Changes in Ultraviolet Radiation Exposure to the Ocular Region: A Population-Based Study

 ,
, 
Abstract
1. Introduction
2. Results
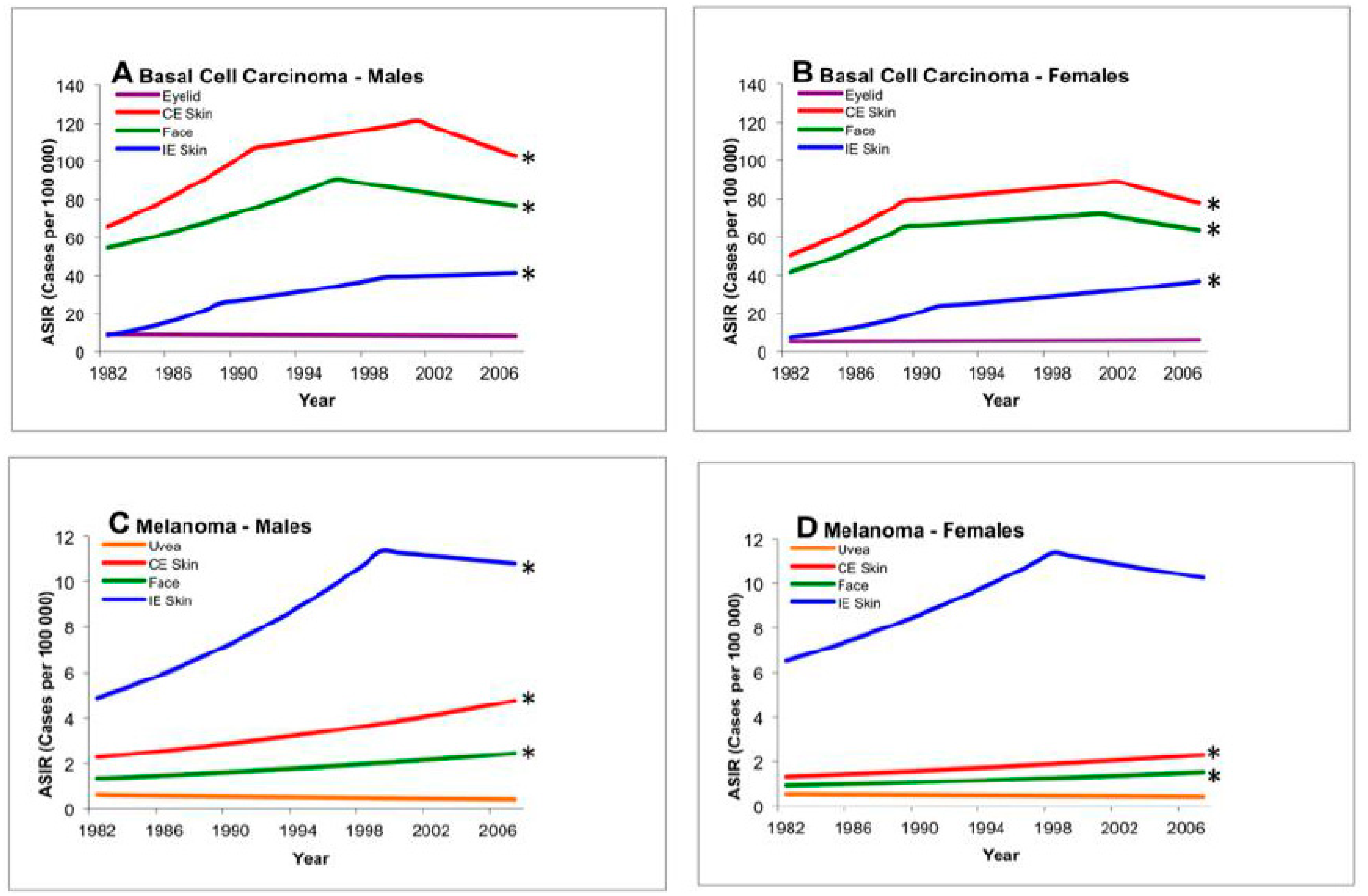
2.1. Age-Standardized Incidence Rates
2.2. Incidence Trends
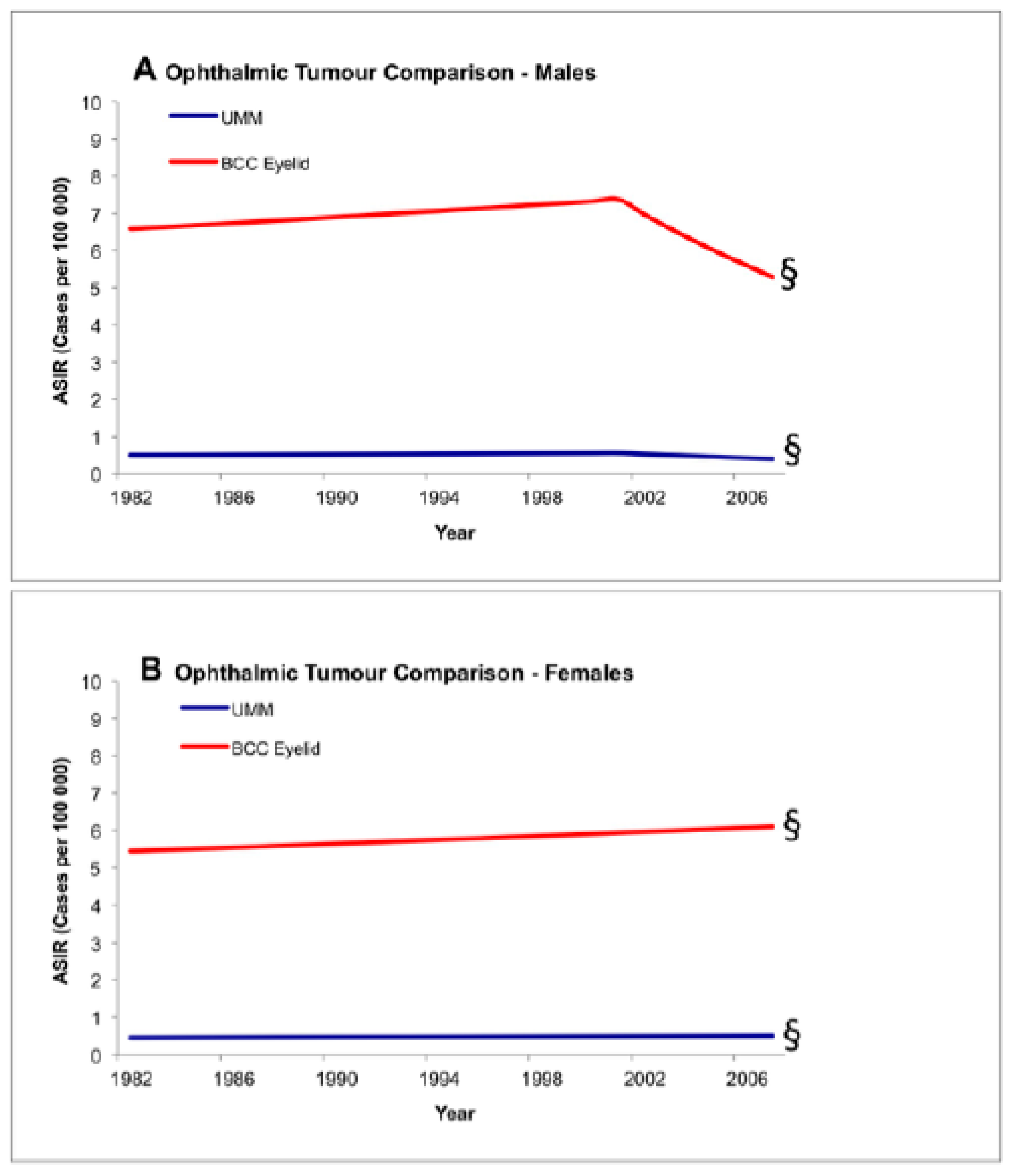
2.3. Comparability Test
3. Discussion
4. Materials and Methods
4.1. The Alberta Cancer Registry
4.2. Data Selection and Age Standardization
4.3. Joinpoint and the Comparability Test for Differences between Groups
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gamel, J.W.; McLean, I.W.; McCurdy, J.B. Biologic distinctions between cure and time to death in 2892 patients with intraocular melanoma. Cancer 1993, 71, 2299–2305. [Google Scholar] [CrossRef]
- Kujala, E.; Makitie, T.; Kivela, T. Very long-term prognosis of patients with malignant uveal melanoma. Invest. Ophthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.E.; Karnell, L.H.; Menck, H.R. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: A Summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer 1998, 83, 1664–1678. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L. Uveal melanoma: Relatively rare but deadly cancer. Eye 2017, 31, 241–257. [Google Scholar] [CrossRef]
- Shields, J.A.; Shields, C.L. Posterior Uveal Melanoma: Management. In Intraocular Tumors: An. Atlas and Textbook. Rev.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1999; pp. 140–175. [Google Scholar]
