11C-hydroxy-ephedrine-PET/CT in the Diagnosis of Pheochromocytoma and Paraganglioma

 ,
, 
Abstract
1. Introduction
2. Results
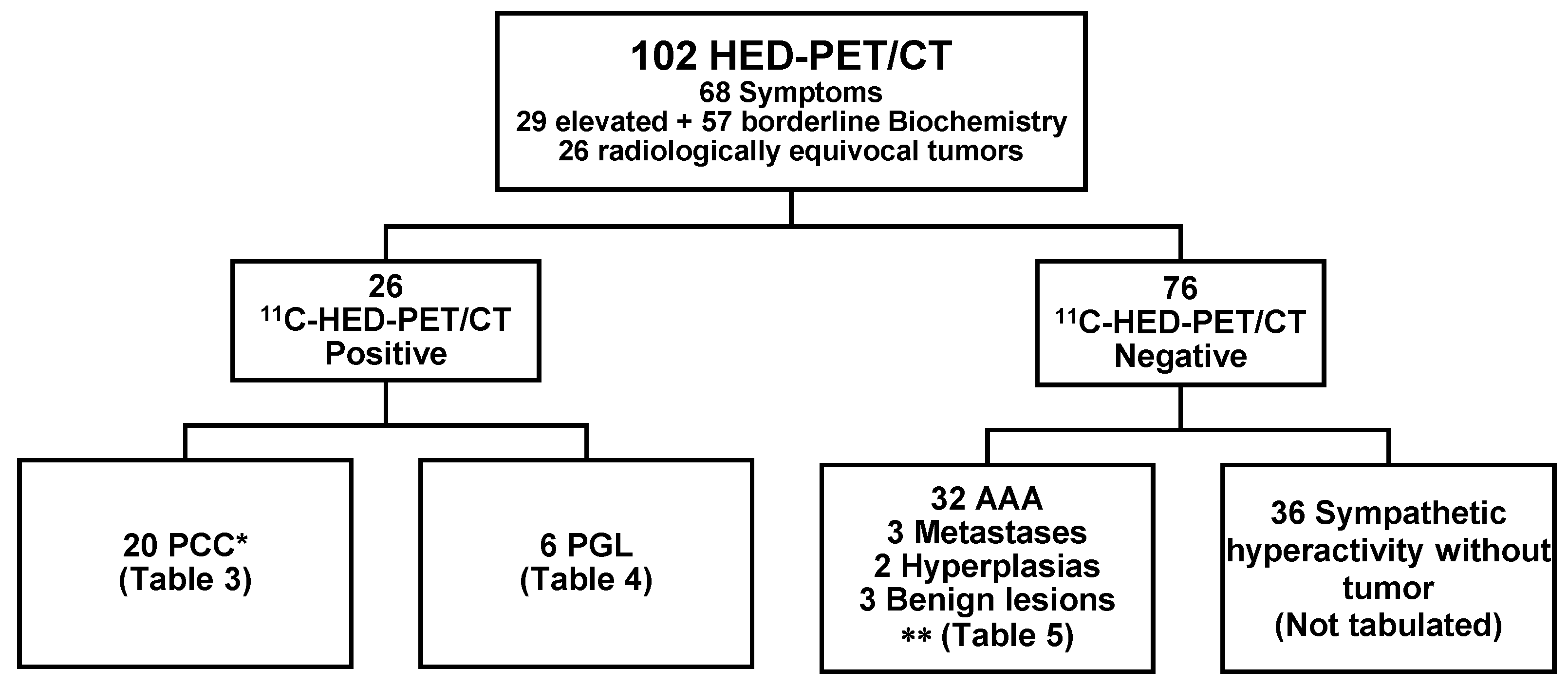
2.1. Baseline Patient Characteristics
2.2. Diagnostic Performance
2.3. Tabulated Results
2.4. 11C-HED Accumulation and Uptake Measurements
3. Discussion
4. Patients and Methods
4.1. Patients
4.2. 11C-Hydroxy-ephedrine-PET/CT Examination
4.3. Image Analysis and Interpretation
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kantorovich, V.; Pacak, K. Pheochromocytoma and Paraganglioma. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2010; Volune 182, pp. 343–373. ISBN 978-0-444-53616-7. [Google Scholar]
- Bravo, E.L. Evolving Concepts in the Pathophysiology, Diagnosis, and Treatment of Pheochromocytoma. Endocr. Rev. 1994, 15, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Lenders, J.W.; Eisenhofer, G.; Mannelli, M.; Pacak, K. Phaeochromocytoma. Lancet 2005, 366, 665–675. [Google Scholar] [CrossRef]
- Lenders, J.W.M.; Pacak, K.; Walther, M.M.; Linehan, W.M.; Mannelli, M.; Friberg, P.; Keiser, H.R.; Goldstein, D.S.; Eisenhofer, G. Biochemical diagnosis of pheochromocytoma: Which test is best? JAMA 2002, 287, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Lenders, J.W.M.; Duh, Q.-Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.-P.; Grebe, S.K.G.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F. Pheochromocytoma and Paraganglioma: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar] [CrossRef] [PubMed]
- Song, J.H.; Chaudhry, F.S.; Mayo-Smith, W.W. The Incidental Adrenal Mass on CT: Prevalence of Adrenal Disease in 1,049 Consecutive Adrenal Masses in Patients with No Known Malignancy. Am. J. Roentgenol. 2008, 190, 1163–1168. [Google Scholar] [CrossRef] [PubMed]
- Hammarstedt, L.; Muth, A.; Wängberg, B.; Björneld, L.; Sigurjónsdóttir, H.A.; Götherström, G.; Almqvist, E.; Widell, H.; Carlsson, S.; Ander, S.; et al. Adrenal lesion frequency: A prospective, cross-sectional CT study in a defined region, including systematic re-evaluation. Acta Radiol. 2010, 51, 1149–1156. [Google Scholar] [CrossRef]
- Blake, M.A.; Cronin, C.G.; Boland, G.W. Adrenal Imaging. Am. J. Roentgenol. 2010, 194, 1450–1460. [Google Scholar] [CrossRef] [PubMed]
- Morelli, V.; Scillitani, A.; Arosio, M.; Chiodini, I. Follow-up of patients with adrenal incidentaloma, in accordance with the European society of endocrinology guidelines: Could we be safe? J. Endocrinol. Investig. 2017, 40, 331–333. [Google Scholar] [CrossRef]
