
Prognostic Value of the Number of Circulating Tumor Cells in Patients with Metastatic Non-Small Cell Lung Cancer

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Information and Study Design
- Histologically proven primary diagnosed non-small cell metastatic lung cancer (IV st.);
- Histologically proven NSCLC of any stage after previous treatment with newly diagnosed distant metastases;
- No medical treatment for metastatic cancer;
- ECOG performance status 0–2;
- Satisfactory hematological parameters (Hb more than 9 g/L, neutrophils more than 3 × 109, platelets more than 100 × 109)
- Satisfactory liver function.
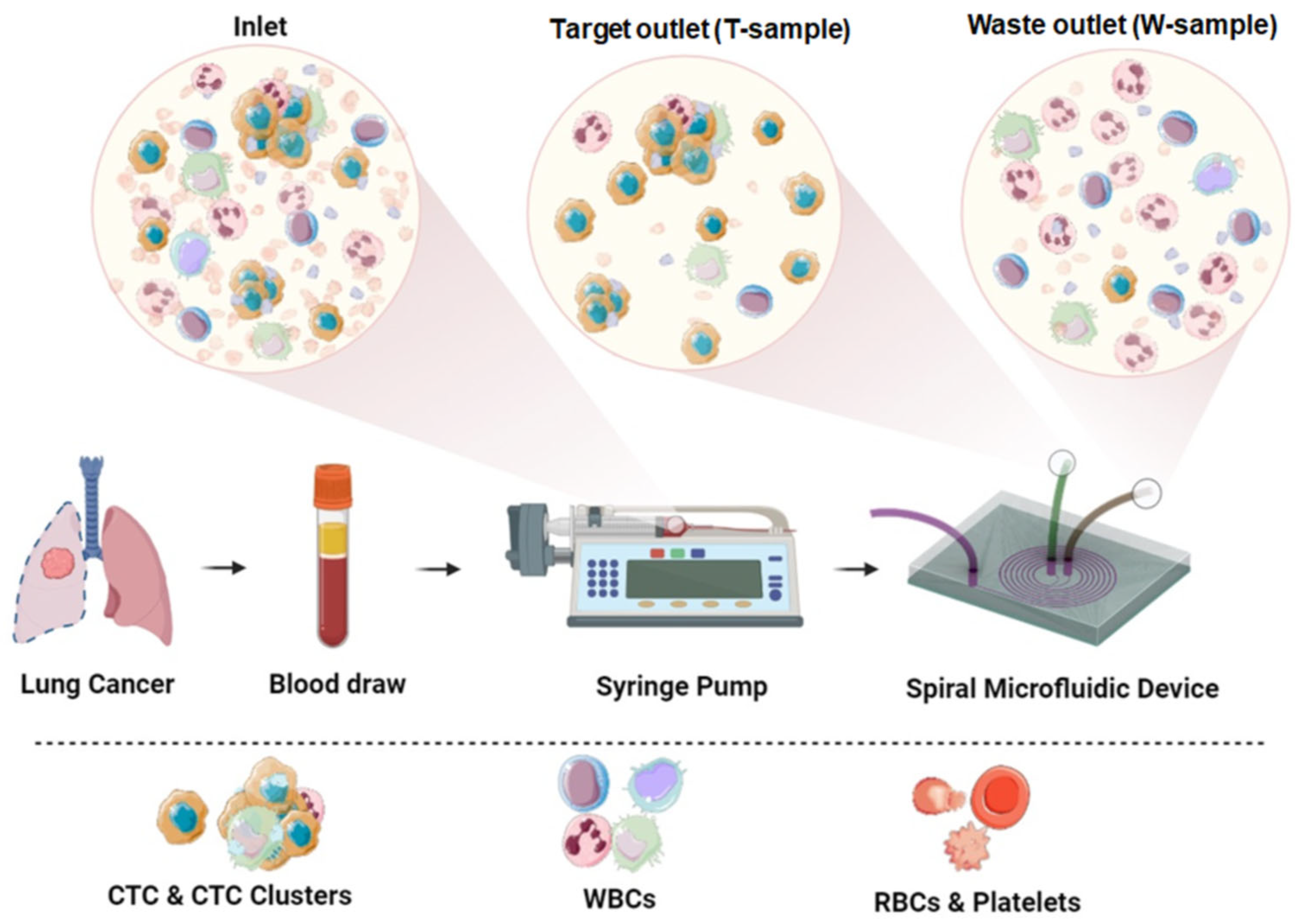
2.2. Method of Collecting Peripheral Blood and Separating CTCs
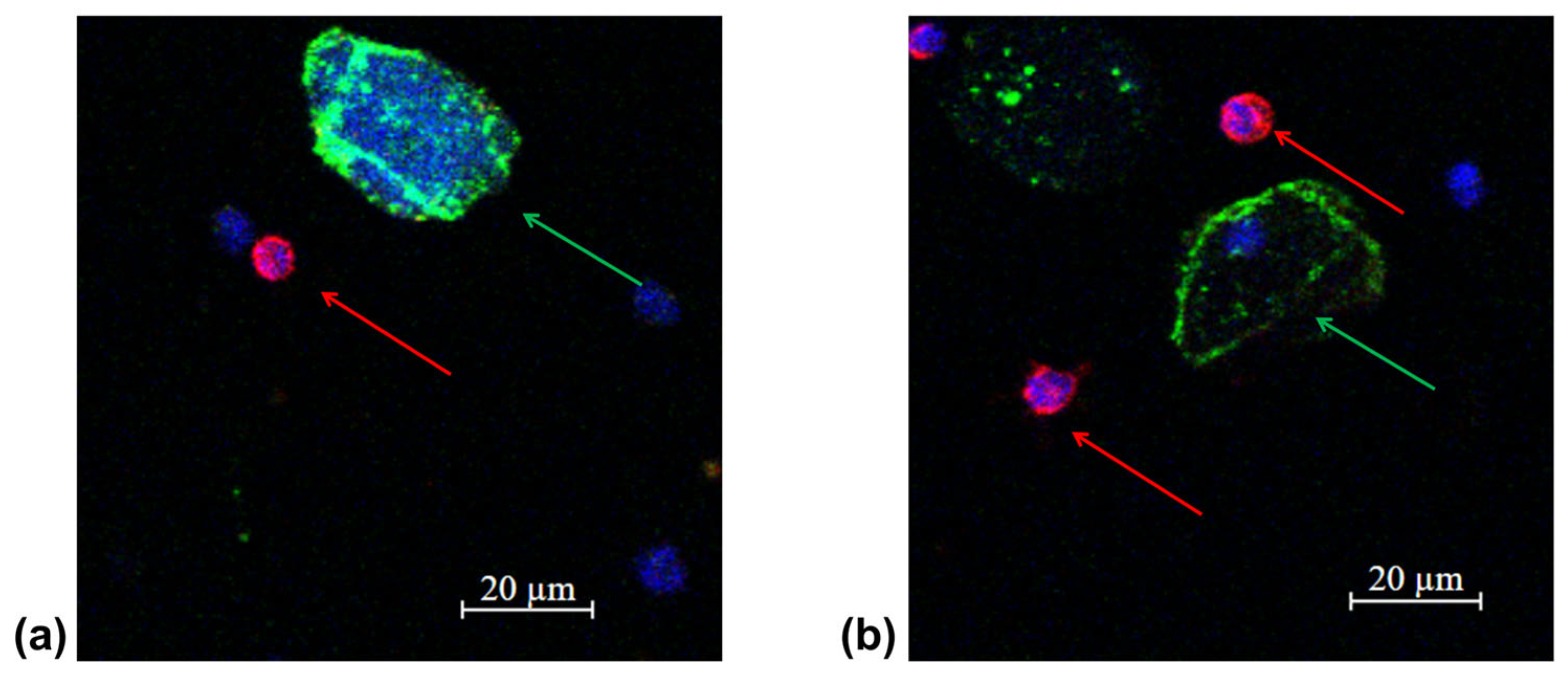
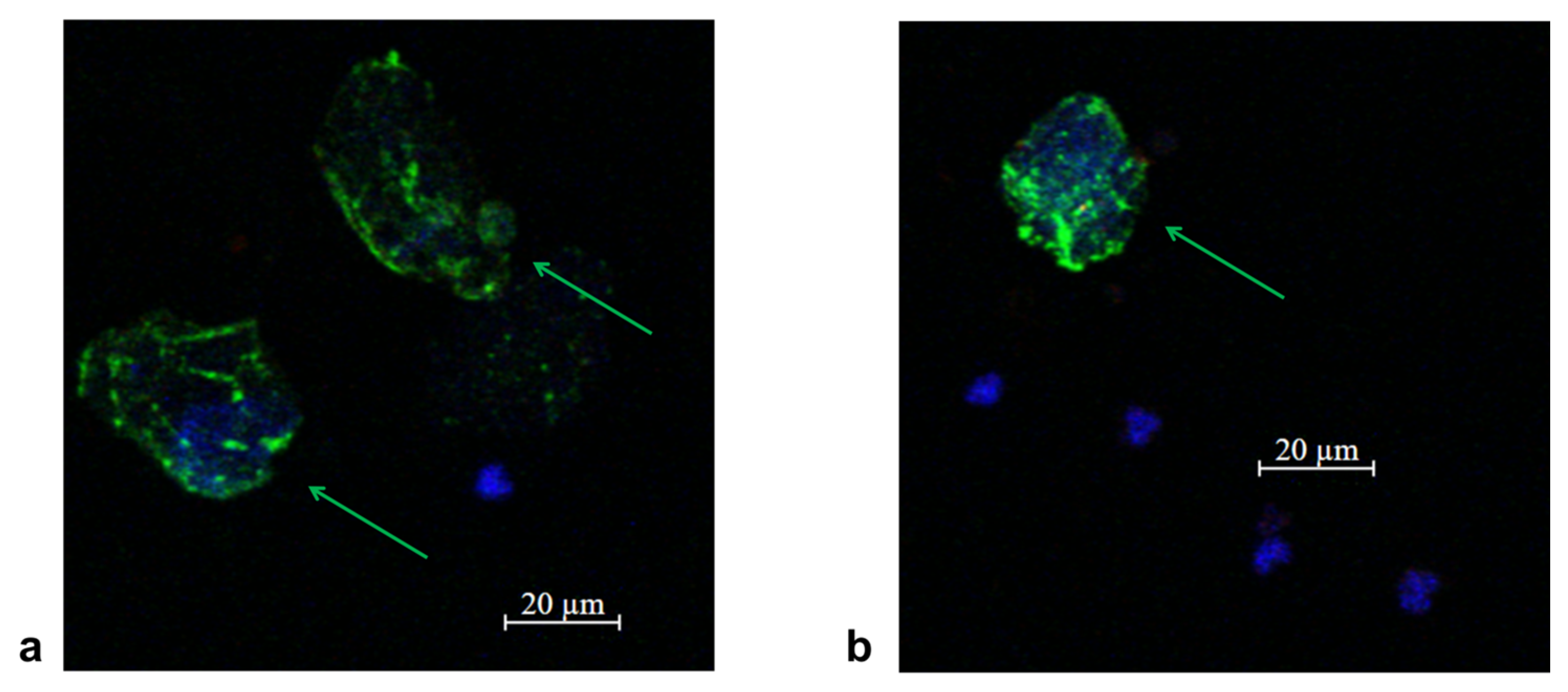
2.3. Method for Characterizing Isolated CTCs Using a Panel of Fluorescent Antibodies
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Patient Survival
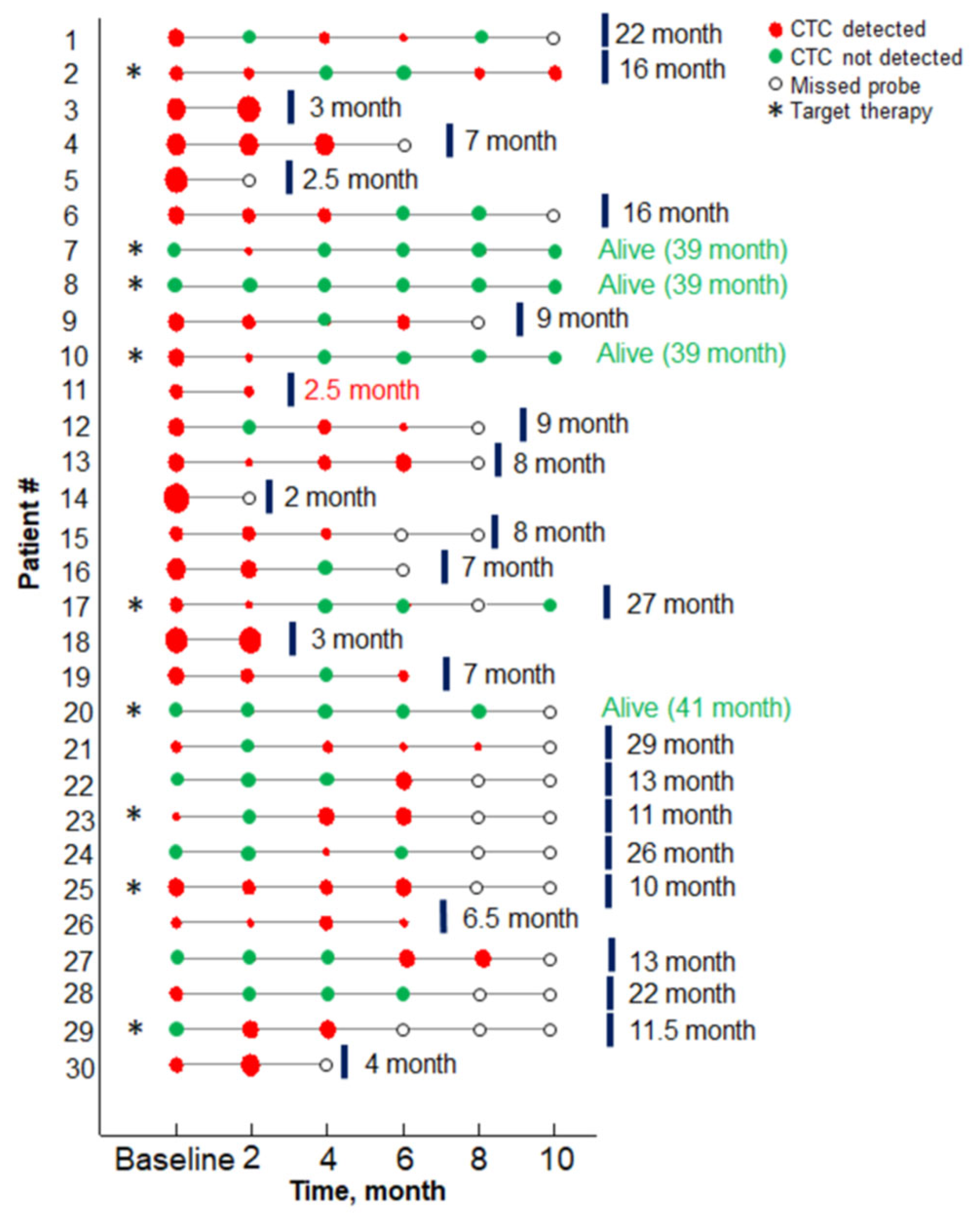
3.3. CTCs Detection
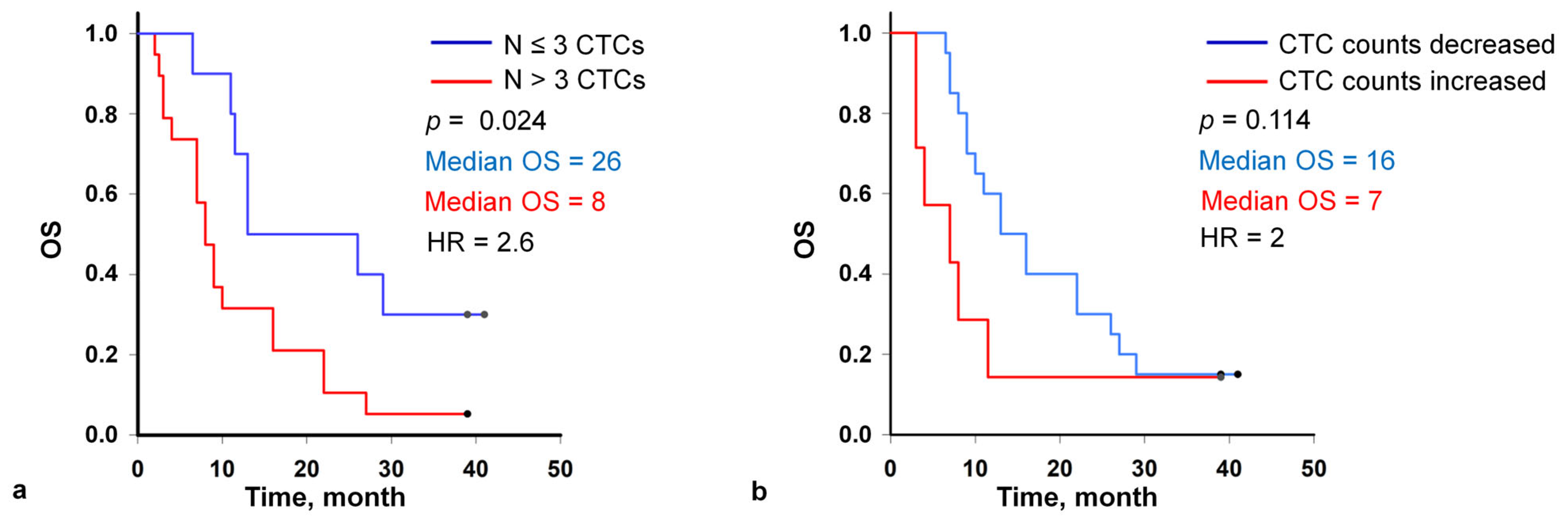
3.4. CTCs Count Associated with Overall Survival
3.5. Target Therapy
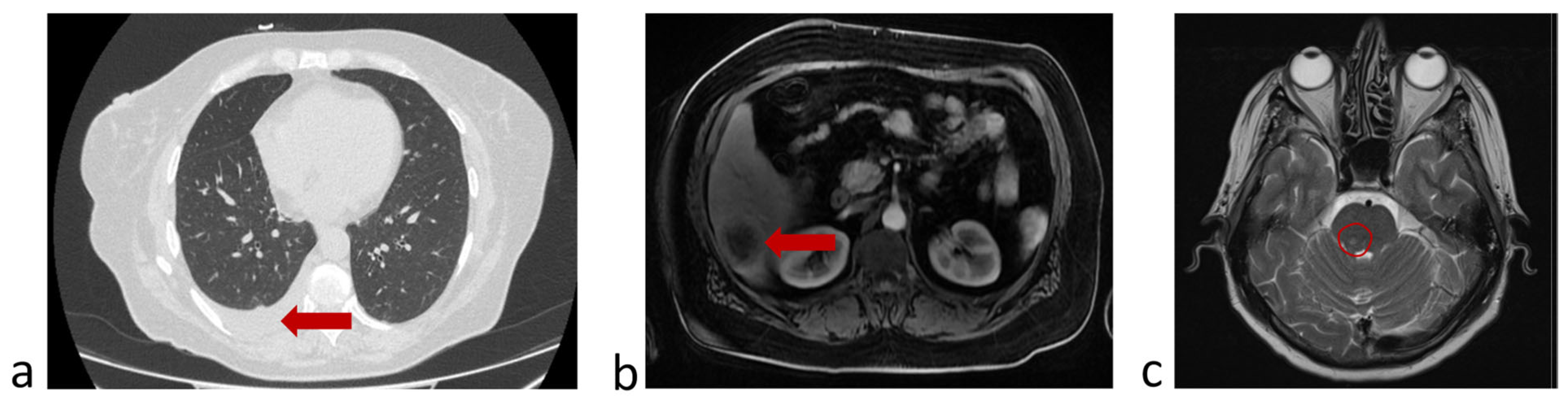
3.6. Clinical Example
3.6.1. A Clinical Example Demonstrating a Favorable Outcome of the Disease and the Evolution of the Number of CTCs Detected in the Peripheral Blood
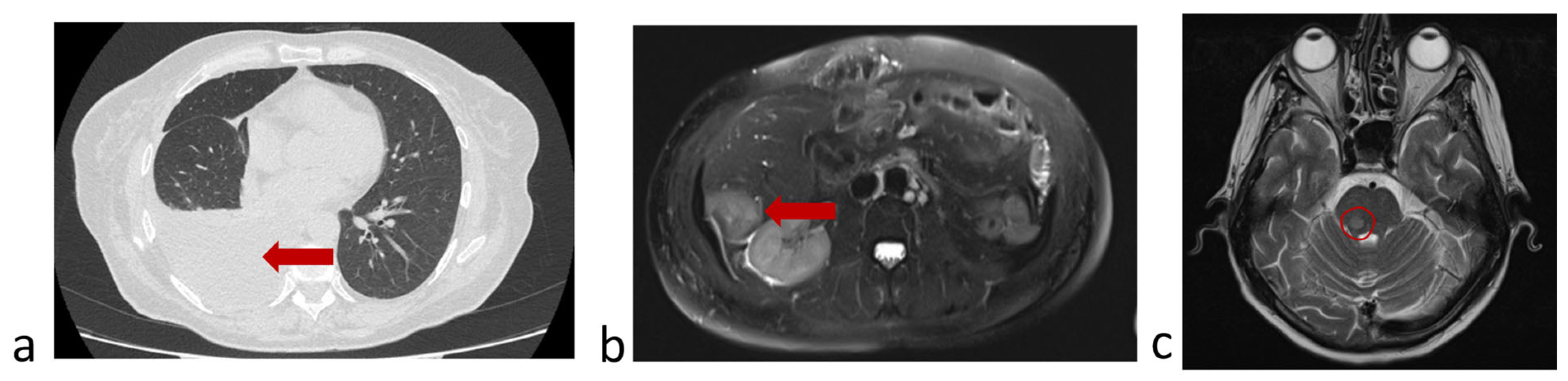
3.6.2. A Clinical Example Demonstrating a Unfavorable Outcome of the Disease and the Evolution of the Number of CTCs Detected in the Peripheral Blood
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Aknowlegments
Conflicts of Interest
Abbreviations
| CI | Confidence intervals |
| CT | Computed tomography |
| CTC | Circulating tumor cells |
| ECOG | Eastern Cooperative Oncology Group |
| EpCAM | Epithelial cell adhesion molecule |
| HR | hazard ratio |
| IHC | Immunohistochemistry |
| MRI | Magnetic resonance imaging |
| NSCLC | Non-small cell lung cancer |
| OS | Overall survival |
