Clinical Impact of Tumor-Infiltrating Lymphocytes and PD-L1-Positive Cells as Prognostic and Predictive Biomarkers in Urological Malignancies and Retroperitoneal Sarcoma

 ,
,  , and
, and
Simple Summary
Abstract
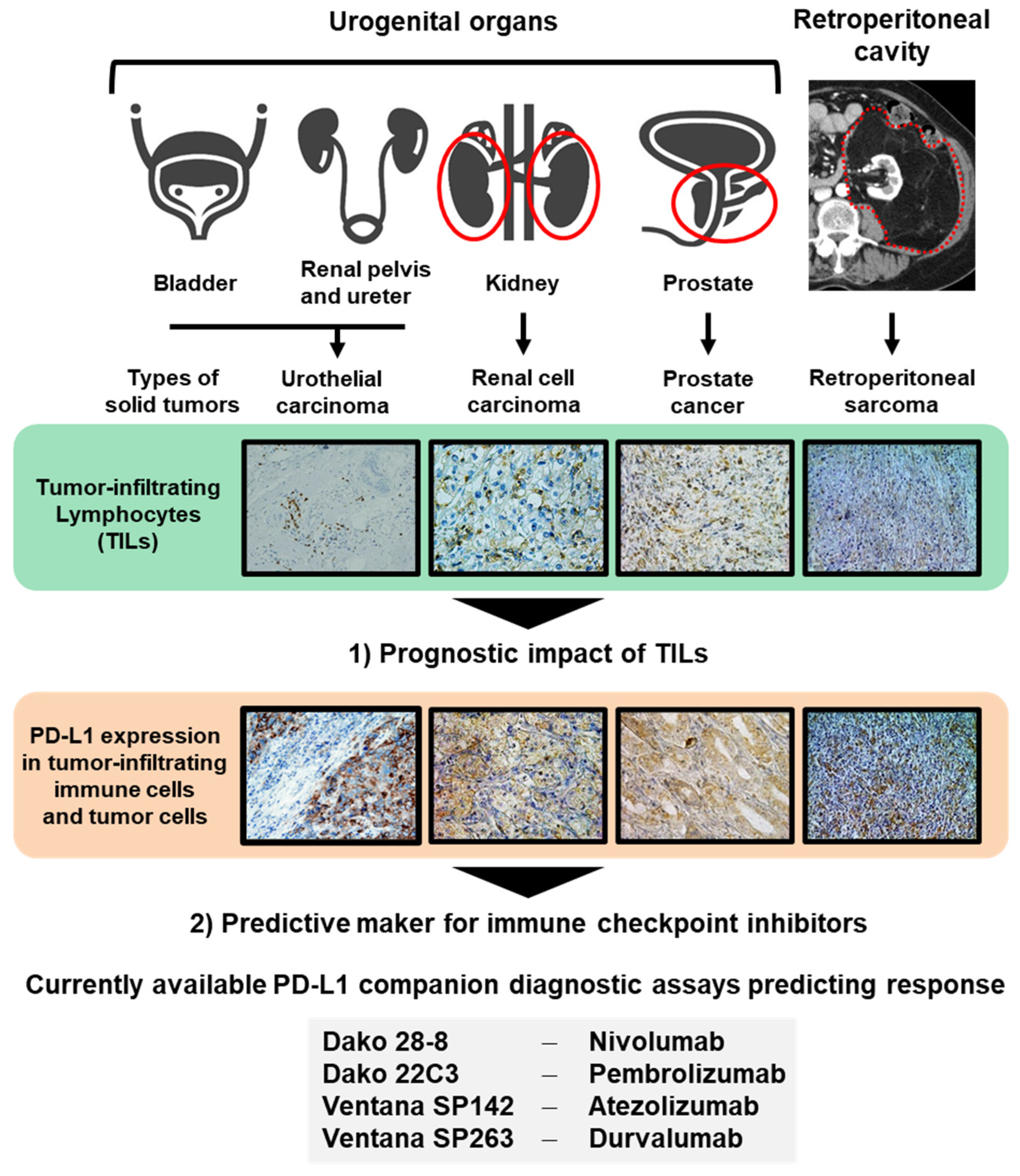
1. Introduction
2. Methods
2.1. Literature Search
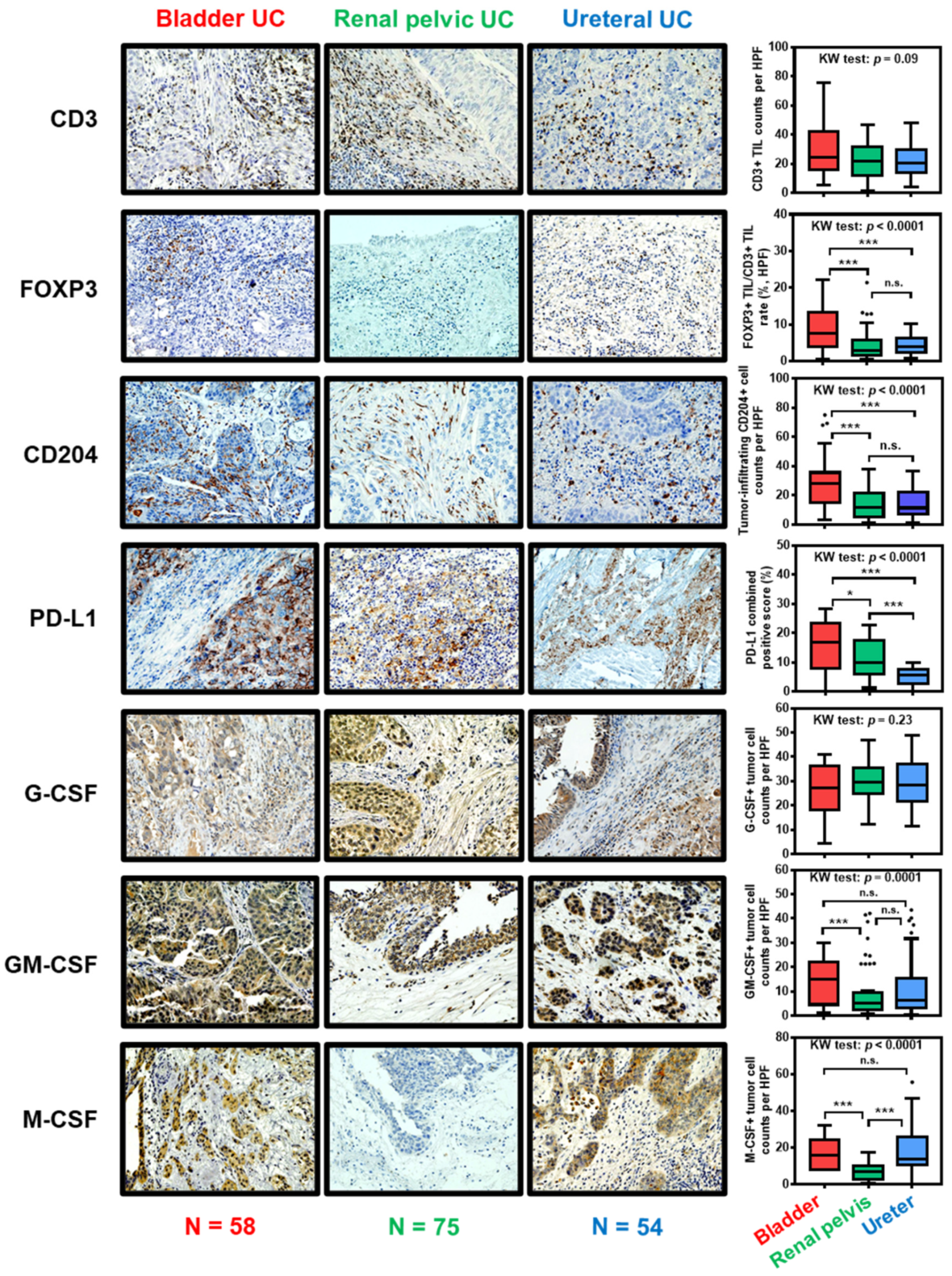
2.2. Immunohistochemical Staining and Quantification in Tumor Tissues of UC Diseases Arising from Different Origins
3. Urothelial Carcinoma (UC)
3.1. Epidemiology and Current Issues of UC
3.2. Clinical Impact of TILs in Patients with UC
3.3. Predictive Biomarkers for Response to ICIs in UC
3.4. The Immunological Profile in the Tumor Microenvironment of UC Arises from Different Primary Origins
4. Renal Cell Carcinoma (RCC)
4.1. Epidemiology and Current Issues of RCC
4.2. Clinical Impact of TILs in Patients with RCC
4.3. Predictive Biomarkers for Response to ICIs in RCC
5. Prostate Cancer (PCa)
5.1. Epidemiology and Current Issues of PCa
5.2. Clinical Impact of TILs in Patients with PCa
5.3. Predictive Biomarkers for Response to ICIs in PCa
6. Retroperitoneal Sarcoma (RSar)
6.1. Epidemiology and Current Issues of RSar
6.2. Clinical Impact of TILs in Patients with RSar
6.3. Predictive Biomarkers for Response to ICIs in RSar
7. Limitations and Current Perspective Regarding the Assessment of TILs
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chen, D.S.; Mellman, I. Oncology meets immunology: The cancer-immunity cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer–immune set point. Nature 2017, 541, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Bruno, A.; Pagani, A.; Magnani, E.; Rossi, T.; Noonan, D.M.; Cantelmo, A.R.; Albini, A. Inflammatory angiogenesis and the tumor microenvironment as targets for cancer therapy and prevention. Cancer Treat. Res. 2014, 159, 401–426. [Google Scholar] [CrossRef] [PubMed]
- Piotrowski, I.; Kulcenty, K.; Suchorska, W. Interplay between inflammation and cancer. Rep. Pract. Oncol. Radiother. 2020, 25, 422–427. [Google Scholar] [CrossRef]
- Frost, F.G.; Cherukuri, P.F.; Milanovich, S.; Boerkoel, C.F. Pan-cancer RNA-seq data stratifies tumours by some hallmarks of cancer. J. Cell. Mol. Med. 2020, 24, 418–430. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed]
- Qian, B.Z.; Pollard, J.W. Macrophage diversity enhances tumor progression and metastasis. Cell 2010, 141, 39–51. [Google Scholar] [CrossRef]
- Shembrey, C.; Huntington, N.D.; Hollande, F. Impact of Tumor and Immunological Heterogeneity on the Anti-Cancer Immune Response. Cancers 2019, 11, 1217. [Google Scholar] [CrossRef]
- Bindea, G.; Mlecnik, B.; Tosolini, M.; Kirilovsky, A.; Waldner, M.; Obenauf, A.C.; Angell, H.; Fredriksen, T.; Lafontaine, L.; Berger, A.; et al. Spatiotemporal dynamics of intratumoral immune cells reveal the immune landscape in human cancer. Immunity 2013, 39, 782–795. [Google Scholar] [CrossRef]
- Lakshmi Narendra, B.; Eshvendar Reddy, K.; Shantikumar, S.; Ramakrishna, S. Immune system: A double-edged sword in cancer. Inflamm. Res. 2013, 62, 823–834. [Google Scholar] [CrossRef] [PubMed]
- Bassani, B.; Baci, D.; Gallazzi, M.; Poggi, A.; Bruno, A.; Mortara, L. Natural Killer Cells as Key Players of Tumor Progression and Angiogenesis: Old and Novel Tools to Divert Their Pro-Tumor Activities into Potent Anti-Tumor Effects. Cancers 2019, 11, 461. [Google Scholar] [CrossRef] [PubMed]
- Gentles, A.J.; Newman, A.M.; Liu, C.L.; Bratman, S.V.; Feng, W.; Kim, D.; Nair, V.S.; Xu, Y.; Khuong, A.; Hoang, C.D.; et al. The prognostic landscape of genes and infiltrating immune cells across human cancers. Nat. Med. 2015, 21, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Doucette, T.; Rao, G.; Rao, A.; Shen, L.; Aldape, K.; Wei, J.; Dziurzynski, K.; Gilbert, M.; Heimberger, A.B. Immune Heterogeneity of Glioblastoma Subtypes: Extrapolation from the Cancer Genome Atlas. Cancer Immunol. Res. 2013, 1, 112–122. [Google Scholar] [CrossRef]
- Reuben, A.; Gittelman, R.; Gao, J.; Zhang, J.; Yusko, E.C.; Wu, C.J.; Emerson, R.; Zhang, J.; Tipton, C.; Li, J.; et al. TCR Repertoire Intratumor Heterogeneity in Localized Lung Adenocarcinomas: An Association with Predicted Neoantigen Heterogeneity and Postsurgical Recurrence. Cancer Discov. 2017, 7, 12–17. [Google Scholar] [CrossRef]
- Miyake, M.; Hori, S.; Morizawa, Y.; Tatsumi, Y.; Nakai, Y.; Anai, S.; Torimoto, K.; Aoki, K.; Tanaka, N.; Shimada, K.; et al. CXCL1-Mediated Interaction of Cancer Cells with Tumor-Associated Macrophages and Cancer-Associated Fibroblasts Promotes Tumor Progression in Human Bladder Cancer. Neoplasia 2016, 18, 636–646. [Google Scholar] [CrossRef]
- Rodallec, A.; Sicard, G.; Fanciullino, R.; Benzekry, S.; Lacarelle, B.; Milano, G.; Ciccolini, J. Turning cold tumors into hot tumors: Harnessing the potential of tumor immunity using nanoparticles. Expert Opin. Drug Metab. Toxicol. 2018, 14, 1139–1147. [Google Scholar] [CrossRef]
- Kawashima, A.; Kanazawa, T.; Goto, K.; Matsumoto, M.; Morimoto-Okazawa, A.; Iwahori, K.; Ujike, T.; Nagahara, A.; Fujita, K.; Uemura, M.; et al. Immunological classification of renal cell carcinoma patients based on phenotypic analysis of immune check-point molecules. Cancer Immunol. Immunother. 2018, 67, 113–125. [Google Scholar] [CrossRef]
- Vareki, S.M. High and low mutational burden tumors versus immunologically hot and cold tumors and response to immune checkpoint inhibitors. J. Immunother. Cancer 2018, 6, 157. [Google Scholar] [CrossRef]
- Strasner, A.; Karin, M. Immune infiltration and prostate Cancer. Front. Oncol. 2015, 5, 128. [Google Scholar] [CrossRef]
- Camus, M.; Tosolini, M.; Mlecnik, B.; Pagè, F.; Kirilovsky, A.; Berger, A.; Costes, A.; Bindea, G.; Charoentong, P.; Bruneval, P.; et al. Coordination of Intratumoral Immune Reaction and Human Colorectal Cancer Recurrence. Cancer Res. 2009, 69, 2685–2693. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, G.C.; Mondal, A.; Dey, S.; Laury-Kleintop, L.D.; Muller, A.J. Inflammatory Reprogramming with IDO1 Inhibitors: Turning Immunologically Unresponsive ’Cold’ Tumors ’Hot’. Trends Cancer 2018, 4, 38–58. [Google Scholar] [CrossRef] [PubMed]
