Overexpression of PSAT1 Gene is a Favorable Prognostic Marker in Lower-Grade Gliomas and Predicts a Favorable Outcome in Patients with IDH1 Mutations and Chromosome 1p19q Codeletion


Abstract
1. Introduction
2. Results
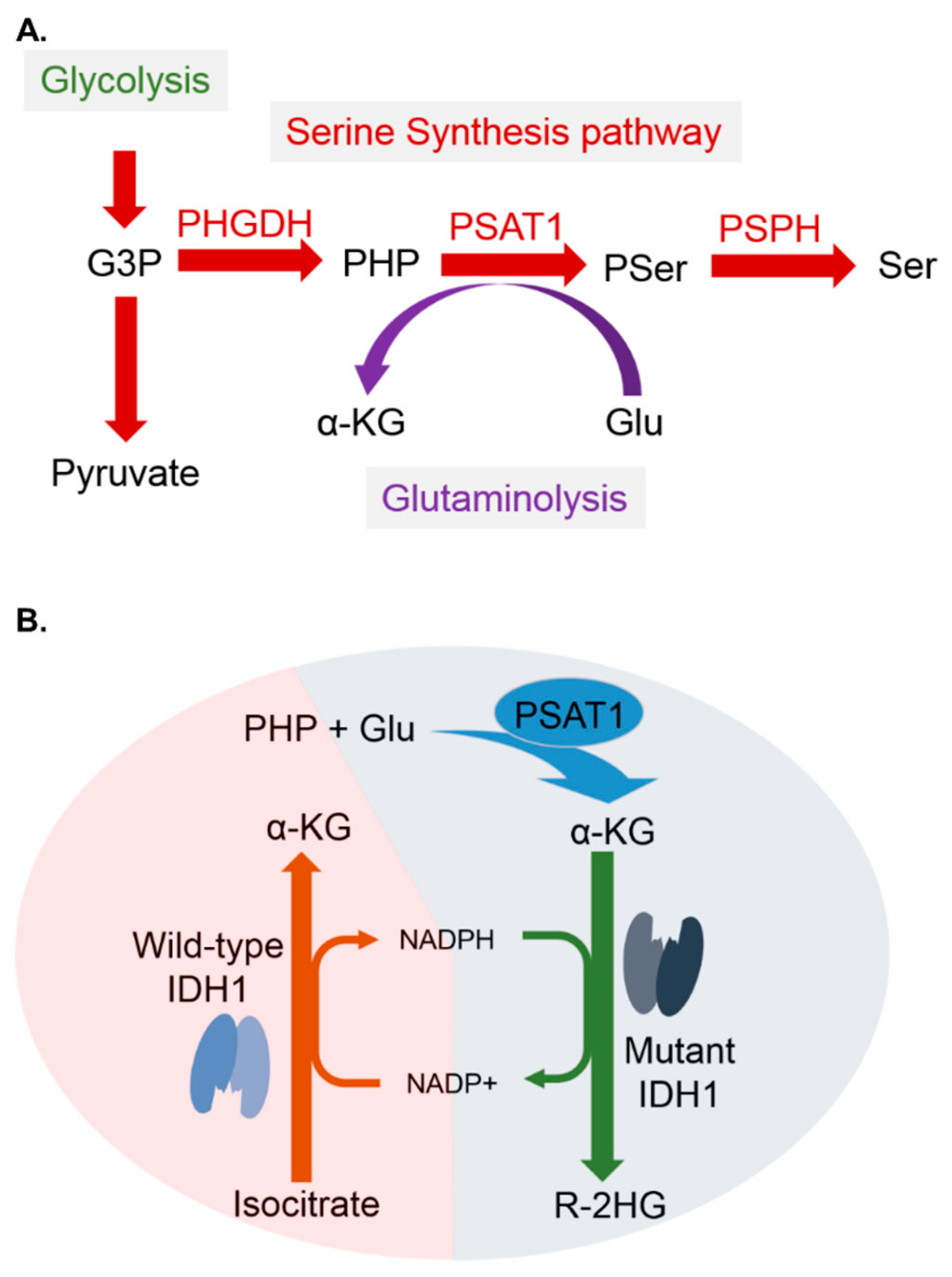
2.1. PHGDH, PSPH, and PSAT1 Are Important Regulators of the SSP and Have Certain Prognostic Significance in Various Cancers
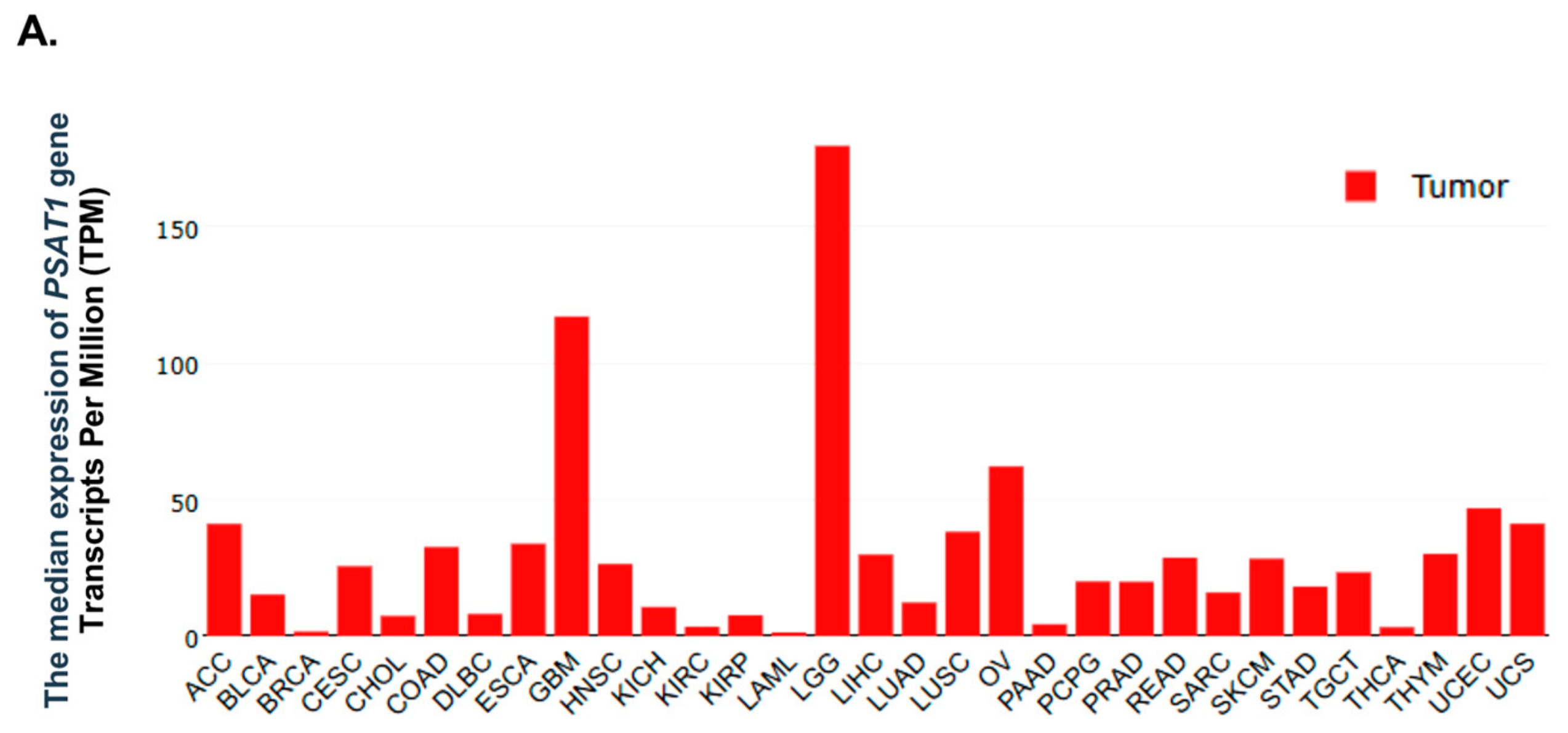
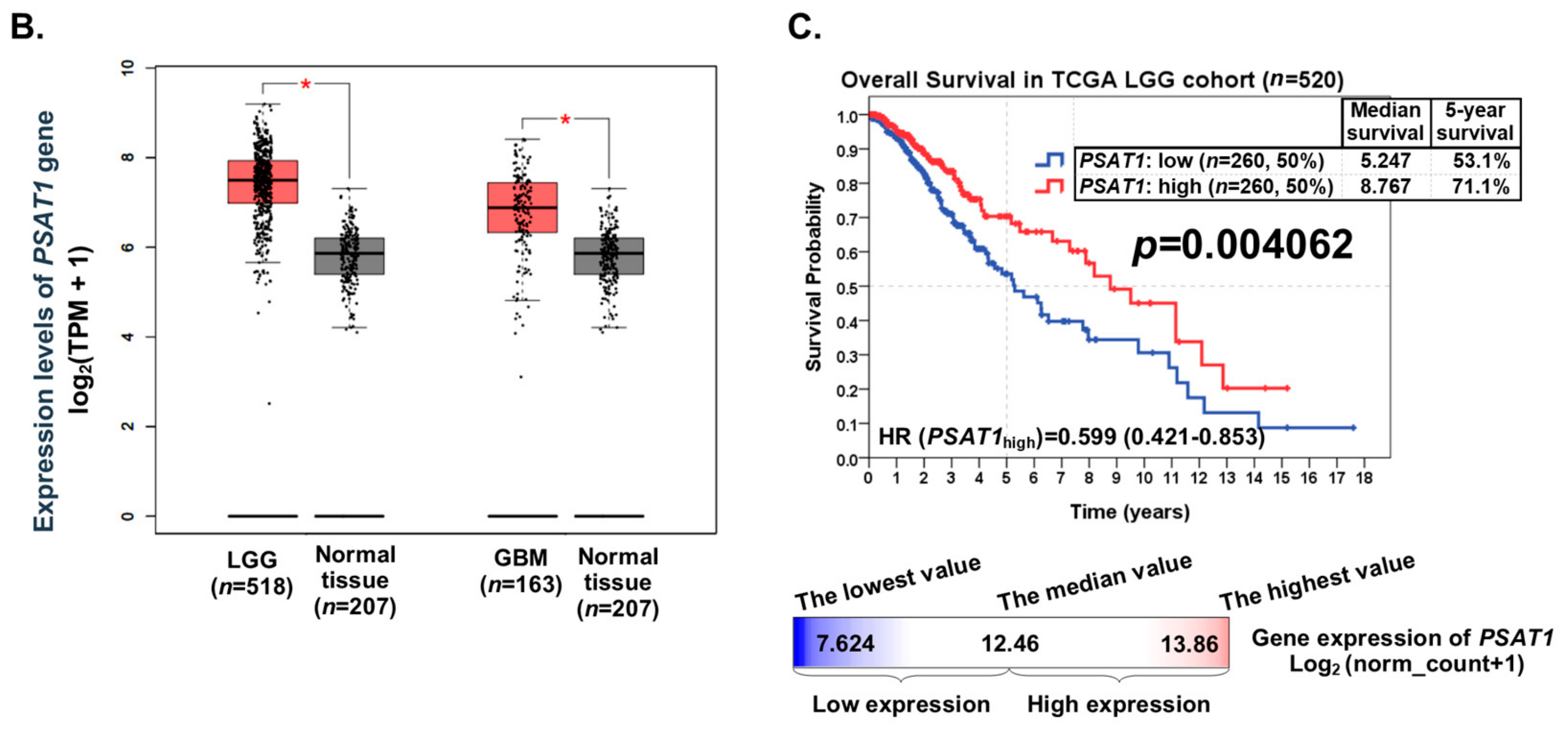
2.2. PSAT1 Is Highly Expressed and Significantly Prognostic in Lower-Grade Gliomas and Could Be a Potential Biomarker Candidate
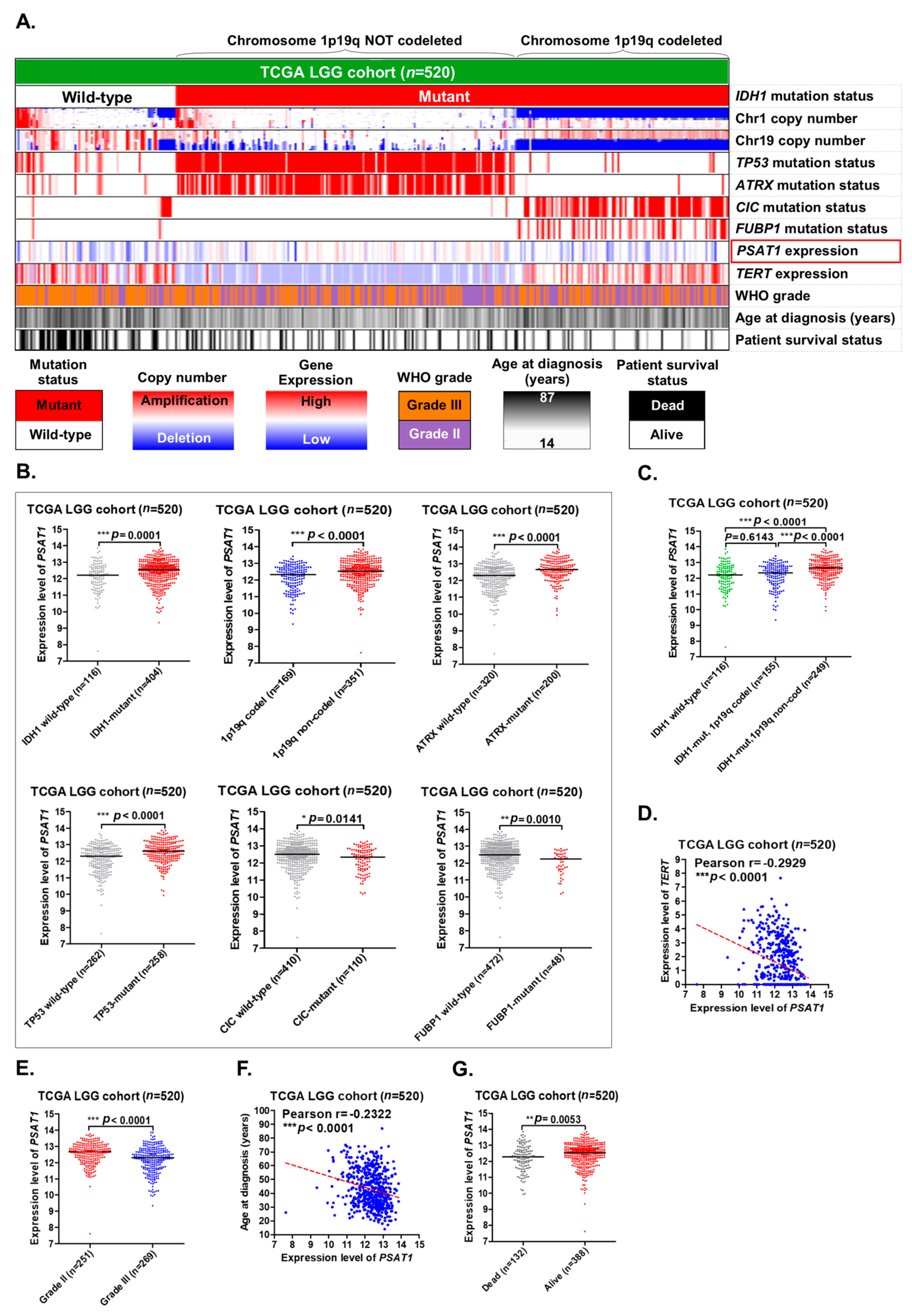
2.3. Overexpression of PSAT1 Correlates with Mutations in IDH1, ATRX and TP53 and a Lower Grade of LGGs, and Is Enriched in IDH1-Mutant LGGs without 1p19q Codeletion
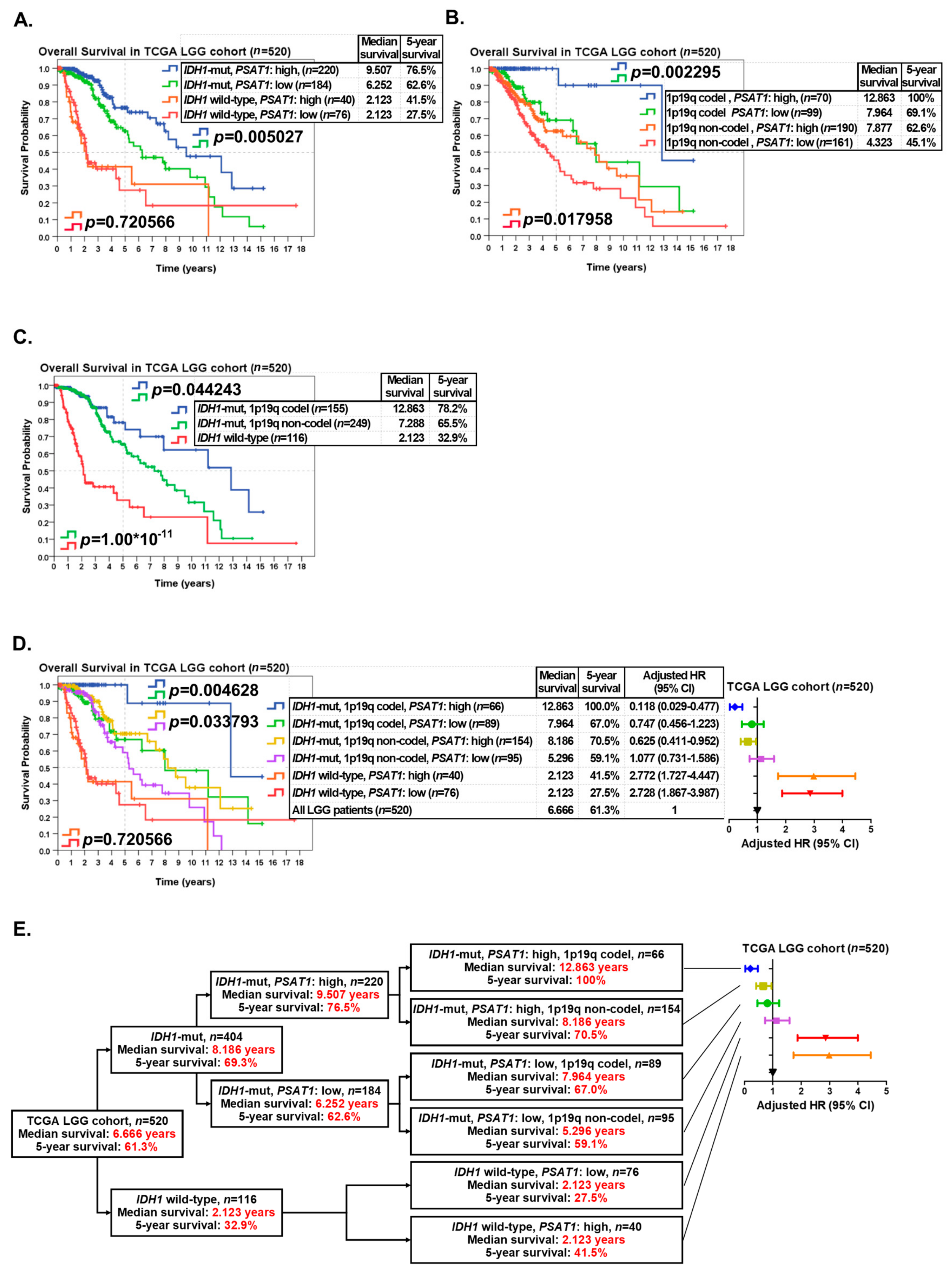
2.4. PSAT1 Expression Is Significantly Prognostic in IDH1-Mutant, 1p19q Codeleted or 1p19q Not-Codeleted LGGs and LGGs Patients with IDH1 Mutations, Chromosome 1p19q Codeletion and Overexpression of PSAT1 Have the Best Overall Survival
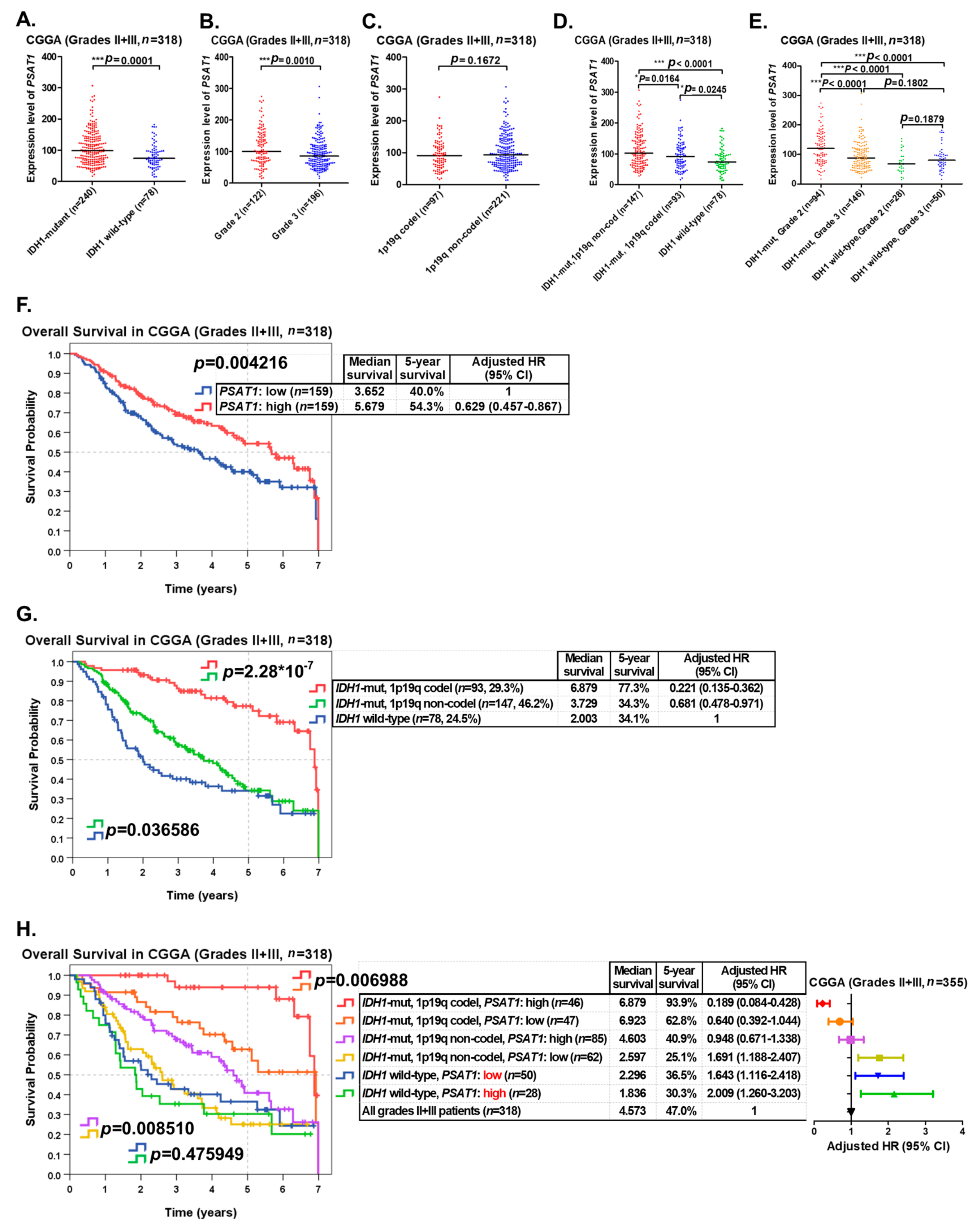
2.5. Validating the Prognostic Significance of PSAT1 in Grade II and III Gliomas Using the CGGA Dataset
3. Discussion
4. Materials and Methods
4.1. Clinical Data and Gene Expression Profiles of LGG Patients from the TCGA Website
4.2. Clinical Data and Gene Expression Profiles of LGG Patients from the CGGA Website
