Epidemiology of Cutaneous T-Cell Lymphomas: A Systematic Review and Meta-Analysis of 16,953 Patients


 ,
, 

Simple Summary
Abstract
1. Introduction
2. Results
2.1. Study Characteristics
2.2. CTCL Subtypes
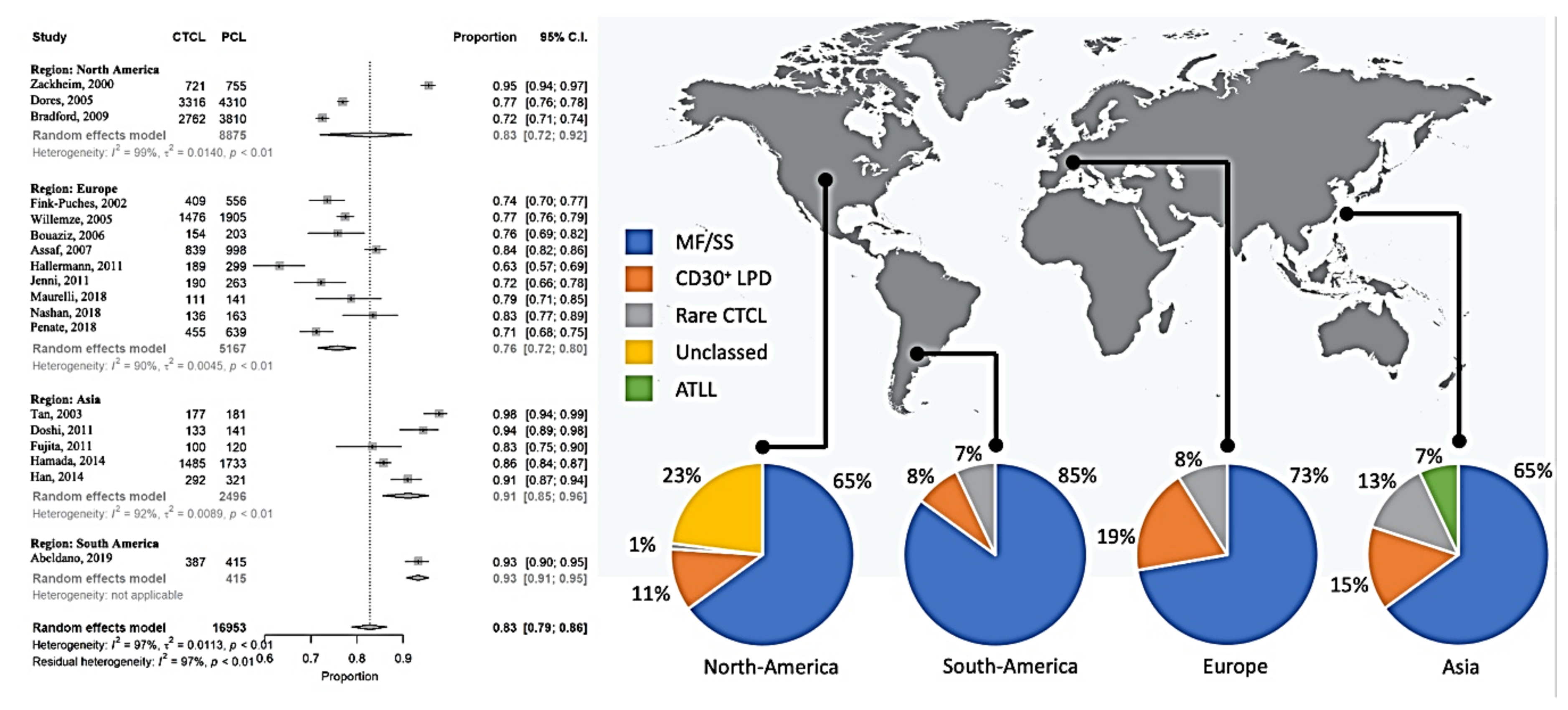
2.2.1. Mycosis Fungoides and Sézary Syndrome
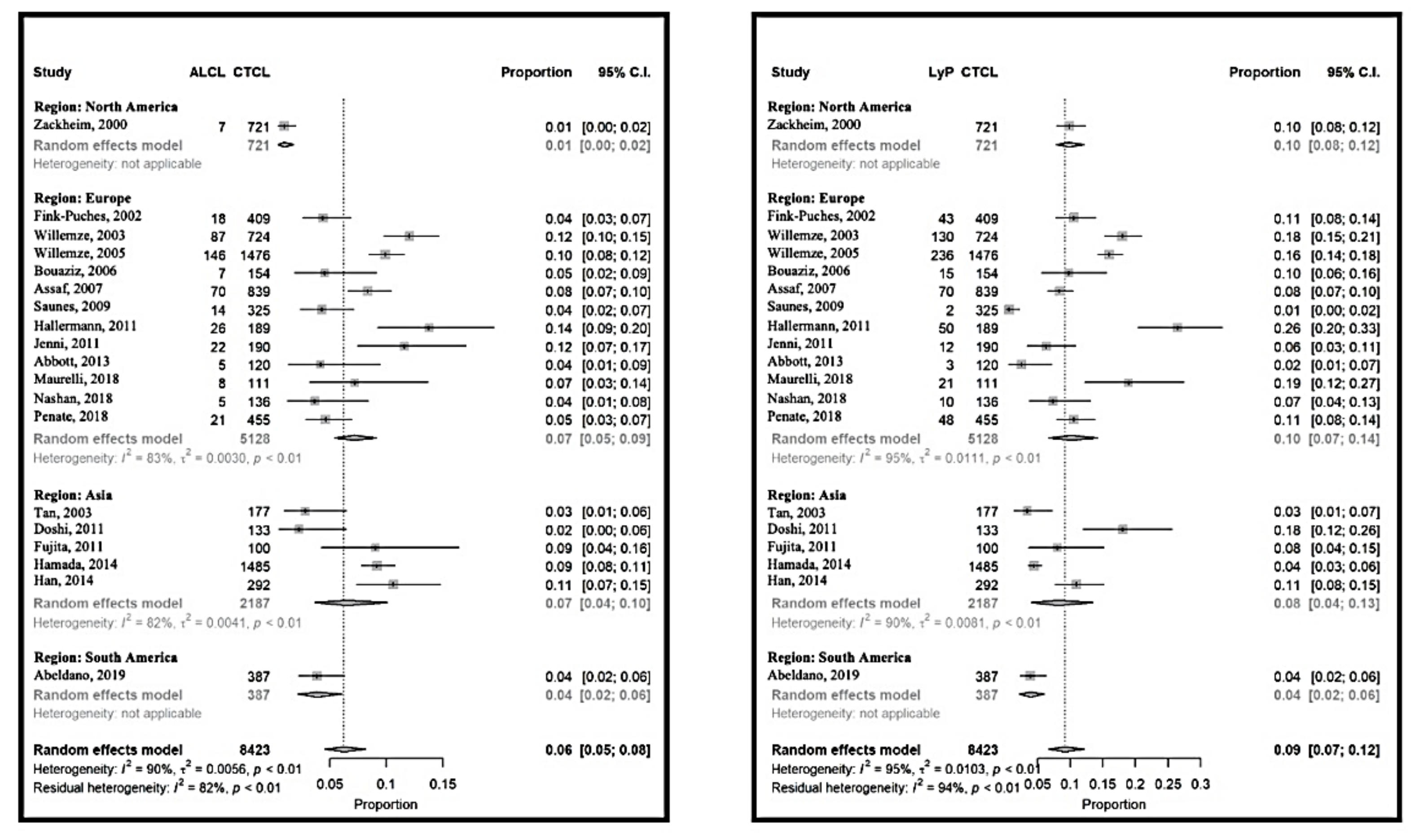
2.2.2. CD30-Positive Lymphoproliferative Disorders
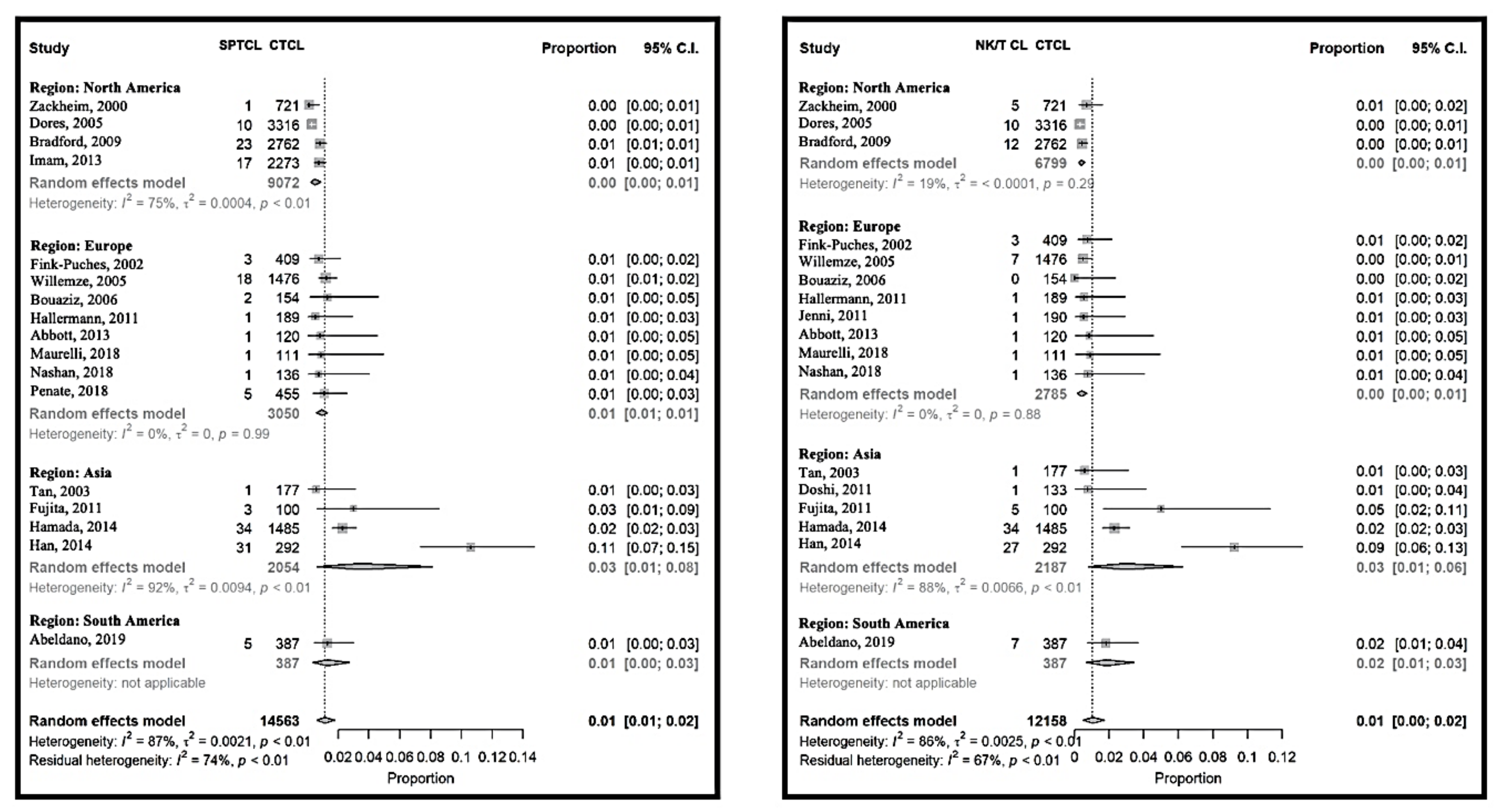
2.2.3. Rare Cutaneous T-Cell Lymphomas
3. Discussion
4. Materials and Methods
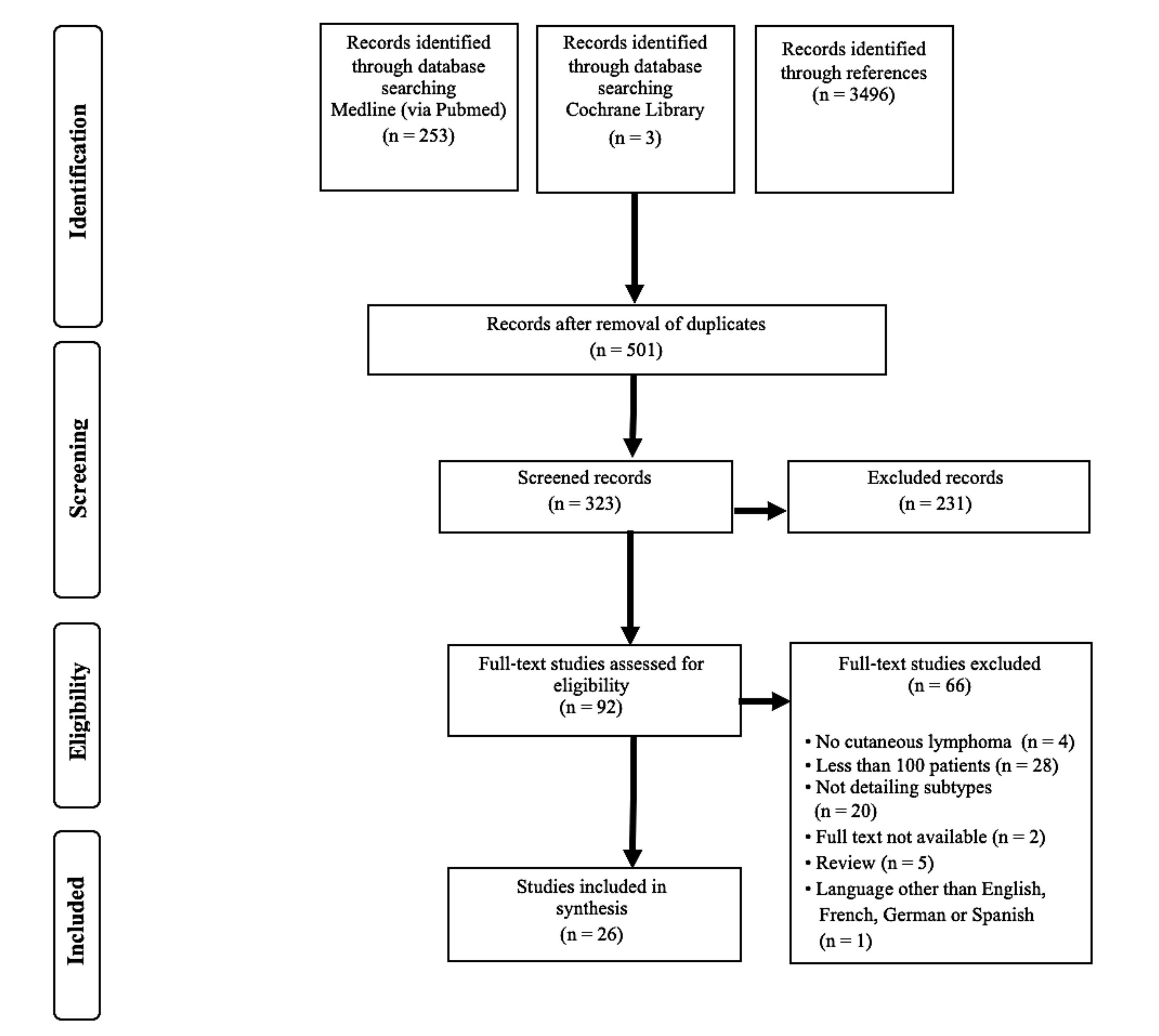
4.1. Literature Search and Selection
4.2. Data Extraction and Quality Appraisal
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Willemze, R.; Cerroni, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019, 133, 1703–1714. [Google Scholar] [CrossRef]
- Gip, L.; Nilsson, E. Clustering of mycosis fungoides in the County of Vasternorrland. Lakartidningen 1977, 74, 1174–1176. [Google Scholar] [PubMed]
- Ghazawi, F.M.; Netchiporouk, E.; Rahme, E.; Tsang, M.; Moreau, L.; Glassman, S.; Provost, N.; Gilbert, M.; Jean, S.E.; Pehr, K.; et al. Comprehensive analysis of cutaneous T-cell lymphoma (CTCL) incidence and mortality in Canada reveals changing trends and geographic clustering for this malignancy. Cancer 2017, 123, 3550–3567. [Google Scholar] [CrossRef] [PubMed]
- Moreau, J.F.; Buchanich, J.M.; Geskin, J.Z.; Akilov, O.E.; Geskin, L.J. Non-random geographic distribution of patients with cutaneous T-cell lymphoma in the Greater Pittsburgh Area. Dermatol. Online J. 2014, 20. [Google Scholar]
- Litvinov, I.V.; Tetzlaff, M.T.; Rahme, E.; Habel, Y.; Risser, D.R.; Gangar, P.; Jennings, M.A.; Pehr, K.; Prieto, V.G.; Sasseville, D.; et al. Identification of geographic clustering and regions spared by cutaneous T-cell lymphoma in Texas using 2 distinct cancer registries. Cancer 2015, 121, 1993–2003. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ni, X.; Covington, K.R.; Yang, B.Y.; Shiu, J.; Zhang, X.; Xi, L.; Meng, Q.; Langridge, T.; Drummond, J.; et al. Genomic profiling of Sezary syndrome identifies alterations of key T cell signaling and differentiation genes. Nat. Genet. 2015, 47, 1426–1434. [Google Scholar] [CrossRef]
