Liver Function Changes in Patients with Hepatocellular Carcinoma Treated with Lenvatinib: Predictive Factors of Progression to Child-Pugh Class B, the Formation of Ascites and the Candidates for the Post-Progression Treatment

 ,
,  , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Results
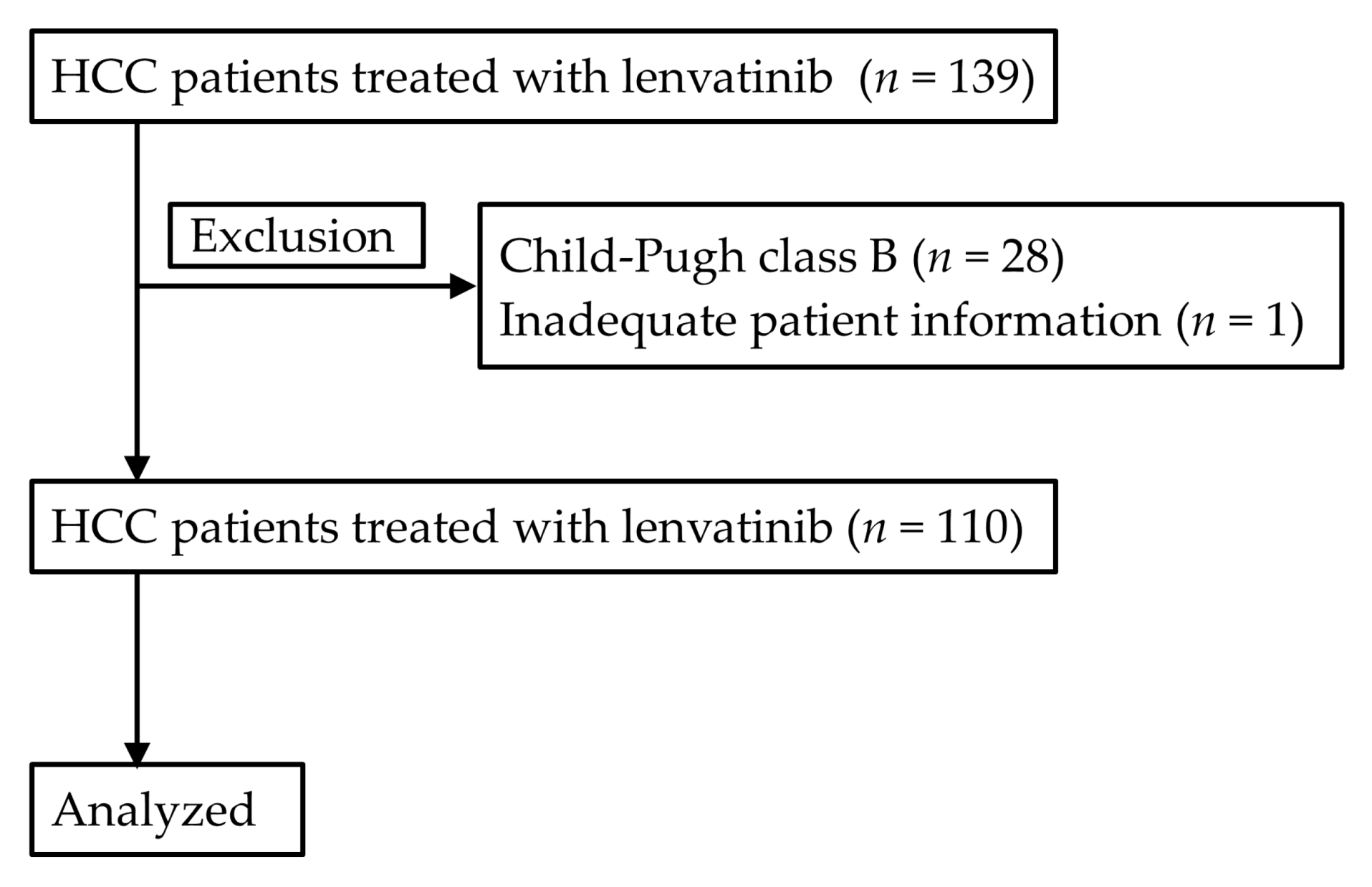
2.1. Patient Characteristics
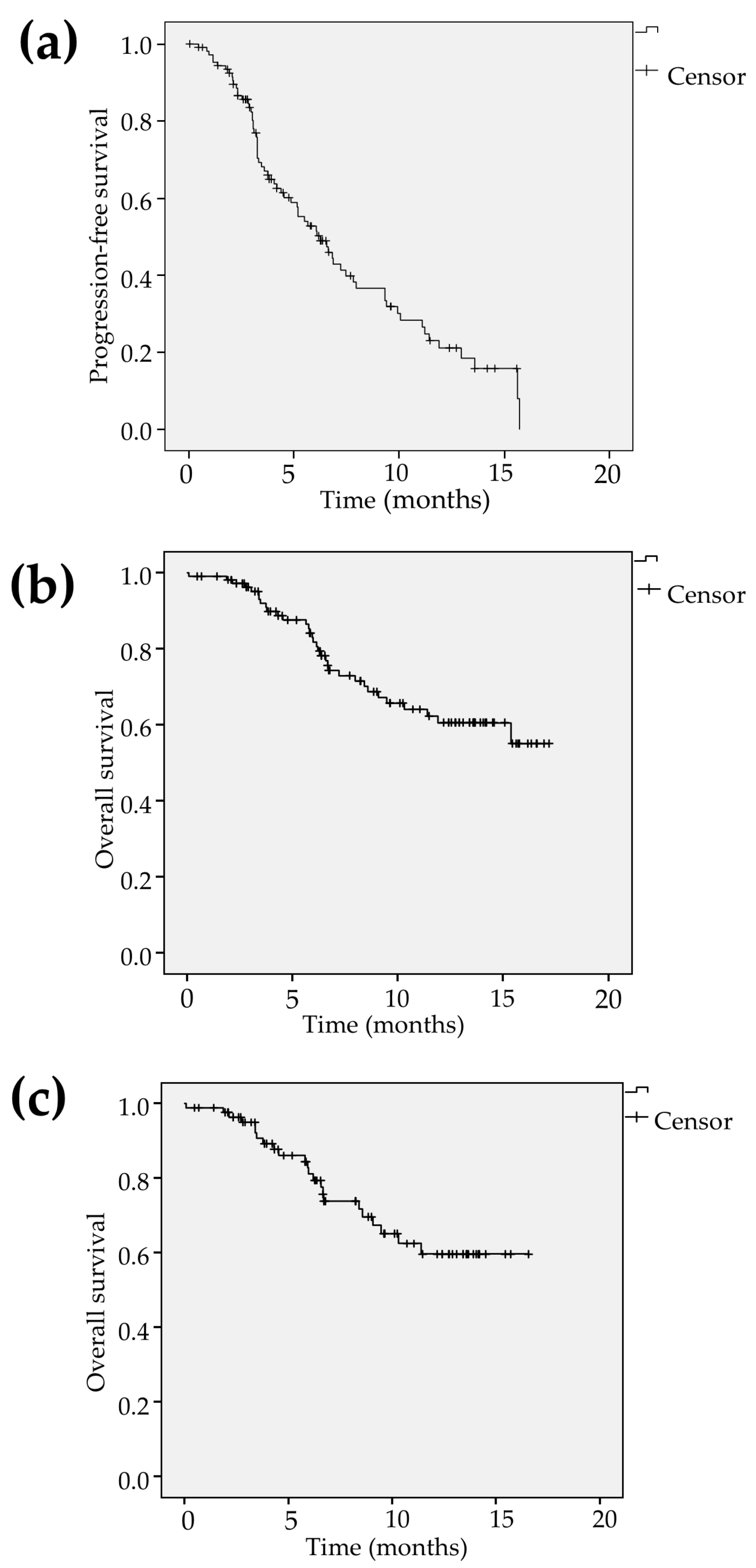
2.2. Tumor Response, PFS and OS
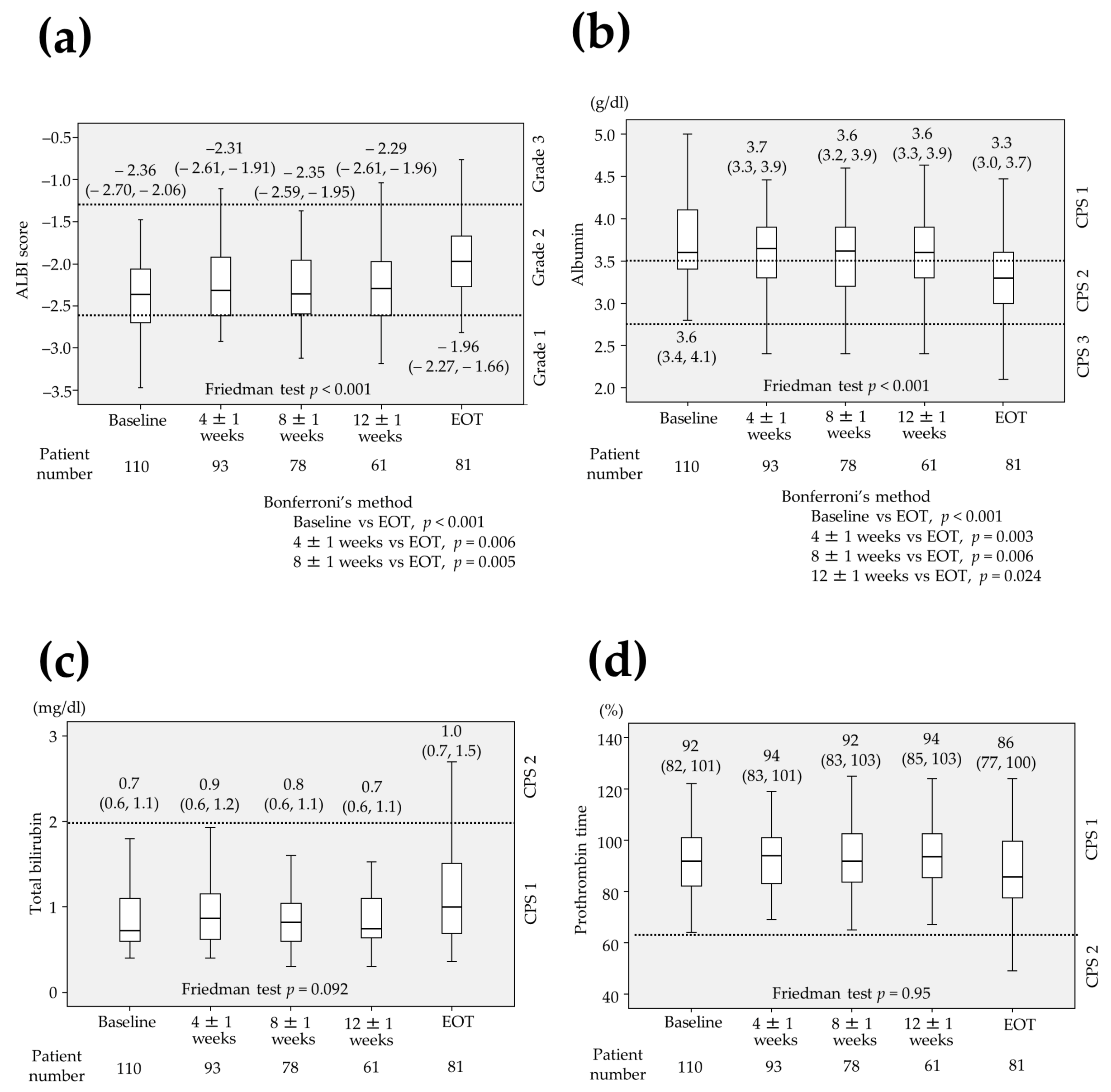
2.3. Changes in Parameters Associated with Liver Function
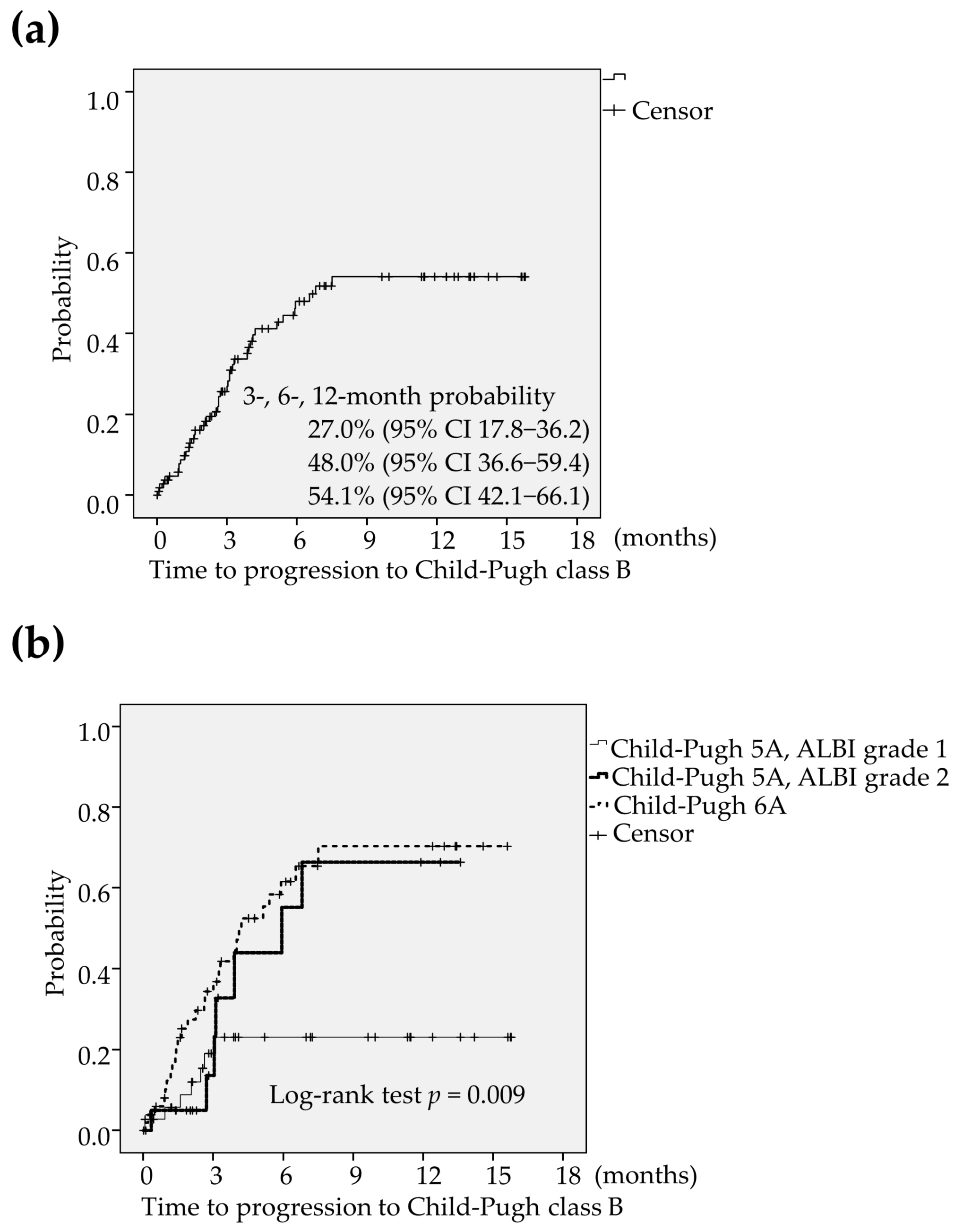
2.4. An Analysis of the Deterioration to CP-B
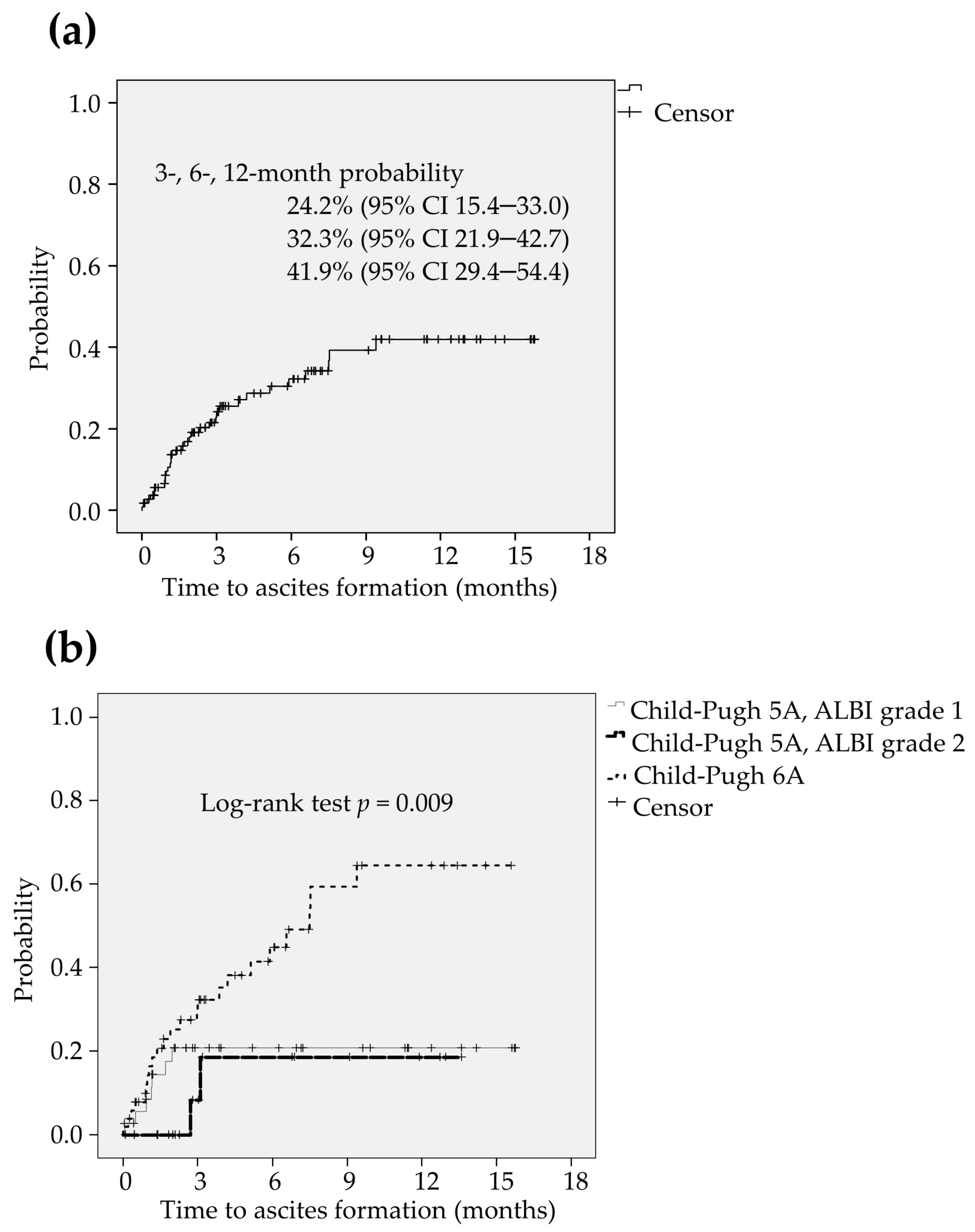
2.5. An Analysis of the Formation of Ascites
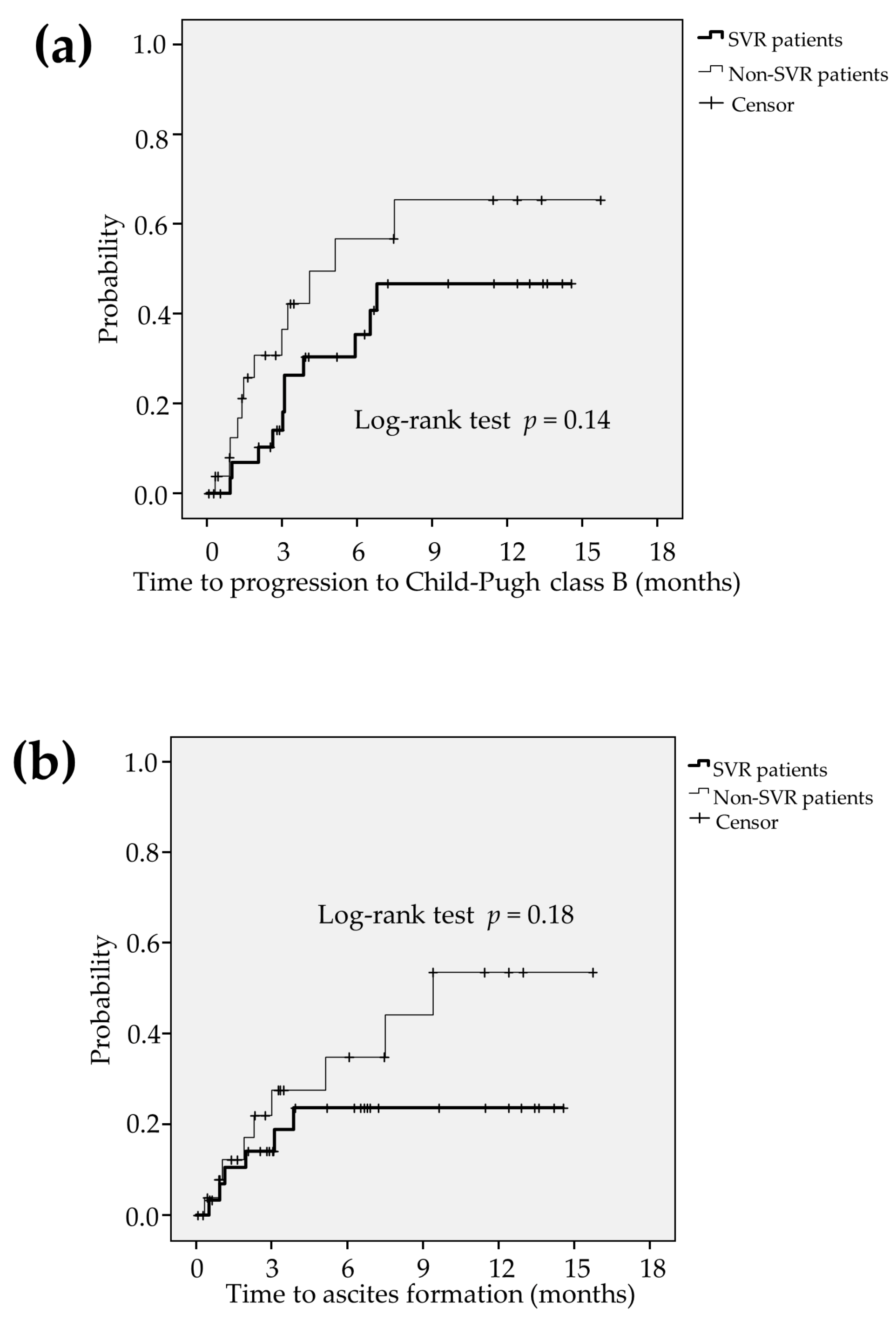
2.6. Comparsion between the Liver Function in SVR Patients and Non-SVR Patients
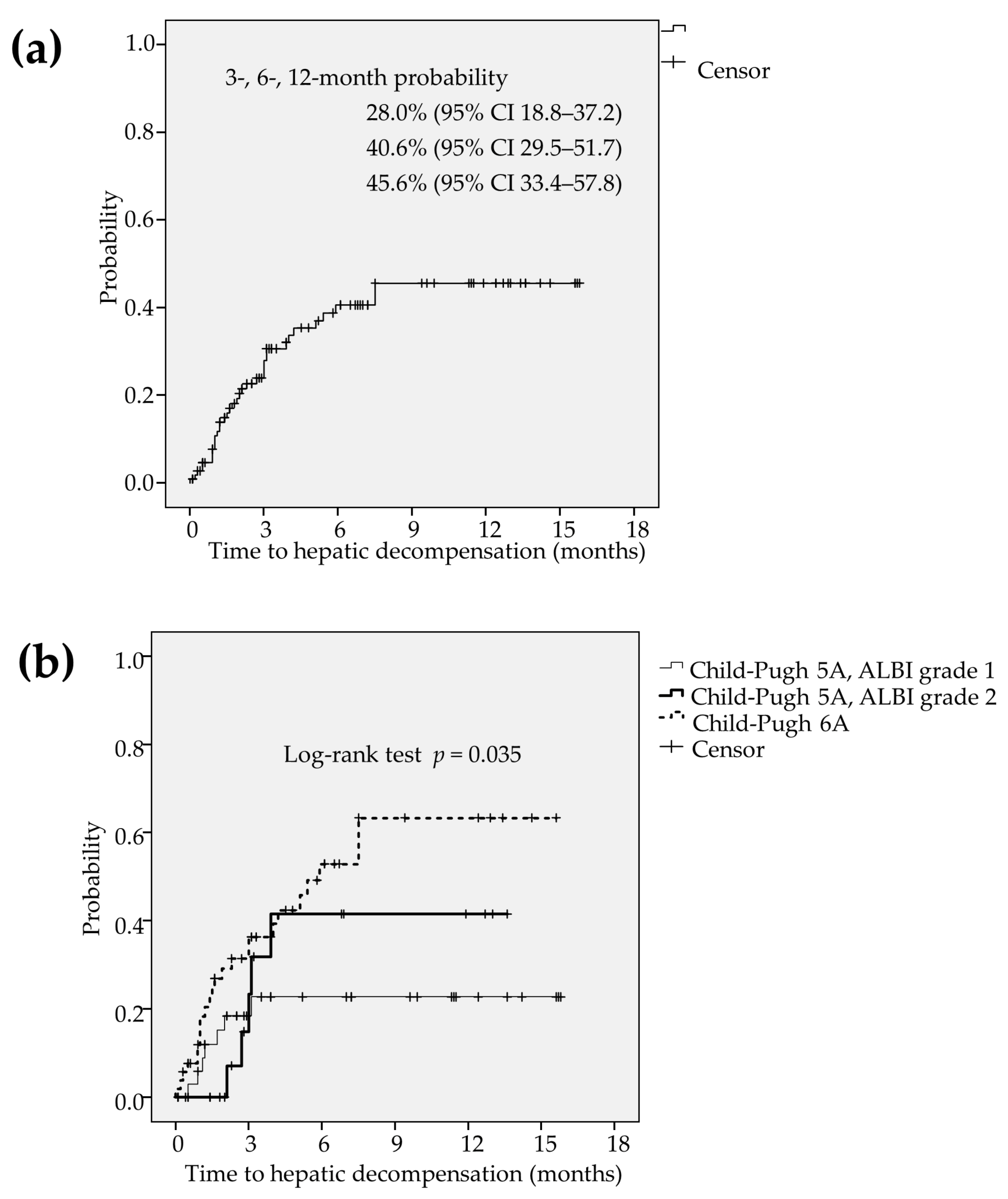
2.7. An Analysis of the Hepatic Decompensation
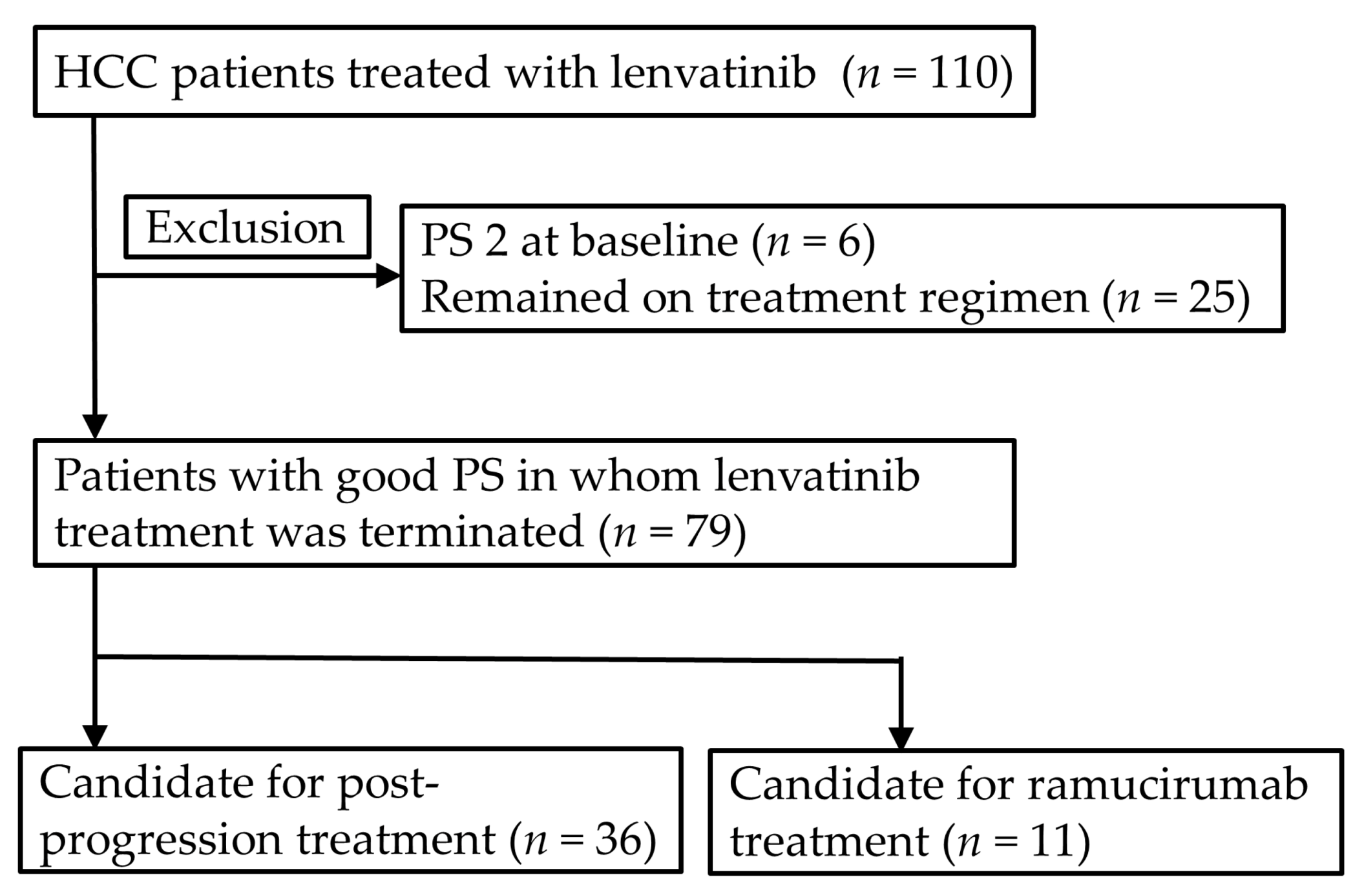
2.8. Candidate for the Post-Progression Treatment and Ramucirumab Treatment
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Lenvatinib Treatment
4.3. Assessment of the Liver Function and the Efficacy of Lenvatinib Treatment
4.4. Eligibility Criteria for Candidate for Post-Progression Treatment
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Lencioni, R.; Kudo, M.; Ye, S.L.; Bronowicki, J.P.; Chen, X.P.; Dagher, L.; Furuse, J.; Geschwind, J.F.; de Guevara, L.L.; Papandreou, C.; et al. GIDEON (Global Investigation of therapeutic DEcisions in hepatocellular carcinoma and Of its treatment with sorafeNib): Second interim analysis. Int. J. Clin. Pract. 2014, 68, 609–617. [Google Scholar] [CrossRef]
- Takeda, H.; Nishikawa, H.; Osaki, Y.; Tsuchiya, K.; Joko, K.; Ogawa, C.; Taniguchi, H.; Orito, E.; Uchida, Y.; Izumi, N. Clinical features associated with radiological response to sorafenib in unresectable hepatocellular carcinoma: A large multicenter study in Japan. Liv. Int. 2015, 35, 1581–1589. [Google Scholar] [CrossRef]