| PBS | Phosphate-buffered saline |
| RBC | Red blood cell |
| RECIST | Response evaluation criteria in solid tumours |
| SPECT | Single-photon emission computed tomography |
| T-sample | Target tube |
| W-sample | Waste tube |
| WBC | White blood cell |
References
- Smit, D.J.; Pantel, K. Circulating tumor cells as liquid biopsy markers in cancer patients. Mol. Asp. Med. 2024, 96, 101258. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Wei, S.; Lv, X. Circulating tumor cells: From new biological insights to clinical practice. Signal Transduct. Target. Ther. 2024, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhao, W.; Hodgson, J.; Egan, M.; Cooper Pope, C.N.; Hicks, G.; Nikolinakos, P.G.; Mao, L. CTC-Race: Single-Cell Motility Assay of Circulating Tumor Cells from Metastatic Lung Cancer Patients. ACS Nano 2024, 18, 8683–8693. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, V.; Kaifi, J.T.; Suvilesh, K.N. Circulating Tumor Cells: How Far Have We Come with Mining These Seeds of Metastasis? Cancers 2024, 16, 816. [Google Scholar] [CrossRef]
- Wang, Y.; Yu, X.; Hartmann, D.; Zhou, J. Circulating tumor cells in peripheral blood of pancreatic cancer patients and their prognostic role: A systematic review and meta-analysis. HPB 2020, 22, 660–669. [Google Scholar] [CrossRef]
- Huang, C.; Lin, X.; He, J.; Liu, N. Enrichment and detection method for the prognostic value of circulating tumor cells in ovarian cancer: A meta-analysis. Gynecol. Oncol. 2021, 161, 613–620. [Google Scholar] [CrossRef]
- Zhang, Z.; Luo, R.; Kelly, W.K.; Chen, J.; Donahue, S.; Ip, K.; Handley, N.R.; Tester, W.J.; Tsang, M.L.; Kim, F.J.; et al. Prostein expression on circulating tumor cells as a prognostic marker in metastatic castration-resistant prostate cancer. Prostate Cancer Prostatic Dis. 2024, 27, 339–347. [Google Scholar] [CrossRef]
- Chrenková, E.; Študentová, H.; Holá, K.; Kahounova, Z.; Hendrychova, R.; Souček, K.; Bouchal, J. Castration-resistant prostate cancer monitoring by cell-free circulating biomarkers. Front. Oncol. 2024, 14, 1394292. [Google Scholar] [CrossRef]
