Efficacy and Safety of Ablative Therapy in the Treatment of Patients with Metastatic Pheochromocytoma and Paraganglioma

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Demographics and Clinical Presentation
2.2. Ablation Sessions
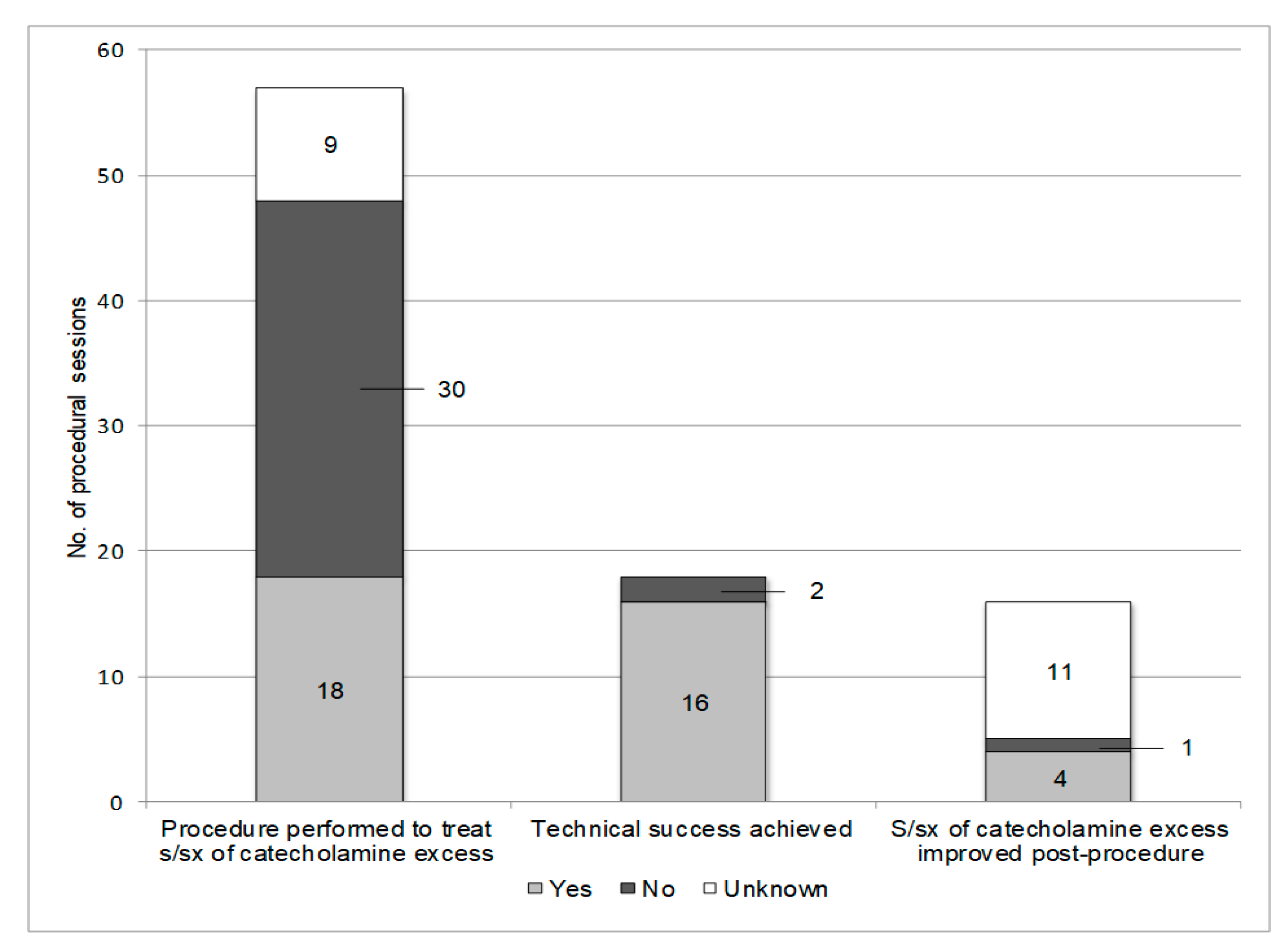
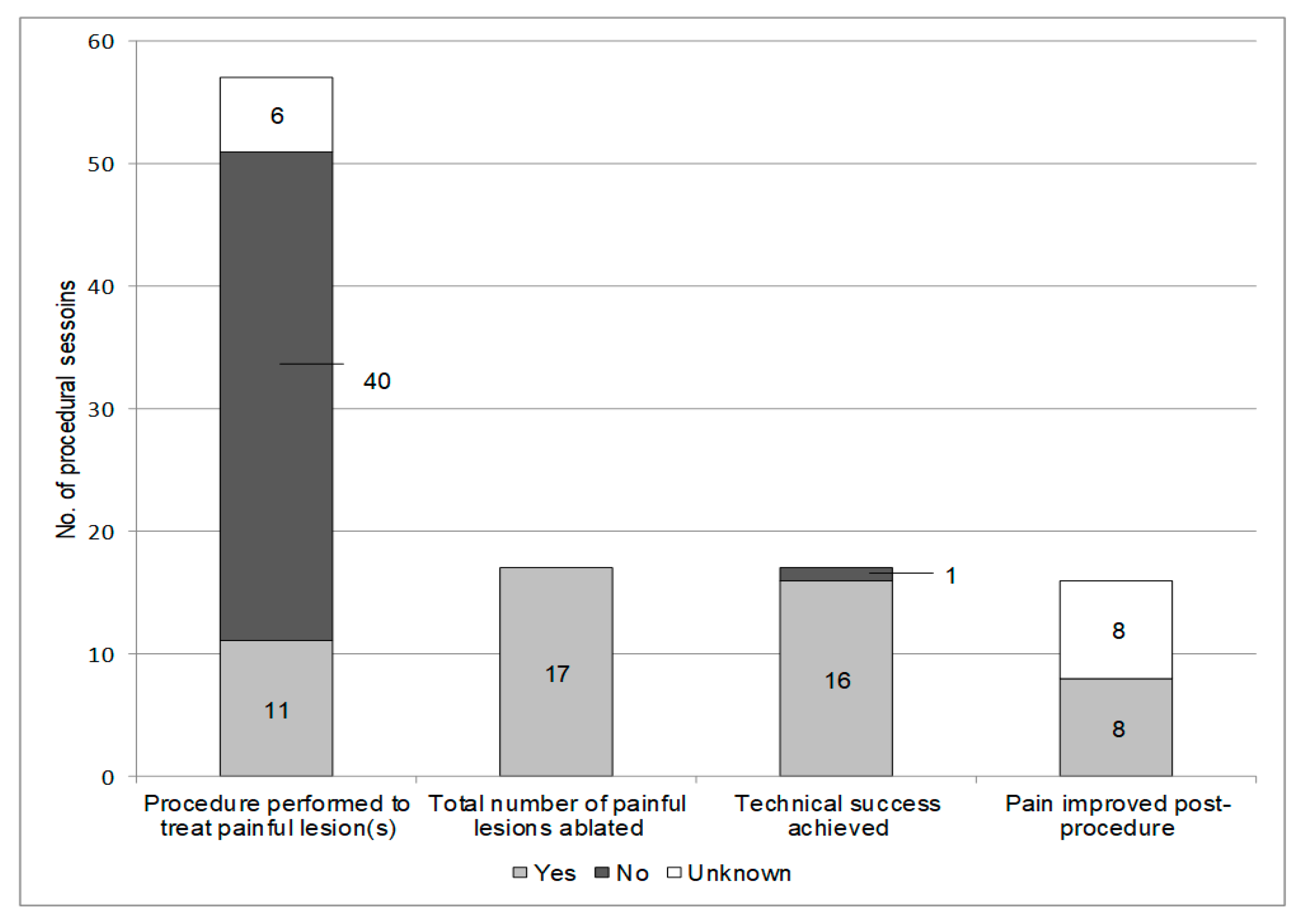
2.3. Ablation Session Indications
2.4. Pre-Ablation Adrenergic Blockade
2.5. Ablated Lesions
2.6. Technical Success
2.7. Radiographic Outcomes
2.8. Symptom Outcomes
2.9. Ablation Session Complications
2.10. Long-Term Outcomes
3. Discussion
4. Materials and Methods
4.1. Patient Demographics and Clinical Presentation
4.2. Subjects
4.3. Disease-Related Definitions
4.4. Thermal and Chemical Ablation Overview
4.5. Radiographic Outcomes Definitions
4.6. Symptom Outcomes
4.7. Procedural Complications
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chen, H.; Sippel, R.S.; O’Dorisio, M.S.; Vinik, A.I.; Lloyd, R.V.; Pacak, K. The North American Neuroendocrine Tumor Society consensus guideline for the diagnosis and management of neuroendocrine tumors: Pheochromocytoma, paraganglioma, and medullary thyroid cancer. Pancreas 2010, 39, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Bravo, E.L. Pheochromocytoma: New concepts and future trends. Kidney Int. 1991, 40, 544–556. [Google Scholar] [CrossRef] [PubMed]
- Plouin, P.F.; Chatellier, G.; Fofol, I.; Corvol, P. Tumor recurrence and hypertension persistence after successful pheochromocytoma operation. Hypertension 1997, 29, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.E.; O’Neill, J.A., Jr.; Holcomb, G.W., 3rd; Morgan, W.M., 3rd; Neblett, W.W., 3rd; Oates, J.A.; Brown, N.; Nadeau, J.; Smith, B.; Page, D.L.; et al. Clinical experience over 48 years with pheochromocytoma. Ann. Surg. 1999, 229, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Tischler, A.S.; de Krijger, R.R.; Gill, A.; Kawashima, A.; Kimura, N.; Komminoth, P.; Papathomas, T.G.; Thompson, L.D.R.; Tissier, F.; Williams, M.D.; et al. Tumours of the Adrenal Medulla and Extra-Adrenal Paraganglia, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017; Volume 10, pp. 184–185. [Google Scholar]