- Hatanaka, T.; Kakizaki, S.; Uehara, D.; Nagashima, T.; Ueno, T.; Namikawa, M.; Saito, S.; Hosonuma, K.; Suzuki, H.; Naganuma, A.; et al. Impact of the prognostic nutritional index on the survival of Japanese patients with hepatocellular carcinoma treated with sorafenib: A multicenter retrospective study. Intern. Med. 2019, 58, 1835–1844. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Kariyama, K.; Takaguchi, K.; Atsukawa, M.; Itobayashi, E.; Tsuji, K.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Clinical features of lenvatinib for unresectable hepatocellular carcinoma in real-world conditions: Multicenter analysis. Cancer Med. 2019, 8, 137–146. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Prognostic factor of lenvatinib for unresectable hepatocellular carcinoma in real-world conditions-Multicenter analysis. Cancer Med. 2019, 8, 3719–3728. [Google Scholar] [CrossRef]
- Ueshima, K.; Nishida, N.; Hagiwara, S.; Aoki, T.; Minami, T.; Chishina, H.; Takita, M.; Minami, Y.; Ida, H.; Takenaka, M.; et al. Impact of baseline ALBI grade on the outcomes of hepatocellular carcinoma patients treated with lenvatinib: A multicenter study. Cancers 2019, 11, 952. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, T.; Kakizaki, S.; Nagashima, T.; Namikawa, M.; Tojima, H.; Shimada, Y.; Takizawa, D.; Naganuma, A.; Arai, H.; Sato, K.; et al. Analyses of objective response rate, progression-free survival, and adverse events in hepatocellular carcinoma patients treated with lenvatinib: A multicenter retrospective study. Hepatol. Res. 2020, 50, 382–395. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased alpha-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; Tajiri, K.; et al. Early relative change in hepatic function with lenvatinib for unresectable hepatocellular carcinoma. Oncology 2019, 97, 334–340. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Fukunishi, S.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; Itobayashi, E.; et al. Post-progression treatment eligibility of unresectable hepatocellular carcinoma patients treated with lenvatinib. Liv. Cancer 2020, 9, 73–83. [Google Scholar] [CrossRef]
