Current Treatment Landscape for Advanced Hepatocellular Carcinoma: Patient Outcomes and the Impact on Quality of Life



Abstract
1. Introduction
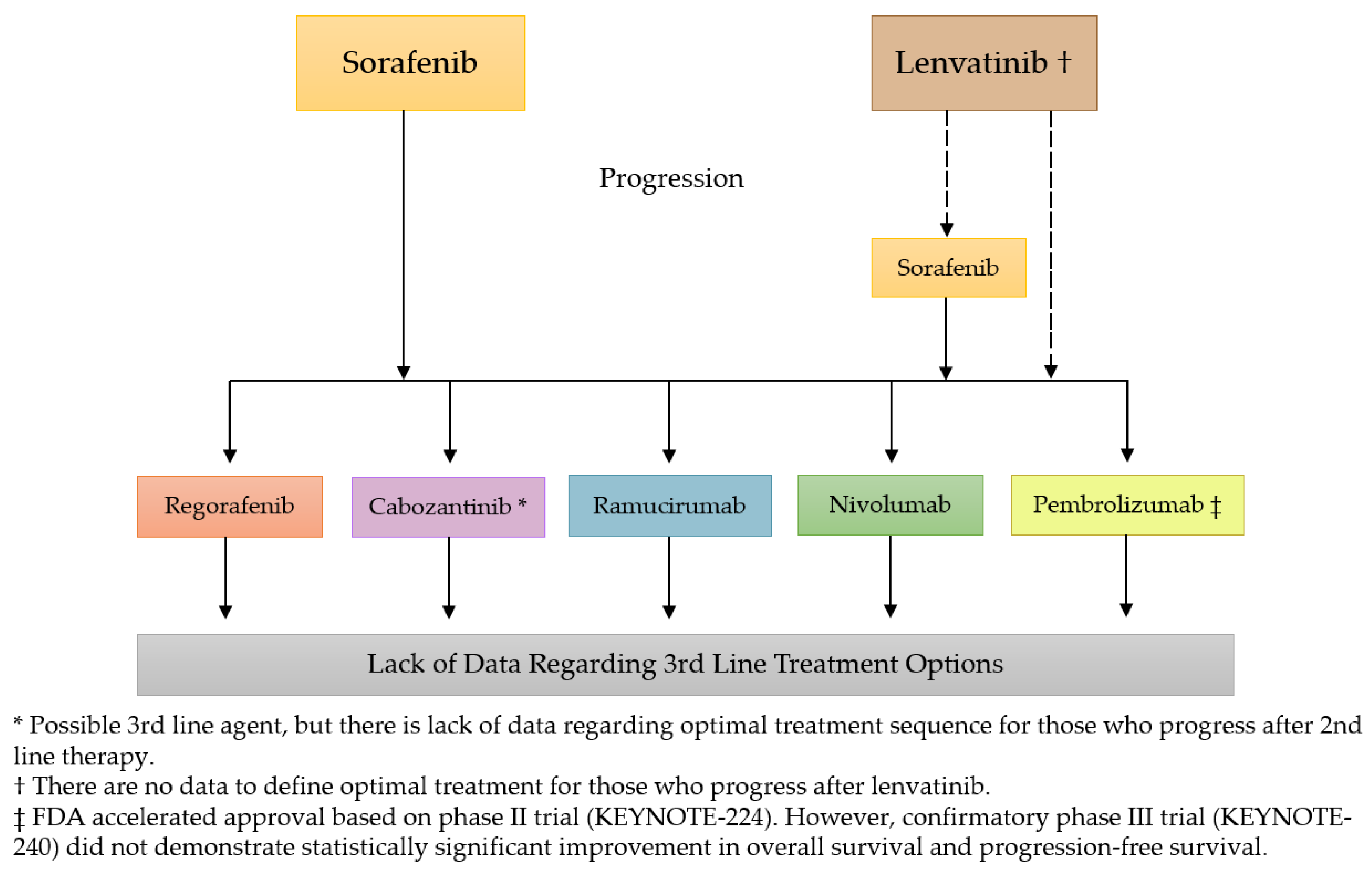
2. Current Treatment Landscape
2.1. Sorafenib
2.2. Lenvatinib
2.3. Regorafenib
2.4. Cabozantinib
2.5. Ramucirumab
2.6. Nivolumab
2.7. Pembrolizumab
3. Quality of Life
3.1. Assessments
3.2. Systemic Treatments
4. Current Challenges in the Treatment Landscape
5. Current and Future Research
6. Conclusions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, K.A.; London, W.T. The Global Epidemiology of Hepatocellular Carcinoma, Present and Future. Clin. Liver Dis. 2011, 15, 223–234. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Rudolph, K.L. Hepatocellular carcinoma: Epidemiology and molecular carcinogenesis. Gastroenterology 2007, 132, 2557–2576. [Google Scholar] [CrossRef]
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2016, 2, 16018. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; El-Serag, H.B. Epidemiology of HCC: Consider the Population. J. Clin. Gastroenterol. 2013, 47, S2–S6. [Google Scholar] [CrossRef] [PubMed]
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16, 1. [Google Scholar] [CrossRef]
- Knudsen, E.S.; Gopal, P.; Singal, A.G. The changing landscape of hepatocellular carcinoma: Etiology, genetics, and therapy. Am. J. Pathol. 2014, 184, 574–583. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Kanwal, F. Epidemiology of Hepatocellular Carcinoma in the United States: Where Are We? Where Do We Go? Hepatology 2014, 60, 1767–1775. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.; Maximin, S.; Meier, J.; Pokharel, S.; Bhargava, P. Hepatocellular Carcinoma: Review of Epidemiology, Screening, Imaging Diagnosis, Response Assessment, and Treatment. Curr. Probl. Diagn. Radiol. 2015, 44, 479–486. [Google Scholar] [CrossRef]
- Fitzmorris, P.; Shoreibah, M.; Anand, B.S.; Singal, A.K. Management of hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2015, 141, 861–876. [Google Scholar] [CrossRef]
- Boland, P.; Wu, J. Systemic therapy for hepatocellular carcinoma: Beyond sorafenib. Chin. Clin. Oncol. 2018, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Peck-Radosavljevic, M. Review article: Systemic treatment of hepatocellular carcinoma. Alimen. Pharmacol. Ther. 2018, 48, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Ingle, P.V.; Samsudin, S.Z.; Chan, P.Q.; Ng, M.K.; Heng, L.X.; Yap, S.C.; Chai, A.S.H.; Wong, A.S.Y. Development and novel therapeutics in hepatocellular carcinoma: A review. Ther. Clin. Risk Manag. 2016, 12, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Cancer Net. Liver Cancer: Statistics. Available online: https://www.cancer.net/cancer-types/liver-cancer/statistics (accessed on 13 March 2019).
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.-Y.; Choo, S.-P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Gill, J.; Baiceanu, A.; Clark, P.J.; Langford, A.; Latiff, J.; Yang, P.-M.; Yoshida, E.M.; Kanavos, P. Insights into the hepatocellular carcinoma patient journey: Results of the first global quality of life survey. Future Oncol. 2018, 14, 1701–1710. [Google Scholar] [CrossRef] [PubMed]