- Hamidi, O.; Young, W.F., Jr.; Iniguez-Ariza, N.M.; Kittah, N.E.; Gruber, L.; Bancos, C.; Tamhane, S.; Bancos, I. Malignant Pheochromocytoma and Paraganglioma: 272 Patients Over 55 Years. J. Clin. Endocrinol. Metab. 2017, 102, 3296–3305. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, O.; Young, W.F., Jr.; Gruber, L.; Smestad, J.; Yan, Q.; Ponce, O.J.; Prokop, L.; Murad, M.H.; Bancos, I. Outcomes of patients with metastatic phaeochromocytoma and paraganglioma: A systematic review and meta-analysis. Clin. Endocrinol. 2017, 87, 440–450. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.F.; Atwell, T.D.; Charboneau, W.J.; Young, W.F., Jr.; Wass, T.C.; Callstrom, M.R. Minimally invasive treatment of metastatic pheochromocytoma and paraganglioma: Efficacy and safety of radiofrequency ablation and cryoablation therapy. J. Vasc. Interv. Radiol. 2011, 22, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Mamlouk, M.D.; vanSonnenberg, E.; Stringfellow, G.; Smith, D.; Wendt, A. Radiofrequency ablation and biopsy of metastatic pheochromocytoma: emphasizing safety issues and dangers. J. Vasc. Interv. Radiol. 2009, 20, 670–673. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, A.M.; Locklin, J.; Lai, E.W.; Adams, K.T.; Fojo, A.T.; Pacak, K.; Wood, B.J. Radiofrequency ablation of metastatic pheochromocytoma. J. Vasc. Interv. Radiol. 2009, 20, 1483–1490. [Google Scholar] [CrossRef] [PubMed]
- Pacak, K.; Fojo, T.; Goldstein, D.S.; Eisenhofer, G.; Walther, M.M.; Linehan, W.M.; Bachenheimer, L.; Abraham, J.; Wood, B.J. Radiofrequency ablation: A novel approach for treatment of metastatic pheochromocytoma. J. Natl. Cancer Inst. 2001, 93, 648–649. [Google Scholar] [CrossRef] [PubMed]
- Gravel, G.; Leboulleux, S.; Tselikas, L.; Fassio, F.; Berraf, M.; Berdelou, A.; Ba, B.; Hescot, S.; Hadoux, J.; Schlumberger, M.; et al. Prevention of serious skeletal-related events by interventional radiology techniques in patients with malignant paraganglioma and pheochromocytoma. Endocrine 2018, 59, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Mukherji, S.K.; Kasper, M.E.; Tart, R.P.; Mancuso, A.A. Irradiated paragangliomas of the head and neck: CT and MR appearance. AJNR 1994, 15, 357–363. [Google Scholar] [PubMed]
