Vascular Complications in Patients with Hepatocellular Carcinoma Treated with Sorafenib

 , , , ,
, , , ,
Simple Summary
Abstract
1. Introduction
2. Results
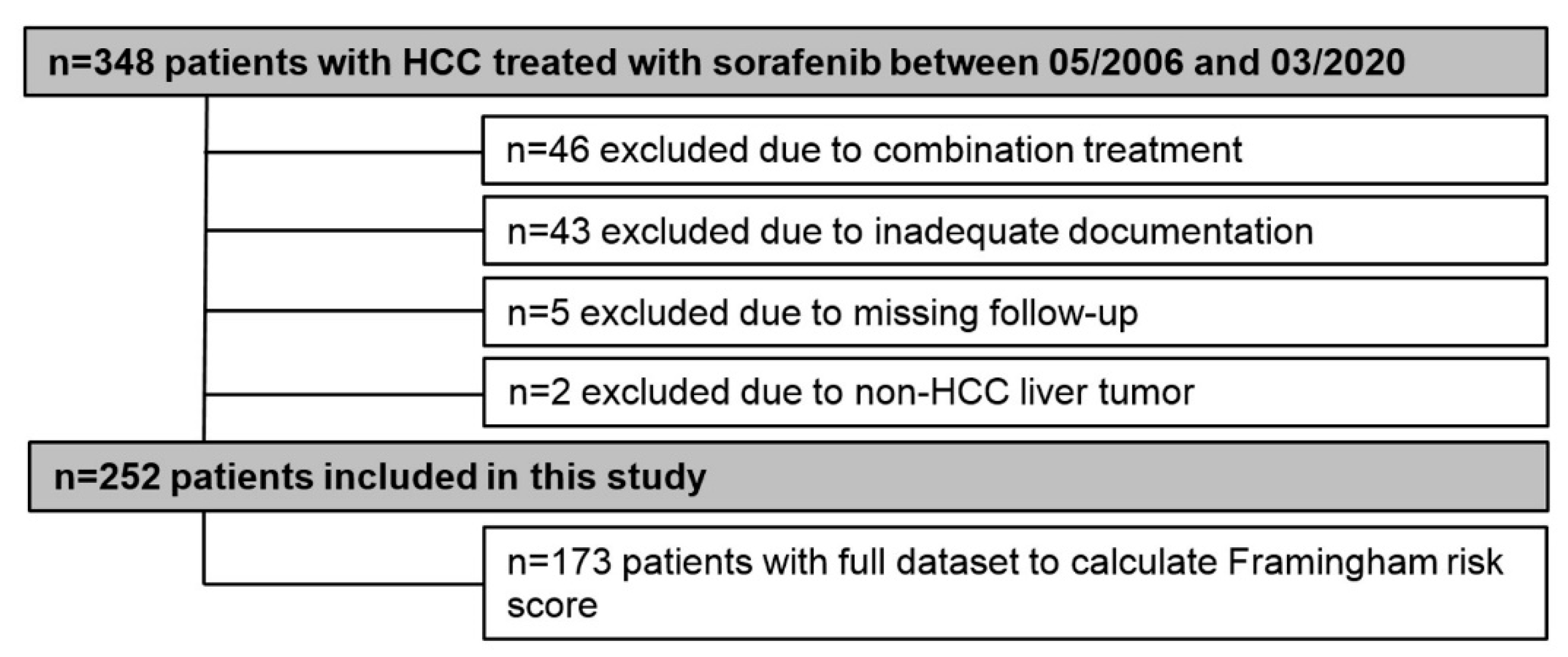
2.1. Patients
2.2. Prevalence of Cardiovascular Risk Factors
2.3. Arterial and Venous Thromboembolic Complications
2.4. Incidence of Arterial Vascular Complications and Impact of Cardiovascular Risk on Survival
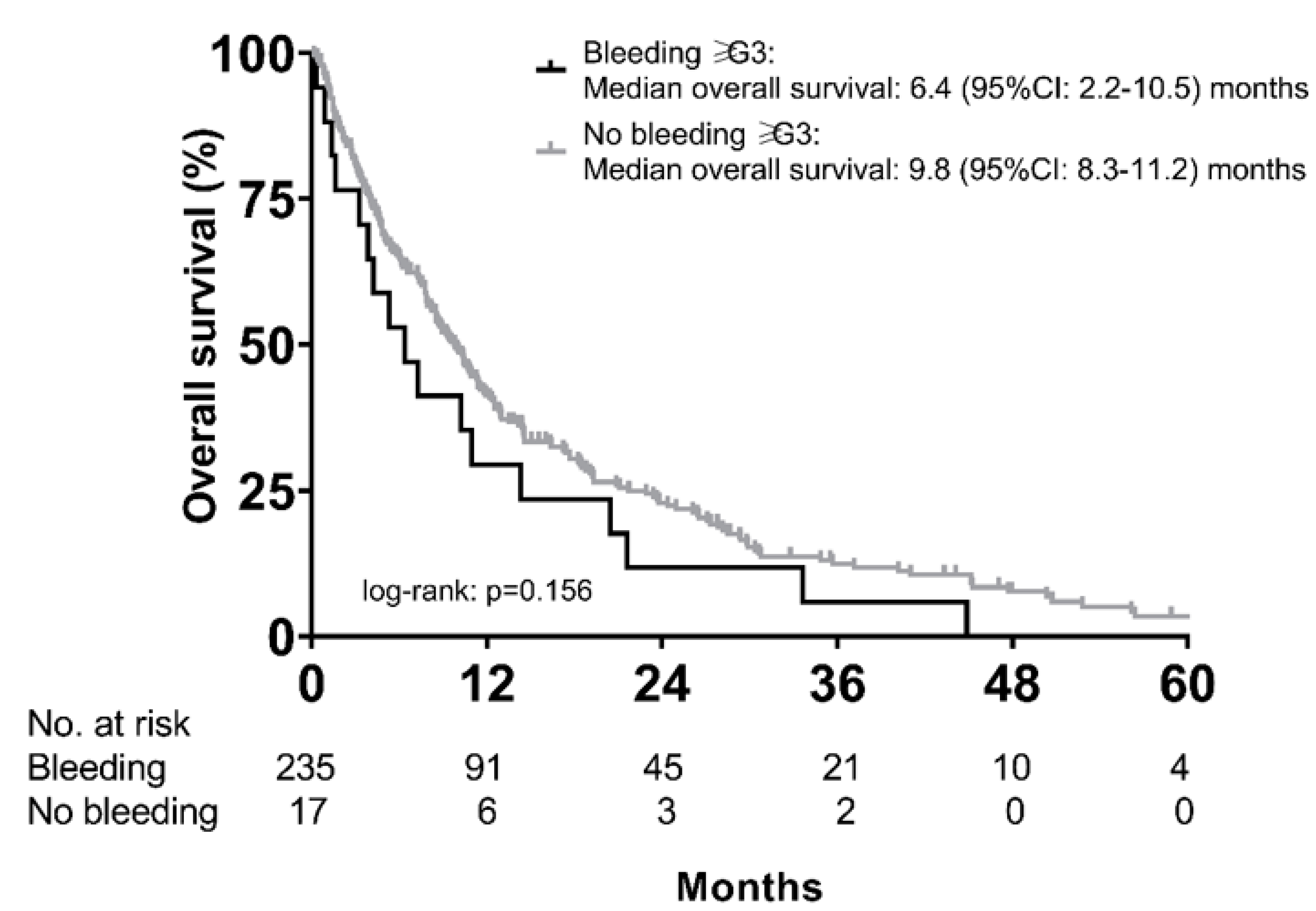
2.5. Bleeding Complications
2.6. Incidence of Vascular (Thromboembolic and Bleeding) Events According to Sorafenib Starting Dose
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patients and Definitions
4.3. Determination of Cardiovascular Risk—Framingham Risk Score
4.4. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- EASL Clinical Practice Guidelines. Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Blachier, M.; Leleu, H.; Peck-Radosavljevic, M.; Valla, D.C.; Roudot-Thoraval, F. The burden of liver disease in Europe: A review of available epidemiological data. J. Hepatol. 2013, 58, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Trauner, M.; Peck-Radosavljevic, M.; Sieghart, W. Cancer and liver cirrhosis: Implications on prognosis and management. ESMO Open 2016, 1, e000042. [Google Scholar] [CrossRef]
- Pinter, M.; Peck-Radosavljevic, M. Review article: Systemic treatment of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2018, 48, 598–609. [Google Scholar] [CrossRef]
- Yamashita, T.; Kudo, M.; Ikeda, K.; Izumi, N.; Tateishi, R.; Ikeda, M.; Aikata, H.; Kawaguchi, Y.; Wada, Y.; Numata, K.; et al. REFLECT—A phase 3 trial comparing efficacy and safety of lenvatinib to sorafenib for the treatment of unresectable hepatocellular carcinoma: An analysis of Japanese subset. J. Gastroenterol. 2020, 55, 113–122. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar]
- Kudo, M. Scientific Rationale for Combined Immunotherapy with PD-1/PD-L1 Antibodies and VEGF Inhibitors in Advanced Hepatocellular Carcinoma. Cancers 2020, 12, 1089. [Google Scholar] [CrossRef]
- Pinter, M.; Scheiner, B.; Peck-Radosavljevic, M. Immunotherapy for advanced hepatocellular carcinoma: A focus on special subgroups. Gut 2020. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. Targeted and immune therapies for hepatocellular carcinoma: Predictions for 2019 and beyond. World J. Gastroenterol. 2019, 25, 789–807. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased alpha-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Carter, C.; Tang, L.; Wilkie, D.; McNabola, A.; Rong, H.; Chen, C.; Zhang, X.; Vincent, P.; McHugh, M.; et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004, 64, 7099–7109. [Google Scholar] [CrossRef] [PubMed]