- Rockey, D. The cellular pathogenesis of portal hypertension: Stellate cell contractility, endothelin, and nitric oxide. Hepatology 1997, 25, 2–5. [Google Scholar] [CrossRef]
- Gracia-Sancho, J.; Laviña, B.; Rodríguez-Vilarrupla, A.; García-Calderó, H.; Bosch, J.; García-Pagán, J.C. Enhanced vasoconstrictor prostanoid production by sinusoidal endothelial cells increases portal perfusion pressure in cirrhotic rat livers. J. Hepatol. 2007, 47, 220–227. [Google Scholar] [CrossRef]
- Mittal, M.K.; Gupta, T.K.; Lee, F.Y.; Sieber, C.C.; Groszmann, R.J. Nitric oxide modulates hepatic vascular tone in normal rat liver. Am. J. Physiol. 1994, 267, G416–G422. [Google Scholar] [CrossRef]
- Sieber, C.C.; Lopez-Talavera, J.C.; Groszmann, R.J. Role of nitric oxide in the in vitro splanchnic vascular hyporeactivity in ascitic cirrhotic rats. Gastroenterology 1993, 104, 1750–1754. [Google Scholar] [CrossRef]
- Shah, V.; Toruner, M.; Haddad, F.; Cadelina, G.; Papapetropoulos, A.; Choo, K.; Sessa, W.C.; Groszmann, R.J. Impaired endothelial nitric oxide synthase activity associated with enhanced caveolin binding in experimental cirrhosis in the rat. Gastroenterology 1999, 117, 1222–1228. [Google Scholar] [CrossRef]
- Moreau, R. VEGF-induced angiogenesis drives collateral circulation in portal hypertension. J. Hepatol. 2005, 43, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Afdhal, N.; McHutchison, J.; Brown, R.; Jacobson, I.; Manns, M.; Poordad, F.; Weksler, B.; Esteban, R. Thrombocytopenia associated with chronic liver disease. J. Hepatol. 2008, 48, 1000–1007. [Google Scholar] [CrossRef]
- Ogasawara, S.; Chiba, T.; Ooka, Y.; Suzuki, E.; Maeda, T.; Yokoyama, M.; Wakamatsu, T.; Inoue, M.; Saito, T.; Kobayashi, K.; et al. Characteristics of patients with sorafenib-treated advanced hepatocellular carcinoma eligible for second-line treatment. Invest. New Drugs. 2018, 36, 332–339. [Google Scholar] [CrossRef]