- Cani, A.K.; Hayes, D.F. Breast Cancer Circulating Tumor Cells: Current Clinical Applications and Future Prospects. Clin. Chem. 2024, 70, 68–80. [Google Scholar] [CrossRef]
- Kotsifaki, A.; Maroulaki, S.; Armakolas, A. Exploring the Immunological Profile in Breast Cancer: Recent Advances in Diagnosis and Prognosis through Circulating Tumor Cells. Int. J. Mol. Sci. 2024, 25, 4832. [Google Scholar] [CrossRef]
- Tsai, K.Y.; Huang, P.S.; Chu, P.Y.; Nguyen, T.N.A.; Hung, H.Y.; Hsieh, C.H.; Wu, M.H. Current applications and future directions of circulating tumor cells in colorectal cancer recurrence. Cancers 2024, 16, 2316. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Gu, X.; Zuo, Z.; Tian, G.; Liu, J. Prognostic value of circulating tumor cells in patients with bladder cancer: A meta-analysis. PLoS ONE 2021, 16, e0254433. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhang, X.; Yang, Y.; Lin, J.; Zhou, K.; Sun, R.; Diao, D. Circulating tumor cells are a good predictor of tumor recurrence in clinical patients with gastric cancer. Sci. Rep. 2024, 14, 12758. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Lao, X.Q.; Ho, K.-F.; Goggins, W.B.; Tse, S.L.A. Incidence and mortality of lung cancer: Global trends and association with socioeconomic status. Sci. Rep. 2017, 7, 14300. [Google Scholar] [CrossRef]
- de Miguel-Pérez, D.; Bayarri-Lara, C.I.; Ortega, F.G.; Russo, A.; Moyano Rodriguez, M.J.; Alvarez-Cubero, M.J.; Maza Serrano, E.; Lorente, J.A.; Rolfo, C.; Serrano, M.J. Post-surgery circulating tumor cells and AXL overexpression as new poor prognostic biomarkers in resected lung adenocarcinoma. Cancers 2019, 11, 1750. [Google Scholar] [CrossRef]
- Li, Z.; Xu, K.; Tartarone, A.; Santarpia, M.; Zhu, Y.; Jiang, G. Circulating tumor cells can predict the prognosis of patients with non-small cell lung cancer after resection: A retrospective study. Transl. Lung Cancer Res. 2021, 10, 995–1006. [Google Scholar] [CrossRef]