- Abeldano, A.; Enz, P.; Maskin, M.; Cervini, A.B.; Torres, N.; Acosta, A.C.; Narbaitz, M.; Vanzulli, S.; Orentrajch, M.; Villareal, M.A.; et al. Primary cutaneous lymphoma in Argentina: A report of a nationwide study of 416 patients. Int. J. Dermatol. 2019, 58, 449–455. [Google Scholar] [CrossRef]
- Assaf, C.; Gellrich, S.; Steinhoff, M.; Nashan, D.; Weisse, F.; Dippel, E.; Coors, E.; Stein, A.; Gollin, P.; Henke, U.; et al. Cutaneous lymphomas in Germany: An analysis of the Central Cutaneous Lymphoma Registry of the German Society of Dermatology (DDG). J. Dtsch. Dermatol. Ges. 2007, 5, 662–668. [Google Scholar] [CrossRef]
- Bouaziz, J.D.; Bastuji-Garin, S.; Poszepczynska-Guigne, E.; Wechsler, J.; Bagot, M. Relative frequency and survival of patients with primary cutaneous lymphomas: Data from a single-centre study of 203 patients. Br. J. Dermatol. 2006, 154, 1206–1207. [Google Scholar] [CrossRef]
- Dores, G.M.; Anderson, W.F.; Devesa, S.S. Cutaneous lymphomas reported to the National Cancer Institute’s surveillance, epidemiology, and end results program: Applying the new WHO-European Organisation for Research and Treatment of Cancer classification system. J. Clin. Oncol. 2005, 23, 7246–7248. [Google Scholar] [CrossRef]
- Fujita, A.; Hamada, T.; Iwatsuki, K. Retrospective analysis of 133 patients with cutaneous lymphomas from a single Japanese medical center between 1995 and 2008. J. Dermatol. 2011, 38, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Jenni, D.; Karpova, M.B.; Seifert, B.; Golling, P.; Cozzio, A.; Kempf, W.; French, L.E.; Dummer, R. Primary cutaneous lymphoma: Two-decade comparison in a population of 263 cases from a Swiss tertiary referral centre. Br. J. Dermatol. 2011, 164, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Senff, N.J.; Hoefnagel, J.J.; Jansen, P.M.; Vermeer, M.H.; van Baarlen, J.; Blokx, W.A.; Canninga-van Dijk, M.R.; Geerts, M.L.; Hebeda, K.M.; Kluin, P.M.; et al. Reclassification of 300 primary cutaneous B-Cell lymphomas according to the new WHO-EORTC classification for cutaneous lymphomas: Comparison with previous classifications and identification of prognostic markers. J. Clin. Oncol. 