- Brito, J.P.; Asi, N.; Gionfriddo, M.R.; Norman, C.; Leppin, A.L.; Zeballos-Palacios, C.; Undavalli, C.; Wang, Z.; Domecq, J.P.; Prustsky, G.; et al. The incremental benefit of functional imaging in pheochromocytoma/paraganglioma: A systematic review. Endocrine 2015, 50, 176–186. [Google Scholar] [CrossRef]
- Taieb, D.; Neumann, H.; Rubello, D.; Al-Nahhas, A.; Guillet, B.; Hindie, E. Modern Nuclear Imaging for Paragangliomas: Beyond SPECT. J. Nucl. Med. 2012, 53, 264–274. [Google Scholar] [CrossRef]
- Shulkin, B.L.; Thompson, N.W.; Shapiro, B.; Francis, I.R.; Sisson, J.C. Pheochromocytomas: Imaging with 2-[Fluorine-18]fluoro-2-deoxy-d-glucose PET. Radiology 1999, 212, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Berglund, A.S.; Hulthén, U.L.; Manhem, P.; Thorsson, O.; Wollmer, P.; Törnquist, C. Metaiodobenzylguanidine (MIBG) scintigraphy and computed tomography (CT) in clinical practice. Primary and secondary evaluation for localization of phaeochromocytomas. J. Intern. Med. 2001, 249, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Hoegerle, S.; Nitzsche, E.; Altehoefer, C.; Ghanem, N.; Manz, T.; Brink, I.; Reincke, M.; Moser, E.; Neumann, H.P.H. Pheochromocytomas: Detection with 18 F DOPA Whole-Body PET—Initial Results. Radiology 2002, 222, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Archier, A.; Varoquaux, A.; Garrigue, P.; Montava, M.; Guerin, C.; Gabriel, S.; Beschmout, E.; Morange, I.; Fakhry, N.; Castinetti, F.; et al. Prospective comparison of (68)Ga-DOTATATE and (18)F-FDOPA PET/CT in patients with various pheochromocytomas and paragangliomas with emphasis on sporadic cases. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1248–1257. [Google Scholar] [CrossRef] [PubMed]
- Moog, S.; Houy, S.; Chevalier, E.; Ory, S.; Weryha, G.; Rame, M.; Klein, M.; Brunaud, L.; Gasman, S.; Cuny, T. 18F-FDOPA PET/CT Uptake Parameters Correlate with Catecholamine Secretion in Human Pheochromocytomas. Neuroendocrinology 2018, 107, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Santhanam, P.; Taïeb, D. Role of (18) F-FDOPA PET/CT imaging in endocrinology. Clin. Endocrinol. (Oxf.) 2014, 81, 789–798. [Google Scholar] [CrossRef]
- Timmers, H.J.L.M.; Chen, C.C.; Carrasquillo, J.A.; Whatley, M.; Ling, A.; Havekes, B.; Eisenhofer, G.; Martiniova, L.; Adams, K.T.; Pacak, K. Comparison of 18F-Fluoro-L-DOPA, 18F-Fluoro-Deoxyglucose, and 18F-Fluorodopamine PET and 123I-MIBG Scintigraphy in the Localization of Pheochromocytoma and Paraganglioma. J. Clin. Endocrinol. Metab. 2009, 94, 4757–4767. [Google Scholar] [CrossRef]