- Tamminga, M.; de Wit, S.; Van De Wauwer, C.; van den Bos, H.; Swennenhuis, J.F.; Klinkenberg, T.J.; Hiltermann, T.J.N.; Andree, K.C.; Spierings, D.C.; Lansdorp, P.M.; et al. Analysis of released circulating tumor cells during surgery for non-small cell lung cancer. Clin. Cancer Res. 2020, 26, 1656–1666. [Google Scholar] [CrossRef]
- Krebs, M.G.; Sloane, R.; Priest, L.; Lancashire, L.; Hou, J.M.; Greystoke, A.; Ward, T.H.; Ferraldeschi, R.; Hughes, A.; Clack, G.; et al. Evaluation and prognostic significance of circulating tumor cells in patients with non-small-cell lung cancer. J. Clin. Oncol. 2011, 29, 1556–1563. [Google Scholar] [CrossRef]
- Lindsay, C.R.; Faugeroux, V.; Michiels, S.; Pailler, E.; Facchinetti, F.; Ou, D.; Bluthgen, M.V.; Pannet, C.; Ngo-Camus, M.; Bescher, G.; et al. A prospective examination of circulating tumor cell profiles in non-small-cell lung cancer molecular subgroups. Ann. Oncol. 2017, 28, 1523–1531. [Google Scholar] [CrossRef]
- Mastromarino, M.G.; Parini, S.; Azzolina, D.; Habib, S.; De Marni, M.L.; Luise, C.; Restelli, S.; Baietto, G.; Trisolini, E.; Massera, F.; et al. Liquid biopsy detecting circulating tumor cells in patients with non-small cell lung cancer: Preliminary results of a pilot study. Biomedicines 2023, 11, 153. [Google Scholar] [CrossRef]
- Tong, B.; Xu, Y.; Zhao, J.; Chen, M.; Xing, J.; Zhong, W.; Wang, M. Prognostic significance of circulating tumor cells in non-small cell lung cancer patients undergoing chemotherapy. Oncotarget 2017, 8, 86615–86624. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Dong, F.; Cui, F.; Xu, R.; Tang, X. The role of circulating tumor cells in evaluation of prognosis and treatment response in advanced non-small-cell lung cancer. Cancer Chemother. Pharmacol. 