- Singh, A.D.; Bergman, L.; Seregard, S. Uveal melanoma: Epidemiologic aspects. Ophthalmol. Clin. N. Am. 2005, 18, 75–84. [Google Scholar] [CrossRef]
- National Institutes of Health Summary of the Consensus Development Conference on Sunlight, Ultraviolet Radiation, and the Skin. Bethesda, Maryland, May 8–10, 1989. Consensus Development Panel. J. Am. Acad. Dermatol. 1991, 24, 608–612.
- IARC monographs on the evaluation of carcinogenic risks to humans. Solar and ultraviolet radiation. IARC Monogr. Eval. Carcinog. Risks Hum. 1992, 55, 1–316.
- Gilchrest, B.A.; Eller, M.S.; Geller, A.C.; Yaar, M. The pathogenesis of melanoma induced by ultraviolet radiation. N. Engl. J. Med. 1999, 340, 1341–1348. [Google Scholar] [CrossRef]
- Leiter, U.; Garbe, C. Epidemiology of melanoma and nonmelanoma skin cancer—The role of sunlight. Adv. Exp. Med. Biol. 2008, 624, 89–103. [Google Scholar]
- Inskip, P.D.; Devesa, S.S.; Fraumeni, J.F., Jr. Trends in the incidence of ocular melanoma in the United States, 1974–1998. Cancer Causes Control 2003, 14, 251–257. [Google Scholar]
- Isager, P.; Osterlind, A.; Engholm, G.; Heegaard, S.; Lindegaard, J.; Overgaard, J.; Storm, H.H. Uveal and conjunctival malignant melanoma in Denmark, 1943–1997: Incidence and validation study. Ophthalmic Epidemiol. 2005, 12, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Rennie, I.G.; Seregard, S.; Giblin, M.; McKenzie, J. Sunlight exposure and pathogenesis of uveal melanoma. Surv. Ophthalmol. 2004, 49, 419–428. [Google Scholar] [CrossRef]