- Eatrides, J.; Wang, E.; Kothari, N.; Kim, R. Role of Systemic Therapy and Future Directions for Hepatocellular Carcinoma. Cancer Control 2017, 24, 1073274817729243. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Rich, N.E.; Yopp, A.C.; Singal, A.G. Medical Management of Hepatocellular Carcinoma. J. Oncol. Pract. 2017, 13, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Mathurin, P.; Rixe, O.; Carbonell, N.; Bernard, B.; Cluzel, P.; Bellin, M.F.; Khayat, D.; Opolon, P.; Poynard, T. Review article: Overview of medical treatments in unresectable hepatocellular carcinom—An impossible meta-analysis? Aliment. Pharmacol. Ther. 1998, 12, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Di Bisceglie, A.M.; Zhu, A.X.; Kramer, B.S.; Gores, G.J.; Talwalkar, J.; Bruix, J.; Llovet, J.M.; Lotze, M.; Sherman, M.; et al. Design and Endpoints of Clinical Trials in Hepatocellular Carcinoma. JNCI J. Natl. Cancer Inst. 2008, 100, 698–711. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Kudo, M.; Ye, S.L.; Bronowicki, J.P.; Chen, X.P.; Dagher, L.; Furuse, J.; Geschwind, J.F.; de Guevara, L.L.; Papandreou, C.; et al. GIDEON (Global Investigation of therapeutic DEcisions in hepatocellular carcinoma and of its treatment with sorafeNib): Second interim analysis. Int. J. Clin. Pract. 2014, 68, 609–617. [Google Scholar] [CrossRef]
- Bruix, J.; Raoul, J.L.; Sherman, M.; Mazzaferro, V.; Bolondi, L.; Craxi, A.; Galle, P.R.; Santoro, A.; Beaugrand, M.; Sangiovanni, A.; et al. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma: Subanalyses of a phase III trial. J. Hepatol. 2012, 57, 821–829. [Google Scholar] [CrossRef]
- Zhu, A.X.; Rosmorduc, O.; Evans, T.R.; Ross, P.J.; Santoro, A.; Carrilho, F.J.; Bruix, J.; Qin, S.; Thuluvath, P.J.; Llovet, J.M.; et al. SEARCH: A phase III, randomized, double-blind, placebo-controlled trial of sorafenib plus erlotinib in patients with advanced hepatocellular carcinoma. J. Clin. 2015, 33, 559–566. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Niedzwieski, D.; Knox, J.J.; Kaubisch, A.; Posey, J.; Tan, B.R.; Kavan, P.; Goel, R.; Murray, J.J.; Bekaii-Saab, T.S.; et al. Phase III randomized study of sorafenib plus doxorubicin versus sorafenib in patients with advanced hepatocellular carcinoma (HCC): CALGB 80802 (Alliance). J. Clin. Oncol. 2016, 34, 192. [Google Scholar] [CrossRef]
- Kudo, M.; Ueshima, K.; Yokosuka, O.; Ogasawara, S.; Obi, S.; Izumi, N.; Aikata, H.; Nagano, H.; Hatano, E.; Sasaki, Y.; et al. Sorafenib plus low-dose cisplatin and fluorouracil hepatic arterial infusion chemotherapy versus sorafenib alone in patients with advanced hepatocellular carcinoma (SILIUS): A randomised, open label, phase 3 trial. Lancet Gastroenterol. Hepatol. 2018, 3, 424–432. [Google Scholar] [CrossRef]
- Group, T.S.T.; Sibert, A.; Ronot, M.; Bouattour, M.; Lebtahi, R.; Allaham, W.; Castera, L.; Vilgrain, V.; Sarran, A.; Brenot-Rossi, I.; et al. Efficacy, tolerability and impact on quality of life of selective internal radiation therapy (with yttrium-90 resin microspheres) or sorafenib in patients with locally advanced hepatocellular carcinoma: The SARAH trial. Ann. Oncol. 2017, 28. [Google Scholar] [CrossRef]
- Gandhi, M.; Choo, S.P.; Thng, C.H.; Tan, S.B.; Low, A.S.C.; Cheow, P.C.; Goh, A.S.W.; Tay, K.H.; Lo, R.H.G.; Goh, B.K.P.; et al. Single administration of Selective Internal Radiation Therapy versus continuous treatment with sorafeNIB in locally advanced hepatocellular carcinoma (SIRveNIB): Study protocol for a phase iii randomized controlled trial. BMC Cancer 2016, 16, 856. [Google Scholar] [CrossRef] [PubMed]
