Comparison of Models for Tumor Recurrence after Liver Transplantation for the Patients with Hepatocellular Carcinoma: A Multicenter Long-Term Follow-Up Study

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Selection Criteria for LDLT
2.3. Comparison with Various LT Criteria
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Baseline Characteristics
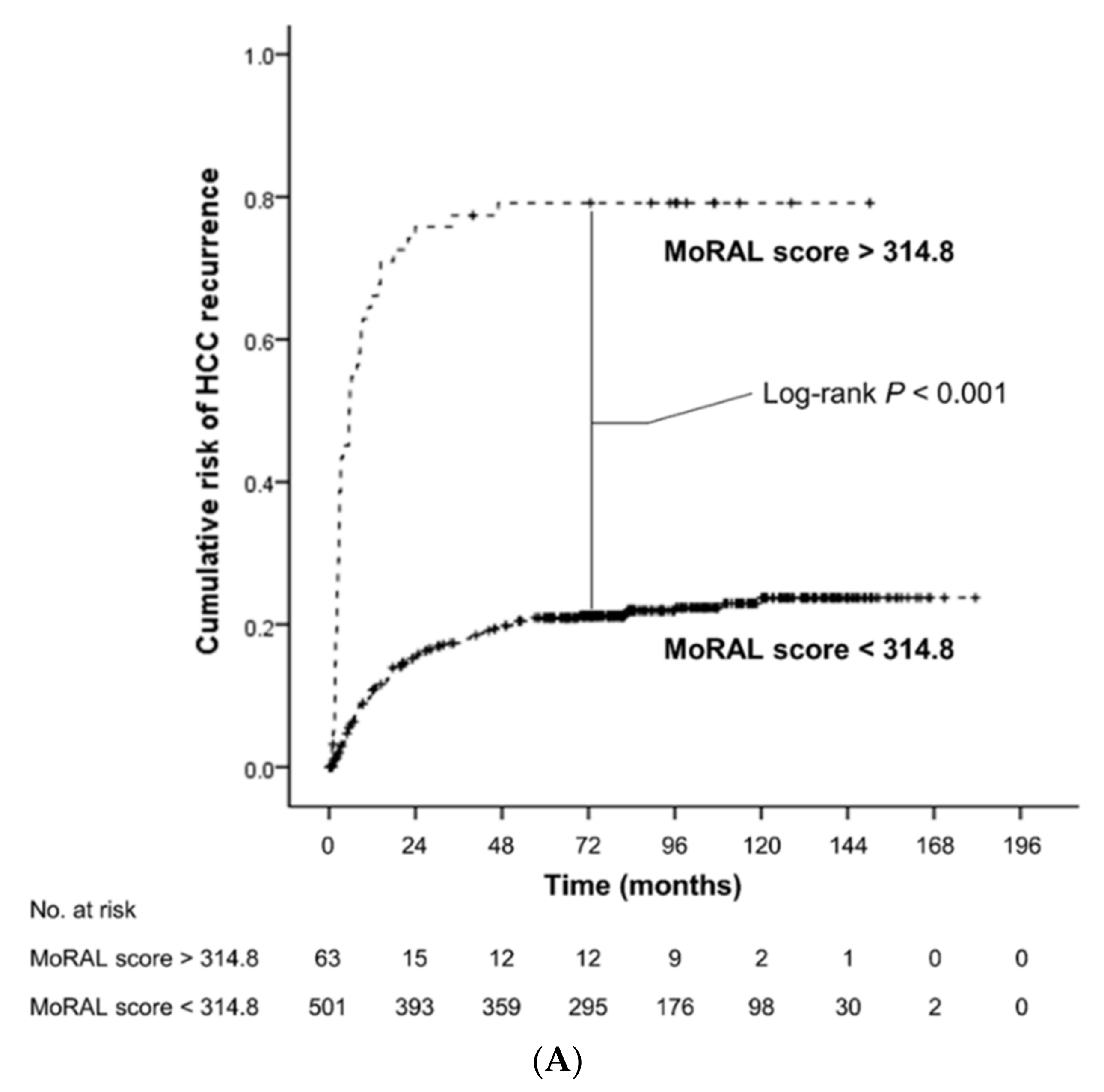
3.2. Impact of the MoRAL Score in HCC Recurrence and OS
3.3. Prognostication Power of the Models for Predicting HCC Recurrence and OS
3.4. Prognostication Power of the Models in the Beyond-MC and Within-MC Sub-Cohorts
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Wiesner, R.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003, 124, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Costentin, C.E.; Bababekov, Y.J.; Zhu, A.X.; Yeh, H. Is it time to reconsider the Milan Criteria for selecting patients with hepatocellular carcinoma for deceased-donor liver transplantation? Hepatology 2019, 69, 1324–1336. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.J.; Kim, D.G.; Na, G.H.; Hong, T.H.; You, Y.K. Extended criteria for living donor liver transplantation in patients with advanced hepatocellular carcinoma. Transplant. Proc. 2012, 44, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Gondolesi, G.E.; Roayaie, S.; Muñoz, L.; Kim-Schluger, L.; Schiano, T.; Fishbein, T.M.; Emre, S.; Miller, C.M.; Schwartz, M.E. Adult living donor liver transplantation for patients with hepatocellular carcinoma: Extending UNOS priority criteria. Ann. Surg. 2004, 239, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Olthoff, K.M.; Goldberg, D.S. The MoRAL path beyond Milan. Ann. Surg. 2016, 263, 851–852. [Google Scholar] [CrossRef]
- DuBay, D.; Sandroussi, C.; Sandhu, L.; Cleary, S.; Guba, M.; Cattral, M.S.; McGilvray, I.; Ghanekar, A.; Selzner, M.; Greig, P.D.; et al. Liver transplantation for advanced hepatocellular carcinoma using poor tumor differentiation on biopsy as an exclusion criterion. Ann. Surg. 2011, 253, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.G.; Hwang, S.; Moon, D.B.; Ahn, C.S.; Kim, K.H.; Sung, K.B.; Ko, G.Y.; Park, K.M.; Ha, T.Y.; Song, G.W. Expanded indication criteria of living donor liver transplantation for hepatocellular carcinoma at one large-volume center. Liver Transplant. 2008, 14, 935–945. [Google Scholar] [CrossRef]
- Ito, T.; Takada, Y.; Ueda, M.; Haga, H.; Maetani, Y.; Oike, F.; Ogawa, K.; Sakamoto, S.; Ogura, Y.; Egawa, H.; et al. Expansion of selection criteria for patients with hepatocellular carcinoma in living donor liver transplantation. Liver Transplant. 2007, 13, 1637–1644. [Google Scholar] [CrossRef]
- Todo, S.; Furukawa, H.; Tada, M. Extending indication: Role of living donor liver transplantation for hepatocellular carcinoma. Liver Transplant. 2007, 13, S48–S54. [Google Scholar] [CrossRef]