- Swerdlow, A.J. Epidemiology of Chronic Disease Risks in Relations to Ultraviolet Radiation Exposure. Radiat. Prot. Dosimet. 2000, 91, 19–23. [Google Scholar] [CrossRef]
- Young, T.A.; Seddon, J.M. Choroidal and cutaneous melanoma: Distinctly different cousins. Ophthalmic Epidemiol. 2005, 12, 221–222. [Google Scholar] [CrossRef]
- Shah, C.P.; Weis, E.; Lajous, M.; Shields, J.A.; Shields, C.L. Intermittent and chronic ultraviolet light exposure and uveal melanoma: A meta-analysis. Ophthalmology 2005, 112, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Weis, E.; Shah, C.P.; Lajous, M.; Shields, J.A.; Shields, C.L. The association between host susceptibility factors and uveal melanoma: A meta-analysis. Arch. Ophthalmol. 2006, 124, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Weis, E.; Shah, C.P.; Lajous, M.; Shields, J.A.; Shields, C.L. The association of cutaneous and iris nevi with uveal melanoma: A meta-analysis. Ophthalmology 2009, 116, 536–543.e2. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risk to Humans. Radiation. Lyon (FR): International Agency for Research on Cancer; 2012. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 100D.) SOLAR AND ULTRAVIOLET RADIATION. Available online: https://www-ncbi-nlm-nih-gov.ezproxy.lib.ucalgary.ca/books/NBK304366/ (accessed on 1 May 2019).