- Amodru, V.; Guerin, C.; Delcourt, S.; Romanet, P.; Loundou, A.; Viana, B.; Brue, T.; Castinetti, F.; Sebag, F.; Pacak, K.; et al. Quantitative 18F-DOPA PET/CT in pheochromocytoma: The relationship between tumor secretion and its biochemical phenotype. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 278–282. [Google Scholar] [CrossRef]
- Ilias, I.; Chen, C.C.; Carrasquillo, J.A.; Whatley, M.; Ling, A.; Lazúrová, I.; Adams, K.T.; Perera, S.; Pacak, K. Comparison of 6-18F-fluorodopamine PET with 123I-metaiodobenzylguanidine and 111in-pentetreotide scintigraphy in localization of nonmetastatic and metastatic pheochromocytoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2008, 49, 1613–1619. [Google Scholar] [CrossRef]
- Ilias, I.; Yu, J.; Carrasquillo, J.A.; Chen, C.C.; Eisenhofer, G.; Whatley, M.; McElroy, B.; Pacak, K. Superiority of 6-[18F]-Fluorodopamine Positron Emission Tomography Versus [131I]-Metaiodobenzylguanidine Scintigraphy in the Localization of Metastatic Pheochromocytoma. J. Clin. Endocrinol. Metab. 2003, 88, 4083–4087. [Google Scholar] [CrossRef]
- Timmers, H.J.L.M.; Eisenhofer, G.; Carrasquillo, J.A.; Chen, C.C.; Whatley, M.; Ling, A.; Adams, K.T.; Pacak, K. Use of 6-[ 18F]-fluorodopamine positron emission tomography (PET) as first-line investigation for the diagnosis and localization of non-metastatic and metastatic phaeochromocytoma (PHEO). Clin. Endocrinol. (Oxf.) 2009, 71, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Kaji, P.; Carrasquillo, J.A.; Linehan, W.M.; Chen, C.C.; Eisenhofer, G.; Pinto, P.A.; Lai, E.W.; Pacak, K. The role of 6-[ 18F]fluorodopamine positron emission tomography in the localization of adrenal pheochromocytoma associated with von Hippel–Lindau syndrome. Eur. J. Endocrinol. 2007, 156, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Gild, M.L.; Naik, N.; Hoang, J.; Hsiao, E.; McGrath, R.T.; Sywak, M.; Sidhu, S.; Delbridge, L.W.; Robinson, B.G.; Schembri, G.; et al. Role of DOTATATE-PET/CT in preoperative assessment of phaeochromocytoma and paragangliomas. Clin. Endocrinol. (Oxf.) 2018, 89, 139–147. [Google Scholar] [CrossRef]
- Janssen, I.; Chen, C.C.; Millo, C.M.; Ling, A.; Taieb, D.; Lin, F.I.; Adams, K.T.; Wolf, K.I.; Herscovitch, P.; Fojo, A.T.; et al. PET/CT comparing 68Ga-DOTATATE and other radiopharmaceuticals and in comparison with CT/MRI for the localization of sporadic metastatic pheochromocytoma and paraganglioma. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1784–1791. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.; Ling, A.; Millo, C.; Gupta, G.; Viana, B.; Lin, F.I.; Herscovitch, P.; Adams, K.T.; Taïeb, D.; Metwalli, A.R.; et al. Superiority of 68Ga-DOTATATE over 18F-FDG and anatomic imaging in the detection of succinate dehydrogenase mutation (SDHx)-related pheochromocytoma and paraganglioma in the pediatric population. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 787–797. [Google Scholar] [CrossRef]