- Galluzzi, L.; Buqué, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunological Effects of Conventional Chemotherapy and Targeted Anticancer Agents. Cancer Cell 2015, 28, 690–714. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Owari, T.; Hori, S.; Nakai, Y.; Fujimoto, K. Emerging biomarkers for the diagnosis and monitoring of urothelial carcinoma. Res. Rep. Urol. 2018, 10, 251–261. [Google Scholar] [CrossRef]
- Fradet, Y.; Bellmunt, J.; Vaughn, D.J.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; Necchi, A.; et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: Results of >2 years of follow-up. Ann. Oncol. 2019, 30, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Tatsumi, Y.; Gotoh, D.; Ohnishi, S.; Owari, T.; Iida, K.; Ohnishi, K.; Hori, S.; Morizawa, Y.; Itami, Y.; et al. Regulatory T Cells and Tumor-Associated Macrophages in the Tumor Microenvironment in Non-Muscle Invasive Bladder Cancer Treated with Intravesical Bacille Calmette-Guérin: A Long-Term Follow-Up Study of a Japanese Cohort. Int. J. Mol. Sci. 2017, 18, 2186. [Google Scholar] [CrossRef]
- Krpina, K.; Babarović, E.; Jonjić, N. Correlation of tumor-infiltrating lymphocytes with bladder cancer recurrence in patients with solitary low-grade urothelial carcinoma. Virchows Arch. 2015, 467, 443–448. [Google Scholar] [CrossRef]
- Zhang, Q.; Hao, C.; Cheng, G.; Wang, L.; Wang, X.; Li, C.; Qiu, J.; Ding, K. High CD4+ T cell density is associated with poor prognosis in patients with non-muscle-invasive bladder cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11510–11516. [Google Scholar]
- Liu, K.; Zhao, K.; Wang, L.; Sun, E. The prognostic values of tumor-infiltrating neutrophils, lymphocytes and neutrophil/lymphocyte rates in bladder urothelial cancer. Pathol. Res. Pract. 2018, 214, 1074–1080. [Google Scholar] [CrossRef]
- Yu, A.; Mansure, J.J.; Solanki, S.; Siemens, D.R.; Koti, M.; Dias, A.B.T.; Burnier, M.M.; Brimo, F.; Kassouf, W. Presence of lymphocytic infiltrate cytotoxic T lymphocyte CD3+, CD8+, and immunoscore as prognostic marker in patients after radical cystectomy. PLoS ONE 2018, 13, e0205746. [Google Scholar] [CrossRef]
- Shi, M.J.; Meng, X.Y.; Wu, Q.J.; Zhou, X.H. High CD3D/CD4 ratio predicts better survival in muscle-invasive bladder cancer. Cancer Manag. Res. 2019, 11, 2987–2995. [Google Scholar] [CrossRef] [PubMed]
- Wahlin, S.; Nodin, B.; Leandersson, K.; Boman, K.; Jirström, K. Clinical impact of T cells, B cells and the PD-1/PD-L1 pathway in muscle invasive bladder cancer: A comparative study of transurethral resection and cystectomy specimens. Oncoimmunology 2019, 8, e1644108. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, A.; Kanazawa, T.; Jingushi, K.; Kato, T.; Ujike, T.; Nagahara, A.; Fujita, K.; Morimoto-Okazawa, A.; Iwahori, K.; Uemura, M.; et al. Phenotypic Analysis of Tumor Tissue-Infiltrating Lymphocytes in Tumor Microenvironment of Bladder Cancer and Upper Urinary Tract Carcinoma. Clin. Genitourin. Cancer 2019, 17, 114–124. [Google Scholar] [CrossRef]
- Zhang, B.; Yu, W.; Feng, X.; Zhao, Z.; Fan, Y.; Meng, Y.; Hu, S.; Cui, Y.; He, Q.; Zhang, H.; et al. Prognostic significance of PD-L1 expression on tumor cells and tumor-infiltrating mononuclear cells in upper tract urothelial carcinoma. Med. Oncol. 2017, 34, 94. [Google Scholar] [CrossRef] [PubMed]
- Krabbe, L.M.; Heitplatz, B.; Preuss, S.; Hutchinson, R.C.; Woldu, S.L.; Singla, N.; Boegemann, M.; Wood, C.G.; Karam, J.A.; Weizer, A.Z.; et al. Prognostic Value of PD-1 and PD-L1 Expression in Patients with High Grade Upper Tract Urothelial Carcinoma. J. Urol. 2017, 198, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.A.; Yang, B.; Rao, W.; Xiao, H.; Wang, D.; Jiang, J. The correlation of BER protein, IRF3 with CD8+ T cell and their prognostic significance in upper tract urothelial carcinoma. Onco. Targets Ther. 2019, 12, 7725–7735. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.S.; Su, H.Y.; Li, P.H.; Chiang, P.H.; Huang, C.H.; Chen, C.H.; Hsieh, M.C. Prognostic impact of tumor infiltrating lymphocytes on patients with metastatic urothelial carcinoma receiving platinum based chemotherapy. Sci. Rep. 2018, 8, 7485. [Google Scholar] [CrossRef]
- Pichler, R.; Fritz, J.; Zavadil, C.; Schäfer, G.; Culig, Z.; Brunner, A. Tumor-infiltrating immune cell subpopulations influence the oncologic outcome after intravesical Bacillus Calmette-Guérin therapy in bladder cancer. Oncotarget 2016, 7, 39916–39930. [Google Scholar] [CrossRef]
- Igarashi, T.; Murakami, S.; Takahashi, H.; Matsuzaki, O.; Shimazaki, J. Changes on distribution of CD4+/CD45RA- and CD8+/CD11- cells in tumor-infiltrating lymphocytes of renal cell carcinoma associated with tumor progression. Eur. Urol. 1992, 22, 323–328. [Google Scholar] [CrossRef]
- Huang, Y.; Wang, J.; Jia, P.; Li, X.; Pei, G.; Wang, C.; Fang, X.; Zhao, Z.; Cai, Z.; Yi, X.; et al. Clonal architectures predict clinical outcome in clear cell renal cell carcinoma. Nat. Commun. 2019, 10, 1245. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, E.; Long, J.; Hu, Z.; Peng, J.; Liu, L.; Tang, F.; Li, L.; Ouyang, Y.; Zeng, Z. Immune infiltration in renal cell carcinoma. Cancer Sci. 2019, 110, 1564–1572. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.C.; Jegede, O.; Shukla, S.A.; Braun, D.A.; Horak, C.E.; Wind-Rotolo, M.; Ishii, Y.; Catalano, P.J.; Grosha, J.; Flaifel, A.; et al. irRECIST for the Evaluation of Candidate Biomarkers of Response to Nivolumab in Metastatic Clear Cell Renal Cell Carcinoma: Analysis of a Phase II Prospective Clinical Trial. Clin. Cancer Res. 2019, 25, 2174–2184. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Kim, K.M.; Bae, J.S.; Park, H.S.; Lee, H.; Chung, M.J.; Moon, W.S.; Lee, D.G.; Jang, K.Y. Tumor-infiltrating PD1-Positive Lymphocytes and FoxP3-Positive Regulatory T Cells Predict Distant Metastatic Relapse and Survival of Clear Cell Renal Cell Carcinoma. Transl. Oncol. 2013, 6, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Jensen, H.K.; Donskov, F.; Nordsmark, M.; Marcussen, N.; von der Maase, H. Increased intratumoral FOXP3-positive regulatory immune cells during interleukin-2 treatment in metastatic renal cell carcinoma. Clin. Cancer Res. 2009, 15, 1052–1058. [Google Scholar] [CrossRef]