2007, 25, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.H.; Sim, C.S.; Ong, B.H. Cutaneous lymphomas other than mycosis fungoides in Singapore: A clinicopathological analysis using recent classification systems. Br. J. Dermatol. 2003, 149, 542–553. [Google Scholar] [CrossRef]
- Zinzani, P.L.; Quaglino, P.; Pimpinelli, N.; Berti, E.; Baliva, G.; Rupoli, S.; Martelli, M.; Alaibac, M.; Borroni, G.; Chimenti, S.; et al. Prognostic factors in primary cutaneous B-cell lymphoma: The Italian Study Group for Cutaneous Lymphomas. J. Clin. Oncol. 2006, 24, 1376–1382. [Google Scholar] [CrossRef]
- Maurelli, M.; Tessari, G.; Colato, C.; Schena, D.; Girolomoni, G. Incidence and ten-year follow-up of primary cutaneous lymphomas: A single-centre cohort study. Eur. J. Dermatol. 2018, 28, 44–49. [Google Scholar] [CrossRef]
- Nashan, D.; Friedrich, C.M.; Geissler, E.; Schmitt-Graeff, A.; Klein, F.; Meiss, F. Primary cutaneous lymphoma-a case series of 163 patients. Hautarzt 2018, 69, 1014–1020. [Google Scholar] [CrossRef]
- Penate, Y.; Servitje, O.; Machan, S.; Fernandez-de-Misa, R.; Estrach, M.T.; Acebo, E.; Mitxelena, J.; Ramon, M.D.; Florez, A.; Blanes, M.; et al. The First Year of the AEVD Primary Cutaneous Lymphoma Registry. Actas Dermo-Sifiliogr. 2018, 109, 610–616. [Google Scholar] [CrossRef]
- Smith, B.D.; Smith, G.L.; Cooper, D.L.; Wilson, L.D. The cutaneous B-cell lymphoma prognostic index: A novel prognostic index derived from a population-based registry. J. Clin. Oncol. 2005, 23, 3390–3395. [Google Scholar] [CrossRef]
- Bradford, P.T.; Devesa, S.S.; Anderson, W.F.; Toro, J.R. Cutaneous lymphoma incidence patterns in the United States: A population-based study of 3884 cases. Blood 2009, 113, 5064–5073. [Google Scholar] [CrossRef]
