Nutrition Impact Symptoms Are Prognostic of Quality of Life and Mortality After Surgery for Oesophageal Cancer

 ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. Data Sources
2.2. Study Design
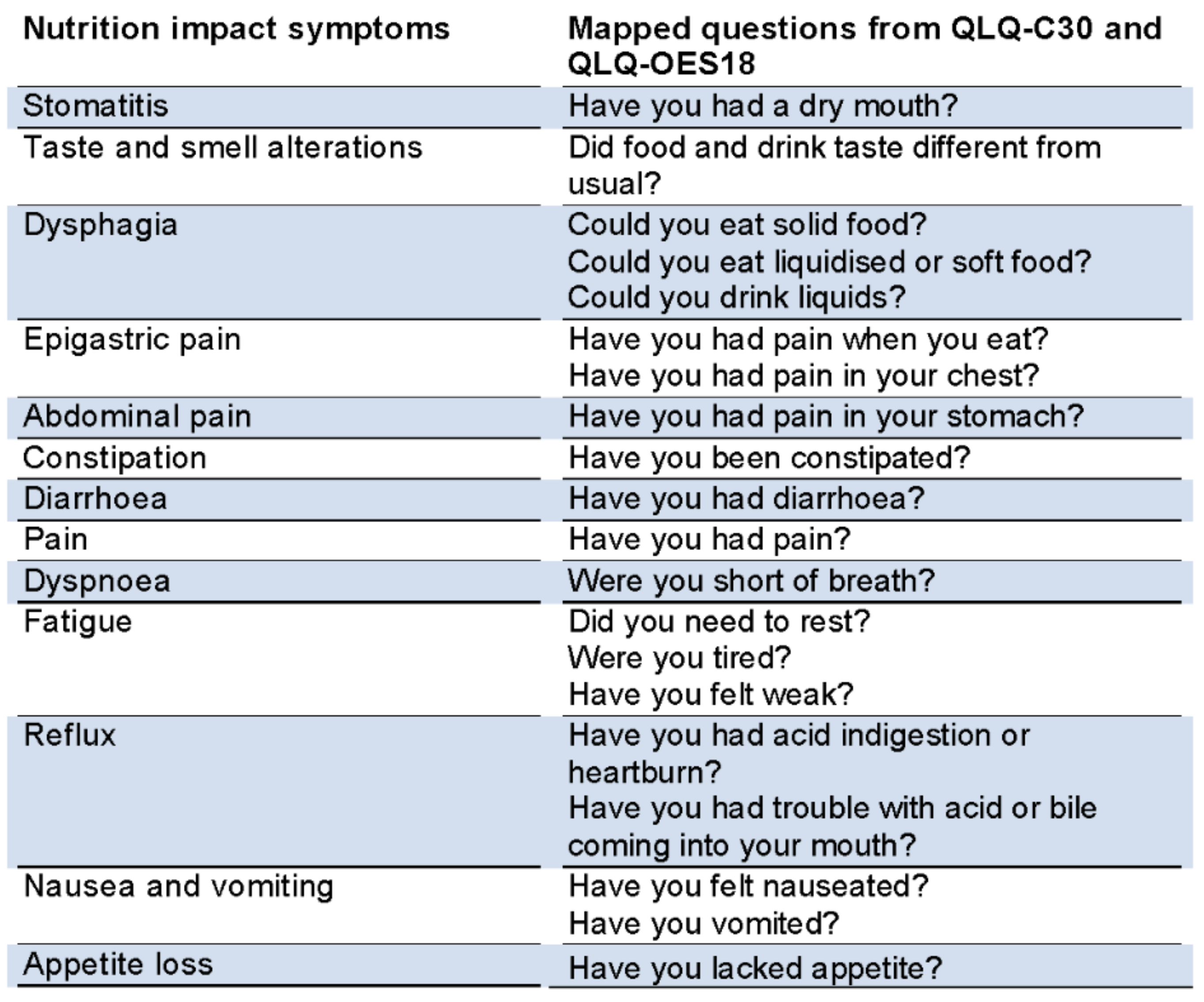
2.2.1. Exposure
2.2.2. Outcome
2.3. Statistical Analysis
3. Results
3.1. Patients
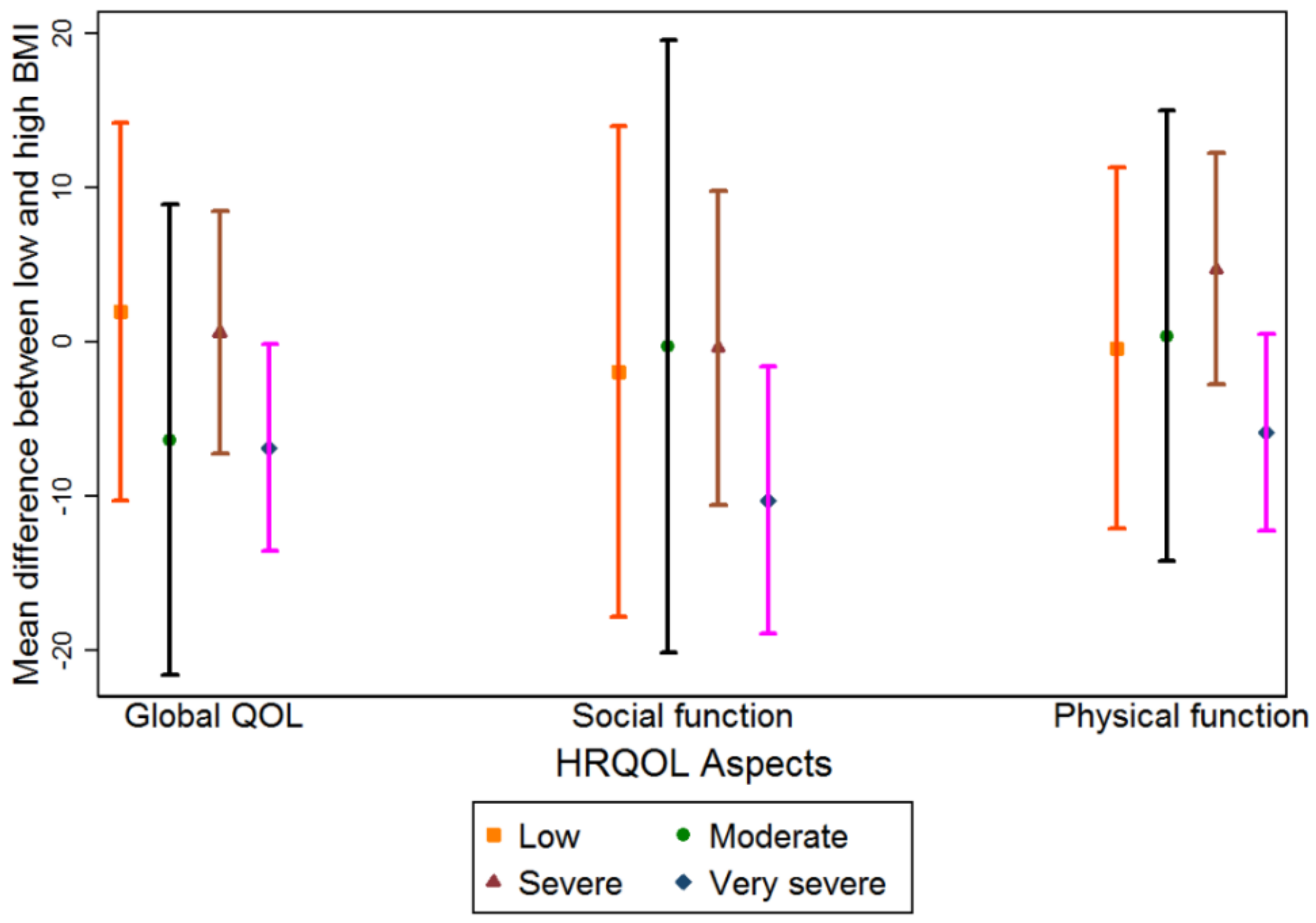
3.2. Health-Related Quality of Life