- Atwell, T.D.; Carter, R.E.; Schmit, G.D.; Carr, C.M.; Boorjian, S.A.; Curry, T.B.; Thompson, R.H.; Kurup, A.N.; Weisbrod, A.J.; Chow, G.K.; et al. Complications following 573 percutaneous renal radiofrequency and cryoablation procedures. J. Vasc. Interv. Radiol. 2012, 23, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Welch, B.T.; Callstrom, M.R.; Carpenter, P.C.; Wass, C.T.; Welch, T.L.; Boorjian, S.A.; Nichols, D.A.; Thompson, G.B.; Lohse, C.M.; Erickson, D.; et al. A single-institution experience in image-guided thermal ablation of adrenal gland metastases. J. Vasc. Interv. Radiol. 2014, 25, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Welch, B.T.; Callstrom, M.R.; Morris, J.M.; Kurup, A.N.; Schmit, G.D.; Weisbrod, A.J.; Lohse, C.M.; Kohli, M.; Costello, B.A.; Olivier, K.R.; et al. Feasibility and oncologic control after percutaneous image guided ablation of metastatic renal cell carcinoma. J. Urol. 2014, 192, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Data, Number (Percent or Range) |
|---|---|
| N | 31 |
| Female sex, n (%) | 22 (71%) |
| Primary tumor, n (%) | |
| PGL PHEO | 24 (77%) 7 (23%) |
| Genetic status, n (%) | |
| SDHB positive SDHD positive NF1 positive Sporadic No genetic testing performed | 17 (74%) 1 (4%) 1 (4%) 4 (17%) 8 |
| Age at primary tumor diagnosis, years (range) | 27 (8–72) |
| Mode of primary tumor discovery, n (%) Symptoms of catecholamine excess Symptoms of tumor-related mass effect Incidental discovery on imaging Symptoms of catecholamine excess + tumor mass effect Hypervascular right tonsillar mass Syncope with neck rotation B symptoms * Unknown | 12 (39%) 9 (29%) 5 (16%) 2 (6%) 1 (3%) 1 (3%) 1 (3%) 1 |
| Primary tumor location, n (%) Abdomen/pelvis Skull base and neck Thorax | 31 (76%) 7 (17%) 3 (7%) |
| Primary tumor hormonal status, n (%) Functional Non-functional Unknown | 19 (83%) 4 (17%) 8 |
| Primary tumor size, mm (range) | 55.5 (10–190) |
| Surgical resection of the primary tumor, n (%) | 32 (94%) |