- Imam, M.H.; Shenoy, P.J.; Flowers, C.R.; Phillips, A.; Lechowicz, M.J. Incidence and survival patterns of cutaneous T-cell lymphomas in the United States. Leuk. Lymphoma 2013, 54, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Saunes, M.; Nilsen, T.I.; Johannesen, T.B. Incidence of primary cutaneous T-cell lymphoma in Norway. Br. J. Dermatol. 2009, 160, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.A.; Aldridge, C.; Dojcinov, S.; Piguet, V. Incidence of primary cutaneous T-cell lymphoma in Wales. Br. J. Dermatol. 2013, 169, 1366–1367. [Google Scholar] [CrossRef] [PubMed]
- Hamada, T.; Iwatsuki, K. Cutaneous lymphoma in Japan: A nationwide study of 1733 patients. J. Dermatol. 2014, 41, 3–10. [Google Scholar] [CrossRef]
- Han, J.H.; Ko, Y.H.; Kang, Y.K.; Kim, W.S.; Kim, Y.J.; Kim, I.; Kim, H.J.; Min, S.K.; Park, C.K.; Park, C.S.; et al. Characteristics of Cutaneous Lymphomas in Korea According to the New WHO-EORTC Classification: Report of a Nationwide Study. Korean J. Pathol. 2014, 48, 126–132. [Google Scholar] [CrossRef]
- Grange, F.; Hedelin, G.; Joly, P.; Beylot-Barry, M.; D’Incan, M.; Delaunay, M.; Vaillant, L.; Avril, M.F.; Bosq, J.; Wechsler, J.; et al. Prognostic factors in primary cutaneous lymphomas other than mycosis fungoides and the Sezary syndrome. The French Study Group on Cutaneous Lymphomas. Blood 1999, 93, 3637–3642. [Google Scholar]
- Zackheim, H.S.; Vonderheid, E.C.; Ramsay, D.L.; LeBoit, P.E.; Rothfleisch, J.; Kashani-Sabet, M. Relative frequency of various forms of primary cutaneous lymphomas. J. Am. Acad. Dermatol. 2000, 43, 793–796. [Google Scholar] [CrossRef]
- Fink-Puches, R.; Zenahlik, P.; Back, B.; Smolle, J.; Kerl, H.; Cerroni, L. Primary cutaneous lymphomas: Applicability of current classification schemes (European Organization for Research and Treatment of Cancer, World Health Organization) based on clinicopathologic features observed in a large group of patients. Blood 2002, 99, 800–805. [Google Scholar] [CrossRef]
- Willemze, R. Cutaneous T-cell lymphoma: Epidemiology, etiology, and classification. Leuk. Lymphoma 2003, 44 (Suppl. 3), S49–S54. [Google Scholar] [CrossRef]