- Li, J.F.; Chu, Y.W.; Wang, G.M.; Zhu, T.Y.; Rong, R.M.; Hou, J.; Xu, M. The prognostic value of peritumoral regulatory T cells and its correlation with intratumoral cyclooxygenase-2 expression in clear cell renal cell carcinoma. BJU Int. 2009, 103, 399–405. [Google Scholar] [CrossRef]
- Siddiqui, S.A.; Frigola, X.; Bonne-Annee, S.; Mercader, M.; Kuntz, S.M.; Krambeck, A.E.; Sengupta, S.; Dong, H.; Cheville, J.C.; Lohse, C.M.; et al. Tumor-infiltrating Foxp3−CD4+CD25+ T cells predict poor survival in renal cell carcinoma. Clin. Cancer Res. 2007, 13, 2075–2081. [Google Scholar] [CrossRef]
- Kawashima, A.; Kanazawa, T.; Kidani, Y.; Yoshida, T.; Hirata, M.; Nishida, K.; Nojima, S.; Yamamoto, Y.; Kato, T.; Hatano, K.; et al. Tumour grade significantly correlates with total dysfunction of tumour tissue-infiltrating lymphocytes in renal cell carcinoma. Sci. Rep. 2020, 10, 6220. [Google Scholar] [CrossRef]
- Giraldo, N.A.; Becht, E.; Vano, Y.; Petitprez, F.; Lacroix, L.; Validire, P.; Sanchez-Salas, R.; Ingels, A.; Oudard, S.; Moatti, A.; et al. Tumor-Infiltrating and Peripheral Blood T-cell Immunophenotypes Predict Early Relapse in Localized Clear Cell Renal Cell Carcinoma. Clin. Cancer Res. 2017, 23, 4416–4428. [Google Scholar] [CrossRef]
- Yao, J.; Xi, W.; Zhu, Y.; Wang, H.; Hu, X.; Guo, J. Checkpoint molecule PD-1-assisted CD8+ T lymphocyte count in tumor microenvironment predicts overall survival of patients with metastatic renal cell carcinoma treated with tyrosine kinase inhibitors. Cancer Manag. Res. 2018, 10, 3419–3431. [Google Scholar] [CrossRef]
- Sorrentino, C.; Musiani, P.; Pompa, P.; Cipollone, G.; Di Carlo, E. Androgen deprivation boosts prostatic infiltration of cytotoxic and regulatory T lymphocytes and has no effect on disease-free survival in prostate cancer patients. Clin. Cancer Res. 2011, 17, 1571–1581. [Google Scholar] [CrossRef]
- Ness, N.; Andersen, S.; Valkov, A.; Nordby, Y.; Donnem, T.; Al-Saad, S.; Busund, L.T.; Bremnes, R.M.; Richardsen, E. Infiltration of CD8+ lymphocytes is an independent prognostic factor of biochemical failure-free survival in prostate cancer. Prostate 2014, 74, 1452–1461. [Google Scholar] [CrossRef]
- Nardone, V.; Botta, C.; Caraglia, M.; Martino, E.C.; Ambrosio, M.R.; Carfagno, T.; Tini, P.; Semeraro, L.; Misso, G.; Grimaldi, A.; et al. Tumor infiltrating T lymphocytes expressing FoxP3, CCR7 or PD-1 predict the outcome of prostate cancer patients subjected to salvage radiotherapy after biochemical relapse. Cancer Biol. Ther. 2016, 17, 1213–1220. [Google Scholar] [CrossRef]
- Watanabe, M.; Kanao, K.; Suzuki, S.; Muramatsu, H.; Morinaga, S.; Kajikawa, K.; Kobayashi, I.; Nishikawa, G.; Kato, Y.; Zennami, K.; et al. Increased infiltration of CCR4-positive regulatory T cells in prostate cancer tissue is associated with a poor prognosis. Prostate 2019, 79, 1658–1665. [Google Scholar] [CrossRef]
- Makito, M.; Oda, Y.; Nishimura, N.; Morizawa, Y.; Ohnishi, S.; Hatakeyama, K.; Fujii, T.; Hori, S.; Gotoh, D.; Nakai, Y.; et al. Integrative assessment of clinicopathological parameters and the expression of PD-L1, PD-L2 and PD-1 in tumor cells of retroperitoneal sarcoma. Oncol. Lett. 2020, 20, 190. [Google Scholar] [CrossRef]
- Tseng, W.W.; Demicco, E.G.; Lazar, A.J.; Lev, D.C.; Pollock, R.E. Lymphocyte composition and distribution in inflammatory, well-differentiated retroperitoneal liposarcoma: Clues to a potential adaptive immune response and therapeutic implications. Am. J. Surg. Pathol. 2012, 36, 941–944. [Google Scholar] [CrossRef]
- Tseng, W.W.; Malu, S.; Zhang, M.; Chen, J.; Sim, G.C.; Wei, W.; Ingram, D.; Somaiah, N.; Lev, D.C.; Pollock, R.E.; et al. Analysis of the intratumoral adaptive immune response in well differentiated and dedifferentiated retroperitoneal liposarcoma. Sarcoma 2015, 2015, 547460. [Google Scholar] [CrossRef]
- Yan, L.; Wang, Z.; Cui, C.; Guan, X.; Dong, B.; Zhao, M.; Wu, J.; Tian, X.; Hao, C. Comprehensive immune characterization and T-cell receptor repertoire heterogeneity of retroperitoneal liposarcoma. Cancer Sci. 2019, 110, 3038–3048. [Google Scholar] [CrossRef]
- Gevaert, T.; Cimadamore, A.; Montironi, R.; Eckstein, M. PD-L1 Testing for Urothelial Carcinoma: Interchangeability, Reliability and Future Perspectives. Curr. Drug Targets 2020, 9. [Google Scholar] [CrossRef]
- Patel, M.R.; Ellerton, J.; Infante, J.R.; Agrawal, M.; Gordon, M.; Aljumaily, R.; Britten, C.D.; Dirix, L.; Lee, K.W.; Taylor, M.; et al. Avelumab in metastatic urothelial carcinoma after platinum failure (javelin Solid Tumor): Pooled results from two expansion cohorts of an open-label, phase 1 trial. Lancet Oncol. 2018, 19, 51–64. [Google Scholar] [CrossRef]
- Sharma, P.; Siefker-Radtke, A.; de Braud, F.; Basso, U.; Calvo, E.; Bono, P.; Morse, M.A.; Ascierto, P.A.; Lopez-Martin, J.; Brossart, P.; et al. Nivolumab Alone and with Ipilimumab in Previously Treated Metastatic Urothelial Carcinoma: CheckMate 032 Nivolumab 1 mg/kg Plus Ipilimumab 3 mg/kg Expansion Cohort Results. J. Clin. Oncol. 2019, 37, 1608–1616. [Google Scholar] [CrossRef]
- Powles, T.; O’Donnell, P.H.; Massard, C.; Arkenau, H.T.; Friedlander, T.W.; Hoimes, C.J.; Lee, J.L.; Ong, M.; Sridhar, S.S.; Vogelzang, N.J.; et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: Updated results from a phase 1/2 open-label study. JAMA Oncol. 2017, 3, e172411. [Google Scholar] [CrossRef]
- Sharma, P.; Retz, M.; Siefker-Radtke, A.; Baron, A.; Necchi, A.; Bedke, J.; Plimack, E.R.; Vaena, D.; Grimm, M.O.; Bracarda, S.; et al. Nivolumab in metastatic urothelial carcinoma after platinum therapy (CheckMate 275): A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2017, 18, 312–322. [Google Scholar] [CrossRef]
- Powles, T.; Durán, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Dudek, A.Z.; Liu, L.C.; Gupta, S.; Logan, T.F.; Singer, E.A.; Joshi, M.; Zakharia, Y.N.; Lang, J.M.; Schwarz, J.K.; Al-Janadi, A.; et al. Phase Ib/II Clinical Trial of Pembrolizumab With Bevacizumab for Metastatic Renal Cell Carcinoma: BTCRC-GU14-003. J. Clin. Oncol. 2020, 38, 1138–1145. [Google Scholar] [CrossRef]
- Taylor, M.H.; Lee, C.H.; Makker, V.; Rasco, D.; Dutcus, C.E.; Wu, J.; Stepan, D.E.; Shumaker, R.C.; Motzer, R.J. Phase IB/II Trial of Lenvatinib Plus Pembrolizumab in Patients With Advanced Renal Cell Carcinoma, Endometrial Cancer, and Other Selected Advanced Solid Tumors. J. Clin. Oncol. 2020, 38, 1154–1163. [Google Scholar] [CrossRef]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef]
