early-Stage and Metastatic Uveal Melanoma. Cancers 2019, 11, 856. [Google Scholar] [CrossRef]
- Tura, A.; Merz, H.; Reinsberg, M.; Lüke, M.; Jager, M.J.; Grisanti, S.; Lüke, J. Analysis of monosomy-3 in immunomagnetically isolated circulating melanoma cells in uveal melanoma patients. Pigment Cell Melanoma Res. 2016, 29, 583–589. [Google Scholar] [CrossRef]
- Bande, M.F.; Santiago, M.; Muinelo-Romay, L.; Blanco, M.J.; Mera, P.; Capeans, C.; Pardo, M.; Piñeiro, A. Detection of circulating melanoma cells in choroidal melanocytic lesions. BMC Res. Notes 2015, 8, 452. [Google Scholar] [CrossRef]
- Terai, M.; Mu, Z.; Eschelman, D.J.; Gonsalves, C.F.; Kageyama, K.; Chervoneva, I.; Orloff, M.; Weight, R.; Mastrangelo, M.J.; Cristofanilli, M.; et al. Arterial Blood, Rather Than Venous Blood, is a Better Source for Circulating Melanoma Cells. EBioMedicine 2015, 2, 1821–1826. [Google Scholar] [CrossRef]
- Tura, A.; Lüke, J.; Merz, H.; Reinsberg, M.; Lüke, M.; Jager, M.J.; Grisanti, S. Identification of circulating melanoma cells in uveal melanoma patients by dual-marker immunoenrichment. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4395–4404. [Google Scholar] [CrossRef]
- Mazzini, C.; Pinzani, P.; Salvianti, F.; Scatena, C.; Paglierani, M.; Ucci, F.; Pazzagli, M.; Massi, D. Circulating tumor cells detection and counting in uveal melanomas by a filtration-based method. Cancers 2014, 6, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.-C.; Madic, J.; Mariani, P.; Piperno-Neumann, S.; Rampanou, A.; Servois, V.; Cassoux, N.; Desjardins, L.; Milder, M.; Vaucher, I.; et al. Detection rate and prognostic value of circulating tumor cells and circulating tumor DNA in metastatic uveal melanoma. Int. J. Cancer 2014, 134, 1207–1213. [Google Scholar] [CrossRef]
- Pinzani, P.; Mazzini, C.; Salvianti, F.; Massi, D.; Grifoni, R.; Paoletti, C.; Ucci, F.; Molinara, E.; Orlando, C.; Pazzagli, M.; et al. Tyrosinase mRNA levels in the blood of uveal melanoma patients: Correlation with the number of circulating tumor cells and tumor progression. Melanoma Res. 2010, 20, 303–310. [Google Scholar] [CrossRef]
- Suesskind, D.; Ulmer, A.; Schiebel, U.; Fierlbeck, G.; Spitzer, B.; Spitzer, M.S.; Bartz-Schmidt, K.U.; Grisanti, S. Circulating melanoma cells in peripheral blood of patients with uveal melanoma before and after different therapies and association with prognostic parameters: A pilot study. Acta Ophthalmol. 2011, 89, 17–24. [Google Scholar] [CrossRef]
- Eide, N.; Faye, R.S.; Høifødt, H.K.; Øvergaard, R.; Jebsen, P.; Kvalheim, G.; Fodstad, Ø. Immunomagnetic detection of micrometastatic cells in bone marrow in uveal melanoma patients. Acta Ophthalmol. 2009, 87, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Ulmer, A.; Beutel, J.; Süsskind, D.; Hilgers, R.-D.; Ziemssen, F.; Lüke, M.; Röcken, M.; Rohrbach, M.; Fierlbeck, G.; Bartz-Schmidt, K.-U.; et al. Visualization of circulating melanoma cells in peripheral blood of patients with primary uveal melanoma. Clin. Cancer Res. 2008, 14, 4469–4474. [Google Scholar] [CrossRef]
- Kang, J.S.; Lee, T.R.; Cha, W.C.; Shin, T.G.; Sim, M.S.; Jo, I.J.; Song, K.J.; Rhee, J.E.; Jeong, Y.K. Finger necrosis after accidental radial artery puncture. Clin. Exp. Emerg. Med. 2014, 1, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Manalac, J.; Das, C.; Ferguson, K.; Shields, J.A. Choroidal melanoma: Clinical features, classification, and top 10 pseudomelanomas. Curr. Opin. Ophthalmol. 2014, 25, 177–185. [Google Scholar] [CrossRef]
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.J.; Uhr, J.W.; Terstappen, L.W.M.M. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef]
- Poulet, G.; Massias, J.; Taly, V. Liquid Biopsy: General Concepts. Acta Cytol. 2019, 63, 449–455. [Google Scholar] [CrossRef]
- Cabel, L.; Riva, F.; Servois, V.; Livartowski, A.; Daniel, C.; Rampanou, A.; Lantz, O.; Romano, E.; Milder, M.; Buecher, B.; et al. Circulating tumor DNA changes for early monitoring of anti-PD1 immunotherapy: A proof-of-concept study. Ann. Oncol. 2017, 28, 1996–2001. [Google Scholar] [CrossRef]