2017, 79, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xiao, Y.; Zhao, J.; Chen, M.; Xu, Y.; Zhong, W.; Xing, J.; Wang, M. Relationship between circulating tumour cell count and prognosis following chemotherapy in patients with advanced non-small-cell lung cancer. Respirology 2016, 21, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Tamminga, M.; de Wit, S.; Schuuring, E.; Timens, W.; Terstappen, L.W.; Hiltermann, T.J.N.; Groen, H.J. Circulating tumor cells in lung cancer are prognostic and predictive for worse tumor response in both targeted- and chemotherapy. Transl. Lung Cancer Res. 2019, 8, 854–861. [Google Scholar] [CrossRef]
- Mondelo-Macía, P.; García-González, J.; León-Mateos, L.; Anido, U.; Aguin, S.; Abdulkader, I.; Sánchez-Ares, M.; Abalo, A.; Rodríguez-Casanova, A.; Díaz-Lagares, Á.; et al. Clinical potential of circulating free DNA and circulating tumour cells in patients with metastatic non-small-cell lung cancer treated with pembrolizumab. Mol. Oncol. 2021, 15, 2923–2940. [Google Scholar] [CrossRef]
- Shishido, S.N.; Carlsson, A.; Nieva, J.; Bethel, K.; Hicks, J.B.; Bazhenova, L.; Kuhn, P. Circulating tumor cells as a response monitor in stage IV non-small cell lung cancer. J. Transl. Med. 2019, 17, 294. [Google Scholar] [CrossRef]
- Jin, F.; Zhu, L.; Shao, J.; Yakoub, M.; Schmitt, L.; Reißfelder, C.; Loges, S.; Benner, A.; Schölch, S. Circulating tumour cells in patients with lung cancer universally indicate poor prognosis. Eur. Respir. Rev. 2022, 31, 220151. [Google Scholar] [CrossRef]
- Hanssen, A.; Loges, S.; Pantel, K.; Wikman, H. Detection of circulating tumor cells in non-small cell lung cancer. Front. Oncol. 2015, 5, 207. [Google Scholar] [CrossRef]
- Hofman, V.; Bonnetaud, C.; Ilie, M.I.; Vielh, P.; Vignaud, J.M.; Flejou, J.F.; Lantuejoul, S.; Piaton, E.; Mourad, N.; Butori, C.; et al. Preoperative circulating tumor cell detection using the isolation by size of epithelial tumor cell method for patients with lung cancer is a new prognostic biomarker. Clin. Cancer Res. 2011, 17, 827–835. [Google Scholar] [CrossRef]