- Doshi, B.R.; Khopkar, U.S. Retrospective study of spectrum of cutaneous lymphoma presenting to dermatology. Indian J. Derm. Venereol. Leprol. 2011, 77, 512–515. [Google Scholar] [CrossRef]
- Willemze, R.; Jaffe, E.S.; Burg, G.; Cerroni, L.; Berti, E.; Swerdlow, S.H.; Ralfkiaer, E.; Chimenti, S.; Diaz-Perez, J.L.; Duncan, L.M.; et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005, 105, 3768–3785. [Google Scholar] [CrossRef] [PubMed]
- Hallermann, C.; Niermann, C.; Fischer, R.J.; Schulze, H.J. Survival data for 299 patients with primary cutaneous lymphomas: A monocentre study. Acta Derm. Venereol. 2011, 91, 521–525. [Google Scholar] [CrossRef]
- Willemze, R.; Kerl, H.; Sterry, W.; Berti, E.; Cerroni, L.; Chimenti, S.; Diaz-Perez, J.L.; Geerts, M.L.; Goos, M.; Knobler, R.; et al. EORTC classification for primary cutaneous lymphomas: A proposal from the Cutaneous Lymphoma Study Group of the European Organization for Research and Treatment of Cancer. Blood 1997, 90, 354–371. [Google Scholar]
- Harris, N.L.; Jaffe, E.S.; Diebold, J.; Flandrin, G.; Muller-Hermelink, H.K.; Vardiman, J.; Lister, T.A.; Bloomfield, C.D. The World Health Organization classification of hematological malignancies report of the Clinical Advisory Committee Meeting, Airlie House, Virginia, November 1997. Mod. Pathol. 2000, 13, 193–207. [Google Scholar] [CrossRef]
- Mourad, A.; Gniadecki, R. Overall Survival in Mycosis Fungoides: A Systematic Review and Meta-Analysis. J. Investig. Dermatol. 2020, 140, 495–497.e.5. [Google Scholar] [CrossRef]
- Wilson, L.D.; Hinds, G.A.; Yu, J.B. Age, race, sex, stage, and incidence of cutaneous lymphoma. Clin. Lymphoma Myeloma Leuk. 2012, 12, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Criscione, V.D.; Weinstock, M.A. Incidence of cutaneous T-cell lymphoma in the United States, 1973–2002. Arch. Dermatol. 2007, 143, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Korgavkar, K.; Xiong, M.; Weinstock, M. Changing incidence trends of cutaneous T-cell lymphoma. JAMA Dermatol. 2013, 149, 1295–1299. [Google Scholar] [CrossRef] [PubMed]