- Tovoli, F.; Negrini, G.; Benevento, F.; Faggiano, C.; Goio, E.; Granito, A. Systemic treatments for hepatocellular carcinoma: Challenges and future perspectives. Hepat. Oncol. 2018, 5, HEP01. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Qin, S.; Park, J.W.; Poon, R.T.; Raoul, J.L.; Philip, P.A.; Hsu, C.H.; Hu, T.H.; Heo, J.; Xu, J.; et al. Brivanib versus sorafenib as first-line therapy in patients with unresectable, advanced hepatocellular carcinoma: Results from the randomized phase III BRISK-FL study. J. Clin. Oncol. 2013, 31, 3517–3524. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Kang, Y.K.; Lin, D.Y.; Park, J.W.; Kudo, M.; Qin, S.; Chung, H.C.; Song, X.; Xu, J.; Poggi, G.; et al. Sunitinib versus sorafenib in advanced hepatocellular cancer: Results of a randomized phase III trial. J. Clin. Oncol. 2013, 31, 4067–4075. [Google Scholar] [CrossRef]
- Cainap, C.; Qin, S.; Huang, W.T.; Chung, I.J.; Pan, H.; Cheng, Y.; Kudo, M.; Kang, Y.K.; Chen, P.J.; Toh, H.C.; et al. Linifanib versus Sorafenib in patients with advanced hepatocellular carcinoma: Results of a randomized phase III trial. J. Clin. Oncol. 2015, 33, 172–179. [Google Scholar] [CrossRef]
- Chow, P.K.H.; Gandhi, M.; Tan, S.B.; Khin, M.W.; Khasbazar, A.; Ong, J.; Choo, S.P.; Cheow, P.C.; Chotipanich, C.; Lim, K.; et al. SIRveNIB: Selective Internal Radiation Therapy Versus Sorafenib in Asia-Pacific Patients with Hepatocellular Carcinoma. J. Clin. Oncol. 2018, 36, 1913–1921. [Google Scholar] [CrossRef]
- Matsuki, M.; Hoshi, T.; Yamamoto, Y.; Ikemori-Kawada, M.; Minoshima, Y.; Funahashi, Y.; Matsui, J. Lenvatinib inhibits angiogenesis and tumor fibroblast growth factor signaling pathways in human hepatocellular carcinoma models. Cancer Med. 2018, 7, 2641–2653. [Google Scholar] [CrossRef]
- Wang, X.W.; Thorgeirsson, S.S. The biological and clinical challenge of liver cancer heterogeneity. Hepat. Oncol. 2014, 1, 349–353. [Google Scholar] [CrossRef]
- Cochin, V.; Gross-Goupil, M.; Ravaud, A.; Godbert, Y.; Le Moulec, S. Cabozantinib: Mechanism of action, efficacy and indications. Bull. Cancer 2017, 104, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Poon, R.; Pastorelli, D.; Blanc, J.-F.; Chung, H.C.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.-K.; Yen, C.-J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Lim, H.Y.; Pracht, M.; et al. REACH-2: A randomized, double-blind, placebo-controlled phase 3 study of ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma (HCC) and elevated baseline alpha-fetoprotein (AFP) following first-line sorafenib. J. Clin. Oncol. 2018, 36, 4003. [Google Scholar] [CrossRef]
- Finn, R.S.; Ryoo, B.-Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.-Y.; Breder, V.V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Results of KEYNOTE-240: Phase 3 study of pembrolizumab (Pembro) vs. best supportive care (BSC) for second line therapy in advanced hepatocellular carcinoma (HCC). J. Clin. Oncol. 2019, 37, 4004. [Google Scholar] [CrossRef]
- Gandhi, S.; Khubchandani, S.; Iyer, R. Quality of life and hepatocellular carcinoma. J. Gastrointest. Oncol. 2014, 5, 296–317. [Google Scholar] [CrossRef] [PubMed]