- Janssen, I.; Blanchet, E.M.; Adams, K.; Chen, C.C.; Millo, C.M.; Herscovitch, P.; Taieb, D.; Kebebew, E.; Lehnert, H.; Fojo, A.T.; et al. Superiority of [68Ga]-DOTATATE PET/CT to Other Functional Imaging Modalities in the Localization of SDHB-Associated Metastatic Pheochromocytoma and Paraganglioma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2015, 21, 3888–3895. [Google Scholar] [CrossRef]
- Yamamoto, S.; Hellman, P.; Wassberg, C.; Sundin, A. 11C-Hydroxyephedrine Positron Emission Tomography Imaging of Pheochromocytoma: A Single Center Experience over 11 Years. J. Clin. Endocrinol. Metab. 2012, 97, 2423–2432. [Google Scholar] [CrossRef][Green Version]
- Yamamoto, S.; Wassberg, C.; Hellman, P.; Sundin, A. (11)C-Hydroxyephedrine Positron Emission Tomography in the Postoperative Management of Pheochromocytoma and Paraganglioma. Neuroendocrinology 2014, 100, 60–70. [Google Scholar] [CrossRef]
- Shulkin, B.L.; Wieland, D.M.; Schwaiger, M.; Thompson, N.W.; Francis, I.R.; Haka, M.S.; Rosenspire, K.C.; Shapiro, B.; Sisson, J.C.; Kuhl, D.E. PET scanning with hydroxyephedrine: An approach to the localization of pheochromocytoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1992, 33, 1125–1131. [Google Scholar]
- Trampal, C.; Engler, H.; Juhlin, C.; Bergström, M.; Långström, B. Pheochromocytomas: Detection with 11C Hydroxyephedrine PET. Radiology 2004, 230, 423–428. [Google Scholar] [CrossRef]
- Franzius, C.; Hermann, K.; Weckesser, M.; Kopka, K.; Juergens, K.U.; Vormoor, J.; Schober, O. Whole-body PET/CT with 11C-meta-hydroxyephedrine in tumors of the sympathetic nervous system: Feasibility study and comparison with 123I-MIBG SPECT/CT. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2006, 47, 1635–1642. [Google Scholar]
- Rosenspire, K.C.; Haka, M.S.; Van Dort, M.E.; Jewett, D.M.; Gildersleeve, D.L.; Schwaiger, M.; Wieland, D.M. Synthesis and preliminary evaluation of carbon-11-meta-hydroxyephedrine: A false transmitter agent for heart neuronal imaging. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1990, 31, 1328–1334. [Google Scholar]
- Shulkin, B.L.; Wieland, D.M.; Baro, M.E.; Ungar, D.R.; Mitchell, D.S.; Dole, M.G.; Rawwas, J.B.; Castle, V.P.; Sisson, J.C.; Hutchinson, R.J. PET hydroxyephedrine imaging of neuroblastoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 1996, 37, 16–21. [Google Scholar]