- Maheswaran, S.; Sequist, L.V.; Nagrath, S.; Ulkus, L.; Brannigan, B.; Collura, C.V.; Inserra, E.; Diederichs, S.; Iafrate, A.J.; Bell, D.W.; et al. Detection of mutations in EGFR in circulating lung-cancer cells. N. Engl. J. Med. 2008, 359, 366–377. [Google Scholar] [CrossRef]
- Charitoudis, G.; Schuster, R.; Joussen, A.M.; Keilholz, U.; Bechrakis, N.E. Detection of tumour cells in the bloodstream of patients with uveal melanoma: Influence of surgical manipulation on the dissemination of tumour cells in the bloodstream. Br. J. Ophthalmol. 2016, 100, 468–472. [Google Scholar] [CrossRef]
- Metz, C.H.; Scheulen, M.; Bornfeld, N.; Lohmann, D.; Zeschnigk, M. Ultradeep sequencing detects GNAQ and GNA11 mutations in cell-free DNA from plasma of patients with uveal melanoma. Cancer Med. 2013, 2, 208–215. [Google Scholar] [CrossRef]
- Schuster, R.; Bechrakis, N.E.; Stroux, A.; Busse, A.; Schmittel, A.; Thiel, E.; Foerster, M.H.; Keilholz, U. Prognostic relevance of circulating tumor cells in metastatic uveal melanoma. Oncology 2011, 80, 57–62. [Google Scholar] [CrossRef]
- Schuster, R.; Bechrakis, N.E.; Stroux, A.; Busse, A.; Schmittel, A.; Scheibenbogen, C.; Thiel, E.; Foerster, M.H.; Keilholz, U. Circulating tumor cells as prognostic factor for distant metastases and survival in patients with primary uveal melanoma. Clin. Cancer Res. 2007, 13, 1171–1178. [Google Scholar] [CrossRef]
- Callejo, S.A.; Antecka, E.; Blanco, P.L.; Edelstein, C.; Burnier, M.N. Identification of circulating malignant cells and its correlation with prognostic factors and treatment in uveal melanoma. A prospective longitudinal study. Eye 2007, 21, 752–759. [Google Scholar] [CrossRef]
- Boldin, I.; Langmann, G.; Richtig, E.; Schwantzer, G.; Ardjomand, N.; Wegscheider, B.; El-Shabrawi, Y. Five-year results of prognostic value of tyrosinase in peripheral blood of uveal melanoma patients. Melanoma Res. 2005, 15, 503–507. [Google Scholar] [CrossRef]
- Keilholz, U.; Goldin-Lang, P.; Bechrakis, N.E.; Max, N.; Letsch, A.; Schmittel, A.; Scheibenbogen, C.; Heufelder, K.; Eggermont, A.; Thiel, E. Quantitative detection of circulating tumor cells in cutaneous and ocular melanoma and quality assessment by real-time reverse transcriptase-polymerase chain reaction. Clin. Cancer Res. 2004, 10, 1605–1612. [Google Scholar] [CrossRef]
- Junqueira-Neto, S.; Batista, I.A.; Costa, J.L.; Melo, S.A. Liquid Biopsy beyond Circulating Tumor Cells and Cell-Free DNA. Acta Cytol. 2019, 63, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yu, X.; Shen, J.; Jiang, Y. MicroRNA dysregulation in uveal melanoma: A new player enters the game. Oncotarget 2015, 6, 4562–4568. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Dutta, A. MicroRNAs in Cancer. Available online: https://pubmed.ncbi.nlm.nih.gov/18817506/?from_term=micro+rna+cancer+review&from_pos=4 (accessed on 9 May 2020).
- Xin, X.; Zhang, Y.; Ling, F.; Wang, L.; Sheng, X.; Qin, L.; Zhao, X. Identification of a nine-miRNA signature for the prognosis of Uveal Melanoma. Exp. Eye Res. 2019, 180, 242–249. [Google Scholar] [CrossRef]
- Stark, M.S.; Gray, E.S.; Isaacs, T.; Chen, F.K.; Millward, M.; McEvoy, A.; Zaenker, P.; Ziman, M.; Soyer, H.P.; Glasson, W.J.; et al. A Panel of Circulating MicroRNAs Detects Uveal Melanoma With High Precision. Transl. Vis. Sci. Technol. 2019, 8, 12. [Google Scholar] [CrossRef]
- Ragusa, M.; Barbagallo, C.; Statello, L.; Caltabiano, R.; Russo, A.; Puzzo, L.; Avitabile, T.; Longo, A.; Toro, M.D.; Barbagallo, D.; et al. miRNA profiling in vitreous humor, vitreal exosomes and serum from uveal melanoma patients: Pathological and diagnostic implications. Cancer Biol. Ther. 2015, 16, 1387–1396. [Google Scholar] [CrossRef]
- Achberger, S.; Aldrich, W.; Tubbs, R.; Crabb, J.W.; Singh, A.D.; Triozzi, P.L. Circulating immune cell and microRNA in patients with uveal melanoma developing metastatic disease. Mol. Immunol. 2014, 58, 182–186. [Google Scholar] [CrossRef]
- Joshi, P.; Kooshki, M.; Aldrich, W.; Varghai, D.; Zborowski, M.; Singh, A.D.; Triozzi, P.L. Expression of natural killer cell regulatory microRNA by uveal melanoma cancer stem cells. Clin. Exp. Metastasis 2016, 33, 829–838. [Google Scholar] [CrossRef]