- Scarisbrick, J.J.; Quaglino, P.; Prince, H.M.; Papadavid, E.; Hodak, E.; Bagot, M.; Servitje, O.; Berti, E.; Ortiz-Romero, P.; Stadler, R.; et al. The PROCLIPI international registry of early-stage mycosis fungoides identifies substantial diagnostic delay in most patients. Br. J. Dermatol. 2019, 181, 350–357. [Google Scholar] [CrossRef] [PubMed]
- DeStefano, C.B.; Desale, S.; Fernandez, S.J.; Shenoy, A.G. The impact of environmental ultraviolet exposure on the clinical course of mycosis fungoides. J. Am. Acad. Dermatol. 2019, 81, 1074–1077. [Google Scholar] [CrossRef] [PubMed]
- Clough, L.; Bayakly, A.R.; Ward, K.C.; Khan, M.K.; Chen, S.C.; Lechowicz, M.J.; Flowers, C.R.; Allen, P.B.; Switchenko, J.M. Clustering of cutaneous T-cell lymphoma is associated with increased levels of the environmental toxins benzene and trichloroethylene in the state of Georgia. Cancer 2020, 126, 1700–1707. [Google Scholar] [CrossRef] [PubMed]
- Nudelmann, L.M.; Bonamigo, R.R. Primary cutaneous lymphoma in southern Brazil: A 12-year single-center experience. Int. J. Dermatol. 2015, 54, e512–e520. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, A.L.; Oliveira, P.D.; Andrade, A.C.; Santos, T.C.; Oliveira, R.F.; Farre, L.; Araujo, I. Analysis of cutaneous lymphomas in a medical center in Bahia, Brazil. Am. J. Clin. Pathol. 2013, 140, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Sonigo, G.; Battistella, M.; Beylot-Barry, M.; Ingen-Housz-Oro, S.; Franck, N.; Barete, S.; Boulinguez, S.; Dereure, O.; Bonnet, N.; Socie, G.; et al. HAVCR2 mutations are associated with severe hemophagocytic syndrome in subcutaneous panniculitis-like T-cell lymphoma. Blood 2020, 135, 1058–1061. [Google Scholar] [CrossRef] [PubMed]
- Au, W.Y.; Ma, S.Y.; Chim, C.S.; Choy, C.; Loong, F.; Lie, A.K.; Lam, C.C.; Leung, A.Y.; Tse, E.; Yau, C.C.; et al. Clinicopathologic features and treatment outcome of mature T-cell and natural killer-cell lymphomas diagnosed according to the World Health Organization classification scheme: A single center experience of 10 years. Ann. Oncol. 2005, 16, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Naresh, K.N.; Srinivas, V.; Soman, C.S. Distribution of various subtypes of non-Hodgkin’s lymphoma in India: A study of 2773 lymphomas using R.E.A.L. and WHO Classifications. Ann. Oncol. 2000, 11 (Suppl. 1), 63–67. [Google Scholar] [CrossRef] [PubMed]