- Uchikawa, S.; Kawaoka, T.; Aikata, H.; Kodama, K.; Nishida, Y.; Inagaki, Y.; Hatooka, M.; Morio, K.; Nakahara, T.; Murakami, E.; et al. Clinical outcomes of sorafenib treatment failure for advanced hepatocellular carcinoma and candidates for regorafenib treatment in real-world practice. Hepatol. Res. 2018, 48, 814–820. [Google Scholar] [CrossRef]
- Yukimoto, A.; Hirooka, M.; Hiraoka, A.; Michitaka, K.; Ochi, H.; Joko, K.; Imai, Y.; Watanabe, T.; Koizumi, Y.; Yoshida, O.; et al. Using ALBI score at the start of sorafenib treatment to predict regorafenib treatment candidates in patients with hepatocellular carcinoma. Jpn. J. Clin. Oncol. 2019, 49, 42–47. [Google Scholar] [CrossRef]
- Takada, H.; Kurosaki, M.; Tsuchiya, K.; Komiyama, Y.; Itakura, J.; Takahashi, Y.; Nakanishi, H.; Yasui, Y.; Tamaki, N.; Maeyashiki, C.; et al. Baseline and early predictors of good patient candidates for second-line after sorafenib treatment in unresectable hepatocellular carcinoma. Cancers 2019, 11, 1256. [Google Scholar] [CrossRef]
- Kuzuya, T.; Ishigami, M.; Ito, T.; Ishizu, Y.; Honda, T.; Ishikawa, T.; Hirooka, Y.; Fujishiro, M. Clinical characteristics and outcomes of candidates for second-line therapy, including regorafenib and ramucirumab, for advanced hepatocellular carcinoma after sorafenib treatment. Hepatol. Res. 2019, 49, 1054–1065. [Google Scholar] [CrossRef]
- Reiss, K.A.; Yu, S.; Mamtani, R.; Mehta, R.; D’Addeo, K.; Wileyto, E.P.; Taddei, T.H.; Kaplan, D.E. Starting dose of sorafenib for the treatment of hepatocellular carcinoma: A retrospective, multi-institutional study. J. Clin. Oncol. 2017, 35, 3575–3581. [Google Scholar] [CrossRef]
- Eso, Y.; Nakano, S.; Mishima, M.; Arasawa, S.; Iguchi, E.; Nakamura, F.; Takeda, H.; Takai, A.; Takahashi, K.; Taura, K.; et al. Dose intensity/body surface area ratio is a novel marker useful for predicting response to lenvatinib against hepatocellular carcinoma. Cancers 2019, 12, 49. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, R.; Fukushima, M.; Haraguchi, M.; Miuma, S.; Miyaaki, H.; Hidaka, M.; Eguchi, S.; Matsuo, S.; Tajima, K.; Matsuzaki, T.; et al. Response to lenvatinib is associated with optimal relative dose intensity in hepatocellular carcinoma: Experience in clinical settings. Cancers 2019, 11, 1769. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Petta, S.; Barbara, M.; Attardo, S.; Bucci, L.; Farinati, F.; Giannini, E.G.; Negrini, G.; Ciccarese, F.; Rapaccini, G.L.; et al. Hepatic decompensation is the major driver of death in HCV-infected cirrhotic patients with successfully treated early hepatocellular carcinoma. J. Hepatol. 2017, 67, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Rimola, J.; Torres, F.; Darnell, A.; Rodriguez-Lope, C.; Forner, A.; Llarch, N.; Rios, J.; Ayuso, C.; Bruix, J. Postprogression survival of patients with advanced hepatocellular carcinoma: Rationale for second-line trial design. Hepatology 2013, 58, 2023–2031. [Google Scholar] [CrossRef]
- Kudo, M. Ramucirumab as second-line systemic therapy in hepatocellular carcinoma. Liv. Cancer 2018, 7, 305–311. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | 73 (66.7–80.0) |
| Males, n (%) | 88 (80.0) |
| PS, 0 / 1 / 2, n (%) | 77 (70.0) / 27 (24.5) / 6 (5.5) |
| Body weight (kg) | 59.6 (53.0–66.2) |
| BMI (kg/m2) | 22.8 (21.1–25.3) |
| Liver diseases, | |
| HBV / HCV / Alcohol / Others, n (%) | 12 (10.9) / 58 (52.7) / 19 (17.3) / 21 (19.1) |
| Antiviral therapy for HBV, n (%) | 8 (66.7) |
| HCV eradication, n (%) | 32 (55.2) |
| Child-Pugh score 5 / 6, n (%) | 58 (52.7) / 52 (47.3) |
| ALBI score | −2.36 (−2.70 to −2.06) |
| ALBI grade 1 / 2, n (%) | 38 (34.5) / 72 (65.5) |
| Albumin (g/dL) | 3.6 (3.4–4.1) |
| Total bilirubin (mg/dL) | 0.73 (0.60–1.10) |
| Prothrombin time (%) | 92 (82–101) |
| Platelet count (×104/μL) | 13.6 (9.9–19.0) |
| Treatment-naïve, n (%) | 20 (18.2) |
| History of hepatic resection, n (%) | 35 (31.8) |
| History of RFA, n (%) | 43 (39.1) |
| History of TACE, n (%) | 93 (84.5) |
| The number of previous TACE treatments | 2 (1–6) |
| History of molecular targeted therapies, n (%) | 26 (23.6) |
| Esophageal varices, None / F1 / F2, n (%) * | 82 (76.6) / 16 (15.0) / 9 (8.4) |
| History of treatment for esophageal varices, n (%) | 9 (8.2) |
| Initial dose, 12 mg / 8 mg / 4 mg, n (%) | 22 (20.0) / 58 (52.7) / 30 (27.3) |