- Russo, A.; Caltabiano, R.; Longo, A.; Avitabile, T.; Franco, L.M.; Bonfiglio, V.; Puzzo, L.; Reibaldi, M. Increased Levels of miRNA-146a in Serum and Histologic Samples of Patients with Uveal Melanoma. Front. Pharmacol. 2016, 7, 424. [Google Scholar] [CrossRef]
- Gómez-Pérez, A.M.; Cornejo Pareja, I.M.; García Alemán, J.; Coín Aragüez, L.; Sebastián Ochoa, A.; Alcaide Torres, J.; Molina Vega, M.; Clu Fernández, C.; Mancha Doblas, I.; Tinahones, F.J. New molecular biomarkers in differentiated thyroid carcinoma: Impact of miR-146, miR-221 and miR-222 levels in the evolution of the disease. Clin. Endocrinol. 2019, 91, 187–194. [Google Scholar] [CrossRef]
- Aksenenko, M.; Palkina, N.; Komina, A.; Tashireva, L.; Ruksha, T. Differences in microRNA expression between melanoma and healthy adjacent skin. BMC Dermatol. 2019, 19, 1. [Google Scholar] [CrossRef]
- Triozzi, P.L.; Achberger, S.; Aldrich, W.; Singh, A.D.; Grane, R.; Borden, E.C. The association of blood angioregulatory microRNA levels with circulating endothelial cells and angiogenic proteins in patients receiving dacarbazine and interferon. J. Transl. Med. 2012, 10, 241. [Google Scholar] [CrossRef]
- Worley, L.A.; Long, M.D.; Onken, M.D.; Harbour, J.W. Micro-RNAs associated with metastasis in uveal melanoma identified by multiplexed microarray profiling. Melanoma Res. 2008, 18, 184–190. [Google Scholar] [CrossRef]
- Yan, D.; Zhou, X.; Chen, X.; Hu, D.-N.; Dong, X.D.; Wang, J.; Lu, F.; Tu, L.; Qu, J. MicroRNA-34a inhibits uveal melanoma cell proliferation and migration through downregulation of c-Met. Investig. Ophthalmol. Vis. Sci. 2009, 50, 1559–1565. [Google Scholar] [CrossRef]
- Dong, F.; Lou, D. MicroRNA-34b/c suppresses uveal melanoma cell proliferation and migration through multiple targets. Mol. Vis. 2012, 18, 537–546. [Google Scholar]
- Eedunuri, V.K.; Rajapakshe, K.; Fiskus, W.; Geng, C.; Chew, S.A.; Foley, C.; Shah, S.S.; Shou, J.; Mohamed, J.S.; Coarfa, C.; et al. miR-137 Targets p160 Steroid Receptor Coactivators SRC1, SRC2, and SRC3 and Inhibits Cell Proliferation. Mol. Endocrinol. 2015, 29, 1170–1183. [Google Scholar] [CrossRef]
- Chen, X.; Wang, J.; Shen, H.; Lu, J.; Li, C.; Hu, D.-N.; Dong, X.D.; Yan, D.; Tu, L. Epigenetics, microRNAs, and carcinogenesis: Functional role of microRNA-137 in uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1193–1199. [Google Scholar] [CrossRef] [PubMed]
- Cheli, Y.; Giuliano, S.; Guiliano, S.; Botton, T.; Rocchi, S.; Hofman, V.; Hofman, P.; Bahadoran, P.; Bertolotto, C.; Ballotti, R. Mitf is the key molecular switch between mouse or human melanoma initiating cells and their differentiated progeny. Oncogene 2011, 30, 2307–2318. [Google Scholar] [CrossRef]
- Wu, S.; Chen, H.; Han, N.; Zhang, C.; Yan, H. Long Noncoding RNA PVT1 Silencing Prevents the Development of Uveal Melanoma by Impairing MicroRNA-17-3p-Dependent MDM2 Upregulation. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4904–4914. [Google Scholar] [CrossRef]
- Xu, H.; Gong, J.; Liu, H. High expression of lncRNA PVT1 independently predicts poor overall survival in patients with primary uveal melanoma. PLoS ONE 2017, 12, e0189675. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; He, J.; Yang, Z.; Ge, S.; Zhang, H.; Zhong, Q.; Fan, X. ZNNT1 long noncoding RNA induces autophagy to inhibit tumorigenesis of uveal melanoma by regulating key autophagy gene expression. Autophagy 2019, 1–14. [Google Scholar] [CrossRef]
- Zheng, X.; Tang, H.; Zhao, X.; Sun, Y.; Jiang, Y.; Liu, Y. Long non-coding RNA FTH1P3 facilitates uveal melanoma cell growth and invasion through miR-224-5p. PLoS ONE 2017, 12, e0184746. [Google Scholar] [CrossRef]
- Sun, L.; Sun, P.; Zhou, Q.-Y.; Gao, X.; Han, Q. Long noncoding RNA MALAT1 promotes uveal melanoma cell growth and invasion by silencing of miR-140. Am. J. Transl. Res. 2016, 8, 3939–3946. [Google Scholar]
- Lu, Q.; Zhao, N.; Zha, G.; Wang, H.; Tong, Q.; Xin, S. LncRNA HOXA11-AS Exerts Oncogenic Functions by Repressing p21 and miR-124 in Uveal Melanoma. DNA Cell Biol. 2017, 36, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Ma, R.; Ren, H.; Qian, J. Genome-Wide Analysis of Uveal Melanoma Metastasis-Associated LncRNAs and Their Functional Network. DNA Cell Biol. 2018, 37, 99–108. [Google Scholar] [CrossRef]