- Nalluri, S.R.; Chu, D.; Keresztes, R.; Zhu, X.; Wu, S. Risk of venous thromboembolism with the angiogenesis inhibitor bevacizumab in cancer patients: A meta-analysis. JAMA 2008, 300, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Qadir, H.; Ethier, J.L.; Lee, D.S.; Thavendiranathan, P.; Amir, E. Cardiovascular toxicity of angiogenesis inhibitors in treatment of malignancy: A systematic review and meta-analysis. Cancer Treat. Rev. 2017, 53, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Touyz, R.M.; Herrmann, S.M.S.; Herrmann, J. Vascular toxicities with VEGF inhibitor therapies-focus on hypertension and arterial thrombotic events. J. Am. Soc. Hypertens. JASH 2018, 12, 409–425. [Google Scholar] [CrossRef]
- Escudier, B.; Eisen, T.; Stadler, W.M.; Szczylik, C.; Oudard, S.; Siebels, M.; Negrier, S.; Chevreau, C.; Solska, E.; Desai, A.A.; et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 125–134. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kamba, T.; McDonald, D.M. Mechanisms of adverse effects of anti-VEGF therapy for cancer. Brit. J. Cancer 2007, 96, 1788–1795. [Google Scholar] [CrossRef]
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J. Hepatol. 2018, 68, 526–549. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Anstee, Q.M.; Arias-Loste, M.T.; Bantel, H.; Bellentani, S.; Caballeria, J.; Colombo, M.; Craxi, A.; Crespo, J.; Day, C.P.; et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J. Hepatol. 2018, 69, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Thaler, J.; Ay, C.; Pabinger, I. Venous thromboembolism in cancer patients—Risk scores and recent randomised controlled trials. Thromb. Haemost. 2012, 108, 1042–1048. [Google Scholar] [PubMed]
- Pabinger, I.; van Es, N.; Heinze, G.; Posch, F.; Riedl, J.; Reitter, E.M.; Di Nisio, M.; Cesarman-Maus, G.; Kraaijpoel, N.; Zielinski, C.C.; et al. A clinical prediction model for cancer-associated venous thromboembolism: A development and validation study in two independent prospective cohorts. Lancet Haematol. 2018, 5, e289–e298. [Google Scholar] [CrossRef]
- Lisman, T.; Leebeek, F.W.; de Groot, P.G. Haemostatic abnormalities in patients with liver disease. J. Hepatol. 2002, 37, 280–287. [Google Scholar] [CrossRef]
- O’Leary, J.G.; Greenberg, C.S.; Patton, H.M.; Caldwell, S.H. AGA Clinical Practice Update: Coagulation in Cirrhosis. Gastroenterology 2019, 157, 34–43.e1. [Google Scholar] [CrossRef]