- Obermayr, E.; Maritschnegg, E.; Speiser, P.; Singer, C.; Schuster, E.M.; Danzinger, S.; Pecha, N.; Zeillinger, R. Circulating rare cells enable highly efficient cancer detection. Cancer Res. 2015, 75, 15. [Google Scholar] [CrossRef]
- Hosokawa, M.; Yoshikawa, T.; Negishi, R.; Yoshino, T.; Koh, Y.; Kenmotsu, H.; Naito, T.; Takahashi, T.; Yamamoto, N.; Kikuhara, Y.; et al. Microcavity array system for size-based enrichment of circulating tumor cells from the blood of patients with small-cell lung cancer. Anal. Chem. 2013, 85, 5692–5698. [Google Scholar] [CrossRef] [PubMed]
- Campton, D.E.; Ramirez, A.B.; Nordberg, J.J.; Drovetto, N.; Clein, A.C.; Varshavskaya, P.; Friemel, B.H.; Quarre, S.; Breman, A.; Dorschner, M.; et al. High-recovery visual identification and single-cell retrieval of circulating tumor cells for genomic analysis using a dual-technology platform integrated with automated immunofluorescence staining. BMC Cancer 2015, 15, 360. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Wu, S.; Wang, Y.; Shi, D. Circulating tumor cell isolation for cancer diagnosis and prognosis. EBioMedicine 2022, 83, 104237. [Google Scholar] [CrossRef] [PubMed]
- Warkiani, M.E.; Guan, G.; Luan, K.B.; Lee, W.C.; Bhagat, A.A.S.; Chaudhuri, P.K.; Tan, D.; Lim, W.T.; Lee, S.C.; Chen, P.C.Y.; et al. Slanted spiral microfluidics for the ultra-fast, label-free isolation of circulating tumor cells. Lab A Chip 2014, 14, 128–137. [Google Scholar] [CrossRef]
- Zhou, J.; Tu, C.; Liang, Y.; Huang, B.; Fang, Y.; Liang, X.; Ye, X. The label-free separation and culture of tumor cells in a microfluidic biochip. Analyst 2020, 145, 1706–1715. [Google Scholar] [CrossRef]
- Volovetskiy, A.B.; Malinina, P.A.; Kapitannikova, A.Y.; Smetanina, S.V.; Kruglova, I.A.; Maslennikova, A.V. Isolation of Circulating Tumor Cells from Peripheral Blood Samples of Cancer Patients Using Microfluidic Technology. Coвременныетехнoлoгии B Mедицине 2020, 12, 62–68. [Google Scholar] [CrossRef]
- Wan, J.W.; Gao, M.Z.; Hu, R.J.; Huang, H.Y.; Wei, Y.Y.; Han, Z.J. A preliminary study on the relationship between circulating tumor cells count and clinical features in patients with non-small cell lung cancer. Ann. Transl. Med. 2015, 3, 352. [Google Scholar]
