Non-Alcoholic Steatohepatitis as a Risk Factor for Intrahepatic Cholangiocarcinoma and Its Prognostic Role


 ,
,  , ,
, ,  , ,
, , 
 , and
, and
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Study Population
2.2. Prevalence of NAFLD and NASH
2.3. Characteristics of NASH-Related iCCA
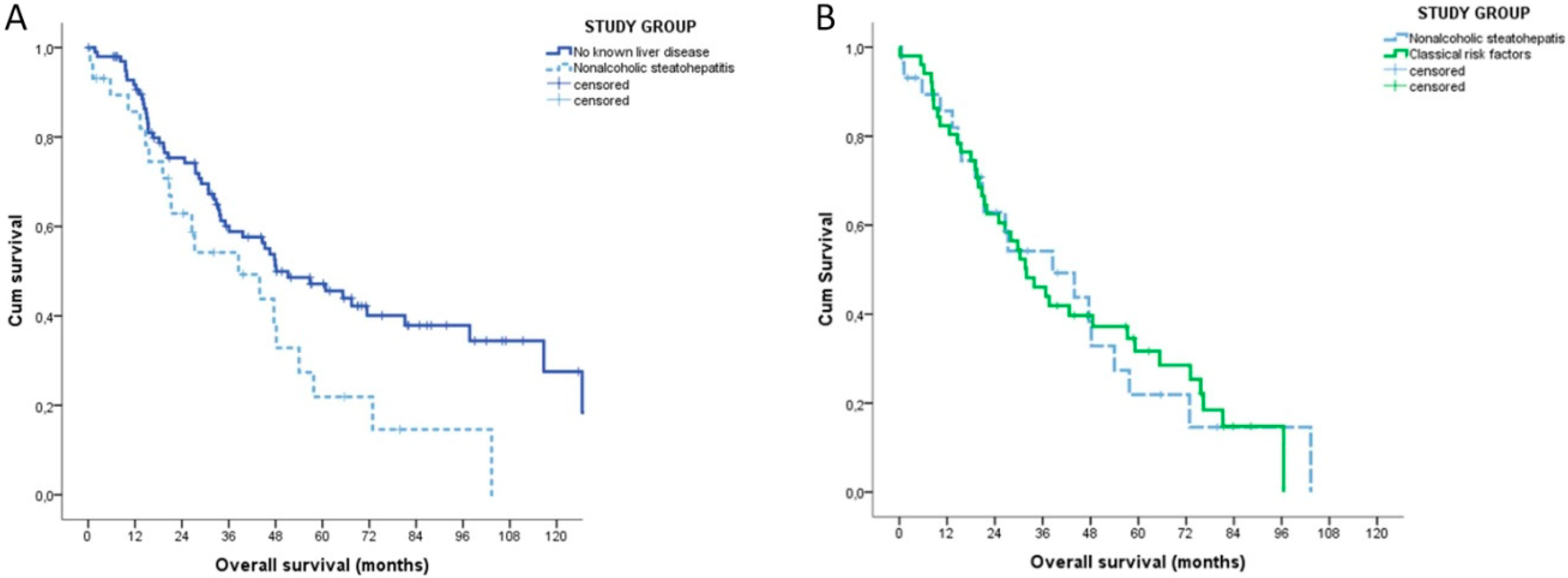
2.4. Survival Correlates
3. Discussion
4. Materials and Methods
4.1. Study Setting and Design
4.2. Evaluation of NAFLD and NASH
4.3. Evaluation of the Clinical Characteristics of NASH-Related iCCA
4.4. Evaluation of the Prognostic Role of NASH
4.5. Statistical Analysis
4.6. Ethics
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.-W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [PubMed]
- Piscaglia, F.; Svegliati-Baroni, G.; Barchetti, A.; Pecorelli, A.; Marinelli, S.; Tiribelli, C.; Bellentani, S. HCC-NAFLD Italian Study Group Clinical patterns of hepatocellular carcinoma in nonalcoholic fatty liver disease: A multicenter prospective study. Hepatology 2016, 63, 827–838. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.M.; Yin, Z.F.; Yang, J.M.; Li, B.; Shao, W.Y.; Xu, F.; Wang, Y.L.; Li, D.Q. Risk factors for intrahepatic cholangiocarcinoma: A case-control study in China. World J. Gastroenterol. 2008, 14, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Ghoz, H.M.; Peeraphatdit, T.; Baichoo, E.; Addissie, B.D.; Harmsen, W.S.; Therneau, T.M.; Olson, J.E.; Chaiteerakij, R.; Roberts, L.R. Aspirin use and the risk of cholangiocarcinoma. Hepatology 2016, 64, 785–796. [Google Scholar] [CrossRef]
- Welzel, T.M.; Graubard, B.I.; El-Serag, H.B.; Shaib, Y.H.; Hsing, A.W.; Davila, J.A.; McGlynn, K.A. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in the United States: A population-based case-control study. Clin. Gastroenterol. Hepatol. 2007, 5, 1221–1228. [Google Scholar] [CrossRef]
- Chang, J.S.; Tsai, C.-R.; Chen, L.-T. Medical risk factors associated with cholangiocarcinoma in Taiwan: A population-based case-control study. PLoS ONE 2013, 8, e69981. [Google Scholar] [CrossRef] [PubMed]
- Stepien, M.; Fedirko, V.; Duarte-Salles, T.; Ferrari, P.; Freisling, H.; Trepo, E.; Trichopoulou, A.; Bamia, C.; Weiderpass, E.; Olsen, A.; et al. Prospective association of liver function biomarkers with development of hepatobiliary cancers. Cancer Epidemiol. 2016, 40, 179–187. [Google Scholar] [CrossRef]
- Kinoshita, M.; Kubo, S.; Tanaka, S.; Takemura, S.; Nishioka, T.; Hamano, G.; Ito, T.; Tanaka, S.; Ohsawa, M.; Shibata, T. The association between non-alcoholic steatohepatitis and intrahepatic cholangiocarcinoma: A hospital based case-control study. J. Surg. Oncol. 2016, 113, 779–783. [Google Scholar] [CrossRef]
- Reddy, S.K.; Hyder, O.; Marsh, J.W.; Sotiropoulos, G.C.; Paul, A.; Alexandrescu, S.; Marques, H.; Pulitano, C.; Barroso, E.; Aldrighetti, L.; et al. Prevalence of nonalcoholic steatohepatitis among patients with resectable intrahepatic cholangiocarcinoma. J. Gastrointest. Surg. 2013, 17, 748–755. [Google Scholar] [CrossRef]