- Padmaja, G.; Vanlalhruaii, C.; Rana, S.; Tiamongla; Kopparty, S. Quality of Life of Patients with Cancer: A Determinant of the Quality of Life of Their Family Caregivers. J. Cancer Educ. 2017, 32, 655–661. [Google Scholar] [CrossRef]
- Blazeby, J.M.; Currie, E.; Zee, B.C.; Chie, W.C.; Poon, R.T.; Garden, O.J. Development of a questionnaire module to supplement the EORTC QLQ-C30 to assess quality of life in patients with hepatocellular carcinoma, the EORTC QLQ-HCC18. Eur. J. Cancer 2004, 40, 2439–2444. [Google Scholar] [CrossRef]
- Bonnetain, F.; Paoletti, X.; Collette, S.; Doffoel, M.; Bouché, O.; Raoul, J.L.; Rougier, P.; Masskouri, F.; Barbare, J.C.; Bedenne, L. Quality of life as a prognostic factor of overall survival in patients with advanced hepatocellular carcinoma: Results from two French clinical trials. Qual. Life Res. 2008, 17, 831. [Google Scholar] [CrossRef] [PubMed]
- Brunocilla, P.R.; Brunello, F.; Carucci, P.; Gaia, S.; Rolle, E.; Cantamessa, A.; Castiglione, A.; Ciccone, G.; Rizzetto, M. Sorafenib in hepatocellular carcinoma: Prospective study on adverse events, quality of life, and related feasibility under daily conditions. Med. Oncol. 2013, 30, 345. [Google Scholar] [CrossRef] [PubMed]
- Carr, B.I.; Cella, D.; Eton, D.T.; Steel, J.L.; Olek, M.C. Clinically meaningful changes in health-related quality of life in patients diagnosed with hepatobiliary carcinoma. Ann. Oncol. 2005, 17, 304–312. [Google Scholar] [CrossRef]
- Chie, W.-C.; Yu, F.; Li, M.; Baccaglini, L.; Blazeby, J.M.; Hsiao, C.-F.; Chiu, H.-C.; Poon, R.T.; Mikoshiba, N.; Al-Kadhimi, G.; et al. Quality of life changes in patients undergoing treatment for hepatocellular carcinoma. Qual. Life Res. 2015, 24, 2499–2506. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, N.; Cella, D.; Webster, K.; Odom, L.; Martone, M.; Passik, S.; Bookbinder, M.; Fong, Y.; Jarnagin, W.; Blumgart, L. Measuring health-related quality of life in patients with hepatobiliary cancers: The functional assessment of cancer therapy-hepatobiliary questionnaire. J. Clin. Oncol. 2002, 20, 2229–2239. [Google Scholar] [CrossRef] [PubMed]
- Chie, W.C.; Blazeby, J.M.; Hsiao, C.F.; Chiu, H.C.; Poon, R.T.; Mikoshiba, N.; Al-Kadhimi, G.; Heaton, N.; Calara, J.; Collins, P.; et al. International cross-cultural field validation of an European Organization for Research and Treatment of Cancer questionnaire module for patients with primary liver cancer, the European Organization for Research and Treatment of Cancer quality-of-life questionnaire HCC18. Hepatology 2012, 55, 1122–1129. [Google Scholar] [CrossRef]
- Tanabe, G.; Ueno, S.; Maemura, M.; Kihara, K.; Aoki, D.; Yoshidome, S.; Ogura, Y.; Hamanoue, M.; Aikou, T. Favorable quality of life after repeat hepatic resection for recurrent hepatocellular carcinoma. Hepato-Gastroenterology 2001, 48, 506–510. [Google Scholar]
- Huang, G.; Chen, X.; Lau, W.Y.; Shen, F.; Wang, R.-Y.; Yuan, S.-X.; Geng, W.-X.; Zhou, W.-P. Quality of life after surgical resection compared with radiofrequency ablation for small hepatocellular carcinomas. Br. J. Surg. 2014, 101, 1006–1015. [Google Scholar] [CrossRef]
- Lee, L.J.-H.; Chen, C.-H.; Yao, G.; Chung, C.-W.; Sheu, J.-C.; Lee, P.-H.; Tsai, Y.-J.; Wang, J.-D. Quality of life in patients with hepatocellular carcinoma received surgical resection. J. Surg. Oncol. 2007, 95, 34–39. [Google Scholar] [CrossRef]
