The Value of Microvascular Imaging for Triaging Indeterminate Cervical Lymph Nodes in Patients with Papillary Thyroid Carcinoma


Simple Summary
Abstract
1. Introduction
2. Results
2.1. Demographic Data
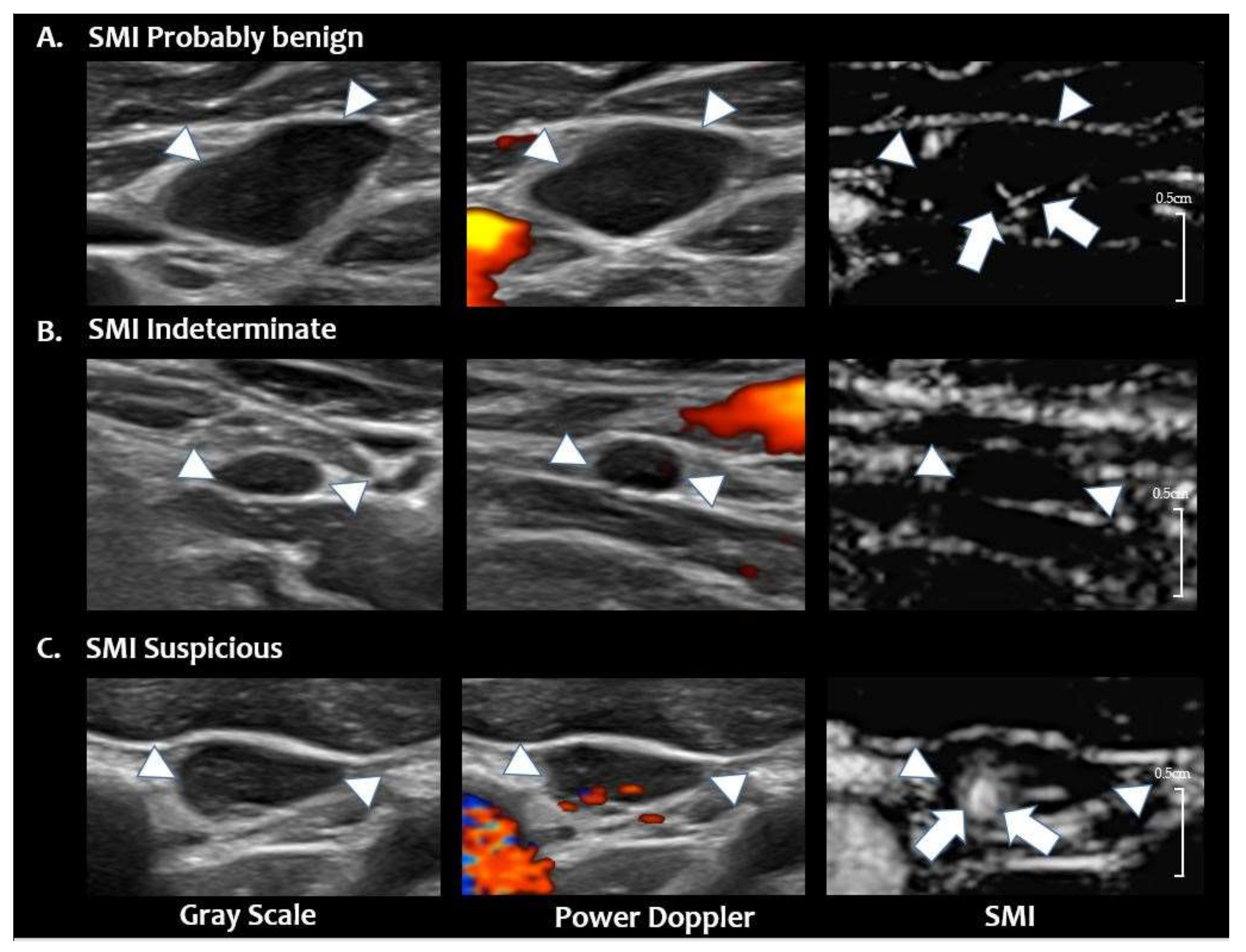
2.2. Analysis of Vascular Patterns on SMI
2.3. Diagnostic Performance of SMI
2.4. Inter-Observer Agreement
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. US Examination
4.3. Imaging Analysis
4.4. Reference Standard
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kim, E.; Park, J.S.; Son, K.R.; Kim, J.H.; Jeon, S.J.; Na, D.G. Preoperative diagnosis of cervical metastatic lymph nodes in papillary thyroid carcinoma: Comparison of ultrasound, computed tomography, and combined ultrasound with computed tomography. Thyroid 2008, 18, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Stulak, J.M.; Grant, C.S.; Farley, D.R.; Thompson, G.B.; Van Heerden, J.A.; Hay, I.D.; Reading, C.C.; Charboneau, J.W. Value of preoperative ultrasonography in the surgical management of initial and reoperative papillary thyroid cancer. Arch. Surg. 2006, 141, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Al-Saif, O.; Farrar, W.B.; Bloomston, M.; Porter, K.; Ringel, M.D.; Kloos, R.T. Long-term efficacy of lymph node reoperation for persistent papillary thyroid cancer. J. Clin. Endocrinol. Metab. 2010, 95, 2187–2194. [Google Scholar] [CrossRef] [PubMed]
- Beasley, N.J.P.; Lee, J.; Eski, S.; Walfish, P.; Witterick, I.; Freeman, J.L. Impact of nodal metastases on prognosis in patients with well-differentiated thyroid cancer. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 825–828. [Google Scholar] [CrossRef]
- Eloy, C.; Santos, J.; Soares, P.; Sobrinho-Simões, M. Intratumoural lymph vessel density is related to presence of lymph node metastases and separates encapsulated from infiltrative papillary thyroid carcinoma. Virchows Arch. 2011, 459, 595–605. [Google Scholar] [CrossRef]
- Hall, F.T.; Freeman, J.L.; Asa, S.L.; Jackson, D.G.; Beasley, N.J. Intratumoral Lymphatics and Lymph Node Metastases in Papillary Thyroid Carcinoma. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 716–719. [Google Scholar] [CrossRef]
- Pereira, F.; Pereira, S.S.; Mesquita, M.; Morais, T.; Costa, M.M.; Quelhas, P.; Lopes, C.; Monteiro, M.P.; Leite, V. Lymph node metastases in papillary and medullary thyroid carcinoma are independent of intratumoral lymphatic vessel density. Eur. Thyroid J. 2017, 6, 57–64. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Lamartina, L.; Grani, G.; Biffoni, M.; Giacomelli, L.; Costante, G.; Lupo, S.; Maranghi, M.; Plasmati, K.; Sponziello, M.; Trulli, F.; et al. Risk stratification of neck lesions detected sonographically during the follow-up of differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 2016, 101, 3036–3044. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedus, L.; Paschke, R.; Valcavi, R.; Vitti, P. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the diagnosis and management of thyroid nodules—2016 Update. Endocr. Pract. 2016, 22, 622–639. [Google Scholar] [CrossRef]
- Leenhardt, L.; Erdogan, M.F.; Hegedus, L.; Mandel, S.J.; Paschke, R.; Rago, T.; Russ, G. 2013 European thyroid association guidelines for cervical ultrasound scan and ultrasound-guided techniques in the postoperative management of patients with thyroid cancer. Eur. Thyroid J. 2013, 2, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR Thyroid Imaging, reporting and data system (TI-RADS): White paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Baek, J.H.; Chung, J.; Ha, E.J.; Kim, J.H.; Lee, Y.H.; Lim, H.K.; Moon, W.J.; Na, D.G.; Park, J.S.; et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: Revised Korean Society of thyroid radiology consensus statement and recommendations. Korean J. Radiol. 2016, 17, 370–395. [Google Scholar] [CrossRef] [PubMed]
- Yoo, R.E.; Kim, J.H.; Bae, J.M.; Hwang, I.; Kang, K.M.; Yun, T.J.; Choi, S.H.; Sohn, C.H.; Rhim, J.H.; Park, S.W. Ultrasonographic indeterminate lymph nodes in preoperative thyroid cancer patients: Malignancy risk and ultrasonographic findings predictive of malignancy. Korean J. Radiol. 2020, 21, 598–604. [Google Scholar] [CrossRef]
- Yoo, R.E.; Kim, J.H.; Hwang, I.; Kang, K.M.; Yun, T.J.; Choi, S.H.; Sohn, C.H.; Park, S.W. Added Value of computed tomography to ultrasonography for assessing LN metastasis in preoperative patients with thyroid cancer: Node-By-Node correlation. Cancers 2020, 12, 1190. [Google Scholar] [CrossRef]
- Demene, C.; Deffieux, T.; Pernot, M.; Osmanski, B.F.; Biran, V.; Gennisson, J.L.; Sieu, L.A.; Bergel, A.; Franqui, S.; Correas, J.M.; et al. Spatiotemporal Clutter filtering of ultrafast ultrasound data highly increases doppler and fultrasound sensitivity. IEEE Trans. Med Imaging 2015, 34, 2271–2285. [Google Scholar] [CrossRef]
- Chae, E.Y.; Yoon, G.Y.; Cha, J.H.; Shin, H.J.; Choi, W.J.; Kim, H.H. Added Value of the vascular index on superb microvascular imaging for the evaluation of breast masses: Comparison with grayscale ultrasound. J. Ultrasound Med. 2020. [Google Scholar] [CrossRef]
- Leong, J.Y.; Wessner, C.E.; Kramer, M.R.; Forsberg, F.; Halpern, E.J.; Lyshchik, A.; Torkzaban, M.; Morris, A.; Byrne, K.; VanMeter, M.; et al. Superb microvascular imaging improves detection of vascularity in indeterminate renal masses. J. Ultrasound Med. 2020. [Google Scholar] [CrossRef]