| Full dose / Reduced dose, n (%) | 58 (52.7) / 52 (47.3) |
| BCLC stage, n (%) | |
| Early / Intermediate / Advanced | 3 (2.7) / 33 (30.0) / 74 (67.3) |
| Extrahepatic spread, n (%) | 36 (32.7) |
| Macroscopic vascular invasion, n (%) | 22 (20.0) |
| Bile duct invasion, n (%) | 10 (9.1) |
| PVTT, n (%) | 15 (13.6) |
| AFP ≧ 200 ng/mL, n (%) | 38 (34.5) |
| DCP ≧ 200 mAU/mL, n (%) | 57 (51.8) |
| CR | 1 (1.1) |
| PR | 26 (28.9) |
| SD | 44 (48.9) |
| PD | 19 (21.1) |
| Objective response rate (%) | 30.0 |
| Disease control rate (%) | 83.3 |
| Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|
| Variable | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| All patients | |||||||
| Sex | Male | 1 | 0.24 | 1 | 0.26 | 1 | 0.17 |
| Female | 1.62 (0.72–3.62) | 1.60 (0.71–3.60) | 1.77 (0.78–4.01) | ||||
| Age (years) | ≧ 73 | 1 | 0.060 | 1 | 0.057 | 1 | 0.071 |
| < 73 | 1.45 (0.25–1.03) | 0.50 (0.25–1.02) | 0.52 (0.26–1.06) | ||||
| ALBI grade | Grade 1 | 1 | 0.059 | ||||
| Grade 2 | 0.45 (0.19–1.03) | ||||||
| Child-Pugh score | 5 | 1 | 0.46 | ||||
| 6 | 1.30 (0.65–2.59) | ||||||
| BCLC stage | Intermediate, Early | 1 | 0.045 | ||||
| Advanced | 2.50 (1.02–6.10) | ||||||
| Patients treated with lenvatinib as first-line treatment | |||||||
| Age (years) | ≧ 73 | 1 | 0.110 | 1 | 0.11 | 1 | 0.096 |
| < 73 | 0.48 (0.20–1.17) | 0.48 (0.20–1.17) | 0.47 (0.19–1.14) | ||||
| ALBI grade | Grade 1 | 1 | 0.36 | ||||
| Grade 2 | 1.52 (0.62–3.69) | ||||||
| Child-Pugh score | 5 | 1 | 0.88 | ||||
| 6 | 1.07 (0.46–2.48) | ||||||
| BCLC stage | Intermediate, Early | 1 | 0.087 | ||||
| Advanced | 2.39 (0.88–6.48) | ||||||
| Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|
| Variable | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Sex | Male | 1 | 0.021 | 1 | 0.024 | 1 | 0.016 |
| Female | 2.27 (1.12–4.54) | 2.24 (1.11–4.53) | 2.33 (1.17–4.65) | ||||
| Platelet count | ≧12 × 104/μL | 1 | 0.24 | ||||
| <12 × 104/μL | 1.45 (0.78–2.70) | ||||||
| ALBI grade | Grade 1 | 1 | 0.030 | 1 | 0.033 | ||
| Grade 2 | 2.38 (1.09–5.26) | 2.35 (1.07–5.15) | |||||