- Welding, I.A.R.C. Molybdenum Trioxide, and Indium Tin Oxide. IARC Monogr. Eval. Carcinog. Risks Hum. 2018, 118, 36–265. [Google Scholar]
- Yam, J.C.; Kwok, A.K. Ultraviolet light and ocular diseases. Int. Ophthalmol. 2014, 34, 383–400. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Abeni, D.; Boyle, P.; Melchi, C.F. Meta-analysis of risk factors for cutaneous melanoma: I. Common and atypical naevi. Eur. J. Cancer 2005, 41, 28–44. [Google Scholar] [CrossRef]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Picconi, O.; Boyle, P.; Melchi, C.F. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur. J. Cancer 2005, 41, 45–60. [Google Scholar] [CrossRef]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Zanetti, R.; Masini, C.; Melchi, C.F. Meta-analysis of risk factors for cutaneous melanoma: III. Family history, actinic damage and phenotypic factors. Eur. J. Cancer 2005, 41, 2040–2059. [Google Scholar] [CrossRef] [PubMed]
- Cress, R.D.; Holly, E.A. Incidence of cutaneous melanoma among non-Hispanic whites, Hispanics, Asians, and blacks: An analysis of California cancer registry data, 1988–1993. Cancer Causes Control 1997, 8, 246–252. [Google Scholar] [CrossRef]
- Glickman, R.D. Ultraviolet phototoxicity to the retina. Eye Contact Lens 2011, 37, 196–205. [Google Scholar] [CrossRef]
- Johansson, P.; Aoude, L.G.; Wadt, K.; Glasson, W.J.; Warrier, S.K.; Hewitt, A.W.; Ingvar, C. Deep sequencing of uveal melanoma identifies a recurrent mutation in PLCB4. Oncotarget 2016, 7, 4624. [Google Scholar] [CrossRef]
- Rivolta, C.; Royer-Bertrand, B.; Rimoldi, D.; Schalenbourg, A.; Zografos, L.; Leyvraz, S.; Moulin, A. UV light signature in conjunctival melanoma; not only skin should be protected from solar radiation. J. Hum. Genet. 2016, 61, 361–362. [Google Scholar] [CrossRef] [PubMed]
- Royer-Bertrand, B.; Torsello, M.; Rimoldi, D.; El Zaoui, I.; Cisarova, K.; Pescini-Gobert, R.; Raynaud, F.; Zografos, L.; Schalenbourg, A.; Speiser, D.; et al. Comprehensive genetic landscape of uveal melanoma by whole-genome sequencing. Am. J. Hum. Genet. 2016, 99, 1190–1198. [Google Scholar] [CrossRef]
- Pandiani, C.; Béranger, G.E.; Leclerc, J.; Ballotti, R.; Bertolotto, C. Focus on cutaneous and uveal melanoma specificities. Genes Dev. 2017, 31, 724–743. [Google Scholar] [CrossRef]
- De Lange, M.J.; Razzaq, L.; Versluis, M.; Verlinde, S.; Dogrusöz, M.; Böhringer, S.; Marinkovic, M.; Luyten, G.P.; de Keizer, R.J.; de Gruijl, F.R.; et al. Distribution of GNAQ and GNA11 Mutation Signatures in Uveal Melanoma Points to a Light Dependent Mutation Mechanism. PLoS ONE 2015, 10, e0138002. [Google Scholar] [CrossRef]