- Paradis, V.; Fukayama, M.; Park, Y.N.; Schirmcher, P. Tumours of the liver and intrahepatic bile ducts. In WHO Classification of Tumours, 5th ed.; WHO Classificaiton of Tumours Editorial Board; World Health Organization: Geneva, Switzerland, 2019; Volume 1, pp. 215–264. [Google Scholar]
- Hobeika, C.; Cauchy, F.; Poté, N.; Rautou, P.-E.; Durand, F.; Farges, O.; Dokmak, S.; Vilgrain, V.; Ronot, M.; Paradis, V.; et al. Short- and Long-Term Outcomes of Liver Resection for Intrahepatic Cholangiocarcinoma Associated with the Metabolic Syndrome. World J. Surg. 2019, 43, 2048–2060. [Google Scholar] [CrossRef]
- Sirica, A.E.; Gores, G.J.; Groopman, J.D.; Selaru, F.M.; Strazzabosco, M.; Wei Wang, X.; Zhu, A.X. Intrahepatic Cholangiocarcinoma: Continuing Challenges and Translational Advances. Hepatology 2019, 69, 1803–1815. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Wongjarupong, N.; Assavapongpaiboon, B.; Susantitaphong, P.; Cheungpasitporn, W.; Treeprasertsuk, S.; Rerknimitr, R.; Chaiteerakij, R. Non-alcoholic fatty liver disease as a risk factor for cholangiocarcinoma: A systematic review and meta-analysis. BMC Gastroenterol. 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed]
- Tovoli, F.; Napoli, L.; Negrini, G.; D’Addato, S.; Tozzi, G.; D’Amico, J.; Piscaglia, F.; Bolondi, L. A Relative Deficiency of Lysosomal Acid Lypase Activity Characterizes Non-Alcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2017, 18, 1134. [Google Scholar] [CrossRef]
- Chavez-Tapia, N.C.; Rosso, N.; Tiribelli, C. Effect of intracellular lipid accumulation in a new model of non-alcoholic fatty liver disease. BMC Gastroenterol. 2012, 12, 20. [Google Scholar] [CrossRef]
- Stefano, J.T.; de Oliveira, C.P.M.S.; Corrêa-Giannella, M.L.; Soares, I.C.; Kubrusly, M.S.; Bellodi-Privato, M.; de Mello, E.S.; de Lima, V.M.R.; Carrilho, F.J.; Alves, V.A.F. Decreased immunoexpression of survivin could be a potential marker in human non-alcoholic fatty liver disease progression? Liver Int. Off. J. Int. Assoc. Study Liver 2011, 31, 377–385. [Google Scholar] [CrossRef]
- Piccinin, E.; Villani, G.; Moschetta, A. Metabolic aspects in NAFLD, NASH and hepatocellular carcinoma: The role of PGC1 coactivators. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 160–174. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Bhoori, S.; Castelli, C.; Putignani, L.; Rivoltini, L.; Del Chierico, F.; Sanguinetti, M.; Morelli, D.; Paroni Sterbini, F.; Petito, V.; et al. Hepatocellular Carcinoma Is Associated With Gut Microbiota Profile and Inflammation in Nonalcoholic Fatty Liver Disease. Hepatology 2019, 69, 107–120. [Google Scholar] [CrossRef]
- Singh, V.; Yeoh, B.S.; Chassaing, B.; Xiao, X.; Saha, P.; Aguilera Olvera, R.; Lapek, J.D.; Zhang, L.; Wang, W.-B.; Hao, S.; et al. Dysregulated Microbial Fermentation of Soluble Fiber Induces Cholestatic Liver Cancer. Cell 2018, 175, 679–694. [Google Scholar] [CrossRef]