- Chiu, C.-C.; Lee, K.-T.; Wang, J.-J.; Sun, D.-P.; Lee, H.-H.; Shi, H.-Y. Health-Related Quality of Life before and after Surgical Resection of Hepatocellular Carcinoma: A Prospective Study. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 65–72. [Google Scholar] [CrossRef]
- Mise, Y.; Satou, S.; Ishizawa, T.; Kaneko, J.; Aoki, T.; Hasegawa, K.; Sugawara, Y.; Makuuchi, M.; Kokudo, N. Impact of Surgery on Quality of Life in Patients with Hepatocellular Carcinoma. World J. Surg. 2014, 38, 958–967. [Google Scholar] [CrossRef]
- He, Q.; Jiang, J.J.; Jiang, Y.X.; Wang, W.T.; Yang, L. Health-Related Quality of Life Comparisons After Radical Therapy for Early-Stage Hepatocellular Carcinoma. Transpl. Proc. 2018, 50, 1470–1474. [Google Scholar] [CrossRef]
- Lei, J.Y.; Yan, L.N.; Wang, W.T.; Zhu, J.Q.; Li, D.J. Health-Related Quality of Life and Psychological Distress in Patients with Early-Stage Hepatocellular Carcinoma After Hepatic Resection or Transplantation. Transpl. Proc. 2016, 48, 2107–2111. [Google Scholar] [CrossRef] [PubMed]
- Poon, R.T.-P.; Fan, S.T.; Yu, W.C.; Lam, B.K.-Y.; Chan, F.Y.-S.; Wong, J. A Prospective Longitudinal Study of Quality of Life After Resection of Hepatocellular Carcinoma. Arch. Surg. 2001, 136, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Toro, A.; Pulvirenti, E.; Palermo, F.; Di Carlo, I. Health-related quality of life in patients with hepatocellular carcinoma after hepatic resection, transcatheter arterial chemoembolization, radiofrequency ablation or no treatment. Surg. Oncol. 2012, 21, e23–e30. [Google Scholar] [CrossRef] [PubMed]
- Hinrichs, J.B.; Hasdemir, D.B.; Nordlohne, M.; Schweitzer, N.; Wacker, F.; Vogel, A.; Kirstein, M.M.; Marquardt, S.; Rodt, T. Health-Related Quality of Life in Patients with Hepatocellular Carcinoma Treated with Initial Transarterial Chemoembolization. Cardiovasc. Intervent. Radiol. 2017, 40, 1559–1566. [Google Scholar] [CrossRef] [PubMed]
- Hartrumpf, K.J.; Marquardt, S.; Werncke, T.; Murray, T.; Kirstein, M.M.; Vogel, A.; Wacker, F.; Rodt, T. Quality of life in patients undergoing repetitive TACE for the treatment of intermediate stage HCC. J. Cancer Res. Clin. Oncol. 2018, 144, 1991–1999. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-B.; Chen, M.-H.; Yan, K.; Yang, W.; Dai, Y.; Yin, S.-S. Quality of life after radiofrequency ablation combined with transcatheter arterial chemoembolization for hepatocellular carcinoma: Comparison with transcatheter arterial chemoembolization alone. Qual. Life Res. 2006, 16, 389. [Google Scholar] [CrossRef] [PubMed]
- Shomura, M.; Kagawa, T.; Okabe, H.; Shiraishi, K.; Hirose, S.; Arase, Y.; Tsuruya, K.; Takahira, S.; Mine, T. Longitudinal alterations in health-related quality of life and its impact on the clinical course of patients with advanced hepatocellular carcinoma receiving sorafenib treatment. BMC Cancer 2016, 16, 878. [Google Scholar] [CrossRef] [PubMed]
- Chau, I.; Peck-Radosavljevic, M.; Borg, C.; Malfertheiner, P.; Seitz, J.F.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Kudo, M.; Poon, R.; et al. Ramucirumab as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib: Patient-focused outcome results from the randomised phase III REACH study. Eur. J. Cancer 2017, 81, 17–25. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Mollon, P.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Kelley, R.K.; Baron, A.D.; Benzaghou, F.; Valcheva, V.V.; Hazra, S.; et al. Quality-adjusted life years assessment using cabozantinib for patients with advanced hepatocellular carcinoma (aHCC) in the CELESTIAL trial. J. Clin. Oncol. 2019, 37, 207. [Google Scholar] [CrossRef]