- Han, S.; Suh, C.H.; Woo, S.; Kim, Y.J.; Lee, J.J. Performance of 68Ga-DOTA–Conjugated Somatostatin Receptor–Targeting Peptide PET in Detection of Pheochromocytoma and Paraganglioma: A Systematic Review and Metaanalysis. J. Nucl. Med. 2019, 60, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Timmers, H.J.L.M.; Kozupa, A.; Chen, C.C.; Carrasquillo, J.A.; Ling, A.; Eisenhofer, G.; Adams, K.T.; Solis, D.; Lenders, J.W.M.; Pacak, K. Superiority of Fluorodeoxyglucose Positron Emission Tomography to Other Functional Imaging Techniques in the Evaluation of Metastatic SDHB -Associated Pheochromocytoma and Paraganglioma. J. Clin. Oncol. 2007, 25, 2262–2269. [Google Scholar] [CrossRef] [PubMed]
- Rischke, H.C.; Benz, M.R.; Wild, D.; Mix, M.; Dumont, R.A.; Campbell, D.; Seufert, J.; Wiech, T.; Rossler, J.; Weber, W.A.; et al. Correlation of the Genotype of Paragangliomas and Pheochromocytomas with Their Metabolic Phenotype on 3,4-Dihydroxy-6-18F-Fluoro-L-Phenylalanin PET. J. Nucl. Med. 2012, 53, 1352–1358. [Google Scholar] [CrossRef]
- Blake, M.A.; Kalra, M.K.; Maher, M.M.; Sahani, D.V.; Sweeney, A.T.; Mueller, P.R.; Hahn, P.F.; Boland, G.W. Pheochromocytoma: An Imaging Chameleon. RadioGraphics 2004, 24, S87–S99. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gold standard | |||
|---|---|---|---|
| Positive | Negative | ||
| 11C-HED-PET/CT | Positive | 25 | 1 |
| Negative | 1 | 75 | |
| Gold standard | |||
|---|---|---|---|
| Positive | Negative | ||
| 11C-HED-PET/CT | Positive | 25 | 1 |
| Negative | 1 | 14 | |
| Pat No. | Age | Sex | Clinical Information | Incidenta-loma | Systolic BP | Diagnosis (PAD) | NA-Ref | A- Ref | A/N Ratio |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 45 | F | Sweating, palpitations anxiety | Y | 220 | L PCC R AAA | 11.5 | 1.00 | 0.09 |
| 2 | 73 | F | Palpitations, headache, HT, alpha blocker | Y | 150 | R PCC+AAA | 2.00 | 3.50 | 1.75 |
| 3 | 67 | F | Sweating, headache, alpha blocker | Y | 150 | R PCC L AAA | 1.33 | 1.00 | 0.75 |
| 4 | 48 | F | Anxiety, palpitations, muscle fasciculations, alpha blocker | Y | 150 | PCC | 12.8 | 1.00 | 0.08 |
| 5 | 85 | F | Rectal cancer Incidentaloma | Y | 140 | PCC with cystic areas | 10.7 | 1.00 | 0.09 |
| 6 | 53 | F | Polycystic kidney disease, HT | Y | 180 | PCC | 1.00 | 5.00 | 5.00 |
| 7 | 52 | M | No symptom | Y | 190 | PCC | 2.00 | 1.44 | 0.72 |
| 8 | 71 | F | Breast cancer, small-intestinal NET | Y | 150 | PCC | 0.56 | 0.51 | 0.92 |
| 9 | 19 | F | Bilateral incidentalomas | Y | 180 | PCC | 1.83 | 3.50 | 1.91 |
| 10 | 58 | F | Palpitations, alpha blocker | Y | 130 | PCC | 1.33 | 1.00 | 0.75 |