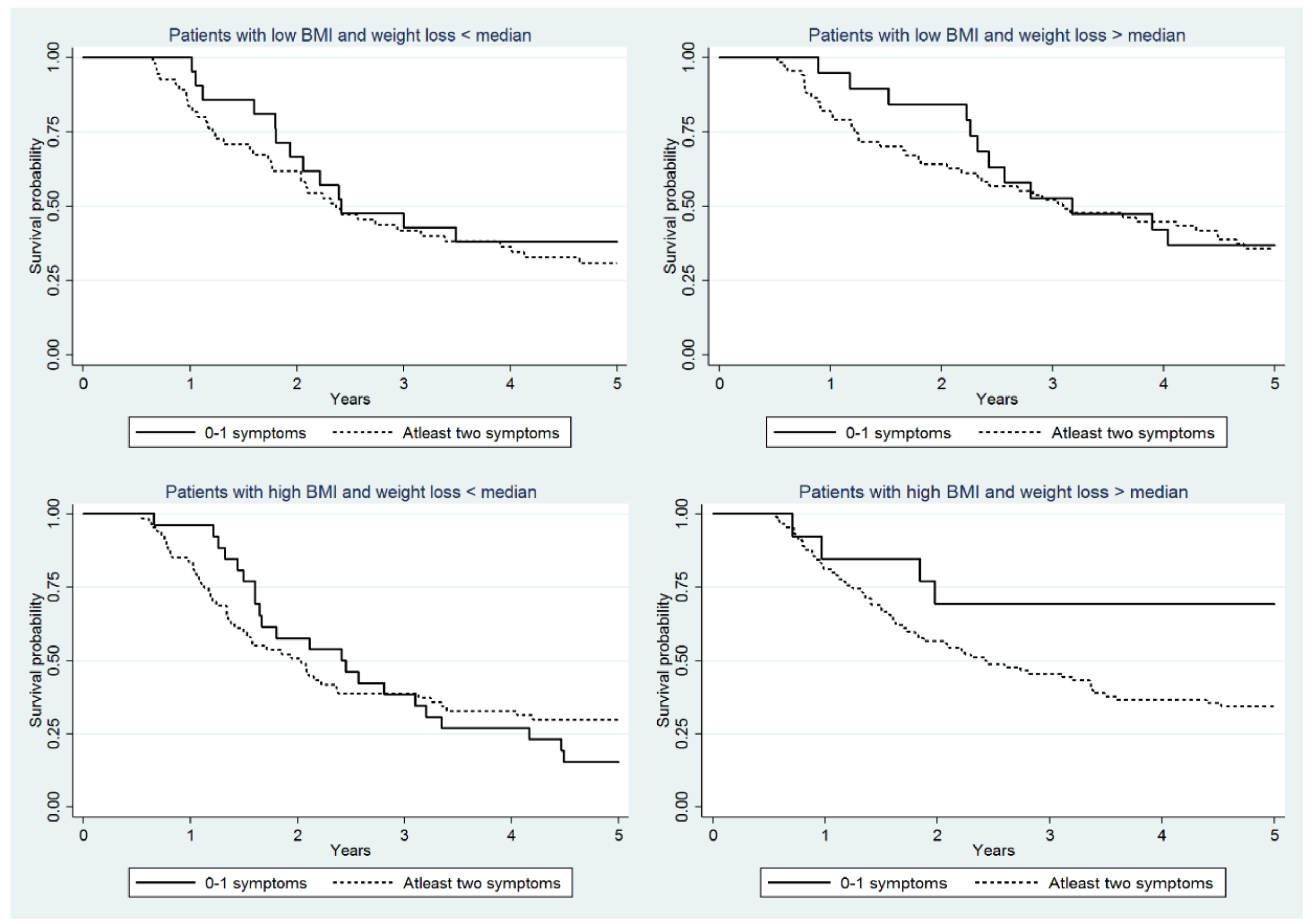
3.3. Overall 5 Year Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Globocan 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (accessed on 7 April 2014).