- Mallet, J.D.; Gendron, S.P.; Drigeard Desgarnier, M.C.; Rochette, P.J. Implication of ultraviolet light in the etiology of uveal melanoma: A review. Photochem. Photobiol. 2014, 90, 15–21. [Google Scholar] [CrossRef]
- Bulliard, J.L.; Cox, B.; Semenciw, R. Trends by anatomic site in the incidence of cutaneous malignant melanoma in Canada, 1969–1993. Cancer Causes Control 1999, 10, 407–416. [Google Scholar] [CrossRef]
- Jemal, A.; Devesa, S.S.; Hartge, P.; Tucker, M.A. Recent trends in cutaneous melanoma incidence among whites in the United States. J. Natl. Cancer Inst. 2001, 93, 678–683. [Google Scholar] [CrossRef]
- Singh, A.D.; Topham, A. Incidence of uveal melanoma in the United States: 1973–1997. Ophthalmology 2003, 110, 956–961. [Google Scholar] [CrossRef]
- Swerdlow, A.J. Epidemiology of eye cancer in adults in England and Wales, 1962–1977. Am. J. Epidemiol. 1983, 118, 294–300. [Google Scholar] [CrossRef]
- Virgili, G.; Gatta, G.; Ciccolallo, L.; Gatta, G.; Ciccolallo, L.; Capocaccia, R.; Biggeri, A.; Crocetti, E.; Lutz, J.M.; Paci, E. EUROCARE Working Group. Incidence of uveal melanoma in Europe. Ophthalmology 2007, 114, 2309–2315. [Google Scholar] [CrossRef]
- Vajdic, C.M.; Kricker, A.; Giblin, M.; McKenzie, J.; Aitken, J.; Giles, G.G.; Armstrong, B.K. Incidence of ocular melanoma in Australia from 1990 to 1998. Int. J. Cancer 2003, 105, 117–122. [Google Scholar] [CrossRef]
- Bergman, L.; Seregard, S.; Nilsson, B.; Ringborg, U.; Lundell, G.; Ragnarsson-Olding, B. Incidence of uveal melanoma in Sweden from 1960 to 1998. Invest. Ophthalmol. Vis. Sci. 2002, 43, 2579–2583. [Google Scholar]
- Armstrong, B.K.; Kricker, A. The epidemiology of UV induced skin cancer. J. Photochem. Photobiol. B 2001, 63, 8–18. [Google Scholar] [CrossRef]
- Hurst, E.A.; Harbour, J.W.; Cornelius, L.A. Ocular melanoma: A review and the relationship to cutaneous melanoma. Arch. Dermatol. 2003, 139, 1067–1073. [Google Scholar] [CrossRef]
- McLaughlin, C.C.; Wu, X.C.; Jemal, A.; Martin, H.J.; Roche, L.M.; Chen, V.W. Incidence of noncutaneous melanomas in the U.S. Cancer 2005, 103, 1000–1007. [Google Scholar] [CrossRef]
- Hu, D.N. Photobiology of ocular melanocytes and melanoma. Photochem. Photobiol. 2005, 81, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Scotto, J.; Fears, T.R.; Fraumeni, J.F.; National Cancer Institute; Fred Hutchinson Cancer Research Center. Incidence of nonmelanoma skin cancer in the United States prepared by Joseph Scotto, Thomas, R. Fears, and Joseph, F. Fraumeni; in collaboration with Fred Hutchinson Cancer Research Center [et al.]. U.S. Dept. of Health and Human Services, Public Health Service, National Institutes of Health, National Cancer Institute: Bethesda, MD, USA, 1983. Available online: https://search.library.wisc.edu/catalog/999552700102121 (accessed on 1 May 2019).