- Manuchehri, H.M.; Rakhshan, M. Characteristics of primary cutaneous lymphomas in Tehran, Iran (1998–2004). J. Eur. Acad. Dermatol. Venereol. 2006, 20, 758–760. [Google Scholar] [CrossRef]
- Khamaysi, Z.; Ben-Arieh, Y.; Izhak, O.B.; Epelbaum, R.; Dann, E.J.; Bergman, R. The applicability of the new WHO-EORTC classification of primary cutaneous lymphomas to a single referral center. Am. J. Dermatopathol. 2008, 30, 37–44. [Google Scholar] [CrossRef]
- Geller, S.; Lebowitz, E.; Pulitzer, M.P.; Horwitz, S.M.; Moskowitz, A.J.; Dusza, S.; Myskowski, P.L. Outcomes and prognostic factors in African American and black patients with mycosis fungoides/Sezary syndrome: Retrospective analysis of 157 patients from a referral cancer center. J. Am. Acad. Dermatol. 2019. [Google Scholar] [CrossRef]
- Adams, S.V.; Newcomb, P.A.; Shustov, A.R. Racial Patterns of Peripheral T-Cell Lymphoma Incidence and Survival in the United States. J. Clin. Oncol. 2016, 34, 963–971. [Google Scholar] [CrossRef]
- Dobos, G.; Bagot, M.; de Masson, A. Epidemiology of Cutaneous Lymphomas: A Systematic Review of Relative Frequencies. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020148295. (accessed on 27 March 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.; Moga, C.; Harstall, C.; Schopflocher, D. A principal component analysis is conducted for a case series quality appraisal checklist. J. Clin. Epidemiol. 2016, 69, 199–207.e2. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.F.; Tukey, J.W. Transformations related to the angular and the square root. Ann. Math. Stat. 1950, 21, 607–611. [Google Scholar] [CrossRef]
- Miller, J.J. The inverse of the Freeman-Tukey double arcsine transformation. Am. Stat. 1978, 32, 138. [Google Scholar]
- Team, R.C. R: A Language and Environment for Statistical Computing. Available online: http://www.R-project.org/ (accessed on 10 October 2020).