- Brandi, G.; De Lorenzo, S.; Candela, M.; Pantaleo, M.A.; Bellentani, S.; Tovoli, F.; Saccoccio, G.; Biasco, G. Microbiota, NASH, HCC and the potential role of probiotics. Carcinogenesis 2017, 38, 231–240. [Google Scholar] [CrossRef]
- Liu, Y.-L.; Patman, G.L.; Leathart, J.B.S.; Piguet, A.-C.; Burt, A.D.; Dufour, J.-F.; Day, C.P.; Daly, A.K.; Reeves, H.L.; Anstee, Q.M. Carriage of the PNPLA3 rs738409 C >G polymorphism confers an increased risk of non-alcoholic fatty liver disease associated hepatocellular carcinoma. J. Hepatol. 2014, 61, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Pais, R.; Fartoux, L.; Goumard, C.; Scatton, O.; Wendum, D.; Rosmorduc, O.; Ratziu, V. Temporal trends, clinical patterns and outcomes of NAFLD-related HCC in patients undergoing liver resection over a 20-year period. Aliment. Pharmacol. Ther. 2017, 46, 856–863. [Google Scholar] [CrossRef]
- Stine, J.G.; Wentworth, B.J.; Zimmet, A.; Rinella, M.E.; Loomba, R.; Caldwell, S.H.; Argo, C.K. Systematic review with meta-analysis: Risk of hepatocellular carcinoma in non-alcoholic steatohepatitis without cirrhosis compared to other liver diseases. Aliment. Pharmacol. Ther. 2018, 48, 696–703. [Google Scholar] [CrossRef]
- Jesper, D.; Heyn, S.G.; Schellhaas, B.; Pfeifer, L.; Goertz, R.S.; Zopf, S.; Neurath, M.F.; Strobel, D. Effects of liver cirrhosis and patient condition on clinical outcomes in intrahepatic cholangiocarcinoma: A retrospective analysis of 156 cases in a single center. Eur. J. Gastroenterol. Hepatol. 2018, 30, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Tovoli, F.; Casadei-Gardini, A.; Benevento, F.; Piscaglia, F. Immunotherapy for hepatocellular carcinoma: A review of potential new drugs based on ongoing clinical studies as of 2019. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2019, 51, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, H.; Lv, P.; Liu, G.; Li, X.; Tian, B.; Chen, D. Prognostic value of cirrhosis for intrahepatic cholangiocarcinoma after surgical treatment. J. Gastrointest. Surg. 2011, 15, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Yuan, L.; Wang, Y.; Ge, R.; Sun, Y.; Wei, G. Survival outcomes and prognostic factors of surgical therapy for all potentially resectable intrahepatic cholangiocarcinoma: A large single-center cohort study. J. Gastrointest. Surg. 2014, 18, 562–572. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Bedossa, P. FLIP Pathology Consortium Utility and appropriateness of the fatty liver inhibition of progression (FLIP) algorithm and steatosis, activity, and fibrosis (SAF) score in the evaluation of biopsies of nonalcoholic fatty liver disease. Hepatology 2014, 60, 565–575. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Brunt, E.M.; Kleiner, D.E.; Kowdley, K.V.; Chalasani, N.; Lavine, J.E.; Ratziu, V.; McCullough, A. Endpoints and clinical trial design for nonalcoholic steatohepatitis. Hepatology 2011, 54, 344–353. [Google Scholar] [CrossRef]