4.3. Classifying LGG Patients Into Distinct Subgroups for Further Analyses
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Vecchione-Koval, T.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2010–2014. Neuro Oncol. 2017, 19, v1–v88. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Nizamutdinov, D.; Stock, E.M.; Dandashi, J.A.; Vasquez, E.A.; Mao, Y.; Dayawansa, S.; Zhang, J.; Wu, E.; Fonkem, E.; Huang, J.H. Prognostication of Survival Outcomes in Patients Diagnosed with Glioblastoma. World Neurosurg. 2018, 109, e67–e74. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lu, X.; Liu, Z.; Guan, R.; Wang, J.; Kong, X.; Chen, L.; Bo, C.; Tian, K.; Xu, S.; et al. Integrating multiple-level molecular data to infer the distinctions between glioblastoma and lower-grade glioma. Int. J. Cancer 2019, 145, 952–961. [Google Scholar] [CrossRef]
- Chammas, M.; Saadeh, F.; Maaliki, M.; Assi, H. Therapeutic Interventions in Adult Low-Grade Gliomas. J. Clin. Neurol. 2019, 15, 1–8. [Google Scholar] [CrossRef]
- Yang, M.; Vousden, K.H. Serine and one-carbon metabolism in cancer. Nat. Rev. Cancer 2016, 16, 650–662. [Google Scholar] [CrossRef]
- Sowers, M.L.; Herring, J.; Zhang, W.; Tang, H.; Ou, Y.; Gu, W.; Zhang, K. Analysis of glucose-derived amino acids involved in one-carbon and cancer metabolism by stable-isotope tracing gas chromatography mass spectrometry. Anal Biochem. 2019, 566, 1–9. [Google Scholar] [CrossRef]