| Child-Pugh score | 5 | 1 | 0.037 | ||||
| 6 | 2.03 (1.04–3.95) | ||||||
| BCLC stage | Intermediate, Early | 1 | 0.048 | ||||
| Advanced | 2.08 (1.01–4.17) | ||||||
| PVTT | Presence | 1 | 0.29 | ||||
| Absence | 0.64 (0.28–1.46) | ||||||
| Bile duct invasion | Presence | 1 | 0.44 | ||||
| Absence | 1.76 (0.42–7.32) | ||||||
| Previous TACE | ≧2 | 1 | 0.39 | ||||
| <1 | 1.32 (0.70–2.48) | ||||||
| Initial dose | Full dose | 1 | 0.53 | ||||
| Reduced dose | 1.22 (0.66–2.24) | ||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Sex | Male | 1 | 0.33 | 1 | 0.75 | 1 | 0.093 | 1 | 0.17 |
| Female | 1.52 (0.66–3.45) | 1.15 (0.49–2.70) | 2.02 (0.89–4.58) | 1.51 (0.67–3.45) | |||||
| Platelet count | ≧ 12 × 104/μL | 1 | 0.013 | 1 | 0.010 | ||||
| < 12 × 104/μL | 2.56 (1.22–5.26) | 2.63 (1.25–5.26) | |||||||
| ALBI grade | Grade 1 | 1 | 0.59 | ||||||
| Grade 2 | 1.25 (0.55–2.86) | ||||||||
| Child-Pugh score | 5 | 1 | 0.041 | ||||||
| 6 | 2.17 (1.03–4.55) | ||||||||
| BCLC stage | Intermediate, Early | 1 | 0.90 | ||||||
| Advanced | 0.96 (0.46–1.99) | ||||||||
| PVTT | Presence | 1 | 0.28 | ||||||
| Absence | 0.60 (0.24–1.52) | ||||||||
| Previous TACE | ≧2 | 1 | 0.57 | ||||||
| <1 | 0.81 (0.39–169) | ||||||||
| Initial dose | Full dose | 1 | 0.92 | ||||||
| Reduced dose | 1.04 (0.51–2.10) | ||||||||
| Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|
| Variable | Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Sex | Male | 1.70 (0.54–5.32) | 0.36 | 1.83 (0.57–5.88) | 0.31 | 2.04 (0.65–6.38) | 0.22 |
| Female | 1 | 1 | 1 | ||||
| ALBI grade | Grade 1 | 3.24 (1.20–8.76) | 0.020 | ||||
| Grade 2 | 1 | ||||||
| Child-Pugh score | 5 | 3.80 (1.45–9.95) | 0.007 | ||||
| 6 | 1 | ||||||
| BCLC stage | Intermediate, Early | 0.95 (0.35–2.62) | 0.93 | ||||
| Advanced | 1 | ||||||
| PVTT | Presence | 0.92 (0.24–3.49) | 0.91 | ||||
| Absence | 1 | ||||||
| Bile duct invasion | Presence | 1.41 (0.33–6.12) | 0.64 | ||||
| Absence | 1 | ||||||
| Initial dose | Full dose | 2.92 (1.15–7.44) | 0.024 | ||||
| Reduced dose | 1 | ||||||