- Ding, P.; VanderWeele, T.J. Sensitivity Analysis Without Assumptions. Epidemiol. Camb. Mass 2016, 27, 368–377. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients Characteristics (n = 180) | Value |
|---|---|
| Male sex | 98 (54.4%) |
| Median age (years) | 66 (57–72) |
| History of other tumours | 38 (21.1%) |
| Arterial hypertension | 85 (47.2%) |
| Type 2 diabetes mellitus | 35 (19.4%) |
| Dyslipidemia | 41 (22.8%) |
| Body mass index (median) | 25.1 (22.9–28.4) |
| Risk factors | |
| Hepatitis B virus infection | 8 (4.4%) |
| Hepatitis C virus infection | 15 (8.3%) |
| Alcohol consumption | 17 (9.4%) |
| Other * | 11 (6.1%) |
| No classical risk factors | 129 (71.7%) |
| Characteristics of Tumour (n = 180) | Value |
|---|---|
| Main tumour dimension (mm) | 60 (38–86) |
| Multinodular disease | 50 (27.8) |
| T | |
| 1a | 38 (21.1) |
| 1b | 48 (26.7) |
| 2 | 66 (36.7) |
| 3 | 13 (7.2) |
| 4 | 15 (8.3) |
| N1 | 36 (20.0) |
| TNM stage (8th edition) | |
| Ia | 37 (20.6) |
| Ib | 42 (23.3) |
| II | 51 (28.3) |
| IIIa | 7 (3.9) |
| IIIb | 43 (23.9) |
| Resection margin | |
| R0 | 131 (72.8) |
| R1 | 46 (25.6) |
| R2 | 3 (1.7) |
| Adjuvant treatment | 76 (42.2) |
| Overall Survival (months, 95% CI) | 44.6 (34.7–54.5) |
| Group | iCCA Patients | Liver Donors | p | Risk Ratio (95% CI) | E-Value (95% CI Closest to the Null) |
|---|---|---|---|---|---|
| All patients (F0–F4) | |||||
| NAFLD | 59/129 (45.7) | 50/129 (38.8) | 0.313 | 1.18 (0.89–1.57) | 1.64 (1.00) |
| NASH | 29/129 (22.5) | 8/129 (6.2) | <0.001 | 3.63 (1.72–7.63) | 6.71 (2.84) |
| No significant fibrosis (F0–F2) | |||||
| NAFLD | 53/115 (46.1) | 49/115 (42.6) | 0.690 | 1.08 (0.80–1.46) | 1.38 (1.00) |
| NASH | 21/115 (18.2) | 5/115(4.3) | 0.001 | 4.20 (1.64–10.76) | 7.87 (2.66) |
| Variables | NASH Group A (n = 29) | No Risk Factors Group B (n = 100) | Classical Risk Factors Group C (n = 51) | Omnibus p-Value * | A vs. B p-Value ** | A vs. C p-Value ** |
|---|---|---|---|---|---|---|
| Sex (Male) | 14 (48.3%) | 49 (49.0%) | 35 (68.6) | 0.056 | 1.000 | 0.096 |
| Age (years) | 70.0 (58.0–75.5) | 66.5 (58.0–72.8) | 63.0 (56.0–70.0) | 0.120 | 0.287 | - |
| History of other tumours | 7 (24.1%) | 21 (21.0%) | 10 (19.6) | 0.891 | 0.799 | 0.777 |
| Hypertension | 22 (75.9%) | 45 (45.0%) | 28 (54.9) | 0.013 | 0.005 | 0.092 |
| Diabetes | 7 (24.1%) | 13 (13.0%) | 14 (27.5) | 0.073 | 0.085 | 0.798 |
| Dyslipidemia | 8 (27.6%) | 22 (22.0%) | 11 (21.6) | 0.795 | 0.618 | 0.591 |
| Body mass index | 29.8 (24.1–32.0) | 24.2 (22.0–26.7) | 26.1 (23.6–28.3) | <0.001 | 0.001 | 0.030 |
| Severe fibrosis (F3–F4) | 6 (20.7) | 8 (8.0) | 22 (43.1) | <0.001 | 0.084 | 0.053 |
| Main tumour dimension (mm) | 50.0 (30.5–79.0) | 65.5 (50.0–95.0) | 50.0 (30.0–70.0) | 0.003 | 0.005 | 1.000 |
| Multinodular disease | 10 (34.5%) | 25 (25.0%) | 15 (29.4) | 0.576 | 0.346 | 0.802 |