- Chen, C.-L.; Kabiling, C.S.; Concejero, A.M. Why does living donor liver transplantation flourish in Asia? Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 746. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Cho, Y.; Kim, H.Y.; Cho, E.J.; Lee, D.H.; Yu, S.J.; Lee, J.W.; Yi, N.J.; Lee, K.W.; Kim, S.H.; et al. Serum tumor markers provide refined prognostication in selecting liver transplantation candidate for hepatocellular carcinoma patients beyond the Milan criteria. Ann. Surg. 2016, 263, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Halazun, K.J.; Najjar, M.; Abdelmessih, R.M.; Samstein, B.; Griesemer, A.D.; Guarrera, J.V.; Kato, T.; Verna, E.C.; Emond, J.C.; Brown, R.S., Jr. Recurrence after liver transplantation for hepatocellular carcinoma: A new MORAL to the story. Ann. Surg. 2017, 265, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M. American association for the study of liver D. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Suh, S.W.; Choi, Y.; Jeong, J.; Yi, N.J.; Kim, H.; Yoon, K.C.; Hong, S.K.; Kim, H.S.; Lee, K.B.; et al. Macrovascular invasion is not an absolute contraindication for living donor liver transplantation. Liver Transplant. 2017, 23, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.; Xiao, L.; Bass, N.; Kerlan, R.; Ascher, N.; Roberts, J. Liver transplantation for hepatocellular carcinoma: Validation of the UCSF-expanded criteria based on preoperative imaging. Am. J. Transplant. 2007, 7, 2587–2596. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]
- Duvoux, C.; Roudot-Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver transplantation for hepatocellular carcinoma: A model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology 2012, 143, 986–994. [Google Scholar] [CrossRef]
- Grąt, M.; Kornasiewicz, O.; Lewandowski, Z.; Hołówko, W.; Grąt, K.; Kobryń, K.; Patkowski, W.; Zieniewicz, K.; Krawczyk, M. Combination of morphologic criteria and alpha-fetoprotein in selection of patients with hepatocellular carcinoma for liver transplantation minimizes the problem of posttransplant tumor recurrence. World J. Surg. 2014, 38, 2698–2707. [Google Scholar] [CrossRef]
- Toso, C.; Meeberg, G.; Hernandez-Alejandro, R.; Dufour, J.F.; Marotta, P.; Majno, P.; Kneteman, N.M. Total tumor volume and alpha-fetoprotein for selection of transplant candidates with hepatocellular carcinoma: A prospective validation. Hepatology 2015, 62, 158–165. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Sposito, C.; Zhou, J.; Pinna, A.D.; De Carlis, L.; Fan, J.; Cescon, M.; Di Sandro, S.; Yi-Feng, H.; Lauterio, A. Metroticket 2.0 model for analysis of competing risks of death after liver transplantation for hepatocellular carcinoma. Gastroenterology 2018, 154, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, M.; Nakashima, Y.; Nakashima, O.; Kojiro, M. Immunohistologic study on the expressions of alpha-fetoprotein and protein induced by vitamin K absence or antagonist II in surgically