- Galle, P.R.; Tovoli, F.; Foerster, F.; Worns, M.A.; Cucchetti, A.; Bolondi, L. The treatment of intermediate stage tumours beyond TACE: From surgery to systemic therapy. J. Hepatol. 2017, 67, 173–183. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K. Ramucirumab and the controversial role of alpha-fetoprotein in hepatocellular carcinoma. Lancet Oncol. 2019, 20, 177–179. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Kudo, M. Ramucirumab in advanced hepatocellular carcinoma in REACH-2: The true value of alpha-fetoprotein. Lancet Oncol. 2019, 20, e191. [Google Scholar] [CrossRef]
- Merck Co. Merck Provides Update on KEYNOTE-240, a Phase 3 Study of KEYTRUDA® (Pembrolizumab) in Previously Treated Patients with Advanced Hepatocellular Carcinoma. Available online: https://investors.merck.com/news/press-release-details/2019/Merck-Provides-Update-on-KEYNOTE-240-a-Phase-3-Study-of-KEYTRUDA-pembrolizumab-in-Previously-Treated-Patients-with-Advanced-Hepatocellular-Carcinoma/default.aspx (accessed on 13 March 2019).
- Li, L.; Mo, F.K.; Chan, S.L.; Hui, E.P.; Tang, N.S.; Koh, J.; Leung, L.K.; Poon, A.N.; Hui, J.; Chu, C.M.; et al. Prognostic values of EORTC QLQ-C30 and QLQ-HCC18 index-scores in patients with hepatocellular carcinoma—clinical application of health-related quality-of-life data. BMC Cancer 2017, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Butt, Z.; Kindler, H.L.; Fuchs, C.S.; Bray, S.; Barlev, A.; Oglesby, A. Validity of the FACT Hepatobiliary (FACT-Hep) questionnaire for assessing disease-related symptoms and health-related quality of life in patients with metastatic pancreatic cancer. Qual. Life Res. 2013, 22, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Park, J.-W.; Cruz, C.M.D.; Anderson, J.; Lang, L.; Neely, J.; Shaw, J.W.; Cheng, A.-L. A randomized, multicenter, phase 3 study of nivolumab vs. sorafenib as first-line treatment in patients (pts) with advanced hepatocellular carcinoma (HCC): CheckMate-459. J. Clin. Oncol. 2016, 34, TPS4147. [Google Scholar] [CrossRef]
- Fan, Y.; Xu, B.; Ding, X.; Ma, F.; Wang, J.; Yuan, P.; Li, Q.; Zhang, P.; Meng, K.; Wang, Z.; et al. Icaritin efficacy and tolerability in advanced hepatocellular carcinoma: Final phase Ib result. J. Clin. Oncol. 2014, 32, e15107. [Google Scholar] [CrossRef]
- Finn, R.S.; Ducreux, M.; Qin, S.; Galle, P.R.; Zhu, A.X.; Ikeda, M.; Kim, T.-Y.; Xu, D.-Z.; Verret, W.; Liu, J.; et al. IMbrave150: A randomized phase III study of 1L atezolizumab plus bevacizumab vs. sorafenib in locally advanced or metastatic hepatocellular carcinoma. J. Clin. Oncol. 2018, 36, TPS4141. [Google Scholar] [CrossRef]
- Barker, H.E.; Paget, J.T.; Khan, A.A.; Harrington, K.J. The tumour microenvironment after radiotherapy: Mechanisms of resistance and recurrence. Nat. Rev. Cancer 2015, 15, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.W.Y.; Tai, D.W.-M.; Koo, S.-L.; Ng, M.C.; Yeong, J.P.S.; Zhai, W.W.; Newell, E.; Chow, P.K.H.; Lim, K.H.; Gogna, A.; et al. A phase II open-label, single-centre, non-randomized trial of Y90 transarterial radioembolization in combination with nivolumab in Asian patients with intermediate stage hepatocellular carcinoma: An immunological study of radioembolization in combination with anti-PD1 therapy in HCC. J. Clin. Oncol. 