| T | ||||||
| 1a | 5 (17.2%) | 17 (17.0%) | 16 (31.4) | |||
| 1b | 4 (13.8%) | 34 (34.0%) | 10 (19.6) | |||
| 2 | 15 (51.7%) | 31 (31.0%) | 17 (33.0) | 0.163 | 0.511 | 0.438 |
| 3a | 3 (10.3%) | 8 (8.0%) | 2 (3.9) | |||
| 3b | 2 (6.9%) | 10 (10.0%) | 6 (11.8) | |||
| n > 0 | 28(27.6%) | 23 (23.0%) | 5 (9.8) | 0.085 | 0.626 | 0.058 |
| R > 0 | 9 (31.0%) | 31 (31.0%) | 9 (17.6) | 0.193 | 1.000 | 0.178 |
| Adjuvant treatment | 12 (41.4%) | 42 (42.0%) | 22 (43.1) | 0.986 | 1.000 | 1.000 |
| Univariate | Variable | Multivariate | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| 0.674 | 0.426–1.065 | 0.091 | Sex (Female) | 0.628 | 0.402–1.012 | 0.056 |
| 1.011 | 0.994–1.029 | 0.207 | Age | |||
| 1.005 | 0.920–1.098 | 0.915 | Centre (France) | |||
| 1.014 | 0.979–1.051 | 0.434 | Body mass index | |||
| 1.152 | 0.709–1.872 | 0.567 | Diabetes | |||
| Ref. | Ref. | Ref. | No risk factors | Ref. | Ref. | Ref. |
| 1.809 | 1.077–3.040 | 0.025 | Classical risk factors | 1.900 | 1.025–3.209 | 0.016 |
| 1.724 | 1.134–2.621 | 0.011 | NASH | 1.773 | 1.156–2.718 | 0.009 |
| 1.307 | 0.836–2.043 | 0.252 | Severe fibrosis | |||
| 1.008 | 1.003–1.014 | 0.002 | Main tumour dimension (mm) | 1.010 | 1.004–1.015 | <0.001 |
| 2.105 | 1.425–3.110 | 0.011 | Multinodularity | 2.043 | 1.375–3.036 | 0.028 |
| 1.385 | 0.896–2.140 | 0.142 | n > 0 | |||
| 1.526 | 1.017–2.290 | 0.041 | R > 0 | 1.596 | 1.055–2.416 | 0.033 |
| 0.909 | 0.624–1.323 | 0.617 | Adjuvant treatment | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Lorenzo, S.; Tovoli, F.; Mazzotta, A.; Vasuri, F.; Edeline, J.; Malvi, D.; Boudjema, K.; Renzulli, M.; Jeddou, H.; D’Errico, A.; et al. Non-Alcoholic Steatohepatitis as a Risk Factor for Intrahepatic Cholangiocarcinoma and Its Prognostic Role. Cancers 2020, 12, 3182. https://doi.org/10.3390/cancers12113182
De Lorenzo S, Tovoli F, Mazzotta A, Vasuri F, Edeline J, Malvi D, Boudjema K, Renzulli M, Jeddou H, D’Errico A, et al. Non-Alcoholic Steatohepatitis as a Risk Factor for Intrahepatic Cholangiocarcinoma and Its Prognostic Role. Cancers. 2020; 12(11):3182. https://doi.org/10.3390/cancers12113182
Chicago/Turabian StyleDe Lorenzo, Stefania, Francesco Tovoli, Alessandro Mazzotta, Francesco Vasuri, Julien Edeline, Deborah Malvi, Karim Boudjema, Matteo Renzulli, Heithem Jeddou, Antonietta D’Errico, and et al. 2020. "Non-Alcoholic Steatohepatitis as a Risk Factor for Intrahepatic Cholangiocarcinoma and Its Prognostic Role" Cancers 12, no. 11: 3182. https://doi.org/10.3390/cancers12113182
APA StyleDe Lorenzo, S., Tovoli, F., Mazzotta, A., Vasuri, F., Edeline, J., Malvi, D., Boudjema, K., Renzulli, M., Jeddou, H., D’Errico, A., Turlin, B., Cescon, M., Uguen, T., Granito, A., Lièvre, A., & Brandi, G. (2020). Non-Alcoholic Steatohepatitis as a Risk Factor for Intrahepatic Cholangiocarcinoma and Its Prognostic Role. Cancers, 12(11), 3182. https://doi.org/10.3390/cancers12113182