| Age at diagnosis of metastatic disease, years (range) | 38 (12–77) |
| Time to diagnosis of metastatic disease, years (range) | 4 (0–53) |
| Metachronous metastases, n (%) | 23 (74%) |
| Location of metastases, n (%) Osseous Abdomen Thorax Pelvis Neck Brain | 27 (90%) 23 (74%) 13 (42%) 10 (33%) 3 (10%) 1 (3%) |
| Metastases per patient, n (range) | >5 (1–>5) |
| Treatment with systemic therapy, n (%) | 14 (45%) |
| Variable | Data |
|---|---|
| Total lesions ablated, n | 123 |
| Total procedural sessions, n | 57 |
| Ablation sessions per patient, n (range) | 1 (1–8) |
| Total ablation sessions, n (%) Radiofrequency ablation Cryoablation Percutaneous ethanol injection | 69 42 (61%) 23 (33%) 4 (6%) |
| Location of ablated lesions, n (%) Osseous Hepatic Abdominal/pelvic, non-hepatic | 63 (51%) 54 (44%) 6 (5%) |
| Lesions ablated per patient, n | 3 (1–15) |
| Size of ablated lesions, mm (range) Osseous Hepatic Abdominal/pelvic, non-hepatic | 15.5 (3–65) 15 (4–47) 21.5 (16–36) |
| Metastases treated at the time of ablation, n (%) Not all present metastases treated All present metastases treated Unknown | 35 (76%) 11 (24%) 11 |
| Technical success for each ablated lesion, n (%) Achieved Not achieved Unknown | 94 (94%) 6 (6%) 19 |
| All Ablated Metastases | |||
|---|---|---|---|
| Variable | Data | ||
| Local control, n (%) Radiofrequency ablation Cryoablation Percutaneous ethanol injection | 69/80 (86%) 44/51 (86%) 24/28 (86%) 1/2 (50%) | ||
| Local control, n (%) Patients treated with systemic therapy Patients not treated with systemic therapy | 69/80 (86%) 36/46 (78%) 33/34 (97%) | ||
| Duration of follow-up for ablated lesions with local control, months (range) | 26 (2–163) | ||
| Progression for ablated lesions, n (%) Radiofrequency ablation Cryoablation Percutaneous ethanol injection | 11/80 (14%) 7/51 (14%) 4/28 (14%) 1/2 (50%) | ||
| Time to progression, months (range) | 16 (6–69) | ||
| Osseous and hepatic metastases treated with radiofrequency ablation and cryoablation | |||
| Osseous | Hepatic | p value | |
| N | 45 | 32 | |
| Local control, n (%) Radiofrequency ablation Cryoablation | 37/45 (82%) 14/19 (74%) 23/26 (88%)* | 30/32 (94%) 30/32 (94%) 0/0 (0%) | 0.14 0.04 |