2018, 36, TPS542. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Chan, S.L.; Furuse, J.; Galle, P.R.; Kelley, R.K.; Qin, S.; Armstrong, J.; Darilay, A.; Vlahovic, G.; Negro, A.; et al. A randomized, multicenter phase 3 study of durvalumab (D) and tremelimumab (T) as first-line treatment in patients with unresectable hepatocellular carcinoma (HCC): HIMALAYA study. J. Clin. Oncol. 2018, 36, TPS4144. [Google Scholar] [CrossRef]


{kind=link}
| Study Name | Design | Met Primary Endpoint(s) | Patients (n) | TTP/PFS (Months) | mOS (Months) |
|---|---|---|---|---|---|
| 1st Line Setting | |||||
| SHARP | Sorafenib vs. placebo | Yes | Sorafenib (299) Placebo (303) | 5.5 vs. 2.8 HR = 0.58 95% CI: 0.45–0.74 p < 0.001 | 10.7 vs. 7.9 HR = 0.69 95% CI: 0.55–0.87 p < 0.001 |
| Asian-Pacific | Sorafenib vs. placebo | Yes | Sorafenib (150) Placebo (76) | 2.8 vs. 1.4 HR = 0.57 95% CI: 0.42–0.79 p < 0.001 | 6.5 vs. 4.2 HR = 0.68 95% CI: 0.50–0.93 p = 0.014 |
| SUN1170 | Sunitinib vs. sorafenib | No | Sunitinib (530) Sorafenib (544) | 4.1 vs. 3.8 HR = 1.13 95% CI: 0.98–1.31 p = 0.308 | 7.9 vs. 10.2 HR = 1.30 95% CI: 1.13–1.50 p = 0.001 |
| BRISK-FL | Brivanib vs. sorafenib | No | Brivanib (577) Sorafenib (578) | 4.2 vs. 4.1 HR = 1.01 95% CI: 0.88–1.16 p = 0.853 | 9.5 vs. 9.9 HR = 1.06 95% CI: 0.93–1.22 p = 0.373 |
| LIGHT | Linifanib vs. sorafenib | No | Linifanib (514) Sorafenib (521) | 5.4 vs. 4.0 HR = 0.76 95% CI: 0.64–0.90 p = 0.001 | 9.1 vs. 9.8 HR = 1.04 95% CI: 0.90–1.22 p = NS |
| SEARCH | Sorafenib +/− erlotinib | No | Sorafenib + Erlotinib (362) Sorafenib + placebo (358) | 3.2 vs. 4.0 HR = 1.135 95% CI: 0.94–1.37 p = 0.180 | 9.5 vs. 8.5 HR = 0.929 95% CI: 0.78–1.11 p = 0.408 |
| CALGB80802 | Sorafenib +/− doxorubicin | No | Sorafenib + Doxorubicin (180) Sorafenib + Placebo (176) | 3.6 vs. 3.2 * HR = 0.90 95% CI: 0.72–1.20 p = NS | 9.3 vs. 10.5 HR = 1.06 95% CI: 0.80–1.40 p = NS |
| REFLECT | Lenvatinib vs. sorafenib | Yes | Lenvatinib (478) Sorafenib (476) | 8.9 vs. 3.7 HR = 0.63 95% CI: 0.53–0.73 p < 0.0001 | 13.6 vs. 12.3 HR = 0.92 95% CI: 0.79–1.06 p = NS |
| SARAH | Y90 vs. sorafenib | No | Y90 (237) Sorafenib (222) | 4.1 vs. 3.7 * HR = 1.03 95% CI: 0.85–1.25 p = 0.760 | 8.0 vs. 9.9 HR = 1.15 95% CI: 0.94–1.14 p = 0.180 |
| SIRveNIB | Y90 vs. sorafenib | No | Y90 (182) Sorafenib (178) | 6.1 vs. 5.4 HR = 0.88 95% CI: 0.70–1.10 p = 0.290 | 8.8 vs. 10.0 HR = 1.10 95% CI: 0.90–1.40 p = 0.360 |
| Study Name | Design | Met Primary Endpoint(s) | Patients (n) | TTP/PFS (months) | mOS (months) |
|---|---|---|---|---|---|
| 2nd Line Setting | |||||
| RESORCE | Regorafenib vs. placebo | Yes | Regorafenib (379) Placebo (194) | 3.2 vs. 1.5 HR = 0.44 95% CI: 0.36–0.55 p < 0.0001 | 10.6 vs. 7.8 HR = 0.63 95% CI: 0.50–0.79 p < 0.0001 |
| CELESTIAL | Cabozantinib vs. placebo | Yes | Cabozantinib (470) Placebo (237) | 5.2 vs. 1.9 * HR = 0.44 95% CI: 0.36–0.52 p < 0.001 | 10.2 vs. 8.0 HR = 0.76 95% CI: 0.63–0.92 p = 0.005 |
| REACH-2 | Ramucirumab vs. placebo | Yes | Ramucirumab (197) Placebo (95) | 3.0 vs. 1.6 HR = 0.43 95% CI: 0.31–0.58 p < 0.0001 | 8.5 vs. 7.3 HR = 0.71 95% CI: 0.53–0.94 p = 0.020 |