- De Koning, T.J.; Klomp, L.W. Serine-deficiency syndromes. Curr. Opin. Neurol. 2004, 17, 197–204. [Google Scholar] [CrossRef]
- Labuschagne, C.F.; Van Den Broek, N.J.; Mackay, G.M.; Vousden, K.H.; Maddocks, O.D. Serine, but not glycine, supports one-carbon metabolism and proliferation of cancer cells. Cell Rep. 2014, 7, 1248–1258. [Google Scholar] [CrossRef]
- Song, Z.; Feng, C.; Lu, Y.; Lin, Y.; Dong, C. PHGDH is an independent prognosis marker and contributes cell proliferation, migration and invasion in human pancreatic cancer. Gene 2018, 642, 43–50. [Google Scholar] [CrossRef]
- Possemato, R.; Marks, K.M.; Shaul, Y.D.; Pacold, M.E.; Kim, D.; Birsoy, K.; Sethumadhavan, S.; Woo, H.K.; Jang, H.G.; Jha, A.K.; et al. Functional genomics reveal that the serine synthesis pathway is essential in breast cancer. Nature 2011, 476, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Song, L.; Wan, Q.; Wu, G.; Li, X.; Wang, Y.; Wang, J.; Liu, Z.; Zhong, X.; He, X.; et al. cMyc-mediated activation of serine biosynthesis pathway is critical for cancer progression under nutrient deprivation conditions. Cell Res. 2015, 25, 429–444. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xun, Z.; Yang, Y. Inhibition of phosphoserine phosphatase enhances the anticancer efficacy of 5-fluorouracil in colorectal cancer. Biochem. Biophys. Res. Commun. 