- Scheiner, B.; Northup, P.G.; Gruber, A.B.; Semmler, G.; Leitner, G.; Quehenberger, P.; Thaler, J.; Ay, C.; Trauner, M.; Reiberger, T.; et al. The impact of ABO blood type on the prevalence of portal vein thrombosis in patients with advanced chronic liver disease. Liver Int. 2020, 40, 1415–1426. [Google Scholar] [CrossRef]
- Zangari, M.; Fink, L.M.; Elice, F.; Zhan, F.; Adcock, D.M.; Tricot, G.J. Thrombotic events in patients with cancer receiving antiangiogenesis agents. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 4865–4873. [Google Scholar] [CrossRef]
- Llovet, J.M.; Bruix, J. Molecular targeted therapies in hepatocellular carcinoma. Hepatology 2008, 48, 1312–1327. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Di Bisceglie, A.M.; Bruix, J.; Kramer, B.S.; Lencioni, R.; Zhu, A.X.; Sherman, M.; Schwartz, M.; Lotze, M.; Talwalkar, J.; et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J. Natl. Cancer Inst. 2008, 100, 698–711. [Google Scholar] [CrossRef] [PubMed]
- Tsigos, C.; Hainer, V.; Basdevant, A.; Finer, N.; Fried, M.; Mathus-Vliegen, E.; Micic, A.; Maislos, M.; Roman, G.; Schutz, Y.; et al. Management of obesity in adults: European clinical practice guidelines. Obes. Facts 2008, 2, 106–116. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.; Atar, D.; Borch-Johnsen, K.; Boysen, G.; Burell, G.; Cifkova, R.; Dallongeville, J.; De Backer, G.; Ebrahim, S.; Gjelsvik, B.; et al. European guidelines on cardiovascular disease prevention in clinical practice: Executive summary: Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by representatives of nine societies and by invited experts). Eur. Heart J. 2007, 28, 2375–2414. [Google Scholar]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Characteristics/Statistics | Number (%) or Mean ± SD/Median (Range) |
|---|---|---|
| N, % | 252 (100%) | |
| Age (years) | Mean ± SD | 66 ± 9.4 |
| Range | 28–88 | |
| Sex | Male | 215 (85%) |
| Female | 37 (15%) | |
| Etiology | ALD | 93 (37%) |
| Viral | 71 (28%) | |
| Unknown | 53 (21%) | |
| Other | 35 (14%) | |
| Cirrhosis a | No Yes | 55 (22%) 188 (75%) |
| Child–Pugh Classification | A | 114 (45%) |
| B | 95 (38%) | |
| C | 43 (17%) | |
| ECOG PS | 0 | 149 (59%) |
| ≥1 | 103 (41%) | |
| Macrovascular | No | 128 (51%) |
| Invasion | Yes | 124 (49%) |
| Extrahepatic | No | 176 (70%) |
| Metastases | Yes | 76 (30%) |
| BCLC stage | A | 18 (7%) |
| B | 45 (18%) | |
| C | 146 (58%) | |
| D | 43 (17%) | |