- Lagergren, J.; Smyth, E.; Cunningham, D.; Lagergren, P. Oesophageal cancer. Lancet 2017, 390, 2383–2396. [Google Scholar] [CrossRef]
- Martin, L.; Lagergren, P. Risk factors for weight loss among patients surviving 5 years after esophageal cancer surgery. Ann. Surg. Oncol. 2015, 22, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Djarv, T.; Lagergren, P. Six-month postoperative quality of life predicts long-term survival after oesophageal cancer surgery. Eur. J. Cancer 2011, 47, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The european organization for research and treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Blazeby, J.M.; Alderson, D.; Winstone, K.; Steyn, R.; Hammerlid, E.; Arraras, J.; Farndon, J.R. Development of an EORTC questionnaire module to be used in quality of life assessment for patients with oesophageal cancer. The EORTC quality of life study group. Eur. J. Cancer 1996, 32A, 1912–1917. [Google Scholar] [CrossRef]
- Ringdal, G.I.; Ringdal, K. Testing the EORTC quality of life questionnaire on cancer patients with heterogeneous diagnoses. Qual. Life Res. 1993, 2, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Hjermstad, M.J.; Fossa, S.D.; Bjordal, K.; Kaasa, S. Test/retest study of the European organization for research and treatment of cancer core quality-of-life questionnaire. J. Clin. Oncol. 1995, 13, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Groenvold, M.; Klee, M.C.; Sprangers, M.A.; Aaronson, N.K. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J. Clin. Epidemiol. 1997, 50, 441–450. [Google Scholar] [CrossRef]
- Ringdal, K.; Ringdal, G.I.; Kaasa, S.; Bjordal, K.; Wisloff, F.; Sundstrom, S.; Hjermstad, M.J. Assessing the consistency of psychometric properties of the hrqol scales within the EORTC QLQ-C30 across populations by means of the mokken scaling model. Qual. Life Res. 1999, 8, 25–43. [Google Scholar] [CrossRef] [PubMed]
- Blazeby, J.M.; Conroy, T.; Hammerlid, E.; Fayers, P.; Sezer, O.; Koller, M.; Arraras, J.; Bottomley, A.; Vickery, C.W.; Etienne, P.L.; et al. Clinical and psychometric validation of an EORTC questionnaire module, the EORTC QLQ-OES18, to assess quality of life in patients with oesophageal cancer. Eur. J. Cancer 2003, 39, 1384–1394. [Google Scholar] [CrossRef]
- Official Statistics of Sweden (2014) Statistics–Health and Medical Care, Causes of Death 2014. Available online: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/19909/2015-8-1.pdf (accessed on 15 August 2015).
- Baracos, V.E. Cancer-associated cachexia and underlying biological mechanisms. Annu. Rev. Nutr. 2006, 26, 435–461. [Google Scholar] [CrossRef] [PubMed]
- Grosvenor, M.; Bulcavage, L.; Chlebowski, R.T. Symptoms potentially influencing weight loss in a cancer population. Correlations with primary site, nutritional status, and chemotherapy administration. Cancer 1989, 63, 330–334. [Google Scholar] [CrossRef]
- Khalid, U.; Spiro, A.; Baldwin, C.; Sharma, B.; McGough, C.; Norman, A.R.; Eisen, T.; O’Brien, M.E.R.; Cunningham, D.; Andreyev, H.J.N. Symptoms and weight loss in patients with gastrointestinal and lung cancer at presentation. Support Care Cancer 2006, 15, 39. [Google Scholar] [CrossRef] [PubMed]
- McCallum, P.D.; Polisena, C.G. The Clinical Guide to Oncology Nutrition, 2nd ed.; American Dietetic Association: Chicago, IL USA, 2006; ISBN 9780880913393. [Google Scholar]