2016, 477, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wu, J.; Cai, J.; He, Z.; Yuan, J.; Zhu, X.; Li, Y.; Li, M.; Guan, H. PSAT1 regulates cyclin D1 degradation and sustains proliferation of non-small cell lung cancer cells. Int. J. Cancer 2015, 136, E39–E50. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Jia, Y.; Cao, Y.; Wu, S.; Jiang, H.; Sun, X.; Ma, J.; Yin, X.; Mao, A.; Shang, M. verexpression of Phosphoserine Aminotransferase 1 (PSAT1) Predicts Poor Prognosis and Associates with Tumor Progression in Human Esophageal Squamous Cell Carcinoma. Cell Physiol. Biochem. 2016, 39, 395–406. [Google Scholar] [CrossRef]
- Gao, S.; Ge, A.; Xu, S.; You, Z.; Ning, S.; Zhao, Y.; Pang, D. PSAT1 is regulated by ATF4 and enhances cell proliferation via the GSK3β/β-catenin/cyclin D1 signaling pathway in ER-negative breast cancer. J. Exp. Clin. Cancer Res. 2017, 36, 179. [Google Scholar] [CrossRef]
- Fang, Y.; Liang, X.; Xu, J.; Cai, X. miR-424 targets AKT3 and PSAT1 and has a tumor-suppressive role in human colorectal cancer. Cancer Manag. Res. 2018, 10, 6537–6547. [Google Scholar] [CrossRef]
- Jiang, J.; Zhang, L.; Chen, H.; Lei, Y.; Zhang, T.; Wang, Y.; Jin, P.; Lan, J.; Zhou, L.; Huang, Z.; et al. Regorafenib induces lethal autophagy arrest by stabilizing PSAT1 in glioblastoma. Autophagy 2019, 1–17. [Google Scholar] [CrossRef]