- Weidle, U.H.; Birzele, F.; Kollmorgen, G.; Rüger, R. The Multiple Roles of Exosomes in Metastasis. Cancer Genom. Proteom. 2017, 14, 1–15. [Google Scholar] [CrossRef]
- Eldh, M.; Olofsson Bagge, R.; Lässer, C.; Svanvik, J.; Sjöstrand, M.; Mattsson, J.; Lindnér, P.; Choi, D.-S.; Gho, Y.S.; Lötvall, J. MicroRNA in exosomes isolated directly from the liver circulation in patients with metastatic uveal melanoma. BMC Cancer 2014, 14, 962. [Google Scholar] [CrossRef]
- Giovannucci, E.; Egan, K.M.; Hunter, D.J.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C.; Speizer, F.E. Aspirin and the risk of colorectal cancer in women. N. Engl. J. Med. 1995, 333, 609–614. [Google Scholar] [CrossRef]
- Simon, T.G.; Duberg, A.-S.; Aleman, S.; Chung, R.T.; Chan, A.T.; Ludvigsson, J.F. Association of Aspirin with Hepatocellular Carcinoma and Liver-Related Mortality. N. Engl. J. Med. 2020, 382, 1018–1028. [Google Scholar] [CrossRef]
- In’t Veld, S.G.; Wurdinger, T. Tumor-educated platelets. Blood 2019, 133, 2359–2364. [Google Scholar] [CrossRef]
- Best, M.G.; Sol, N.; Kooi, I.; Tannous, J.; Westerman, B.A.; Rustenburg, F.; Schellen, P.; Verschueren, H.; Post, E.; Koster, J.; et al. RNA-Seq of Tumor-Educated Platelets Enables Blood-Based Pan-Cancer, Multiclass, and Molecular Pathway Cancer Diagnostics. Cancer Cell 2015, 28, 666–676. [Google Scholar] [CrossRef]
- Goddard, E.T.; Bozic, I.; Riddell, S.R.; Ghajar, C.M. Dormant tumour cells, their niches and the influence of immunity. Nat. Cell Biol. 2018, 20, 1240–1249. [Google Scholar] [CrossRef]
- Blanco, P.L.; Lim, L.A.; Miyamoto, C.; Burnier, M.N. Uveal melanoma dormancy: An acceptable clinical endpoint? Melanoma Res. 2012, 22, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, A.; Costa-Silva, B.; Shen, T.-L.; Rodrigues, G.; Hashimoto, A.; Tesic Mark, M.; Molina, H.; Kohsaka, S.; Di Giannatale, A.; Ceder, S.; et al. Tumour exosome integrins determine organotropic metastasis. Nature 2015, 527, 329–335. [Google Scholar] [CrossRef]
- Peinado, H.; Alečković, M.; Lavotshkin, S.; Matei, I.; Costa-Silva, B.; Moreno-Bueno, G.; Hergueta-Redondo, M.; Williams, C.; García-Santos, G.; Ghajar, C.; et al. Melanoma exosomes educate bone marrow progenitor cells toward a pro-metastatic phenotype through MET. Nat. Med. 2012, 18, 883–891. [Google Scholar] [CrossRef]
- Sollier, E.; Go, D.E.; Che, J.; Gossett, D.R.; O’Byrne, S.; Weaver, W.M.; Kummer, N.; Rettig, M.; Goldman, J.; Nickols, N.; et al. Size-selective collection of circulating tumor cells using Vortex technology. Lab Chip 2014, 14, 63–77. [Google Scholar] [CrossRef]
- Eide, N.; Faye, R.S.; Høifødt, H.K.; Sandvik, L.; Qvale, G.A.; Faber, R.; Jebsen, P.; Kvalheim, G.; Fodstad, Ø. The Results of Stricter Inclusion Criteria in an Immunomagnetic Detection Study of Micrometastatic Cells in Bone Marrow of Uveal Melanoma Patients-Relevance for Dormancy. Pathol. Oncol. Res. 2019, 25, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.N.; Bhowmick, N.A. Role of EMT in Metastasis and Therapy Resistance. J. Clin. Med. 2016, 5, 17. [Google Scholar] [CrossRef]
- Kahlert, U.D.; Joseph, J.V.; Kruyt, F.A.E. EMT- and MET-related processes in nonepithelial tumors: Importance for disease progression, prognosis, and therapeutic opportunities. Mol. Oncol. 2017, 11, 860–877. [Google Scholar] [CrossRef]
- Marshall, J.-C.; Nantel, A.; Blanco, P.; Ash, J.; Cruess, S.R.; Burnier, M.N. Transcriptional profiling of human uveal melanoma from cell lines to intraocular tumors to metastasis. Clin. Exp. Metastasis 2007, 24, 353–362. [Google Scholar] [CrossRef]
- Sun, J.; Xi, H.-Y.; Shao, Q.; Liu, Q.-H. Biomarkers in retinoblastoma. Int. J. Ophthalmol. 2020, 13, 325–341. [Google Scholar] [CrossRef]
- Munier, F.L.; Gaillard, M.-C.; Balmer, A.; Soliman, S.; Podilsky, G.; Moulin, A.P.; Beck-Popovic, M. Intravitreal chemotherapy for vitreous disease in retinoblastoma revisited: From prohibition to conditional indications. Br. J. Ophthalmol. 2012, 96, 1078–1083. [Google Scholar] [CrossRef]