- Sarhill, N.; Mahmoud, F.; Walsh, D.; Nelson, K.A.; Komurcu, S.; Davis, M.; LeGrand, S.; Abdullah, O.; Rybicki, L. Evaluation of nutritional status in advanced metastatic cancer. Support Care Cancer 2003, 11, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Rouvelas, I.; Zeng, W.; Lindblad, M.; Viklund, P.; Ye, W.; Lagergren, J. Survival after surgery for oesophageal cancer: A population-based study. Lancet Oncol. 2005, 6, 864–870. [Google Scholar] [CrossRef]
- Zhu, Z.J.; Hu, Y.; Zhao, Y.F.; Chen, X.Z.; Chen, L.Q.; Chen, Y.T. Early recurrence and death after esophagectomy in patients with esophageal squamous cell carcinoma. Ann. Thorac. Surg. 2011, 91, 1502–1508. [Google Scholar] [CrossRef] [PubMed]
- Dresner, S.M.; Griffin, S.M. Pattern of recurrence following radical oesophagectomy with two-field lymphadenectomy. Br. J. Surg. 2000, 87, 1426–1433. [Google Scholar] [CrossRef] [PubMed]
- Abate, E.; DeMeester, S.R.; Zehetner, J.; Oezcelik, A.; Ayazi, S.; Costales, J.; Banki, F.; Lipham, J.C.; Hagen, J.A.; DeMeester, T.R. Recurrence after esophagectomy for adenocarcinoma: Defining optimal follow-up intervals and testing. J. Am. Coll. Surg. 2010, 210, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Lagergren, J.; Lindblad, M.; Rouvelas, I.; Lagergren, P. Malnutrition after oesophageal cancer surgery in sweden. Br. J. Surg. 2007, 94, 1496–1500. [Google Scholar] [CrossRef] [PubMed]
- D’Journo, X.B.; Ouattara, M.; Loundou, A.; Trousse, D.; Dahan, L.; Nathalie, T.; Doddoli, C.; Seitz, J.F.; Thomas, P.A. Prognostic impact of weight loss in 1-year survivors after transthoracic esophagectomy for cancer. Dis. Esophagus. 2012, 25, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.A.; Docherty, N.G.; Eckhardt, H.G.; Doyle, S.L.; Guinan, E.M.; Ravi, N.; Reynolds, J.V.; Roux, C.W. Weight loss, satiety, and the postprandial gut hormone response after esophagectomy: A prospective study. Ann. Surg. 2016, 266, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Haverkort, E.B.; Binnekade, J.M.; Busch, O.R.; van Berge Henegouwen, M.I.; de Haan, R.J.; Gouma, D.J. Presence and persistence of nutrition-related symptoms during the first year following esophagectomy with gastric tube reconstruction in clinically disease-free patients. World J. Surg. 2010, 34, 2844–2852. [Google Scholar] [CrossRef] [PubMed]
- Anandavadivelan, P.; Wikman, A.; Johar, A.; Lagergren, P. Impact of weight loss and eating difficulties on health-related quality of life up to 10 years after oesophagectomy for cancer. Br. J. Surg. 2018, 5, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Lagergren, P. Long-term weight change after oesophageal cancer surgery. Br. J. Surg. 2009, 96, 1308–1314. [Google Scholar] [CrossRef] [PubMed]
- Akkerman, R.D.; Haverkamp, L.; van Hillegersberg, R.; Ruurda, J.P. Surgical techniques to prevent delayed gastric emptying after esophagectomy with gastric interposition: A systematic review. Ann. Thorac. Surg. 2014, 98, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Andreyev, H.J.; Davidson, S.E.; Gillespie, C.; Allum, W.H.; Swarbrick, E. Practice guidance on the management of acute and chronic gastrointestinal problems arising as a result of treatment for cancer. Gut 2012, 61, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Backemar, L.; Lagergren, P.; Johar, A.; Lagergren, J. Impact of co-morbidity on mortality after oesophageal cancer surgery. Br. J. Surg. 2015, 102, 1097–1105. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 358) | Low BMI (n = 162) | High BMI (n = 196) |