resected small hepatocellular carcinoma. Hepatology 2001, 34, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Todo, S.; Furukawa, H.; Japanese Study Group on Organ T. Living donor liver transplantation for adult patients with hepatocellular carcinoma: Experience in Japan. Ann. Surg. 2004, 240, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.H.; Suh, K.S.; Lee, H.W.; Cho, E.H.; Cho, J.Y.; Cho, Y.B.; Kim, I.H.; Yi, N.J.; Lee, K.U. A revised scoring system utilizing serum alphafetoprotein levels to expand candidates for living donor transplantation in hepatocellular carcinoma. Surgery 2007, 141, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Tan, J.C.; McGilvray, I.D.; Cattral, M.S.; Cleary, S.P.; Levy, G.A.; Greig, P.D.; Grant, D.R. Accuracy of staging as a predictor for recurrence after liver transplantation for hepatocellular carcinoma. Transplantation 2006, 81, 1633–1639. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.Y.; Larson, A.M.; Fix, O.K.; Yeh, M.M.; Levy, A.E.; Bakthavatsalam, R.; Halldorson, J.B.; Reyes, J.D.; Perkins, J.D. Identifying risk for recurrent hepatocellular carcinoma after liver transplantation: Implications for surveillance studies and new adjuvant therapies. Liver Transplant. 2008, 14, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Vibert, E.; Azoulay, D.; Hoti, E.; Iacopinelli, S.; Samuel, D.; Salloum, C.; Lemoine, A.; Bismuth, H.; Castaing, D.; Adam, R. Progression of alphafetoprotein before liver transplantation for hepatocellular carcinoma in cirrhotic patients: A critical factor. Am. J. Transplant. 2010, 10, 129–137. [Google Scholar] [CrossRef]
- Poté, N.; Cauchy, F.; Albuquerque, M.; Voitot, H.; Belghiti, J.; Castera, L.; Puy, H.; Bedossa, P.; Paradis, V. Performance of PIVKA-II for early hepatocellular carcinoma diagnosis and prediction of microvascular invasion. J. Hepatol. 2015, 62, 848–854. [Google Scholar] [CrossRef]
- Durazo, F.A.; Blatt, L.M.; Corey, W.G.; Lin, J.H.; Han, S.; Saab, S.; Busuttil, R.W.; Tong, M.J. Des-gamma-carboxyprothrombin, alpha-fetoprotein and AFP-L3 in patients with chronic hepatitis, cirrhosis and hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2008, 23, 1541–1548. [Google Scholar] [CrossRef]
- Marrero, J.A.; Feng, Z.; Wang, Y.; Nguyen, M.H.; Befeler, A.S.; Roberts, L.R.; Reddy, K.R.; Harnois, D.; Llovet, J.M.; Normolle, D.; et al. Alpha-fetoprotein, des-gamma carboxyprothrombin, and lectin-bound alpha-fetoprotein in early hepatocellular carcinoma. Gastroenterology 2009, 137, 110–118. [Google Scholar] [CrossRef]
- Bae, H.M.; Lee, J.H.; Yoon, J.H.; Kim, Y.J.; Heo, D.S.; Lee, H.S. Protein induced by vitamin K absence or antagonist-II production is a strong predictive marker for extrahepatic metastases in early hepatocellular carcinoma: A prospective evaluation. BMC Cancer 2011, 11, 435. [Google Scholar] [CrossRef] [PubMed]