- Soliman, S.E.; Racher, H.; Zhang, C.; MacDonald, H.; Gallie, B.L. Genetics and Molecular Diagnostics in Retinoblastoma–An Update. Asia Pac. J. Ophthalmol. 2017, 6, 197–207. [Google Scholar] [CrossRef]
- Soliman, S.E.; Wan, M.J.; Heon, E.; Hazrati, L.-N.; Gallie, B. Retinoblastoma versus advanced Coats’ disease: Is enucleation the answer? Ophthalmic Genet. 2017, 38, 291–293. [Google Scholar] [CrossRef]
- Berry, J.L.; Xu, L.; Kooi, I.; Murphree, A.L.; Prabakar, R.K.; Reid, M.; Stachelek, K.; Le, B.H.A.; Welter, L.; Reiser, B.J.; et al. Genomic cfDNA Analysis of Aqueous Humor in Retinoblastoma Predicts Eye Salvage: The Surrogate Tumor Biopsy for Retinoblastoma. Mol. Cancer Res. 2018, 16, 1701–1712. [Google Scholar] [CrossRef]
- Xu, L.; Polski, A.; Prabakar, R.K.; Reid, M.W.; Chevez-Barrios, P.; Jubran, R.; Kim, J.W.; Kuhn, P.; Cobrinik, D.; Hicks, J.; et al. Chromosome 6p Amplification in Aqueous Humor Cell-Free DNA Is a Prognostic Biomarker for Retinoblastoma Ocular Survival. Mol. Cancer Res. 2020, 18, 1166–1175. [Google Scholar] [CrossRef] [PubMed]
- Gerrish, A.; Stone, E.; Clokie, S.; Ainsworth, J.R.; Jenkinson, H.; McCalla, M.; Hitchcott, C.; Colmenero, I.; Allen, S.; Parulekar, M.; et al. Non-invasive diagnosis of retinoblastoma using cell-free DNA from aqueous humour. Br. J. Ophthalmol. 2019. [Google Scholar] [CrossRef]
- Kothari, P.; Marass, F.; Yang, J.L.; Stewart, C.M.; Stephens, D.; Patel, J.; Hasan, M.; Jing, X.; Meng, F.; Enriquez, J.; et al. Cell-free DNA profiling in retinoblastoma patients with advanced intraocular disease: An MSKCC experience. Cancer Med. 2020. [Google Scholar] [CrossRef]
- Ghiam, B.K.; Xu, L.; Berry, J.L. Aqueous Humor Markers in Retinoblastoma, a Review. Transl. Vis. Sci. Technol. 2019, 8, 13. [Google Scholar] [CrossRef]
- Beta, M.; Venkatesan, N.; Vasudevan, M.; Vetrivel, U.; Khetan, V.; Krishnakumar, S. Identification and Insilico Analysis of Retinoblastoma Serum microRNA Profile and Gene Targets towards Prediction of Novel Serum Biomarkers. Bioinform. Biol. Insights 2013, 7, 21–34. [Google Scholar] [CrossRef]
- Scholz, S.L.; Cosgarea, I.; Süßkind, D.; Murali, R.; Möller, I.; Reis, H.; Leonardelli, S.; Schilling, B.; Schimming, T.; Hadaschik, E.; et al. NF1 mutations in conjunctival melanoma. Br. J. Cancer 2018, 118, 1243–1247. [Google Scholar] [CrossRef]
- Kaštelan, S.; Gverović Antunica, A.; Beketić Orešković, L.; Salopek Rabatić, J.; Kasun, B.; Bakija, I. Conjunctival Melanoma-Epidemiological Trends and Features. Pathol. Oncol. Res. 2018, 24, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Maiorano, B.A.; Pagliara, M.M.; Sammarco, M.G.; Dosa, T.; Martini, M.; Rindi, G.; Bria, E.; Blasi, M.A.; Tortora, G.; et al. Dabrafenib and Trametinib in BRAF Mutant Metastatic Conjunctival Melanoma. Front. Oncol. 2019, 9, 232. [Google Scholar] [CrossRef]
- Sagiv, O.; Thakar, S.D.; Kandl, T.J.; Ford, J.; Sniegowski, M.C.; Hwu, W.-J.; Esmaeli, B. Immunotherapy With Programmed Cell Death 1 Inhibitors for 5 Patients With Conjunctival Melanoma. JAMA Ophthalmol. 2018, 136, 1236–1241. [Google Scholar] [CrossRef]
- Finger, P.T.; Pavlick, A.C. Checkpoint inhibition immunotherapy for advanced local and systemic conjunctival melanoma: A clinical case series. J. Immunother. Cancer 2019, 7, 83. [Google Scholar] [CrossRef]
- Huang, S.K.; Hoon, D.S.B. Liquid biopsy utility for the surveillance of cutaneous malignant melanoma patients. Mol. Oncol. 2016, 10, 450–463. [Google Scholar] [CrossRef]
- Kenawy, N.; Garrick, A.; Heimann, H.; Coupland, S.E.; Damato, B.E. Conjunctival squamous cell neoplasia: The Liverpool Ocular Oncology Centre experience. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 143–150. [Google Scholar] [CrossRef]
- Gichuhi, S.; Ohnuma, S.; Sagoo, M.S.; Burton, M.J. Pathophysiology of ocular surface squamous neoplasia. Exp. Eye Res. 2014, 129, 172–182. [Google Scholar] [CrossRef]
- Santoni, A.; Thariat, J.; Maschi, C.; Herault, J.; Baillif, S.; Lassalle, S.; Peyrichon, M.L.; Salleron, J.; Caujolle, J.-P. Management of Invasive Squamous Cell Carcinomas of the Conjunctiva. Am. J. Ophthalmol. 2019, 200, 1–9. [Google Scholar] [CrossRef]