|---|---|---|---|
| Sex | |||
| Male | 291 (81.3) | 119 (33.2) | 172 (48.0) |
| Female | 67 (18.7) | 43 (12.0) | 24 (6.7) |
| Average age at operation * | 66 (65–67) | 66 (64–67) | 65 (64–67) |
| Charlson co-morbidity score | |||
| 0 | 203 (56.7) | 103 (28.8) | 100 (27.9) |
| 1 | 90 (25.1) | 39 (10.9) | 51 (14.3) |
| >2 | 65 (18.2) | 20 (5.6) | 45 (12.6) |
| Histology | |||
| Adenocarcinoma and dysplasia | 276 (77.1) | 103 (28.8) | 173 (48.3) |
| Squamous cell carcinoma | 82 (22.9) | 59 (16.5) | 23 (6.4) |
| Tumour stage | |||
| 0–I | 80 (22.6) | 37 (10.5) | 43 (12.2) |
| II | 112 (31.6) | 58 (16.4) | 54 (15.3) |
| III | 137 (38.7) | 60 (17.0) | 77 (21.8) |
| IV | 25 (7.1) | 4 (1.1) | 21 (5.9) |
| Tumour location in oesophagus | |||
| Upper and Middle | 304 (84.9) | 126 (35.2) | 178 (49.7) |
| Lower and Cardia (Siewert II/III) | 54 (15.1) | 36 (10.1) | 18 (5.0) |
| Type of operation | |||
| Oesophageal resection | 269 (75.6) | 121 (34.0) | 148 (41.6) |
| Cardia resection | 16 (4.5) | 3 (0.8) | 13 (3.7) |
| Extended total gastrectomy | 34 (9.6) | 17 (4.8) | 17 (4.8) |
| Total gastrectomy and oesophageal resection | 37 (10.4) | 20 (5.6) | 17 (4.8) |
| Surgical complications | |||
| No | 243 (67.9) | 115 (32.1) | 128 (35.8) |
| Yes | 115 (32.1) | 47 (13.1) | 68 (19.0) |
| Nutritional Problems | Low BMI | High BMI | ||||
|---|---|---|---|---|---|---|
| Global QOL MD 95% CI | Social Function MD 95% CI | Physical Function MD 95% CI | Global QOL MD 95% CI | Social Function MD 95% CI | Physical Function MD 95% CI | |
| Low (Reference) | 73 (63–84) | 87 (73–100) | 84 (74–94) | 71 (62–81) | 89 (76–101) | 84 (75–94) |
| Moderate | −3 (−17–10) | −2 (−19–16) | −1 (−14–11) | 5 (−9–19) | −3 (−22–15) | −2 (−16–12) |
| Severe | −21 (−32 to −11) *†† | −23 (−37 to −9) *†† | −14 (−24 to −4) *† | −20 (−29 to −11) *†† | −24 (−37 to −12) *†† | −19 (−28 to −10) *† |
| Very severe | −29 (−39 to −19) *†† | -28 (−41 to −14) *†† | −23 (−33 to −13) *†† | −20(−29 to −11) *†† | −19 (−31 to −7) *†† | −17 (−26 to −9) *† |
| At Least 2 Symptoms Vs 0–1 Symptom | <Median Weight Loss HR (95% CI) | p Value | >Median Weight Loss HR (95% CI) | p Value |
|---|---|---|---|---|
| Low BMI | 1.16 (0.57–2.34) | 0.68 | 1.92 (0.90–4.14) | 0.09 |
| High BMI | 0.92 (0.53–1.58) | 0.75 | 4.64 (1.38–15.56) * | 0.01 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anandavadivelan, P.; Martin, L.; Djärv, T.; Johar, A.; Lagergren, P. Nutrition Impact Symptoms Are Prognostic of Quality of Life and Mortality After Surgery for Oesophageal Cancer. Cancers 2018, 10, 318. https://doi.org/10.3390/cancers10090318
Anandavadivelan P, Martin L, Djärv T, Johar A, Lagergren P. Nutrition Impact Symptoms Are Prognostic of Quality of Life and Mortality After Surgery for Oesophageal Cancer. Cancers. 2018; 10(9):318. https://doi.org/10.3390/cancers10090318
Chicago/Turabian StyleAnandavadivelan, Poorna, Lena Martin, Therese Djärv, Asif Johar, and Pernilla Lagergren. 2018. "Nutrition Impact Symptoms Are Prognostic of Quality of Life and Mortality After Surgery for Oesophageal Cancer" Cancers 10, no. 9: 318. https://doi.org/10.3390/cancers10090318
APA StyleAnandavadivelan, P., Martin, L., Djärv, T., Johar, A., & Lagergren, P. (2018). Nutrition Impact Symptoms Are Prognostic of Quality of Life and Mortality After Surgery for Oesophageal Cancer. Cancers, 10(9), 318. https://doi.org/10.3390/cancers10090318