| Prior therapy | None | 141 (56%) |
| TACE/MWA/RFA | 59 (23%) | |
| Resection | 12 (5%) | |
| Other | 40 (16%) | |
| AFP (IU/mL) b | Median (Range) | 49 (1–50,000) |
| Platelet Count (G/L) c | Median (Range) | 148 (29–778) |
| Diabetes | NIDDM | 76 (30%) |
| IDDM | 19 (8%) | |
| None | 157 (62%) | |
| BMI (kg/m2) d | Mean ± SD | 26 ± 5.7 |
| Obesity (BMI ≥ 30 kg/m2) | 58 (23%) | |
| Arterial Hypertension e | No | 96 (38%) |
| Yes | 154 (62%) | |
| Antihypertensive treatment * | No | 140 (56%) |
| Yes | 112 (44%) | |
| Smoking | No | 146 (58%) |
| Yes | 106 (42%) | |
| Hypercholesterinemia f (cutoff > 200 mg/dL) | No | 177 (76%) |
| Yes | 55 (24%) | |
| Statin therapy | No | 214 (85%) |
| Yes | 38 (15%) | |
| Anticoagulation + | No | 214 (85%) |
| Yes | 37 (15%) | |
| Antiplatelet therapy | No | 211 (84%) |
| Yes | 37 (15%) | |
| Hypertriglyceridemia g (cutoff > 200 mg/dL) | No | 216 (93%) |
| Yes | 16 (7%) | |
| Coronary heart disease | No | 229 (91%) |
| Yes | 23 (9%) | |
| Arterial occlusive disease | No | 230 (92%) |
| Yes | 22 (8%) | |
| Renal function according to CKD stages (GFR in mL/min) | 1 | 196 (78%) |
| 2 | 38 (15%) | |
| 3 | 16 (6%) | |
| 4 | 1 (0.4%) | |
| 5 | 1 (0.4%) |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | |
|---|---|---|---|---|---|---|---|---|
| Event | MCI/PVT | Ischemic stroke | DVT/PVT | DVT/PVT | DVT | PE | DVT | PE |
| CPS | B | A | A | A | A | A | B | A |
| BCLC | C | C | C | C | C | A | C | C |
| Etiology | Unknown | Viral | ALD | ALD | Unknown | Unknown | ALD | Unknown |
| Macrovascular Invasion | Yes | Yes | No | Yes | Yes | No | Yes | Yes |
| Extrahepatic Metastases | No | No | Yes | Yes | Yes | No | No | No |
| AFP (IU/mL) | 3.8 | 2.5 | 31.8 | - | 866.0 | - | - | 17,312.0 |
| Known coronary heart disease | No | No | No | No | No | No | No | No |
| Known arterial occlusive disease | No | Yes | No | Yes | No | No | No | No |
| Diabetes mellitus | No | Yes | No | No | Yes | Yes | Yes | No |
| Arterial hypertension | No | Yes | No | No | No | Yes | No | No |
| Framingham risk score points (risk, %) | 11 (7.3%) | 17 (29.4%) | N/A | N/A | N/A | N/A | N/A | N/A |
| Framingham risk class | Low | High | Low | High | High | N/A | High | N/A |
| Time to (first) event (months) | 1.4 | 19.6 | 15.9 | 3.8 | 3.8 | 3.4 | 2.7 | 11.0 |
| Sorafenib Dose at event (mg) | 800 | 200 | 800 | 800 | 400 | 800 | 800 | 400 |
| Event Management | Sorafenib: Discontinued | Sorafenib: Interrupted | Sorafenib: Continued | Sorafenib: Continued | Sorafenib: Continued | |||