- Motzer, R.J.; Penkovm, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef]
- Motzer, R.J.; Rini, B.I.; McDermott, D.F.; Frontera, O.A.; Hammers, H.J.; Carducci, M.A.; Salman, P.; Escudier, B.; Beuselinck, B.; Amin, A.; et al. Nivolumab plus ipilimumab versus sunitinib in first-line treatment for advanced renal cell carcinoma: Extended follow-up of efficacy and safety results from a randomised, controlled, phase 3 trial. Lancet Oncol. 2019, 20, 1370–1385. [Google Scholar] [CrossRef]
- Rini, B.I.; Powles, T.; Atkins, M.B.; Escudier, B.; McDermott, D.F.; Suarez, C.; Bracarda, S.; Stadler, W.M.; Donskov, F.; Lee, J.L.; et al. Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): A multicentre, open-label, phase 3, randomised controlled trial. Lancet 2019, 393, 2404–2415. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- McFalls, E.O.; Ward, H.B.; Moritz, T.E.; Goldman, S.; Krupski, W.C.; Littooy, F.; Pierpont, G.; Santilli, S.; Rapp, J.; Hattler, B.; et al. Coronary-artery revascularization before elective major vascular surgery. N. Engl. J. Med. 2004, 351, 2795–2804. [Google Scholar] [CrossRef] [PubMed]
- De Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): A multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef]
- D’Angelo, S.P.; Mahoney, M.R.; Van Tine, B.A.; Atkins, J.; Milhem, M.M.; Jahagirdar, B.N.; Antonescu, C.R.; Horvath, E.; Tap, W.D.; Schwartz, G.K.; et al. Nivolumab with or without ipilimumab treatment for metastatic sarcoma (Alliance A091401): Two open-label, non-comparative, randomised, phase 2 trials. Lancet Oncol. 2018, 19, 416–426. [Google Scholar] [CrossRef]
- Kelly, C.M.; Antonescu, C.R.; Bowler, T.; Munhoz, R.; Chi, P.; Dickson, M.A.; Gounder, M.M.; Keohan, M.L.; Movva, S.; Dholakia, R.; et al. Objective Response Rate Among Patients with Locally Advanced or Metastatic Sarcoma Treated With Talimogene Laherparepvec in Combination with Pembrolizumab: A Phase 2 Clinical Trial. JAMA Oncol. 2020, 6, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Wilky, B.A.; Trucco, M.M.; Subhawong, T.K.; Florou, V.; Park, W.; Kwon, D.; Wieder, E.D.; Kolonias, D.; Rosenberg, A.E.; Kerr, D.A.; et al. Axitinib plus pembrolizumab in patients with advanced sarcomas including alveolar soft-part sarcoma: A single-centre, single-arm, phase 2 trial. Lancet Oncol. 2019, 20, 837–848. [Google Scholar] [CrossRef]
- Green, D.A.; Rink, M.; Xylinas, E.; Matin, S.F.; Stenzl, A.; Roupret, M.; Karakiewicz, P.I.; Scherr, D.S.; Shariat, S.F. Urothelial carcinoma of the bladder and the upper tract: Disparate twins. J. Urol. 2013, 189, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Yates, D.R.; Catto, J.W. Distinct patterns and behaviour of urothelial carcinoma with respect to anatomical location: How molecular biomarkers can augment clinico-pathological predictors in upper urinary tract tumours. World J. Urol. 2013, 31, 21–29. [Google Scholar] [CrossRef]
- Miyake, M.; Tatsumi, Y.; Matsumoto, H.; Nagao, K.; Matsuyama, H.; Inamoto, T.; Azuma, H.; Yasumoto, H.; Shiina, H.; Fujimoto, K. Nishinihon Uro-Oncology Collaborative Group. Outcomes of subsequent non-muscle-invasive bladder cancer treated with intravesical Bacillus Calmette-Guérin after radical nephroureterectomy for upper urinary tract urothelial carcinoma. BJU Int. 2018, 121, 764–773. [Google Scholar] [CrossRef]
- Morizawa, Y.; Miyake, M.; Shimada, K.; Hori, S.; Tatsumi, Y.; Nakai, Y.; Tanaka, N.; Fujii, T.; Fujimoto, K. Colony-stimulating factors detected in tumor cells and voided urine are potential prognostic markers for patients with muscle-invasive bladder cancer undergoing radical cystectomy. Res. Rep. Urol. 2018, 10, 103–111. [Google Scholar] [CrossRef]
- Hori, S.; Miyake, M.; Onishi, S.; Morizawa, Y.; Nakai, Y.; Tatsumi, Y.; Onishi, K.; Iida, K.; Gotoh, D.; Itami, Y.; et al. Evaluation of pro- and anti-tumor effects induced by three colony-stimulating factors, G-CSF, GM-CSF and M-CSF, in bladder cancer cells: Is G-CSF a friend of bladder cancer cells? Int. J. Oncol. 2019, 54, 2237–2249. [Google Scholar] [CrossRef]
- Hori, S.; Miyake, M.; Onishi, S.; Morizawa, Y.; Nakai, Y.; Tatsumi, Y.; Onishi, K.; Iida, K.; Gotoh, D.; Itami, Y.; et al. Supplementary granulocyte macrophage colony-stimulating factor to chemotherapy and programmed death-ligand 1 blockade decreases local recurrence after surgery in bladder cancer. Cancer Sci. 2019, 110, 3315–3327. [Google Scholar] [CrossRef]
- Sun, Y.; Xu, S. Tumor-Associated CD204-Positive Macrophage Is a Prognostic Marker in Clinical Stage I Lung Adenocarcinoma. Biomed. Res. Int. 2018, 2018, 8459193. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef]
- Rini, B.I.; Escudier, B.; Tomczak, P.; Kaprin, A.; Szczylik, C.; Hutson, T.E.; Michaelson, M.D.; Gorbunova, V.A.; Gore, M.E.; Rusakov, I.G.; et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): A randomised phase 3 trial. Lancet 2011, 378, 1931–1939. [Google Scholar] [CrossRef]
- Lam, J.S.; Leppert, J.T.; Belldegrun, A.S.; Figlin, R.A. Novel approaches in the therapy of metastatic renal cell carcinoma. World J. Urol. 2005, 23, 202–212. [Google Scholar] [CrossRef]
- Barry, M.J.; Simmons, L.H. Prevention of Prostate Cancer Morbidity and Mortality: Primary Prevention and Early Detection. Med. Clin. N. Am. 2017, 101, 787–806. [Google Scholar] [CrossRef]
- Dy, G.W.; George, J.L.; Forouzanfer, M.H.; Naghavi, M.; Fitzmaurice, C. Global Burden of Urologic Cancers, 1990–2013. Eur. Urol. 2017, 71, 437–446. [Google Scholar] [CrossRef]
- De Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B., Jr.; Saad, F.; et al. Abiraterone and increased survival in metastatic prostate cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef]
- Antonarakis, E.S.; Piulats, J.M.; Gross-Goupil, M.; Goh, J.; Ojamaa, K.; Hoimes, C.J.; Vaishampayan, U.; Berger, R.; Sezer, A.; Alanko, T.; et al. Pembrolizumab for Treatment-Refractory Metastatic Castration-Resistant Prostate Cancer: Multicohort, Open-Label Phase II KEYNOTE-199 Study. J. Clin. Oncol. 2020, 38, 395–405. [Google Scholar] [CrossRef]