- Xu, Y.H.; Zhou, J.; Pan, X.F. Detecting circulating tumor cells in patients with advanced non-small cell lung cancer. Genet. Mol. Res. 2015, 14, 10352–10358. [Google Scholar] [CrossRef]
- Wang, S.; Liu, X.; Lv, H.; Yu, J.; Li, H. The detection of circulating tumor cells indicates poor therapeutic efficacy and prognosis in patients with nonsmall cell lung cancer: A systematic review and meta-analysis. J. Evid. Based Med. 2024, 17, 329–340. [Google Scholar] [CrossRef]
- Araghi, M.; Mannani, R.; Heidarnejad maleki, A.; Hamidi, A.; Rostami, S.; Safa, S.H.; Faramarzi, F.; Khorasani, S.; Alimohammadi, M. Recent advances in non-small cell lung cancer targeted therapy; an update review. Cancer Cell Int. 2023, 23, 162. [Google Scholar] [CrossRef]
- Kwon, C.S.; Lin, H.M.; Crossland, V.; Churchill, E.N.; Curran, E.; Forsythe, A.; Tomaras, D.; Ou, S.H.I. Non-small cell lung cancer with EGFR exon 20 insertion mutation: A systematic literature review and meta-analysis of patient outcomes. Curr. Med. Res. Opin. 2022, 38, 1341–1350. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criterion | Number of Patients (%) | |
|---|---|---|
| Age | 41–50 | 5 (17%) |
| 51–60 | 13 (43%) | |
| 61–70 | 8 (27%) | |
| >70 | 4 (13%) | |
| Stage of disease (at time of diagnosis) | IB | 1 (3.33%) |
| IIA | 1 (3.33%) | |
| IIIa | 6 (20%) | |
| IIIb | 1 (3.33%) | |
| IV | 21 (70%) | |
| Histology | Squamous cell carcinoma G2 | 8 (26.7%) |
| Squamous cell carcinoma G3 | 1 (3.3%) | |
| Adenocarcinoma G1 | 2 (7%) | |
| Adenocarcinoma G2 | 7 (23.3%) | |
| Adenocarcinoma G3 | 12 (39.7%) | |
| IHC markers/presence of mutations | Del 19 | 3 (10%) |
| L858R | 2 (6.6%) | |
| T790M | 1 (3.3%) | |
| ALK | 3 (13.3%) | |
| High PD-L1 expression | 7 (23.3%) | |
| No activating mutations | 14 (46.8%) | |
| Drug treatment regimen (1 line) | Target therapy | 9 (30%) |
| Polychemotherapy | 11 (36.7%) | |