| Full Dose Group (n = 35) | Reduced Dose Group (n = 44) | |
|---|---|---|
| ALBI score | −2.41 (−2.79 to −1.97) | −2.34 (−2.66 to −2.07) |
| ALBI grade 1 | 14 (40.0) | 12 (27.3) |
| Child-Pugh score 5 | 17 (48.6) | 24 (54.5) |
| PS 0 | 29 (82.9) | 29 (65.9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatanaka, T.; Kakizaki, S.; Nagashima, T.; Namikawa, M.; Ueno, T.; Tojima, H.; Takizawa, D.; Naganuma, A.; Arai, H.; Sato, K.; et al. Liver Function Changes in Patients with Hepatocellular Carcinoma Treated with Lenvatinib: Predictive Factors of Progression to Child-Pugh Class B, the Formation of Ascites and the Candidates for the Post-Progression Treatment. Cancers 2020, 12, 2906. https://doi.org/10.3390/cancers12102906
Hatanaka T, Kakizaki S, Nagashima T, Namikawa M, Ueno T, Tojima H, Takizawa D, Naganuma A, Arai H, Sato K, et al. Liver Function Changes in Patients with Hepatocellular Carcinoma Treated with Lenvatinib: Predictive Factors of Progression to Child-Pugh Class B, the Formation of Ascites and the Candidates for the Post-Progression Treatment. Cancers. 2020; 12(10):2906. https://doi.org/10.3390/cancers12102906
Chicago/Turabian StyleHatanaka, Takeshi, Satoru Kakizaki, Tamon Nagashima, Masashi Namikawa, Takashi Ueno, Hiroki Tojima, Daichi Takizawa, Atsushi Naganuma, Hirotaka Arai, Ken Sato, and et al. 2020. "Liver Function Changes in Patients with Hepatocellular Carcinoma Treated with Lenvatinib: Predictive Factors of Progression to Child-Pugh Class B, the Formation of Ascites and the Candidates for the Post-Progression Treatment" Cancers 12, no. 10: 2906. https://doi.org/10.3390/cancers12102906
APA StyleHatanaka, T., Kakizaki, S., Nagashima, T., Namikawa, M., Ueno, T., Tojima, H., Takizawa, D., Naganuma, A., Arai, H., Sato, K., Harimoto, N., Shirabe, K., & Uraoka, T. (2020). Liver Function Changes in Patients with Hepatocellular Carcinoma Treated with Lenvatinib: Predictive Factors of Progression to Child-Pugh Class B, the Formation of Ascites and the Candidates for the Post-Progression Treatment. Cancers, 12(10), 2906. https://doi.org/10.3390/cancers12102906