- White, D.L.; Thrift, A.P.; Kanwal, F.; Davila, J.; El-Serag, H.B. Incidence of hepatocellular carcinoma in all 50 United States, from 2000 through 2012. Gastroenterology 2017, 152, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Yopp, A.C.; Singal, A.G. Diagnostic delays are common among patients with hepatocellular carcinoma. J. Natl. Compr. Cancer Netw. 2015, 13, 543–549. [Google Scholar] [CrossRef]
- Malik, H.Z.; Prasad, K.R.; Halazun, K.J.; Aldoori, A.; Al-Mukhtar, A.; Gomez, D.; Lodge, J.P.; Toogood, G.J. Preoperative prognostic score for predicting survival after hepatic resection for colorectal liver metastases. Ann. Surg. 2007, 246, 806–814. [Google Scholar] [CrossRef]
- Lee, H.W.; Suh, K.-S. Liver transplantation for advanced hepatocellular carcinoma. Clin. Mol. Hepatol. 2016, 22, 309. [Google Scholar] [CrossRef] [PubMed]
- Roayaie, S.; Schwartz, J.D.; Sung, M.W.; Emre, S.H.; Miller, C.M.; Gondolesi, G.E.; Krieger, N.R.; Schwartz, M.E. Recurrence of hepatocellular carcinoma after liver transplant: Patterns and prognosis. Liver Transplant. 2004, 10, 534–540. [Google Scholar] [CrossRef]
- Peng, S.Y.; Chen, W.J.; Lai, P.L.; Jeng, Y.M.; Sheu, J.C.; Hsu, H.C. High α-fetoprotein level correlates with high stage, early recurrence and poor prognosis of hepatocellular carcinoma: Significance of hepatitis virus infection, age, p53 and β-catenin mutations. Int. J. Cancer 2004, 112, 44–50. [Google Scholar] [CrossRef]
- Liu, S.H.; Lin, C.Y.; Peng, S.Y.; Jeng, Y.M.; Pan, H.W.; Lai, P.L.; Liu, C.L.; Hsu, H.C. Down-regulation of annexin A10 in hepatocellular carcinoma is associated with vascular invasion, early recurrence, and poor prognosis in synergy with p53 mutation. Am. J. Pathol. 2002, 160, 1831–1837. [Google Scholar] [CrossRef]
- Lin, S.Y.; Pan, H.W.; Liu, S.H.; Jeng, Y.M.; Hu, F.C.; Peng, S.Y.; Lai, P.L.; Hsu, H.C. ASPM is a novel marker for vascular invasion, early recurrence, and poor prognosis of hepatocellular carcinoma. Clin. Cancer Res. 2008, 14, 4814–4820. [Google Scholar] [CrossRef]
- Sapisochin, G.; Goldaracena, N.; Astete, S.; Laurence, J.M.; Davidson, D.; Rafael, E.; Castells, L.; Sandroussi, C.; Bilbao, I.; Dopazo, C.; et al. Benefit of treating hepatocellular carcinoma recurrence after liver transplantation and analysis of prognostic factors for survival in a large Euro-American series. Ann. Surg. Oncol. 2015, 22, 2286–2294. [Google Scholar] [CrossRef]
- Fernandez-Sevilla, E.; Allard, M.A.; Selten, J.; Golse, N.; Vibert, E.; Sa Cunha, A.; Cherqui, D.; Castaing, D.; Adam, R. Recurrence of hepatocellular carcinoma after liver transplantation: Is there a place for resection? Liver Transplant. 2017, 23, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Bodzin, A.S.; Lunsford, K.E.; Markovic, D.; Harlander-Locke, M.P.; Busuttil, R.W.; Agopian, V.G. Predicting mortality in patients developing recurrent hepatocellular carcinoma after liver transplantation: Impact of treatment modality and recurrence characteristics. Ann. Surg. 2017, 266, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Dutkowski, P.; De Rougemont, O.; Müllhaupt, B.; Clavien, P.A. Current and future trends in liver transplantation in Europe. Gastroenterology 2010, 138, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Park, J.