- Eckel-Passow, J.E.; Lachance, D.H.; Molinaro, A.M.; Walsh, K.M.; Decker, P.A.; Sicotte, H.; Pekmezci, M.; Rice, T.; Kosel, M.L.; Smirnov, I.V.; et al. Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors. N. Engl. J. Med. 2015, 372, 2499–2508. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive, Integrative Genomic Analysis of Diffuse Lower-Grade Gliomas. N. Engl. J. Med. 2015, 372, 2481–2498. [Google Scholar] [CrossRef]
- Foote, M.B.; Papadopoulos, N.; Diaz, L.A., Jr. Genetic Classification of Gliomas: Refining Histopathology. Cancer Cell 2015, 28, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Vatrinet, R.; Leone, G.; De Luise, M.; Girolimetti, G.; Vidone, M.; Gasparre, G.; Porcelli, A.M. The alpha-ketoglutarate dehydrogenase complex in cancer metabolic plasticity. Cancer Metab. 2017, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Sjöblom, T.; Jones, S.; Wood, L.D.; Parsons, D.W.; Lin, J.; Barber, T.D.; Mandelker, D.; Leary, R.J.; Ptak, J.; Silliman, N.; et al. The consensus coding sequences of human breast and colorectal cancers. Science 2006, 314, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Parsons, D.W.; Jones, S.; Zhang, X.; Lin, J.C.H.; Leary, R.J.; Angenendt, P.; Mankoo, P.; Carter, H.; Siu, I.M.; Gallia, G.L.; et al. An integrated genomic analysis of human glioblastoma multiforme. Science 2008, 321, 1807–1812. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Parsons, D.W.; Jin, G.; McLendon, R.; Rasheed, B.A.; Yuan, W.; Kos, I.; Batinic-Haberle, I.; Jones, S.; Riggins, G.J.; et al. IDH1 and IDH2 mutations in gliomas. N. Engl. J. Med. 2009, 360, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Labussiere, M.; Sanson, M.; Idbaih, A.; Delattre, J.Y. IDH1 gene mutations: A new paradigm in glioma prognosis and therapy? Oncologist 2010, 15, 196–199. [Google Scholar] [CrossRef]
- Lee, S.M.; Koh, H.J.; Park, D.C.; Song, B.J.; Huh, T.L.; Park, J.W. Cytosolic NADP(+)-dependent isocitrate dehydrogenase status modulates oxidative damage to cells. Free Radic. Biol. Med. 2002, 32, 1185–1196. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Enzyme | Classification | Substrate | Product | Prognostic Roles in Cancers |
|---|---|---|---|---|
| PHGDH | Oxidoreductase | 3-phosphoglycerate; NAD+ | 3-phosphohydroxypyruvate; NADH; H+ | A poor prognostic marker in Pancreatic cancer [10] and Breast cancer [11] |
| PSPH | Phosphatase | 3-Phosphoserine | Serine; phosphate ion | A poor prognostic marker in Hepatocellular cancer [12] and Colorectal cancer [13] |
| PSAT1 | Amino transferase | 3-phosphohydroxypyruvate; glutamate | 3-Phosphoserine; α-ketoglutarate | A poor prognostic marker in NSCLC [14], Esophageal Squamous Cell carcinoma [15], ER (-) Breast cancer [16] and Colorectal cancer [17] A favorable prognostic marker in Glioblastoma with regorafenib treatment [18] |