- Coebergh, J.W.; Neumann, H.A.; Vrints, L.W.; van der Heijden, L.; Meijer, W.J.; Verhagen-Teulings, M.T. Trends in the incidence of non-melanoma skin cancer in the SE Netherlands 1975–1988, A registry-based study. Br. J. Dermatol. 1991, 125, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Paavilainen, V.; Tuominen, J.; Pukkala, E.; Saari, K.M. Basal cell carcinoma of the eyelid in Finland during 1953–1997. Acta. Ophthalmol. Scand. 2005, 83, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.B.; Saw, S.M.; Au Eong, K.G.; Chan, T.K.; Lee, H.P. Incidence of eyelid cancers in Singapore from 1968 to 1995. Br. J. Ophthalmol. 1999, 83, 595–597. [Google Scholar] [CrossRef] [PubMed]
- Dal, H.; Boldemann, C.; Lindelof, B. Trends during a half century in relative squamous cell carcinoma distribution by body site in the Swedish population: Support for accumulated sun exposure as the main risk factor. J. Dermatol. 2008, 35, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Diffey, B.L.; Tate, T.; Davis, A. Solar dosimetry of the face: The relationship of natural ultraviolet radiation exposure to basal cell carcinoma localisation. Phys. Med. Biol. 1979, 24, 931–939. [Google Scholar] [CrossRef]
- Downs, N.; Parisi, A. Measurements of the anatomical distribution of erythemal ultraviolet: A study comparing exposure distribution to the site incidence of solar keratoses, basal cell carcinoma and squamous cell carcinoma. Photochem. Photobiol. Sci. 2009, 8, 1195–1201. [Google Scholar] [CrossRef][Green Version]
- Rosenthal, F.S.; Safran, M.; Taylor, H.R. The ocular dose of ultraviolet radiation from sunlight exposure. Photochem. Photobiol. 1985, 42, 163–171. [Google Scholar] [CrossRef]
- Rosenthal, F.S.; Phoon, C.; Bakalian, A.E.; Taylor, H.R. The ocular dose of ultraviolet radiation to outdoor workers. Invest. Ophthalmol. Vis. Sci. 1988, 29, 649–656. [Google Scholar]
- Birt, B.; Cowling, I.; Coyne, S.; Michael, G. The effect of the eye’s surface topography on the total irradiance of ultraviolet radiation on the inner canthus. J. Photochem. Photobiol. B. 2007, 87, 27–36. [Google Scholar] [CrossRef]
- Behar-Cohen, F.; Bailet, G.; de Ayguavives, T.; Garcia, P.O.; Krutmann, J.; Pena-Garcia, P.; Wolffsohn, J.S. Ultraviolet damage to the eye revisited: Eye-sun protection factor (E-SPF®), a new ultraviolet protection label for eyewear. Clin. Ophthalmol. 2014, 8, 87. [Google Scholar] [CrossRef]
- Sliney, D.H. Geometrical assessment of ocular exposure to environmental UV radiation—Implications for ophthalmic epidemiology. J. Epidemiol. 1999, 9, S22–S32. [Google Scholar] [CrossRef]
- Margo, C.E.; Waltz, K. Basal cell carcinoma of the eyelid and periocular skin. Surv. Ophthalmol. 1993, 38, 169–192. [Google Scholar] [CrossRef]
- Population by Year, by Province and Territory. Available online: http://www40.statcan.gc.ca/l01/cst01/demo02a-eng.htm (accessed on 27 December 2010).
- Canadian Registries Certified in 2009 for 2006 Incidence Data. Available online: http://www.naaccr.org/Certification/CANCert2006 (accessed on 27 December 2010).
- Wolfenden, H.H. On the Methods of Comparing the Moralities of Two or More Communities, and the Standardization of Death-Rates. J. R. Stat. Soc. 1923, 86, 399–411. [Google Scholar] [CrossRef]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- National Cancer Institute. Statistical Research and Applications Branch. In Joinpoint Regression Program; April 2010; 3.4.3. Available online: https://surveillance.cancer.gov/branches/srab/ (accessed on 27 December 2010).