- Park, A.Y.; Seo, B.K.; Woo, O.H.; Jung, K.S.; Cho, K.R.; Park, E.K.; Cha, S.H.; Cha, J. The utility of ultrasound superb microvascular imaging for evaluation of breast tumour vascularity: Comparison with colour and power Doppler imaging regarding diagnostic performance. Clin. Radiol. 2018, 73, 304–311. [Google Scholar] [CrossRef]
- Yongfeng, Z.; Ping, Z.; Hong, P.; Wengang, L.; Yan, Z. Superb microvascular imaging compared with contrast-enhanced ultrasound to assess microvessels in thyroid nodules. J. Med. Ultrason. 2020, 47, 287–297. [Google Scholar] [CrossRef]
- Bayramoglu, Z.; Caliskan, E.; Karakas, Z.; Karaman, S.; Tugcu, D.; Somer, A.; Acar, M.; Akıcı, F.; Adaletli, I. Diagnostic performances of superb microvascular imaging, shear wave elastography and shape index in pediatric lymph nodes categorization: A comparative study. Br. J. Radiol. 2018, 91, 20180129. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, I.; Suh, S.; You, S.H.; Seol, H.Y. Usefulness of microvascular ultrasonography in differentiating metastatic lymphadenopathy from tuberculous lymphadenitis. Ultrasound Med. Biol. 2016, 42, 2189–2195. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.K.; Lee, J.Y.; Hong, H.S. Differentiation Between malignant and benign lymph nodes: Role of superb microvascular imaging in the evaluation of cervical lymph nodes. J. Ultrasound Med. 2019, 38, 3025–3036. [Google Scholar] [CrossRef]
- Ryoo, I.; Suh, S.; Lee, Y.H.; Seo, H.S.; Seol, H.Y.; Woo, J.-S.; Kim, S.C. Vascular pattern analysis on microvascular sonography for differentiation of pleomorphic adenomas and warthin tumors of salivary glands. J. Ultrasound Med. 2018, 37, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Bunone, G.; Vigneri, P.; Mariani, L.; Buto, S.; Collini, P.; Pilotti, S.; Pierotti, M.A.; Bongarzone, I. Expression of angiogenesis stimulators and inhibitors in human thyroid tumors and correlation with clinical pathological features. Am. J. Pathol. 1999, 155, 1967–1976. [Google Scholar] [CrossRef]
- Turner, H.E.; Harris, A.L.; Melmed, S.; Wass, J.A. Angiogenesis in endocrine tumors. Endocr. Rev. 2003, 24, 600–632. [Google Scholar] [CrossRef]
- Na, D.G.; Lim, H.K.; Byun, H.S.; Kim, H.D.; Ko, Y.H.; Baek, J.H. Differential diagnosis of cervical lymphadenopathy: Usefulness of color Doppler sonography. Am. J. Roentgenol. 1997, 168, 1311–1316. [Google Scholar] [CrossRef]
- Ying, M.; Bhatia, K.S.; Lee, Y.P.; Yuen, H.Y.; Ahuja, A.T. Review of ultrasonography of malignant neck nodes: Greyscale, Doppler, contrast enhancement and elastography. Cancer Imaging 2014, 13, 658–669. [Google Scholar] [CrossRef]