| Progression, n (%) Radiofrequency ablation Cryoablation | 8/45 (18%) 5/19 (26%) 3/26 (12%)* | 2/32 (6%) 2/32 (6%) 0/0 (0%) | 0.14 0.04 |
| Complication and Mortality Rates | Data, Number (Percent or Range) |
|---|---|
| Procedural session complication rate, n (%) No complication Grade I Grade II Grade III Grade IV Grade V | 33 (67%) 7 (14%) 7 (14%) 0 1 (2%) 1 (2%) |
| Long-term patient outcomes | |
| Deceased secondary to metastatic PPGL, n (%) | 10 (32%) |
| Time from ablation session to death, months (range) Session 1 (n = 10) Session 2 (n = 4) Session 3 (n = 3) Session 4 (n = 2) Session 5 (n = 2) Session 6 (n = 1) | 63.5 (2–133) 68.5 (8–113) 52 (51–89) 21 (0–42) 17.5 (0–35) 26 |
| Alive at time of last follow-up, n (%) Time from ablation session 1 to most recent follow-up, months (range) | 21 (68%) 60 (0–163) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohlenberg, J.; Welch, B.; Hamidi, O.; Callstrom, M.; Morris, J.; Sprung, J.; Bancos, I.; Young, W., Jr. Efficacy and Safety of Ablative Therapy in the Treatment of Patients with Metastatic Pheochromocytoma and Paraganglioma. Cancers 2019, 11, 195. https://doi.org/10.3390/cancers11020195
Kohlenberg J, Welch B, Hamidi O, Callstrom M, Morris J, Sprung J, Bancos I, Young W Jr. Efficacy and Safety of Ablative Therapy in the Treatment of Patients with Metastatic Pheochromocytoma and Paraganglioma. Cancers. 2019; 11(2):195. https://doi.org/10.3390/cancers11020195
Chicago/Turabian StyleKohlenberg, Jacob, Brian Welch, Oksana Hamidi, Matthew Callstrom, Jonathan Morris, Juraj Sprung, Irina Bancos, and William Young, Jr. 2019. "Efficacy and Safety of Ablative Therapy in the Treatment of Patients with Metastatic Pheochromocytoma and Paraganglioma" Cancers 11, no. 2: 195. https://doi.org/10.3390/cancers11020195
APA StyleKohlenberg, J., Welch, B., Hamidi, O., Callstrom, M., Morris, J., Sprung, J., Bancos, I., & Young, W., Jr. (2019). Efficacy and Safety of Ablative Therapy in the Treatment of Patients with Metastatic Pheochromocytoma and Paraganglioma. Cancers, 11(2), 195. https://doi.org/10.3390/cancers11020195