- Clegg, L.X.; Hankey, B.F.; Tiwari, R.; Feuer, E.J.; Edwards, B.K. Estimating average annual per cent change in trend analysis. Stat. Med. 2009, 28, 3670–3682. [Google Scholar] [CrossRef]
- Kim, H.J.; Fay, M.P.; Yu, B.; Barrett, M.J.; Feuer, E.J. Comparability of segmented line regression models. Biometrics 2004, 60, 1005–1014. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Anatomical Grouping | Males | Females | Combined | |||
|---|---|---|---|---|---|---|
| n | Average ASIR ± SE | n | Average ASIR ± SE | n | Average ASIR ± SE | |
| Basal cell carcinoma | ||||||
| Eyelid | 1867 | 6.72 ± 0.83 | 1844 | 5.71 ± 0.70 | 3711 | 6.13 ± 0.53 |
| Chronically exposed skin | 27,934 | 102.21 ± 3.29 | 24,819 | 77.52 ± 2.58 | 52,753 | 88.41 ± 2.03 |
| Face | 20,803 | 76.11 ± 2.84 | 20,296 | 63.56 ± 2.34 | 41,099 | 69.05 ± 1.80 |
| Intermittently exposed skin | 9228 | 29.91 ± 1.65 | 8361 | 24.15 ± 1.37 | 17,589 | 26.69 ± 1.05 |
| Melanoma | ||||||
| Uvea | 137 | 0.49 ± 0.21 | 144 | 0.46 ± 0.19 | 288 | 0.47 ± 0.14 |
| Eyelid | 12 | 0.04 ± 0.04 | 18 | 0.05 ± 0.04 | 30 | 0.04 ± 0.04 |
| Chronically exposed skin | 905 | 3.33 ± 0.60 | 573 | 1.71 ± 0.37 | 1478 | 2.42 ± 0.33 |
| Face | 464 | 1.81 ± 0.45 | 372 | 1.13 ± 0.30 | 836 | 1.42 ± 0.26 |
| Intermittently exposed skin | 2849 | 8.68 ± 0.86 | 3282 | 9.36 ± 0.86 | 6131 | 8.99 ± 0.61 |
| Anatomical Grouping | Males | Females | ||
|---|---|---|---|---|
| Trend | AAPC (95% CI) | Trend | AAPC (95% CI) | |
| Basal cell carcinoma | ||||
| Eyelid | Stable | −0.4 (−1.1 to 0.4) | Stable | 0.6 (−0.1 to 1.2) |
| Chronically exposed skin | Increasing | 1.8 * (0.9 to 2.8) | Increasing | 1.7 * (1.1 to 2.4) |
| Face | Increasing | 1.4 * (0.7 to 2.1) | Increasing | 1.7 * (0.9 to 2.5) |
| Intermittently exposed skin | Increasing | 6.3 * (5.1 to 7.6) | Increasing | 6.4 * (5.2 to 7.7) |
| Melanoma | ||||
| Uvea | Stable | −1.4 (−3.6 to 0.8) | Stable | −0.9 (−2.9 to 1.2) |
| Eyelid | § | § | ||
| Chronically exposed skin | Increasing | 3.0 * (1.9 to 4.1) | Increasing | 2.2 * (0.5 to 3.9) |
| Face | Increasing | 2.4 * (1.0 to 3.8) | Stable | 2.1 (−0.0 to 4.3) |
| Intermittently exposed skin | Increasing | 3.2 * (1.9 to 4.5) | Increasing | 2.0 * (0.6 to 3.3) |
| Test of Parallelism | Result | ||
|---|---|---|---|
| Group 1 | Group 2 | Males | Females |
| Basal cell carcinoma | |||
| Eyelid vs. | Chronically exposed skin | * Not parallel (p = 0.001) | * Not parallel (p = 0.01) |
| Face | * Not parallel (p = 0.002) | * Not parallel (p = 0.02) | |
| Intermittently exposed skin | * Not parallel (p = 0.0002) | * Not parallel (p = 0.0002) | |
| Chronically exposed skin vs. | Intermittently exposed skin | * Not parallel (p = 0.0002) | * Not parallel (p = 0.0002) |
| Melanoma | |||
| Uvea vs. | Chronically exposed skin | * Not parallel (p = 0.001) | * Not parallel (p = 0.04) |
| Face | * Not parallel (p = 0.002) | * Not parallel (p = 0.03) | |
| Intermittently exposed skin | * Not parallel (p = 0.005) | Parallel (p = 0.06) | |