| CheckMate 040 | Nivolumab phase I/II | Yes | Dose-escalation (48) Dose-expansion (214) | Dose-escalation: 3.4 Dose-expansion: 4.1 | Dose-escalation: 15.0 Dose-expansion: NR |
| KEYNOTE-224 | Pembrolizumab phase II | Yes | Pembrolizumab (104) | 4.9 95% CI: 3.9–8.0 | 12.9 95% CI: 9.7–15.5 |
| KEYNOTE-240 | Pembrolizumab vs. placebo | No | Not provided | Not provided HR = 0.78 95% CI: 0.61–0.99 p = 0.021 | Not provided HR = 0.78 95% CI: 0.61–1.00 p = 0.024 |
| Agent | Study Type | No. of Patients | HRQoL Assessment Tool | Scale(s)/Domain(s) | Outcome |
|---|---|---|---|---|---|
| Sorafenib | Prospective | 36 | FACT-Hep | Physical well-being | Score decrease was detected from baseline to week 1, with a median reduction of −8.3 (range: −60.1 to −17.9; p = 0.0003) |
| Sorafenib | Prospective | 54 | SF-36 (Japanese Version) | All domains | Scores >40 maintained over a 1-year period (n = 13) |
| Physical functioning | Baseline scores ≥40 significantly associated with longer overall survival (p = 0.053) | ||||
| Social functioning | Baseline scores ≥40 associated with longer treatment duration (p = 0.016) | ||||
| Lenvatinib | Phase III Trial | 954 | EORTC QLQ-C30, EORTC QLQ-HCC18 | EORTC QLQ-C30: role functioning, pain, and diarrhea EORTC QLQ-HCC18: nutrition and body image | Clinically meaningful deterioration observed later in lenvatinib compared to sorafenib |
| EORTC QLQ-C30 summary score | No significant difference between lenvatinib and sorafenib (HR = 0.87, 95% CI: 0.75–1.01) | ||||
| Regorafenib | Phase III Trial | 573 | FACT-G, HACT-Hep, EQ-5D, EQ-VAS | All scales and domains | No clinically meaningful differences between regorafenib and placebo |
| Ramucirumab | Subanalysis | 565 | FACT Hepatobiliary Symptom Index (FHSI)-8, EuroQoL (EQ-5D) | All scales and domains | No significant treatment differences |
| FHSI-8 | Subpopulation of patients with baseline AFP ≥400ng/mL had significantly reduced deterioration at the end of treatment compared with placebo (p = 0.038) | ||||
| Cabozantinib | Subanalysis | 707 | EQ-5D-5L | Quality-adjusted life years (QALY) | Mean accrued QALYs with cabozantinib was +0.115 vs. placebo (95% CI: 0.032 to 0.198; p = 0.007) |
| Nivolumab | Phase I/II Trial | 262 | EQ-5D-3L, EQ-5D-VAS | All scales and domains | Stable patient-reported outcomes despite previous treatment with sorafenib |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Sedano, S.; Allen, R.; Gong, J.; Cho, M.; Sharma, S. Current Treatment Landscape for Advanced Hepatocellular Carcinoma: Patient Outcomes and the Impact on Quality of Life. Cancers 2019, 11, 841. https://doi.org/10.3390/cancers11060841
Li D, Sedano S, Allen R, Gong J, Cho M, Sharma S. Current Treatment Landscape for Advanced Hepatocellular Carcinoma: Patient Outcomes and the Impact on Quality of Life. Cancers. 2019; 11(6):841. https://doi.org/10.3390/cancers11060841
Chicago/Turabian StyleLi, Daneng, Sabrina Sedano, Rebecca Allen, Jun Gong, May Cho, and Sunil Sharma. 2019. "Current Treatment Landscape for Advanced Hepatocellular Carcinoma: Patient Outcomes and the Impact on Quality of Life" Cancers 11, no. 6: 841. https://doi.org/10.3390/cancers11060841
APA StyleLi, D., Sedano, S., Allen, R., Gong, J., Cho, M., & Sharma, S. (2019). Current Treatment Landscape for Advanced Hepatocellular Carcinoma: Patient Outcomes and the Impact on Quality of Life. Cancers, 11(6), 841. https://doi.org/10.3390/cancers11060841