| Polychemotherapy + immunotherapy | 5 (17%) | |
| Polychemotherapy + target therapy | 1 (3.3%) | |
| Immunotherapy | 3 (10%) | |
| Changing the line of therapy due to progression | Polychemotherapy—immunotherapy | 1 (3.3%) |
| Target therapy—immunotherapy—polychemotherapy | 1 (3.3%) | |
| Line change after identification of an activating mutation | Polychemotherapy—target therapy | 1 (3.3%) |
| Total | 30 (100%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volovetsky, A.B.; Novikova, V.A.; Boloban, A.; Rzhevskiy, A.S.; Kapitannikova, A.; Ovchinnikova, E.G.; Klejmentjeva, T.P.; Grishin, V.A.; Pigareva, Y.; Zvyagin, A.V.; et al. Prognostic Value of the Number of Circulating Tumor Cells in Patients with Metastatic Non-Small Cell Lung Cancer. Micromachines 2025, 16, 470. https://doi.org/10.3390/mi16040470
Volovetsky AB, Novikova VA, Boloban A, Rzhevskiy AS, Kapitannikova A, Ovchinnikova EG, Klejmentjeva TP, Grishin VA, Pigareva Y, Zvyagin AV, et al. Prognostic Value of the Number of Circulating Tumor Cells in Patients with Metastatic Non-Small Cell Lung Cancer. Micromachines. 2025; 16(4):470. https://doi.org/10.3390/mi16040470
Chicago/Turabian StyleVolovetsky, Arthur B., Victoria A. Novikova, Anastasia Boloban, Alexey S. Rzhevskiy, Alina Kapitannikova, Elena G. Ovchinnikova, Tatjana P. Klejmentjeva, Vladislav A. Grishin, Yana Pigareva, Andrei V. Zvyagin, and et al. 2025. "Prognostic Value of the Number of Circulating Tumor Cells in Patients with Metastatic Non-Small Cell Lung Cancer" Micromachines 16, no. 4: 470. https://doi.org/10.3390/mi16040470
APA StyleVolovetsky, A. B., Novikova, V. A., Boloban, A., Rzhevskiy, A. S., Kapitannikova, A., Ovchinnikova, E. G., Klejmentjeva, T. P., Grishin, V. A., Pigareva, Y., Zvyagin, A. V., Ebrahimi Warkiani, M., & Maslennikova, A. V. (2025). Prognostic Value of the Number of Circulating Tumor Cells in Patients with Metastatic Non-Small Cell Lung Cancer. Micromachines, 16(4), 470. https://doi.org/10.3390/mi16040470