- Graff, J.N.; Beer, T.M.; Alumkal, J.J.; Slottke, R.E.; Redmond, W.L.; Thomas, G.V.; Thompson, R.F.; Wood, M.A.; Koguchi, Y.; Chen, Y.; et al. A phase II single-arm study of pembrolizumab with enzalutamide in men with metastatic castration-resistant prostate cancer progressing on enzalutamide alone. J. Immunother. Cancer 2020, 8, e000642. [Google Scholar] [CrossRef]
- Hansen, A.R.; Massard, C.; Ott, P.A.; Haas, N.B.; Lopez, J.S.; Ejadi, S.; Wallmark, J.M.; Keam, B.; Delord, J.P.; Aggarwal, R.; et al. Pembrolizumab for advanced prostate adenocarcinoma: Findings of the KEYNOTE-028 study. Ann. Oncol. 2018, 29, 1807–1813. [Google Scholar] [CrossRef]
- Kwon, E.D.; Drake, C.G.; Scher, H.I.; Fizazi, K.; Bossi, A.; van den Eertwegh, A.J.; Krainer, M.; Houede, N.; Santos, R.; Mahammedi, H.; et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): A multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014, 15, 700–712. [Google Scholar] [CrossRef]
- Ebelt, K.; Babaryka, G.; Figel, A.M.; Pohla, H.; Buchner, A.; Stief, C.G.; Eisenmenger, W.; Kirchner, T.; Schendel, D.J.; Noessner, E. Dominance of CD4+ lymphocytic infiltrates with disturbed effector cell characteristics in the tumor microenvironment of prostate carcinoma. Prostate 2008, 68, 1–10. [Google Scholar] [CrossRef]
- Yunger, S.; Bar El, A.; Zeltzer, L.A.; Fridman, E.; Raviv, G.; Laufer, M.; Schachter, J.; Markel, G.; Itzhaki, O.; Besser, M.J. Tumor-infiltrating lymphocytes from human prostate tumors reveal anti-tumor reactivity and potential for adoptive cell therapy. Oncoimmunology 2019, 8, e1672494. [Google Scholar] [CrossRef]
- Martin, A.M.; Nirschl, T.R.; Nirschl, C.J.; Francica, B.J.; Kochel, C.M.; van Bokhoven, A.; Meeker, A.K.; Lucia, M.S.; Anders, R.A.; DeMarzo, A.M.; et al. Paucity of PD-L1 expression in prostate cancer: Innate and adaptive immune resistance. Prostate Cancer Prostatic Dis. 2015, 18, 325–332. [Google Scholar] [CrossRef]
- Mercader, M.; Bodner, B.K.; Moser, M.T.; Kwon, P.S.; Park, E.S.; Manecke, R.G.; Ellis, T.M.; Wojcik, E.M.; Yang, D.; Flanigan, R.C.; et al. T cell infiltration of the prostate induced by androgen withdrawal in patients with prostate cancer. Proc. Natl. Acad. Sci. USA 2001, 98, 14565–14570. [Google Scholar] [CrossRef]
- Haffner, M.C.; Guner, G.; Taheri, D.; Netto, G.J.; Palsgrove, D.N.; Zheng, Q.; Guedes, L.B.; Kim, K.; Tsai, H.; Esopi, D.M.; et al. Comprehensive Evaluation of Programmed Death-Ligand 1 Expression in Primary and Metastatic Prostate Cancer. Am. J. Pathol. 2018, 188, 1478–1485. [Google Scholar] [CrossRef]
- Burningham, Z.; Hashibe, M.; Spector, L.; Schiffman, J.D. The epidemiology of sarcoma. Clin. Sarcoma Res. 2012, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Messiou, C.; Moskovic, E.; Vanel, D.; Morosi, C.; Benchimol, R.; Strauss, D.; Miah, A.; Douis, H.; van Houdt, W.; Bonvalot, S. Primary retroperitoneal soft tissue sarcoma: Imaging appearances, pitfalls and diagnostic algorithm. Eur. J. Surg. Oncol. 2017, 43, 1191–1198. [Google Scholar] [CrossRef]
- Gronchi, A.; Strauss, D.C.; Miceli, R.; Bonvalot, S.; Swallow, C.J.; Hohenberger, P.; Van Coevorden, F.; Rutkowski, P.; Callegaro, D.; Hayes, A.J.; et al. Variability in patterns of recurrence after resection of primary retroperitoneal sarcoma (RPS): A report on 1007 patients from the multiinstitutional collaborative RPS Working Group. Ann. Surg. 2016, 263, 1002–1009. [Google Scholar] [CrossRef]
- D’Ambrosio, L.; Touati, N.; Blay, J.Y.; Grignani, G.; Flippot, R.; Czarnecka, A.M.; Piperno-Neumann, S.; Martin-Broto, J.; Sanfilippo, R.; Katz, D.; et al. Doxorubicin plus dacarbazine, doxorubicin plus ifosfamide, or doxorubicin alone as a first-line treatment for advanced leiomyosarcoma: A propensity score matching analysis from the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group. Cancer 2020, 126, 2637–2647. [Google Scholar] [CrossRef] [PubMed]
- Mitsis, D.; Francescutti, V.; Skitzki, J. Current immunotherapies for sarcoma: Clinical trials and rationale. Sarcoma 2016, 2016, 9757219. [Google Scholar] [CrossRef] [PubMed]
- Angelo, S.P.D. Manipulating the immune system with checkpoint inhibitors for patients with metastatic sarcoma. Am. Soc. Clin. Oncol. Educ. Book 2016, 36, e558–e564. [Google Scholar] [CrossRef]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; Van De Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non-Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv. Anat. Pathol. 2017, 24, 311–335. [Google Scholar] [CrossRef]
- Galsky, M.D.; Arija, J.Á.A.; Bamias, A.; Davis, I.D.; De Santis, M.; Kikuchi, E.; Garcia-Del-Muro, X.; De Giorgi, U.; Mencinger, M.; Izumi, K.; et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2020, 395, 1547–1557. [Google Scholar] [CrossRef]
- Sharma, P.; Shen, Y.; Wen, S.; Yamada, S.; Jungbluth, A.A.; Gnjatic, S.; Bajorin, D.F.; Reuter, V.E.; Herr, H.; Old, L.J.; et al. CD8 tumor-infiltrating lymphocytes are predictive of survival in muscle-invasive urothelial carcinoma. Proc. Natl. Acad. Sci. USA 2007, 104, 3967–3972. [Google Scholar] [CrossRef] [PubMed]
- Kolbeck, P.C.; Kaveggia, F.F.; Johansson, S.L.; Gune, M.; Taylor, R. The relationships among tumor-infiltrating lymphocytes, histopathologic findings, and long-term clinical follow-up in renal cell carcinoma. Mod. Pathol. 1992, 5, 420–425. [Google Scholar] [PubMed]
- Bromwich, E.J.; McArdle, P.A.; Canna, K.; McMillan, D.; McNicol, A.; Brown, M.; Aitchisonet, M. The relationship between T-lymphocyte infiltration, stage, tumour grade and survival in patients undergoing curative surgery for renal cell cancer. Br. J. Cancer. 2003, 89, 1906–1908. [Google Scholar] [CrossRef] [PubMed]
- Remark, R.; Alifano, M.; Cremer, I.; Lupo, A.; Dieu-Nosjean, M.C.; Riquet, M.; Crozet, L.; Ouakrim, H.; Goc, J.; Cazes, A.; et al. Characteristics and Clinical Impacts of the Immune Environments in Colorectal and Renal Cell Carcinoma Lung Metastases: Influence of Tumor Origin. Clin. Cancer Res. 2013, 19, 4079–4091. [Google Scholar] [CrossRef] [PubMed]
- Nakano, O.; Sato, M.; Naito, Y.; Suzuki, K.; Orikasa, S.; Aizawa, M.; Suzuki, Y.; Shintaku, I.; Nagura, H.; Ohtani, H. Proliferative Activity of Intratumoral CD8+ T-Lymphocytes As a Prognostic Factor in Human Renal Cell Carcinoma. Cancer Res. 2001, 61, 5132–5136. [Google Scholar] [PubMed]