| Medical treatment: DAPT (ASA + Clopidogrel) | Medical treatment: none | Medical treatment: anti-coagulation (LMWH) | N/A | N/A | N/A | Medical treatment: anti-coagulation (LMWH) | Medical treatment: anti-coagulation (LMWH) | |
| Intervention: PCI | Intervention: none | Intervention: none | Intervention: none | Intervention: none | ||||
| Death within 14 days (yes/no) | Yes | No | No | No | Yes | No | No | No |
| Patient Characteristics | HR | 95% CI | p-Value (Cox Regression) | |
|---|---|---|---|---|
| Cardiovascular risk (Framingham risk score) | Low/intermediate | 1 | ||
| High | 1.53 | 1.07–2.19 | 0.019 | |
| BCLC stage | A | 1 | ||
| B | 1.04 | 0.48–2.24 | 0.928 | |
| C | 1.21 | 0.63–2.30 | 0.568 | |
| D | 2.34 | 1.16–4.71 | 0.018 | |
| AFP (IU/mL) | ≤400 | 1 | ||
| >400 | 2.04 | 1.44–2.90 | <0.001 |
| Type of Bleeding Event | CPS A (n = 114) | CPS B (n = 95) | CPS C (n = 43) | p–Value |
|---|---|---|---|---|
| Gastrointestinal bleeding | 13 (11.4%) | 13 (13.7%) | 9 (21%) | 0.305 |
| Epistaxis | 5 (4.4%) | 6 (6.3%) | 1 (2.3%) | 0.576 |
| Intracerebral hemorrhage | - | 1 (1%) | - | - |
| Hemorrhoidal hemorrhage | 2 (1.8%) | - | 1 (2.3%) | 0.382 |
| Gingival bleeding | 1 (0.9%) | - | - | - |
| Any bleeding | 20 (17.5%) | 18 (18.9%) | 10 (23.3%) | 0.718 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomej, K.; Scheiner, B.; Park, D.; Bauer, D.; Balcar, L.; Meischl, T.; Mandorfer, M.; Reiberger, T.; Müller, C.; Trauner, M.; et al. Vascular Complications in Patients with Hepatocellular Carcinoma Treated with Sorafenib. Cancers 2020, 12, 2961. https://doi.org/10.3390/cancers12102961
Pomej K, Scheiner B, Park D, Bauer D, Balcar L, Meischl T, Mandorfer M, Reiberger T, Müller C, Trauner M, et al. Vascular Complications in Patients with Hepatocellular Carcinoma Treated with Sorafenib. Cancers. 2020; 12(10):2961. https://doi.org/10.3390/cancers12102961
Chicago/Turabian StylePomej, Katharina, Bernhard Scheiner, Dabin Park, David Bauer, Lorenz Balcar, Tobias Meischl, Mattias Mandorfer, Thomas Reiberger, Christian Müller, Michael Trauner, and et al. 2020. "Vascular Complications in Patients with Hepatocellular Carcinoma Treated with Sorafenib" Cancers 12, no. 10: 2961. https://doi.org/10.3390/cancers12102961
APA StylePomej, K., Scheiner, B., Park, D., Bauer, D., Balcar, L., Meischl, T., Mandorfer, M., Reiberger, T., Müller, C., Trauner, M., & Pinter, M. (2020). Vascular Complications in Patients with Hepatocellular Carcinoma Treated with Sorafenib. Cancers, 12(10), 2961. https://doi.org/10.3390/cancers12102961