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Scarisbrick, J.J.; Prince, H.M.; Vermeer, M.H.; Quaglino, P.; Horwitz, S.; Porcu, P.; Stadler, R.; Wood, G.S.; Beylot-Barry, M.; Pham-Ledard, A.; et al. Cutaneous Lymphoma International Consortium Study of Outcome in Advanced Stages of Mycosis Fungoides and Sezary Syndrome: Effect of Specific Prognostic Markers on Survival and Development of a Prognostic Model. J. Clin. Oncol. 2015, 33, 3766–3773. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Country | Inclusion of Patients | N | Prospective Data Collection | Multi-Centric | Consecutive | Classification Used | Survival Reported | Reporting Bias | Classifi-Cation Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Grange [26] | 1999 | France | 1986–1997 | 158 A | 1 | 1 | EORTC 1997 | 1 | 1 | ||
| Zackheim [27] | 2000 | USA | 1995–1998 | 755 | 1 | 1 | EORTC 1997 | 1 | 1 | ||
| Fink-Puches [28] | 2002 | Austria | 1960–1999 | 556 | EORTC 1997 + WHO | ||||||
| Tan [14] | 2003 | Singapore | 1990–2001 | 181 | EORTC 1997 + WHO | ||||||
| Willemze [29] | 2003 | Netherlands | 1985–1999 | 724 B | 1 | 1 | EORTC 1997 + WHO | 1 | |||
| Dores [10] | 2005 | USA | 1992–2002 | 4310 C | 1 | 1 | WHO-EORTC 2005 | 1 | 1 | 1 | |
| Smith [19] | 2005 | USA | 1973–2001 | 4551 C | 1 | 1 | WHO | 1 | 1 | ||
| Willemze [31] | 2005 | Austria + Netherlands | 1986–2002 | 1905 | 1 | 1 | WHO-EORTC 2005 | 1 | |||
| Bouaziz [9] | 2006 | France | 1997–2003 | 203 | 1 | 1 | WHO-EORTC 2005 | 1 | |||
| Zinzani [15] | 2006 | Italy | 1980–2003 | 467 B | 1 | WHO-EORTC 2005 | 1 | ||||
| Assaf [8] | 2007 | Germany | 1999–2007 | 998 | 1 | 1 | WHO-EORTC 2005 | 1 | |||
| Senff [13] | 2007 | Netherlands | 1985–2005 | 300 B | 1 | 1 | WHO, EORTC 1997, WHO-EORTC 2005 | 1 | |||
| Bradford [20] | 2009 | USA | 2001–2005 | 3845 C | 1 | 1 | WHO-EORTC 2005 | 1 | 1 | 1 | |
| Saunes [22] | 2009 | Norway | 1980–2003 | 325 C,D | 1 | 1 | not available | 1 | |||
| Doshi [30] | 2011 | India | 2004–2008 | 141 | not available | 1 | 1 | ||||
| Fujita [11] | 2011 | Japan | 1995–2008 | 120 | 1 | WHO | 1 | ||||
| Hallermann [32] | 2011 | Germany | 1980–2005 | 299 | WHO-EORTC 2005 | 1 | |||||
| Jenni [12] | 2011 | Switzerland | 1990–2009 | 263 | WHO-EORTC 2005 | 1 | |||||
| Abbott [23] | 2013 | United Kingdom | 2003–2011 | 120 C,D | 1 | 1 | WHO-EORTC 2005 | ||||
| Imam [21] | 2013 | USA | 2005–2008 | 2273 C,D | 1 | 1 | WHO | 1 | 1 | 1 | |
| Hamada [24] | 2014 | Japan | 2007–2011 | 1485 C | 1 | 1 | WHO-EORTC 2005 | ||||
| Han [25] | 2014 | South-Korea | 2006–2010 | 321 C | 1 | WHO-EORTC 2005 | |||||
| Maurelli [16] | 2018 | Italy | 2005–2015 | 141 | WHO-EORTC 2005 | 1 | |||||
| Nashan [17] | 2018 | Germany | 2005–2011 | 163 | 1 | WHO-EORTC 2005 | |||||
| Penate [18] | 2018 | Spain | nk–2017 | 639 | 1 | 1 | WHO-EORTC 2005 | 1 | |||
| Abeldano [7] | 2019 | Argentina | 2010–2015 | 415 | 1 | 1 | 1 | WHO-EORTC 2005 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobos, G.; Pohrt, A.; Ram-Wolff, C.; Lebbé, C.; Bouaziz, J.-D.; Battistella, M.; Bagot, M.; de Masson, A. Epidemiology of Cutaneous T-Cell Lymphomas: A Systematic Review and Meta-Analysis of 16,953 Patients. Cancers 2020, 12, 2921. https://doi.org/10.3390/cancers12102921
Dobos G, Pohrt A, Ram-Wolff C, Lebbé C, Bouaziz J-D, Battistella M, Bagot M, de Masson A. Epidemiology of Cutaneous T-Cell Lymphomas: A Systematic Review and Meta-Analysis of 16,953 Patients. Cancers. 2020; 12(10):2921. https://doi.org/10.3390/cancers12102921
Chicago/Turabian StyleDobos, Gabor, Anne Pohrt, Caroline Ram-Wolff, Céleste Lebbé, Jean-David Bouaziz, Maxime Battistella, Martine Bagot, and Adèle de Masson. 2020. "Epidemiology of Cutaneous T-Cell Lymphomas: A Systematic Review and Meta-Analysis of 16,953 Patients" Cancers 12, no. 10: 2921. https://doi.org/10.3390/cancers12102921
APA StyleDobos, G., Pohrt, A., Ram-Wolff, C., Lebbé, C., Bouaziz, J.-D., Battistella, M., Bagot, M., & de Masson, A. (2020). Epidemiology of Cutaneous T-Cell Lymphomas: A Systematic Review and Meta-Analysis of 16,953 Patients. Cancers, 12(10), 2921. https://doi.org/10.3390/cancers12102921