-W. Epidemiology of liver cancer in South Korea. Clin. Mol. Hepatol. 2018, 24, 1. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | MoRAL < 314.8 (n = 501) | MoRAL > 314.8 (n = 63) | p Value |
|---|---|---|---|
| Age, year | 49.1 ± 19.1 | 55.1 ± 9.3 | <0.001 |
| Male, N (%) | 409 (81.6%) | 56 (88.9%) | 0.10 |
| AFP, ng/mL | 13 (5.9, 58.1) | 810 (126.6, 6509.4) | <0.001 |
| PIVKA-II, AU/mL | 26 (15, 61) | 1200 (726.5, 2218.5) | <0.001 |
| MoRAL score | 66.7 (51.87, 113.79) | 478.7 (386.53, 694.92) | <0.001 |
| Child-Pugh class: A/B/C, N (%) | 299/119/83 (59.7/23.8/16.5%) | 36/16/11 (57.7/25/17.3%) | 0.66 |
| BCLC stage: 0/A/B/C/D, N (%) | 61/226/81/36/97 (12.2/45.1/16.2/7.2/19.4%) | 1/9/18/23/12 (1.6/14.3/28.6/36.5/19%) | <0.001 |
| Maximal size of HCC, cm | 2.5 ± 1.5 | 6.0 ± 3.2 | <0.001 |
| Number of HCC, N | 2.3 ± 2.7 | 5.9 ± 8.4 | <0.001 |
| Type of HCC: nodular/diffuse or infiltrative, N (%) | 475/26 (94.9/5.1%) | 35/28 (54.9/45.1%) | <0.001 |
| Portal vein invasion, N (%) | 54 (10.7%) | 29 (46%) | <0.001 |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Serum | 1.003 (1.003–1.004) | <0.001 | 1.002 (1.001–1.003) | <0.001 |
| Serum | 1.02 (1.016–1.023) | <0.001 | 1.018 (1.015–1.022) | <0.001 |
| NLR | 1.01 (0.99–1.04) | 0.32 | 1.003 (0.97–1.03) | 0.87 |
| Maximal size of HCC | 1.34 (1.27–1.40) | <0.001 | ||
| Number of HCC | 1.08 (1.05–1.10) | <0.001 | ||
| Diffuse or infiltrative type of HCC | 3.27 (2.33–4.58) | <0.001 | ||
| A: C-Indices for Predicting HCC Recurrence by Various Models in the Entire Cohort | ||||||||||
| Models | C-Index | 95% Confidence Interval | p Value * | |||||||
| Lower | Upper | |||||||||
| MoRAL score | 0.77 | 0.73 | 0.82 | |||||||
| WCM model | 0.69 | 0.65 | 0.73 | <0.001 | ||||||
| AFP model | 0.68 | 0.65 | 0.72 | <0.001 | ||||||
| UCSF or Up-to-seven and AFP | 0.68 | 0.64 | 0.71 | <0.001 | ||||||
| Metroticket 2.0 Model | 0.68 | 0.64 | 0.71 | <0.001 | ||||||
| Milan criteria | 0.64 | 0.60 | 0.67 | <0.001 | ||||||
| UCSF criteria | 0.62 | 0.58 | 0.65 | <0.001 | ||||||
| Up-to-seven criteria | 0.61 | 0.58 | 0.64 | <0.001 | ||||||
| Total tumor volume/AFP criteria | 0.52 | 0.49 | 0.55 | <0.001 | ||||||
| Kyoto criteria | 0.50 | 0.47 | 0.53 | <0.001 | ||||||
| B: Comparison of the AUROC for Predicting 1-Year, 3-Year, and 5-Year HCC Recurrence by Various Predicting Models in the Entire Cohort | ||||||||||
| Models | AUROC | 95% CI | p Value * | p Value † | ||||||
| Lower | Upper | |||||||||
| 1 year | MoRAL score | 0.85 | 0.80 | 0.89 | <0.001 | |||||
| WCM model | 0.75 | 0.70 | 0.81 | <0.001 | <0.001 | |||||
| AFP model | 0.76 | 0.70 | 0.82 | <0.001 | <0.001 | |||||