- Hotta, K.; Sho, M.; Fujimoto, K.; Shimada, K.; Yamato, I.; Anai, S.; Konishi, N.; Hirao, Y.; Nonomura, K.; Nakajima, Y. Prognostic significance of CD45RO+ memory T cells in renal cell carcinoma. Br. J. Cancer. 2011, 105, 1191–1196. [Google Scholar] [CrossRef]
- Irani, J.; Goujon, J.M.; Ragni, E.; Peyrat, L.; Hubert, J.; Saint, F.; Mottet, N. High-grade inflammation in prostate cancer as a prognostic factor for biochemical recurrence after radical prostatectomy. Urology 1999, 54, 467–472. [Google Scholar] [CrossRef]
- Karja, V.; Aaltomaa, S.; Lipponen, P.K.; Isotalo, T.; Talja, M.; Mokka, R. Tumour-infiltrating Lymphocytes: A Prognostic Factor of PSA-free Survival in Patients with Local Prostate Carcinoma Treated by Radical Prostatectomy. Anticancer Res. 2005, 25, 4435–4438. [Google Scholar]
- Zeigler-Johnson, C.; Morales, K.H.; Lal, P.; Feldman, M. The Relationship between Obesity, Prostate Tumor Infiltrating Lymphocytes and Macrophages, and Biochemical Failure. PLoS ONE 2016, 11, e0159109. [Google Scholar] [CrossRef]
- Richardsen, E.; Uglehaus, R.D.; Due, J.; Busch, C.; Busund, L.T. The prognostic impact of M-CSF, CSF-1 receptor, CD68 and CD3 in prostatic carcinoma. Histopathology 2008, 53, 30–38. [Google Scholar] [CrossRef]
- McArdle, P.A.; Canna, K.; McMillan, D.C.; McNicol, A.M.; Campbell, R.; Underwood, M.A. The relationship between T-lymphocyte subset infiltration and survival in patients with prostate cancer. Br. J. Cancer 2004, 91, 541–543. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Types of Tumor | No. of Patients | Treatment | Makers or Assessment | Assay | Clinical Relevance | Reference No. |
|---|---|---|---|---|---|---|
| Urothelial Carcinoma (UC) | ||||||
| NMIBC | 154 | TURBT followed by intravesical BCG | FOXP3, CD204 | IHC | High Tregs and tumor-associated macrophages were associated with a high risk of intravesical recurrence. | [26] |
| NMIBC | 115 | TURBT | CD3, CD4, CD8, CD20, CD56, CD68, granzyme B | IHC | Low CD3+ TILs and CD8+ TILs were associated with a high risk of intravesical recurrence. | [27] |
| NMIBC | 131 | TURBT | CD4 | IHC | High CD4+ TILs were associated with poor OS. | [28] |
| NMIBC | 102 | TURBT | CD8, CD66b | IHC | High tumor-infiltrating neutrophils and NLR were associated with poor OS. High TILs were related to longer OS. | [29] |
| MIBC | 67 | Radical cystectomy | CD3, CD8 | IHC | High CD8+ TILs and CD3+ TILs in the invasion margin were associated with better DFS and OS. | [30] |
| MIBC | 406 | Radical cystectomy | CD3D, CD4, CD8A | mRNA (TCGA dataset) | High CD3D/CD4 ratio was associated with improved survival. The power was stronger in basal-squamous tumors. | [31] |
| MIBC | 145 | Radical cystectomy | CD8, FOXP3, CD20, PD-1, PD-L1 | IHC | High density of CD8, FOXP3, CD20, and PD-1 was associated with a low risk of recurrence. | [32] |
| Bladder cancer and UTUC | 52 and 18 | Surgical resection | Nine extracellular surface markers | FCM | The immunologically activated group showed poorer PFS and CSS compared that in to the CD4+ T-cell-dominant group in bladder cancer. However, there was no significant difference in UTUC. | [33] |
| UTUC | 162 | Radical nephroureterectomy | PD-L1 | IHC | High PD-L1 expression in tumor cells was associated with shorter CSS. High PD-L1 expression on TILs was associated with longer CSS. | [34] |
| UTUC | 423 | Radical nephroureterectomy | PD-1, PD-L1 | IHC | High PD-1 level was associated with poor CSS and OS. In patients with organ-confined disease (pT2≤, N0/xM0), high PD-L1 was associated with a high risk of recurrence and poor OS. | [35] |
| UTUC | 88 | Radical nephroureterectomy | CD4, CD8, CD20, APE1, NTH1, OGG1, XRCC1, polβ, STING, IRF3, PD-L1, PD-L2 | IHC | High CD8+ TILs were associated with poor DFS. | [36] |
| Metastatic UC | 259 | Platinum-based chemotherapy | Recommendations by an International TILs Working Group 2014 | Hematoxylin and eosin staining | High TIL levels were associated with better OS after chemotherapy both in bladder cancer and UTUC. | [37] |
| Renal cell carcinoma (RCC) | ||||||
| ccRCC | 43 | Untreated stage III/IV disease | CD4, CD45RA, CD8, CD11, HLA-DR, CD3, CD16, CD57 | FCM | An increase in CD8+/CD11- and a decrease in CD4+/CD45RA- cells were observed along with the aggravation of tumor stage and grade. | [39] |
| ccRCC | 473 | Previously treated | Th17, CTL, Tregs, Th2 | mRNA (TCGA dataset) | Long-lived patients have high levels of Th17 and CD8+ T cells, while short-lived patients have high levels of Tregs and Th2. | [40] |
| RCC | 891 | Untreated | M1 macrophages, M2 macrophages, memory CD4+ T, γδ T, CD8+ T, Tregs, naïve CD4+ T, NK cell, mast cells, B cells, DC, monocytes, plasma cells, neutrophils, eosinophils | CIBERSORT | CD8+ T cells were associated with prolonged OS. A higher proportion of regulatory T cells was associated with a poorer outcome. M1 macrophages were associated with a favorable outcome, while M2 macrophages indicated a poorer outcome. | [41] |
| Metastatic ccRCC | 167 | Previously treated | CD8, PD-1, TIM-3, LAG-3 | IHC | A high percentage of CD8+/PD-1+/TIM-3-/LAG-3- cells correlated with high levels of T-cell activation and were associated with longer median irPFS and higher irORR. | [42] |
| ccRCC | 199 | Previously treated | PD-1, FOXP3 | IHC | PD1-positive or FOXP3-positive lymphocytes can be used as significant prognostic indicators, and PD1 positivity could be very helpful in the prediction of latent distant metastasis. | [43] |
| Metastatic ccRCC | 58 | interleukin-2-based immunotherapy | FOXP3 | IHC | Intratumoral FOXP3-positive regulatory immune cells significantly increased during interleukin-2–based immunotherapy, and high numbers of on-treatment FOXP3-positive cells were correlated with poor prognosis. | [44] |
| ccRCC | 125 | Radical nephrectomy or nephron-sparing surgery | CD4, FOXP3 | IHC | Increased peritumoral Tregs are associated with a poorer prognosis. | [45] |
| ccRCC | 170 | Radical nephrectomy or nephron-sparing surgery | CD4, CD25, FOXP3 | IHC | Increased number of CD4+CD25+Foxp3+ T cells was not associated with RCC death. In contrast, CD4+CD25+Foxp3- T cells, which may represent a unique set of Tregs or activated helper T cells, were significantly associated with the outcome. | [46] |