- Mathis, T.; Jardel, P.; Loria, O.; Delaunay, B.; Nguyen, A.-M.; Lanza, F.; Mosci, C.; Caujolle, J.-P.; Kodjikian, L.; Thariat, J. New concepts in the diagnosis and management of choroidal metastases. Prog. Retin. Eye Res. 2019, 68, 144–176. [Google Scholar] [CrossRef]
- Konstantinidis, L.; Rospond-Kubiak, I.; Zeolite, I.; Heimann, H.; Groenewald, C.; Coupland, S.E.; Damato, B. Management of patients with uveal metastases at the Liverpool Ocular Oncology Centre. Br. J. Ophthalmol. 2014, 98, 92–98. [Google Scholar] [CrossRef]
- Shields, C.L.; Shields, J.A.; Gross, N.E.; Schwartz, G.P.; Lally, S.E. Survey of 520 eyes with uveal metastases. Ophthalmology 1997, 104, 1265–1276. [Google Scholar] [CrossRef]
- Bouhlel, L.; Hofman, V.; Maschi, C.; Ilié, M.; Allégra, M.; Marquette, C.-H.; Audigier-Valette, C.; Thariat, J.; Hofman, P. The liquid biopsy: A tool for a combined diagnostic and theranostic approach for care of a patient with late-stage lung carcinoma presenting with bilateral ocular metastases. Expert Rev. Anticancer Ther. 2017, 17, 1087–1092. [Google Scholar] [CrossRef]
- Daxecker, F.; Zirm, M. Diagnostic value of determining carcino-embryonic antigens in the aqueous humor (author’s transl). Klin. Mon. Augenheilkd. 1980, 177, 768–771. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Antibody Marker | Molecular Marker |
|---|---|
| Melan-A | Tyrosinase |
| HMW-MAA | GNAQ, GNA11 |
| GP 100 | BAP 1 |
| Authors | Study Population | Number of Patients | CTC Isolation Method and Device | CTC Identification | Mean CTC (Range) | Main Findings | Follow-Up: Months (Range) |
|---|---|---|---|---|---|---|---|
| Anand et al. [29] | Primary and metastatic UM | 39 patients 20 primary UM 19 metastatic UM | Immunomagnetism Cellsearch | Cellsearch protocol: DAPI+ HMW-MAA+ CD146+ CD45- CD34- | 5.9 (1–38) | At initial sampling: CTC detected in 14 out of 39 (36%) patients. CTC detected in 6/20 (30%) primary UM and 8/19 (42%) metastatic UM During the follow-up period: CTC detected in 21/39 (54%) of patients CTC were more likely detected in Class 2 UM (83%) | 16.4 |
| Tura et al. [30] | Primary UM | 44 UM patients | Immuno-FISH isolation | NKIC3 and MCSP antibodies | Median: 2.4 (0–10.2) Median CTC in Monosomy 3 patients: 3.4 (0.7–10.2) Median CTC without Monosomy 3: 1.2 (0.3–8.4) | CTC detected in 40/444 (91%) patients Monosomy 3 detected in 23/40 (58%) patients Monosomy 3 on CTC associated with a higher TNM stage (T3) | 48 |
| Bande et al. [31] | Primary UM Uveal naevi | 12 patients 8 primary UM 4 uveal naevi | Immunomagnetism CellSearch | Cellsearch protocol: DAPI+ HMW-MAA+ CD146+ CD45- CD34- | UM: 1 (0–3) | CTC detected in 50% of UM patients and 0% in uveal naevi No relationship between CTC detection and the UM clinical-pathological features | 25 (16–27) |
| Terai et al. [32] | Metastatic UM | 17 patients 10 hepatic metastases 7 extra hepatic metastases | Immunomagnetism CellSearch | Cellsearch protocol: DAPI+ HMW-MAA+ CD146+ CD45- CD34- | Arterial: median: 5 (1–168) Venous: median: 1 (0–5) | No morphological difference between CTC collected through the arterial and venous route Arterial blood: CTC detection in 100% of cases Venous blood: CTC detection in 52.9% of cases No correlation between CTC number and number and size of metastases | None |
| Tura et al. [33] | Primary UM | 31 patients | Immunomagnetism Immunobeads | 2 antibodies: NKI/C3, NKI/beteb | Median: 3.5 (0–10.2) | CTC detected in 29/31 (93.6%) of patients No correlation between the CTC count and clinical parameters | None |
| Mazzini et al. [34] | Primary UM Metastatic UM Uveal nevi | 31 UM 10 uveal nevi | Isolation by size ISET | Antibodies anti S100, anti MART-1 and anti-tyrosinase | Median 8 (2–50) | CTC detected in 17/31 (55%) of UM patients. No CTC detected in uveal nevi patients No correlation between clinical and biological parameters and CTC positivity Detection of >10 CTC associated with a larger basal diameter, tumor height, disease free survival, and OS | 24–60 |