| UCSF or Up-to-seven and AFP | 0.76 | 0.71 | 0.82 | <0.001 | <0.001 | |||||
| Metroticket 2.0 Model | 0.75 | 0.69 | 0.81 | <0.001 | <0.001 | |||||
| 3 year | MoRAL score | 0.82 | 0.78 | 0.87 | <0.001 | |||||
| WCM model | 0.72 | 0.67 | 0.78 | <0.001 | <0.001 | |||||
| AFP model | 0.73 | 0.68 | 0.78 | <0.001 | <0.001 | |||||
| UCSF or Up-to-seven and AFP | 0.73 | 0.68 | 0.78 | <0.001 | <0.001 | |||||
| Metroticket 2.0 Model | 0.71 | 0.65 | 0.76 | <0.001 | <0.001 | |||||
| 5 year | MoRAL score | 0.79 | 0.75 | 0.83 | <0.001 | |||||
| WCM model | 0.70 | 0.65 | 0.76 | <0.001 | <0.001 | |||||
| AFP model | 0.70 | 0.65 | 0.75 | <0.001 | <0.001 | |||||
| UCSF or Up-to-seven and AFP | 0.70 | 0.65 | 0.75 | <0.001 | <0.001 | |||||
| Metroticket 2.0 Model | 0.68 | 0.63 | 0.74 | <0.001 | <0.001 | |||||
| Models | C-Index | 95% Confidence Interval | p Value * | |
|---|---|---|---|---|
| Lower | Upper | |||
| MoRAL score | 0.64 | 0.59 | 0.69 | |
| WCM model | 0.62 | 0.58 | 0.66 | 0.16 |
| AFP model | 0.58 | 0.55 | 0.62 | 0.004 |
| UCSF or Up-to-seven and AFP | 0.58 | 0.54 | 0.62 | 0.003 |
| Metroticket 2.0 Model | 0.58 | 0.54 | 0.61 | 0.002 |
| UCSF criteria | 0.55 | 0.51 | 0.58 | <0.001 |
| Milan criteria | 0.54 | 0.50 | 0.58 | <0.001 |
| Up-to-seven criteria | 0.53 | 0.50 | 0.56 | <0.001 |
| Total tumor volume/AFP criteria | 0.52 | 0.49 | 0.55 | <0.001 |
| Kyoto criteria | 0.51 | 0.48 | 0.54 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.; Cho, Y.; Lee, J.-H.; Lee, Y.B.; Cho, E.J.; Yu, S.J.; Sinn, D.H.; Kim, B.H.; Kim, S.H.; Yi, N.-J.; et al. Comparison of Models for Tumor Recurrence after Liver Transplantation for the Patients with Hepatocellular Carcinoma: A Multicenter Long-Term Follow-Up Study. Cancers 2019, 11, 1295. https://doi.org/10.3390/cancers11091295
Chang Y, Cho Y, Lee J-H, Lee YB, Cho EJ, Yu SJ, Sinn DH, Kim BH, Kim SH, Yi N-J, et al. Comparison of Models for Tumor Recurrence after Liver Transplantation for the Patients with Hepatocellular Carcinoma: A Multicenter Long-Term Follow-Up Study. Cancers. 2019; 11(9):1295. https://doi.org/10.3390/cancers11091295
Chicago/Turabian StyleChang, Young, Yuri Cho, Jeong-Hoon Lee, Yun Bin Lee, Eun Ju Cho, Su Jong Yu, Dong Hyun Sinn, Bo Hyun Kim, Seoung Hoon Kim, Nam-Joon Yi, and et al. 2019. "Comparison of Models for Tumor Recurrence after Liver Transplantation for the Patients with Hepatocellular Carcinoma: A Multicenter Long-Term Follow-Up Study" Cancers 11, no. 9: 1295. https://doi.org/10.3390/cancers11091295
APA StyleChang, Y., Cho, Y., Lee, J.-H., Lee, Y. B., Cho, E. J., Yu, S. J., Sinn, D. H., Kim, B. H., Kim, S. H., Yi, N.-J., Lee, K.-W., Kim, J. M., Park, J.-W., Kim, Y. J., Yoon, J.-H., Joh, J.-W., & Suh, K.-S. (2019). Comparison of Models for Tumor Recurrence after Liver Transplantation for the Patients with Hepatocellular Carcinoma: A Multicenter Long-Term Follow-Up Study. Cancers, 11(9), 1295. https://doi.org/10.3390/cancers11091295