| Chronically exposed skin vs. | Intermittently exposed skin | Parallel (p = 0.81) | Parallel (p = 0.46) |
| Inter-ophthalmic | |||
| Uveal malignant melanoma vs. | Eyelid basal cell carcinoma | Parallel (p = 0.08) | Parallel (p = 0.24) |
| Name | ICD-O Code | ICD-O Category | ICD-O Description |
|---|---|---|---|
| Topographical group criteria | |||
| Uvea | C69.3 | Eye and adnexa | Choroid |
| Eyelid | C44.1 | Skin | Eyelid |
| Chronically exposed skin | C44.0, C44.2–C44.4 | Skin | Skin of lip NOS, external ear, skin of other and unspecified parts of the face, skin of scalp and neck |
| Face | C44.3 | Skin | Skin of other and unspecified parts of the face |
| Intermittently exposed skin | C44.5–C44.7 | Skin | Skin of trunk, skin of upper limb and shoulder, skin of lower limb and hip |
| Morphological tumor criteria | |||
| Basal cell carcinoma | 8090/3-8094/3, 8097/3, 8098/3 | Basal cell neoplasms | Basal cell carcinoma, NOS; multifocal superficial basal cell carcinoma; infiltrating basal cell carcinoma, NOS; basal cell carcinoma, fibroepithelial; basosquamous carcinoma; basal cell carcinoma, nodular; adenoid basal cell carcinoma |
| Malignant melanoma | 8720/3–8723/3, 8730/3, 8740/3–8746/3, 8761/3, 8770/3–8774/3,8780/3 | Nevi and melanomas | Malignant melanoma, NOS; nodular melanoma; balloon cell melanoma; malignant melanoma, regressing; amelanotic melanoma; malignant melanoma in junctional nevus; malignant melanoma in precancerous melanosis; lentigo maligna melanoma; superficial spreading melanoma; acral lentiginous melanoma, malignant; desmoplastic melanoma, malignant; mucosal lentiginous melanoma; malignant melanoma in giant pigmented nevus; mixed epithelioid and spindle cell melanoma; epithelioid cell melanoma; spindle cell melanoma, NOS; spindle cell melanoma, type A; spindle cell melanoma, type B; blue nevus, malignant |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weis, E.; Vrouwe, S.Q.; LeBaron, D.B.; Parliament, M.B.; Shields, J.; Shields, C.L. Changes in Ultraviolet Radiation Exposure to the Ocular Region: A Population-Based Study. Cancers 2019, 11, 719. https://doi.org/10.3390/cancers11050719
Weis E, Vrouwe SQ, LeBaron DB, Parliament MB, Shields J, Shields CL. Changes in Ultraviolet Radiation Exposure to the Ocular Region: A Population-Based Study. Cancers. 2019; 11(5):719. https://doi.org/10.3390/cancers11050719
Chicago/Turabian StyleWeis, Ezekiel, Sebastian Q. Vrouwe, David B. LeBaron, Matthew B. Parliament, Jerry Shields, and Carol L. Shields. 2019. "Changes in Ultraviolet Radiation Exposure to the Ocular Region: A Population-Based Study" Cancers 11, no. 5: 719. https://doi.org/10.3390/cancers11050719
APA StyleWeis, E., Vrouwe, S. Q., LeBaron, D. B., Parliament, M. B., Shields, J., & Shields, C. L. (2019). Changes in Ultraviolet Radiation Exposure to the Ocular Region: A Population-Based Study. Cancers, 11(5), 719. https://doi.org/10.3390/cancers11050719