| Clinicopathological Feature | N | PSAT1 Expression, N (%) | p | |
|---|---|---|---|---|
| 520 | Low, n = 260 (50.0) | High, n = 260 (50.0) | ||
| Overall survival indicator | *** 0.000286 | |||
| 1 (dead) | 132 | 84 (63.6) | 48 (36.4) | |
| 0 (alive) | 388 | 176 (45.4) | 212 (54.6) | |
| Chromosome 1p19q status | * 0.011473 | |||
| Codeleted | 169 | 98 (58.0) | 71 (42.0) | |
| Not-codeleted | 351 | 162 (46.2) | 189 (53.8) | |
| Age | ** 0.001172 | |||
| >40 | 265 | 151 (57.0) | 114 (43.0) | |
| ≤40 | 255 | 109 (42.7) | 146 (57.3) | |
| WHO histological Grade | *** 2.246 × 10−7 | |||
| Grade III | 269 | 164 (61.0) | 105 (39.0) | |
| Grade II | 251 | 96 (38.2) | 155 (61.8) | |
| IDH1 status | *** 0.000149 | |||
| Wild-type | 116 | 76 (65.5) | 40 (34.5) | |
| Mutant | 404 | 184 (45.5) | 220 (54.5) | |
| TP53 status | *** 0.000055 | |||
| Wild-type | 262 | 154 (58.8) | 108 (41.2) | |
| Mutant | 258 | 106 (41.1) | 152 (58.9) | |
| ATRX status | *** 1.713 × 10−7 | |||
| Wild-type | 320 | 189 (59.1) | 131 (40.9) | |
| Mutant | 200 | 71 (35.5) | 129 (64.5) | |
| CIC status | 0.053261 | |||
| Mutant | 110 | 64 (58.2) | 46 (41.8) | |
| Wild-type | 410 | 196 (47.8) | 214 (52.2) | |
| FUBP1 status | ** 0.006392 | |||
| Mutant | 48 | 33 (68.8) | 15 (31.3) | |
| Wild-type | 472 | 227 (48.1) | 245 (51.9) | |