| 11 | 28 | F | No symptoms | Y | 120 | PCC | 1.56 | 2.13 | 1.37 |
| 12 | 30 | F | Palpitations, panic attack | N | 110 | PCC | 1.33 | 3.02 | 2.27 |
| 13 | 72 | F | Sweating, alpha blocker | N | 220 | PCC | 3.74 | 1.67 | 0.45 |
| 14 | 50 | F | Palpitations, headache, HT | N | 215 | PCC | 61.7 | 95.0 | 1.54 |
| 15 | 59 | M | Incidentaloma | Y | 200 | PCC | 1.00 | 2.50 | 2.50 |
| 16 | 42 | F | Palpitations, sweating, headache, tremor | N | 130 | PCC with cystic areas | 2.68 | 9.80 | 3.66 |
| 17 | 58 | F | Sweating, palpitations HT, alpha blocker | N | 170 | PCC with necrosis | 8.83 | 39.5 | 4.47 |
| 18 | 64 | M | HT, alpha blocker | N | 220 | PCC with necrosis | 22.3 | 107 | 4.77 |
| 19 | 61 | F | Headache, flushing, sweating, palpitations, alpha blocker | N | 230 | L PCC* R hyperplasia | 11.4 | 3.89 | 0.34 |
| 20 | 65 | F | Sweating, palpitations, alpha blocker | N | 140 | PCC | 2 | 1 | 0.5 |
| Pat No. | Age | Sex | Clinical Information | Inci-denta-loma | Systolic BP | Location | Diagnosis (PAD) | P-met-tyramine (< 0.2) | NA | A | A/NARatio |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 21 | 60 | F | Back pain | Y | 145 | Para-aortic | PGL | 0.4 | 6.17 | 0.67 | 0.11 |
| 22 | 34 | F | Headache, palpitations | N | 220 | Pre-aortic | PGL | ND | 18.3 | 0.67 | 0.04 |
| 23 | 16 | M | Palpitations, headache, HT | N | 180 | Pre-aortic | PGL | ND | 1.67 | 2.00 | 1.20 |
| 24 | 71 | M | Abdominal pain | N | 130 | Pre-aortic | PGL | 1.1 | 0.50 | 0.67 | 1.33 |
| 25 | 56 | M | Abdominal pain | Y | 180 | Pre-aortic | PGL | 0.5 | 2.50 | 0.67 | 0.27 |
| 26 | 70 | M | Unclear symptoms | N | 135 | Neck | PGL | 0.8 | 2.33 | 0.67 | 0.29 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vyakaranam, A.R.; Crona, J.; Norlén, O.; Hellman, P.; Sundin, A. 11C-hydroxy-ephedrine-PET/CT in the Diagnosis of Pheochromocytoma and Paraganglioma. Cancers 2019, 11, 847. https://doi.org/10.3390/cancers11060847
Vyakaranam AR, Crona J, Norlén O, Hellman P, Sundin A. 11C-hydroxy-ephedrine-PET/CT in the Diagnosis of Pheochromocytoma and Paraganglioma. Cancers. 2019; 11(6):847. https://doi.org/10.3390/cancers11060847
Chicago/Turabian StyleVyakaranam, Achyut Ram, Joakim Crona, Olov Norlén, Per Hellman, and Anders Sundin. 2019. "11C-hydroxy-ephedrine-PET/CT in the Diagnosis of Pheochromocytoma and Paraganglioma" Cancers 11, no. 6: 847. https://doi.org/10.3390/cancers11060847
APA StyleVyakaranam, A. R., Crona, J., Norlén, O., Hellman, P., & Sundin, A. (2019). 11C-hydroxy-ephedrine-PET/CT in the Diagnosis of Pheochromocytoma and Paraganglioma. Cancers, 11(6), 847. https://doi.org/10.3390/cancers11060847