- Leboulleux, S.; Girard, E.; Rose, M.; Travagli, J.P.; Sabbah, N.; Caillou, B.; Hartl, D.M.; Lassau, N.; Baudin, E.; Schlumberger, M. Ultrasound criteria of malignancy for cervical lymph nodes in patients followed up for differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 2007, 92, 3590–3594. [Google Scholar] [CrossRef]
- Rosário, P.W.; De Faria, S.; Bicalho, L.; Alves, M.F.; Borges, M.A.; Purisch, S.; Padrão, E.L.; Rezende, L.L.; Barroso, A.L. Ultrasonographic differentiation between metastatic and benign lymph nodes in patients with papillary thyroid carcinoma. J. Ultrasound Med. 2005, 24, 1385–1389. [Google Scholar] [CrossRef]
- Kuna, S.K.; Bracic, I.; Tesic, V.; Kuna, K.; Herceg, G.H.; Dodig, D. Ultrasonographic differentiation of benign from malignant neck lymphadenopathy in thyroid cancer. J. Ultrasound Med. 2006, 25, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Sohn, Y.M.; Kwak, J.Y.; Kim, E.K.; Moon, H.J.; Kim, S.J.; Kim, M.J. Diagnostic approach for evaluation of lymph node metastasis from thyroid cancer using ultrasound and fine-needle aspiration biopsy. AJR. Am. J. Roentgenol. 2010, 194, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.W.; Bauer, A.J.; Bernet, V.A.; Ferris, R.L.; Loevner, L.A.; Mandel, S.J.; Orloff, L.A.; Randolph, G.W.; Steward, D.L. American Thyroid Association statement on preoperative imaging for thyroid cancer surgery. Thyroid 2015, 25, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Ardito, G.; Revelli, L.; Giustozzi, E.; Salvatori, M.; Fadda, G.; Ardito, F.; Avenia, N.; Ferretti, A.; Rampin, L.; Chondrogiannis, S.; et al. Aggressive papillary thyroid microcarcinoma: Prognostic factors and therapeutic strategy. Clin. Nucl. Med. 2013, 38, 25–28. [Google Scholar] [CrossRef]
- Siddiqui, S.; White, M.G.; Antic, T.; Grogan, R.H.; Angelos, P.; Kaplan, E.L.; Cipriani, N.A. Clinical and pathologic predictors of lymph node metastasis and recurrence in papillary thyroid microcarcinoma. Thyroid 2016, 26, 807–815. [Google Scholar] [CrossRef]
- Hoang, J.K.; Vanka, J.; Ludwig, B.J.; Glastonbury, C.M. Evaluation of cervical lymph nodes in head and neck cancer with CT and MRI: Tips, traps, and a systematic approach. Am. J. Roentgenol. 2013, 200, W17–W25. [Google Scholar] [CrossRef]
- Moon, J.H.; Kim, Y.I.; Lim, J.A.; Choi, H.S.; Cho, S.W.; Kim, K.W.; Park, H.J.; Paeng, J.C.; Park, Y.J.; Yi, K.H.; et al. Thyroglobulin in washout fluid from lymph node fine-needle aspiration biopsy in papillary thyroid cancer: Large-scale validation of the cutoff value to determine malignancy and evaluation of discrepant results. J. Clin. Endocrinol. Metab. 2013, 98, 1061–1068. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Benign (n = 39) | Metastasis (n = 41) | p |