| RCC | 97 | Previously treated | CD45, CD3, CD4, CD8, CD45RA, ICOS, Tim3, CD25, PD-1, FOXP3 | FCM | Tumor grade significantly correlated with dysfunction of both CD4+ and CD8+ TILs and the efficacy of nivolumab treatment. | [47] |
| Localized ccRCC | 40 | Radical nephrectomy or nephron-sparing surgery | CD3, CD4, CD8, CD45RA, CCR7, CD69, CD38, CD40L, ICOS, GITR, PD-1, TIM-3, CTLA-4, LAG-3, CD127, CD25 | FCM | Infiltration with CD8+PD-1+Tim-3+Lag-3+ exhausted TILs and ICOS+ Tregs identified patients with deleterious prognosis who could benefit from adjuvant therapy with TME-modulating agents and checkpoint blockade. | [48] |
| Metastatic RCC | 231 | Tyrosine kinase inhibitors | CD8, PD-1, PD-L1 | IHC | Increased numbers of CD8+ T cells are significantly associated with improved survival in patients with mRCC treated with TKIs. PD-1 could be used as a predictive and prognostic factor. | [49] |
| Prostate cancer (PCa) | ||||||
| Localized PCa | 126 | Radical prostatectomy | CD8, FOXP3 | IHC | High CD8+ TILs were significantly associated with good DFS, whereas FOXP3+Treg tumor infiltration was significantly correlated with poor DFS. | [50] |
| Localized PCa | 535 | Radical prostatectomy | CD8 | IHC | A high density of CD8+ TILs is an independent negative prognostic factor for biochemical failure-free survival. | [51] |
| Biochemical recurence after radical prostatectomy | 22 | Salvage radiotherapy | PD-1, FOXP3 | IHC | High PD-1 and FOXP3+ Treg tumor infiltration was significantly associated with short PFS. | [52] |
| Localized PCa | 75 | Radical prostatectomy | CCR4 | IHC | CCR4+ Tregs are highly infiltrated in the prostate tissue with poor prognosis, with a strong potential to progress to CRPC. | [53] |
| Retroperitoneal sarcoma (RSar) | ||||||
| RSar (various types) | 51 | Surgical resection | PD-1, PD-L1, PD-L2, Ki-67 | IHC | The prognostic value of PD-L1, PD-L2, and PD-1 expression was evaluated, and only high expression of PD-1 was a possible predictor of postoperative recurrence. | [54] |
| RSar (WDLPS) | 6 | Surgical resection | CD4, CD8, CD20 | IHC | CD8+ T cells were mostly seen in scattered gout of the tumor. CD4+ T cells were observed in clusters and follicles. CD20+ cells (B cells) were found almost exclusively in cluster and forming immature follicles. | [55] |
| RSar (WDLPS/DDLPS) | 8 | Surgical resection | CD3, CD4,CD8, PD-1, 4-1BB | IHC FCM | Cytotoxic CD8+ T cells accounted for 20% of CD3+ T cells. Notably, 65% of CD8+ T cells were positive for PD-1. Immune cell aggregates evaluated by IHC were associated with poorer prognosis in both well-differentiated and dedifferentiated retroperitoneal liposarcoma. | [56] |
| RSar (WDLPS/DDLPS/MLPS/PLPS) | 56 | Surgical resection | CD4, CD8, FOXP3, CD20, PD-1, PD-L1 | IHC | Higher FOXP3+ Treg or PD-1/PD-L1+ cells tended to be associated with poor prognosis. Heterogeneous TIL distribution was found in 50% of patients and tended to correlate with favorable disease-free survival. | [57] |
| Types of Tumor | No. of Patients | Treatment (Phase) | Outcomes and Response | Assay | Marker Assessment | Clinical Relevance of Maker Assessment | Reference No. | ||
|---|---|---|---|---|---|---|---|---|---|
| OS | PFS | ORR | |||||||
| Urothelial carcinoma (UC) | |||||||||
| Advanced Muc (JAVELIN Solid Tumor) | 249 | Second-line avelumab (Phase I) | 6.5 months | 1.7 months | 17% | NA | NA | NA | [59] |
| Advanced mUC (CheckMate 032) | 274 | Platinum-pretreated nivolumab ± ipilimumab (Phase I/II) | 10.4 months in NIVO3 7.4 months in NIVO3+IPI1 27.6 months in NIVO1+IPI3 | 2.8 months in NIVO3 2.6 months in NIVO3+IPI1 4.9 months in NIVO1+IPI3 | 26% in NIVO3 27% in NIVO3+IPI1 38% in NIVO1+IPI3 | IHC Dako 28-8 | PD-L1 expression in tumor cells | PD-L1 expression was not associated with ORR. High PD-L1 expression was associated with longer mOS. | [60] |
| Advanced mUC | 191 | Durvalumab (Phase I/II) | 18.2 months | 1.5 months | 18% | IHC Ventana SP263 | PD-L1 (combined assessment of PD-L1 staining of tumor cells and immune cells) | Tumor response to durvalumab was not associated with PD-L1 staining. | [61] |
| Advanced mUC (CheckMate 275) | 270 | Second-line Nivolumab (Phase II) | 8.7 months | 2.0 months | 20% | IHC Dako 28-8 | PD-L1 expression in tumor cells | OR was observed in 28% of patients with PD-L1 expression of 5% or greater, 24% of patients with PD-L1 expression of 1% or greater, and 16% of patients with PD-L1 expression of less than 1%. | [62] |
| Advanced mUC (KEYNOTE-045) | 542 | Second-line Pembrolizuma vs. chemotherapy (Phase III) | 10.3 vs. 7.4 months HR: 0.73 p value: 0.002 | 2.1 vs. 3.3 months HR: 0.98 p value: 0.42 | 21% vs. 11% | IHC Dako 22C3 | PD-L1 combined positive score (CPS; the percentage of PD-L1-expressing tumor and infiltrating immune cells relative to the total number of tumor cells) | Treatment response was similar in patients with a CPS of 10% or more. | [25] |
| Advanced mUC (IMvigor211) | 931 | Second-line Atezolizumab vs. chemotherapy (Phase III) | 11.1 vs. 10.6 months HR:0.87 p value: 0.41 | 2.4 vs. 4.2 months HR: 1.01 | 23% vs. 22% | IHC Ventana SP142 | PD-L1 expression on <1% [IC0], 1% to <5% [IC1], and ³5% of tumor-infiltrating immune cells [IC2/3] | Atezolizumab was not associated with longer OS than chemotherapy in patients with IC2/3. | [63] |
| Renal cell carcinoma (RCC) | |||||||||
| Metastatic RCC (BTCRC-GU14-003) | 61 | Second or Third-line pembrolizumab plus bevacizumab (Phase Ib/II) | NA at the median follow-up of 28.3 months | 20.7 months | 60.90% | IHC Dako 22C3 | PD-L1 expression in tumor cells | Patients with tumors overexpressing PD-L1 > 0 showed a trend toward better PFS after 20 months, but there was no statistical difference in overall PFS. | [64] |
| Metastatic RCC | 30 | Second or Third-line lenvatinib plus pembrolizumab (Phase Ib/II) | NA | 19.8 months | 70% | NA | NA | NA | [65] |
| Advanced RCC (KEYNOTE-426) | 861 | First-line pembrolizumab plus axitinib vs. sunitinib (Phase III) | HR: 0.53 p value: <0.0001 | 15.1 vs. 11.1 months HR = 0.69 p value: <0.001 | 59.7% vs. 35.7% | IHCDako 22C3 | PD-L1 combined positive score (the percentage of PD-L1+ tumor and infiltrating immune cells/the total tumor cells) | The benefit of pembrolizumab plus axitinib was observed in patients with tumors expressing PD-L1 expression and those with tumors without PD-L1 expression. | [66] |