| TERT expression | *** 0.000026 | |||
| High | 260 | 154 (59.2) | 106 (40.8) | |
| Low | 260 | 106 (40.8) | 154 (59.2) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.-P.; Chan, Y.-C.; Huang, S.-Y.; Lin, Y.-F. Overexpression of PSAT1 Gene is a Favorable Prognostic Marker in Lower-Grade Gliomas and Predicts a Favorable Outcome in Patients with IDH1 Mutations and Chromosome 1p19q Codeletion. Cancers 2020, 12, 13. https://doi.org/10.3390/cancers12010013
Huang S-P, Chan Y-C, Huang S-Y, Lin Y-F. Overexpression of PSAT1 Gene is a Favorable Prognostic Marker in Lower-Grade Gliomas and Predicts a Favorable Outcome in Patients with IDH1 Mutations and Chromosome 1p19q Codeletion. Cancers. 2020; 12(1):13. https://doi.org/10.3390/cancers12010013
Chicago/Turabian StyleHuang, Shang-Pen, Yung-Chieh Chan, Shang-Yu Huang, and Yuan-Feng Lin. 2020. "Overexpression of PSAT1 Gene is a Favorable Prognostic Marker in Lower-Grade Gliomas and Predicts a Favorable Outcome in Patients with IDH1 Mutations and Chromosome 1p19q Codeletion" Cancers 12, no. 1: 13. https://doi.org/10.3390/cancers12010013
APA StyleHuang, S.-P., Chan, Y.-C., Huang, S.-Y., & Lin, Y.-F. (2020). Overexpression of PSAT1 Gene is a Favorable Prognostic Marker in Lower-Grade Gliomas and Predicts a Favorable Outcome in Patients with IDH1 Mutations and Chromosome 1p19q Codeletion. Cancers, 12(1), 13. https://doi.org/10.3390/cancers12010013