| Bidard et al. [35] | Metastatic UM | 40 patients | For CTC detection: Immunomagentism Cellsearch For Ct-DNA detection: BiPAP technique with 3 mutations screening: GNAQ c.626A > T, GNAQ c.626A > C and GNA11 c.626A > T | Cellsearch protocol: DAPI+ HMW-MAA+ CD146+ CD45- CD34- | 0 CTC: 70% ≥ 1 CTC: 30% 1 CTC: 10% 3 CTC: 15% 12 CTC: 2.5% 20 CTC: 2.5% DNA quantity: Median: 4.1 ng/mL (0.5–512) | Liver miliary associated with higher ct-DNA levels and CTC counts Correlation between CTC, ct-DNA, and tumor volume assessed by liver MRI Univariate analysis: CTC and ct-DNA positivity associated with PFS and OS Multivariate analysis: Only ct-DNA was associated with PFS and OS | 8 (median) |
| Pinzani et al. [36] | Primary UM Healthy Controls | 41 primary UM 16 controls | mRNA detected by RT-PCR (41 patients) CTC: Isolation by size using ISET device (16 patients) Blood samples repeated every 6 months | CTC morphology: cell size > 16-micron, nucleocytoplasmic ratio > 50%, irregular nuclear shape, hyperchromatic nucleus, and basophilic cytoplasm | PCR: median: 0.8 cell equivalent /mL of blood (0.1–14.4) ISET: 5.8, 2.33, 2.00, 1.25, and 0.75 CTC/ml | RT-PCR positivity in 20/41 (49%) of patients among at least one of the blood samples PCR positivity associated with decreased PFS and OS CTC detected in 5/16 (31%) patients Tyrosinase level correlated with CTC detection | 55 |
| Suesskind et al. [37] | Primary UM | 81 primary UM 94 samples before /after treatment | Immunomagnetism MACS | MCSP antibody | Preoperative median CTC count: 1 (1–8) Post-treatment: median CTC count: 7.5 (1–26) | CTC count before and after treatment (enucleation =7, radiotherapy stereotaxic =49, endoresection =19, brachytherapy =15, thermotherapy = 4) Before treatment: CTC detected in 13/94 (14%) of patients After treatment: CTC detected in 9/94 (10%) of patients No significant difference in terms of the CTC count before and after treatment No relationship between the CTC positivity and patient characteristics and metastatic status | 16 (median) |
| Eide et al. [38] | Primary UM | 328 patients | Immunomagnetism | Several anti-melanoma antibodies (9.2.27 antimelanoma-associated antibody, IgG1 Ep-1 antibody, 376.96 antibody) | Median cells number: 50 (1–500) | CTC detected in 4/328 (1,6%) patients Tumor cells detected in 98/328 (29.9%) patients in bone marrow No relationship between bone marrow tumor detection and further metastatic spread | 60 |
| Ulmer et al. [39] | Primary UM Healthy controls | 52 primary UM before treatment 20 healthy controls | Immunomagnetism MACS | MCSP antibody | Median: 2.5 (1–5) for 50 ml | CTC detected in 10/52 (19%) of patients No CTC detected in controls CTC positivity associated with ciliary body invasion, advanced local tumor stage, and anterior tumor localization Multivariate analysis: Only ciliary body involvement associated with CTC positivity | None |
| Authors | Study Population | Number of Patients | Ct-DNA/ct-RNA Detection | Main Findings | Follow-Up: Months (Range) |
|---|---|---|---|---|---|
| Charitoudis et al. [46] | Primary UM undergoing surgery | 202 patients | RT-PCR screening tyrosinase and MELAN-A/MART-1 | RT-PCR tyrosinase positive in 2/184 (1.1%) patients before and 4/180 (2.2%) patients after surgery RT-PCR MELAN-A/MART-1 positive in 20/184 (10.9%) before and in 25/180 (13.9%) patients after surgery RT-PCR results on MELAN-A/MART-1 and Tyrosinase levels were not affected by surgical manipulation | 24 |
| Metz et al. [47] | Primary and metastatic UM | 28 patients | PCR screening GNAQ Q209 (298 bp), GNAQ R183 (212 bp), GNA11 Q209 (150 bp), and GNA11 R183 (249 bp) | Oncogenic GNAQ/GNA11 mutations identified in ct-DNA of 9 out of 22 (41%) metastatic patients. Ct-DNA correlated with the metastatic status ct-DNA detected in younger patients with larger metastases | None |
| Schuster et al. [48] | Metastatic UM | 68 patients | RT-PCR screening tyrosinase and MELAN-A/MART 1 | RT-PCR positive in 43/68 (63%) patients 31 patients positive for tyrosinase 40 patients positive for MELAN-A /MART 1 28 patients positive for both RT-PCR positivity associated with poorer PFS and OS | 10 (median) |