|---|---|---|---|
| Female patients | 27 (69.2) | 27 (65.9) | 0.933 |
| Age (mean) | 43.4 ± 16.1 | 57.3 ± 20.2 | 0.001 |
| Treatment status | |||
| 1st thyroid cancer surgery | 34 (87.2) | 36 (87.8) | 0.824 |
| Repeated thyroid cancer surgery | 5 (12.8) | 5 (12.2) | |
| Primary tumor | |||
| Largest diameter, range (mm) | 7.1–38.0 | 6.7–45.0 | 0.421 |
| Multifocal tumor | 22 (56.4) | 26 (63.4) | 0.586 |
| Gross extrathyroidal extension | 0.877 | ||
| T3 | 2 (5.1) | 4 (9.8) | |
| T4 | 0 (0) | 1 (2.4) | |
| BRAFV600E mutation | 30 (76.9) | 35 (85.4) | 0.641 |
| Mean minimal axial diameter of LN (mm) | 8.1 ± 6.2 | 9.2 ± 5.9 | 0.533 |
| Laterality of LN | 0.877 | ||
| Left | 17 (43.5) | 18 (44.0) | |
| Right | 22 (56.4) | 23 (56.1) | |
| Location of LN | 0.001 | ||
| 1 | 1 (2.6) | 0 (0.0) | |
| 2 | 17 (43.6) | 3 (7.3) | |
| 3 | 6 (15.4) | 10 (24.4) | |
| 4 | 7 (17.9) | 22 (53.6) | |
| 5 | 4 (10.3) | 0 (0.0) | |
| 6 | 4 (10.3) | 6 (14.6) |
| Category | Numbers (%) | Malignancy Risk (%) |
|---|---|---|
| Probably benign | 26 (32.5) | 5/26 (19.2) |
| Indeterminate | 20 (25.0) | 4/20 (20.0) |
| Suspicious | 34 (42.5) | 32/34 (94.1) |
| Parameter | SMI |
|---|---|
| Sensitivity | 78.1% (32/41) |
| Specificity | 94.9% (37/39) |
| False-positive rate | 5.1% (2/39) |
| False-negative rate | 22.0% (9/41) |
| Accuracy | 86.3 % (74/80) |
| Positive predictive value | 94.1% (32/34) |
| Negative predictive value | 80.4% (37/46) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Lee, J.Y.; Yoon, R.G.; Kim, J.-h.; Hong, H.S. The Value of Microvascular Imaging for Triaging Indeterminate Cervical Lymph Nodes in Patients with Papillary Thyroid Carcinoma. Cancers 2020, 12, 2839. https://doi.org/10.3390/cancers12102839
Lee S, Lee JY, Yoon RG, Kim J-h, Hong HS. The Value of Microvascular Imaging for Triaging Indeterminate Cervical Lymph Nodes in Patients with Papillary Thyroid Carcinoma. Cancers. 2020; 12(10):2839. https://doi.org/10.3390/cancers12102839
Chicago/Turabian StyleLee, Seongyong, Ji Ye Lee, Ra Gyoung Yoon, Ji-hoon Kim, and Hyun Sook Hong. 2020. "The Value of Microvascular Imaging for Triaging Indeterminate Cervical Lymph Nodes in Patients with Papillary Thyroid Carcinoma" Cancers 12, no. 10: 2839. https://doi.org/10.3390/cancers12102839
APA StyleLee, S., Lee, J. Y., Yoon, R. G., Kim, J.-h., & Hong, H. S. (2020). The Value of Microvascular Imaging for Triaging Indeterminate Cervical Lymph Nodes in Patients with Papillary Thyroid Carcinoma. Cancers, 12(10), 2839. https://doi.org/10.3390/cancers12102839