| Advanced RCC (JAVELIN Renal 101) | 886 | First-line avelumab plus axitinib vs. sunitinib (Phase III) | 12.0 and 11.5 months HR: 0.78 p value: 0.14 | 13.8 vs. 8.4 months HR = 0.69 p value: <0.001 | 51.4% vs. 25.7% | IHC Ventana SP263 | PD-L1 expression in tumor cells | ORR among patients with PD-L1–positive tumors who received avelumab plus axitinib was twice as that in patients who received sunitinib (55.2% vs. 25.5%, respectively). | [67] |
| Advanced or Metastatic RCC (CheckMate 214) | 1096 | First-line nivolumab plus ipilimumab vs. sunitinib (Phase III) | NR and 26.6 months HR: 0.66 p value: <0.0001 | 8.2 vs. 8.3 months HR = 0.77 p value: 0.0014 | 42% vs. 29% | IHC Dako 28-8 | PD-L1 expression in tumor cells | Partial responders and complete responders to nivolumab plus ipilimumab both had higher baseline tumor PD-L1 expression than that in non-responders. | [68] |
| Advanced or Metastatic RCC (IMmotion151 trial) | 915 | First-line atezolizumab plus bevacizumab vs. sunitinib (Phase III) | 33.6 and 34.9 months HR = 0.93 p value: 0.48 | 11.2 and 8.4 months HR = 0.83 p value: 0.022 | 37% vs. 33% | IHC Ventana SP142 | PD-L1 expression in tumor cells | In the PD-L1 positive population, the median progression-free survival in the atezolizumab plus bevacizumab group was significantly longer than that in the sunitinib group. PD-L1 can be used as a supporting tool for treatment selection. | [69] |
| Advanced or Metastatic RCC (CheckMate 025) | 821 | Second or Third-line Nivolumab vs. everolimus (Phase III) | 25.0 and 19.6 months HR: 0.73 p value: 0.002 | 4.6 vs. 4.4 months HR = 0.88 p value: 0.11 | 25% vs. 5% | IHC Dako 28-8 | PD-L1 expression in tumor cells | Higher levels of PD-L1 expression are associated with poorer survival, while it does not support PD-L1 as a marker of treatment benefit. | [70] |
| Prostate cancer (PCa)/castration resistant PCa (CRPC) | |||||||||
| Metastatic CRPCKEYNOTE-199 | 258 | Pembrolizumab after docetaxel or ARATs | 9.5, 7.9, and 14.1 months in cohort 1 (PD-L1 positive), cohort 2 (PD-L1 negative), and cohort 3 (Bone-predominant) | 2.1, 2.1, and 3.7 months in cohort 1 (PD-L1 positive), cohort 2 (PD-L1 negative), and cohort 3 (Bone-predominant) | 7% and 2 % in cohort 1 (PD-L1 positive) and cohort 2 (PD-L1 negative) | IHC Dako 22C3 | PD-L1 expression and aberrations of homologous recombination repair (HRR) gene in tumor cells | There were no significant differences in the response to pemblolizumab between the PD-L1-positive and -negative groups. | [71] |
| Metastatic CRPC | 28 | Pemblolizumab and enzalutamide | 22.2 months | 3.7 months (PSA-PFS) | 18% | IHC and FCM | PD-L1 expression in tumor cells | The frequency of granzyme B+ CD8+ and perforin+CD8+ T cells were higher in responders those that in non-responders. | [72] |
| Retroperitoneal sarcoma (RSar) | |||||||||
| STS and BS (SARC028) | 40 and 40 | Pembrolizumab (phase II) | 12.3 months (95% CI, 8.5–18.3) | 4.2mounths (95% CI, 2.0–5.3) | NA | IHC Dako 22C3 | Score was expressed as percentage of tumour cells positive for PD-L1. A tumour was considered positive for PD-L1 expression if more than 1% of its cells showed membranous staining. | PD-L1 expression was observed in only 5% of samples; both were UPS and responded to therapy. Pembrolizumab showed encouraging activity in patients with UPS or DDLPS. | [73] |
| Advanced or metastaic STS and BS (Alliance A091401) | 43 and 42 | Nivolumab vs. Nivolumab+ipilimmab (phase II) | 10.7 and 14.3 months (95% CI, 5.5–15.4 and NA) | 1.7 and 4.1 months (95% CI, 1.4–4.3 and 1.4–4.7) | NA | NA | NA | Treatment with nivolumab plus ipilimumab in an unselected cohort of heavily treated patients with advanced sarcoma, achieved a proportion of 16% of 38 patients with confirmed objective responses, which is similar to the results obtained with standard chemotherapy. | [74] |
| Locally advanced or metastaic sarcoma | 20 | T-VEC plus pemblolizumab (phase II) | 18.7 months (95% CI, 12.3–NA) | 4.3 months (95% CI, 3.2–NA) | 30% | IHC | PD-L1 tumor membrane expression and CD3+/CD8+ TILs at the infiltrating edge of the tumor. The patients underwent pretreatment and posttreatment tumor biopsies. | The data show that 64% of the posttreatment tumors were PD-L1 positive and 55% of patients converted from PD-L1 negative to PD-L1 positive after treatment. | [75] |
| Advanced sarcomas including alveolar soft-part sarcoma | 33 | Axitinib plus pembrolizumab (phase II) | 18.7 months (95% CI, 12.0–NA) | 4.7 months (95% CI, 3.0–9.4) | 25% | IHC | PD-L1 expression in sarcoma cells | PD-L1 expression was positive in 52% of patients with evaluable tumor biopsy samples. Neither PD-L1 positivity nor increased TIL score correlated with progression-free survival of longer than 6 months or with achieving a partial response. | [76] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyake, M.; Hori, S.; Owari, T.; Oda, Y.; Tatsumi, Y.; Nakai, Y.; Fujii, T.; Fujimoto, K. Clinical Impact of Tumor-Infiltrating Lymphocytes and PD-L1-Positive Cells as Prognostic and Predictive Biomarkers in Urological Malignancies and Retroperitoneal Sarcoma. Cancers 2020, 12, 3153. https://doi.org/10.3390/cancers12113153
Miyake M, Hori S, Owari T, Oda Y, Tatsumi Y, Nakai Y, Fujii T, Fujimoto K. Clinical Impact of Tumor-Infiltrating Lymphocytes and PD-L1-Positive Cells as Prognostic and Predictive Biomarkers in Urological Malignancies and Retroperitoneal Sarcoma. Cancers. 2020; 12(11):3153. https://doi.org/10.3390/cancers12113153
Chicago/Turabian StyleMiyake, Makito, Shunta Hori, Takuya Owari, Yuki Oda, Yoshihiro Tatsumi, Yasushi Nakai, Tomomi Fujii, and Kiyohide Fujimoto. 2020. "Clinical Impact of Tumor-Infiltrating Lymphocytes and PD-L1-Positive Cells as Prognostic and Predictive Biomarkers in Urological Malignancies and Retroperitoneal Sarcoma" Cancers 12, no. 11: 3153. https://doi.org/10.3390/cancers12113153
APA StyleMiyake, M., Hori, S., Owari, T., Oda, Y., Tatsumi, Y., Nakai, Y., Fujii, T., & Fujimoto, K. (2020). Clinical Impact of Tumor-Infiltrating Lymphocytes and PD-L1-Positive Cells as Prognostic and Predictive Biomarkers in Urological Malignancies and Retroperitoneal Sarcoma. Cancers, 12(11), 3153. https://doi.org/10.3390/cancers12113153