| Schuster et al. [49] | Primary UM | 110 patients | RT-PCR screening tyrosinase, MELAN-A/ MART1 | RT-PCR positive in 11/110 (10%) patients (5 tyrosinase, 5 MALAN-A/MART1, 1 both) No correlation between RT-PCR positivity and clinical features Univariate analysis: The relationship between RT-PCR positivity and time to progression and OS RT-PCR positivity indicated an increased risk of metastasis and disease-specific mortality | 22 (median) |
| Callejo et al. [50] | Primary UM | 30 patients | RT-PCR screening tyrosinase, Melan-A | RT-PCR positive in 29/30 (97%) patients (119 visits, 1360 samples, 2720 PCR performed) No correlation between RT-PCR positivity, tumor size and treatment | NR |
| Boldin et al. [51] | Primary UM | 41 patients | RT-PCR screening tyrosinase | RT-PCR positive in 16/41 (39%) patients at baseline 11/16 (69%) patients initially positive were negative after treatment RT-PCR positivity associated with decreased 5-year OS RT-PCR positivity not correlated with tumor size and histology | 60–66 |
| Keilholz et al. [52] | Primary and metastatic UM | 61 patients 21 primary UM 40 metastatic UM | RT-PCR screening tyrosinase, MELAN-A/MART-1 and GP100 | Primary UM: tyrosinase detected in 3 (12.5%) patients, MELAN/MART detected in 1 (4%) patient and GP100 detected in 1 (4%) patient. Metastatic UM: Tyrosinase detected in 24 (60%) patients, Melan/MART 31 (77%) patients and GP100 in 4/26 (15%) patients GP100 positive in 4/40 (10%) samples. Accuracy detection rates: Tyrosinase > Melan > GP100 | 6 |
| LB Feature | Advantages | Disadvantages |
|---|---|---|
| CTC | ● Allows a better understanding of the metastatic process by screening genetical mutations and surface biomarkers ● Allows laboratory cell culture and further in vivo investigations | ● Lack of consensus concerning pre- and post-analytic processes ● May be less reliable than ct-DNA, according to Bidard et al. |
| Ct-DNA | ● More reliable and standardized techniques compared to CTC ● More stable than ct-RNA | ● Less instructive than CTC in understanding the underlying tumorigenesis ● GNAQ and GNA11 mutations are not found in all UM |
| Ct-RNA | ● Detection by reliable techniques (RT-PCR) | ● Instability (degradation by RNAase) Low abundance ● Half-life very low |
| miRNA | ● Longer half-life, especially when encapsulated ● More stable compared to ct-DNA and ct-RNA ● Detected by reliable techniques (RT-PCR) | ● Lack of consensus regarding pre- and post-analytic processes ● Conflicting results regarding the role of certain mi-RNAs |
| TRE | ● Stable ● Long half-life ● Possibility to investigate mi-RNA, DNA, RNA, as well as surface markers | ● Lack of consensus regarding exosome definition (different definitions based on the size to distinguish exosomes from other small extracellular vesicles) ● Lack of available studies ● Lack of process standardization |
| TEP | ● Promising preliminary results in other solid malignancies ● TEPs are easily obtained and processed ● Available in large amounts | ● Lack of studies into UM |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martel, A.; Baillif, S.; Nahon-esteve, S.; Gastaud, L.; Bertolotto, C.; Roméo, B.; Mograbi, B.; Lassalle, S.; Hofman, P. Liquid Biopsy for Solid Ophthalmic Malignancies: An Updated Review and Perspectives. Cancers 2020, 12, 3284. https://doi.org/10.3390/cancers12113284
Martel A, Baillif S, Nahon-esteve S, Gastaud L, Bertolotto C, Roméo B, Mograbi B, Lassalle S, Hofman P. Liquid Biopsy for Solid Ophthalmic Malignancies: An Updated Review and Perspectives. Cancers. 2020; 12(11):3284. https://doi.org/10.3390/cancers12113284
Chicago/Turabian StyleMartel, Arnaud, Stephanie Baillif, Sacha Nahon-esteve, Lauris Gastaud, Corine Bertolotto, Barnabé Roméo, Baharia Mograbi, Sandra Lassalle, and Paul Hofman. 2020. "Liquid Biopsy for Solid Ophthalmic Malignancies: An Updated Review and Perspectives" Cancers 12, no. 11: 3284. https://doi.org/10.3390/cancers12113284
APA StyleMartel, A., Baillif, S., Nahon-esteve, S., Gastaud, L., Bertolotto, C., Roméo, B., Mograbi, B., Lassalle, S., & Hofman, P. (2020). Liquid Biopsy for Solid Ophthalmic Malignancies: An Updated Review and Perspectives. Cancers, 12(11), 3284. https://doi.org/10.3390/cancers12113284